Appendix 1 Cardiovascular Monitoring of HIV-Infected Subjects and Cardiovascular Risk Stratification and Prevention of Cardiovascular Disease in Patients Receiving HAART
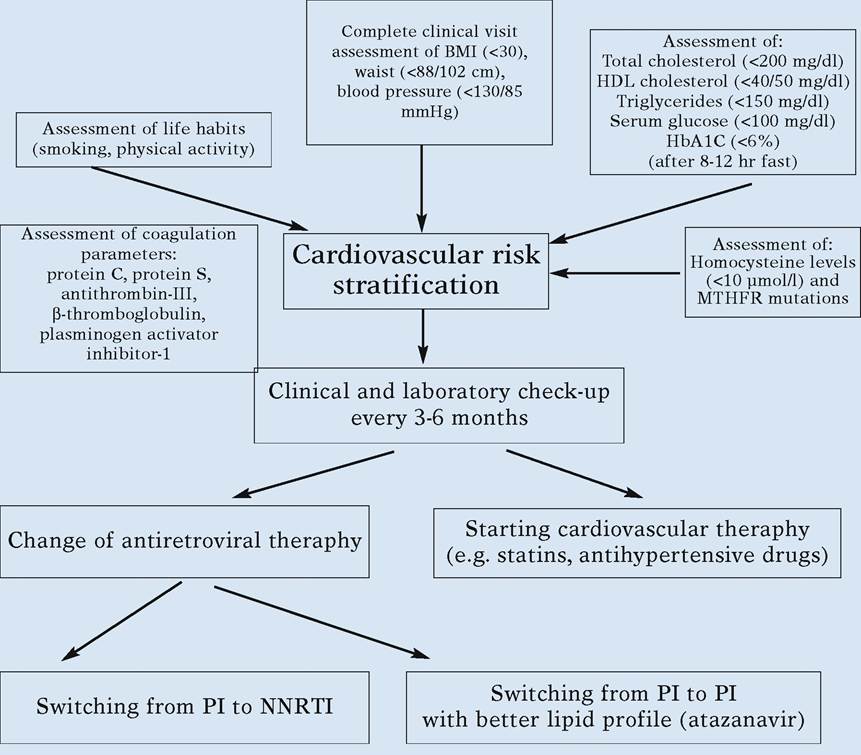
Algorithm 1. Cardiovascular Risk Stratification in HIV-Infected Patients Receiving HAART [1]
Algorithm 8.
European AIDS Clinical Society (EACS) Metabolic Guidelines [5]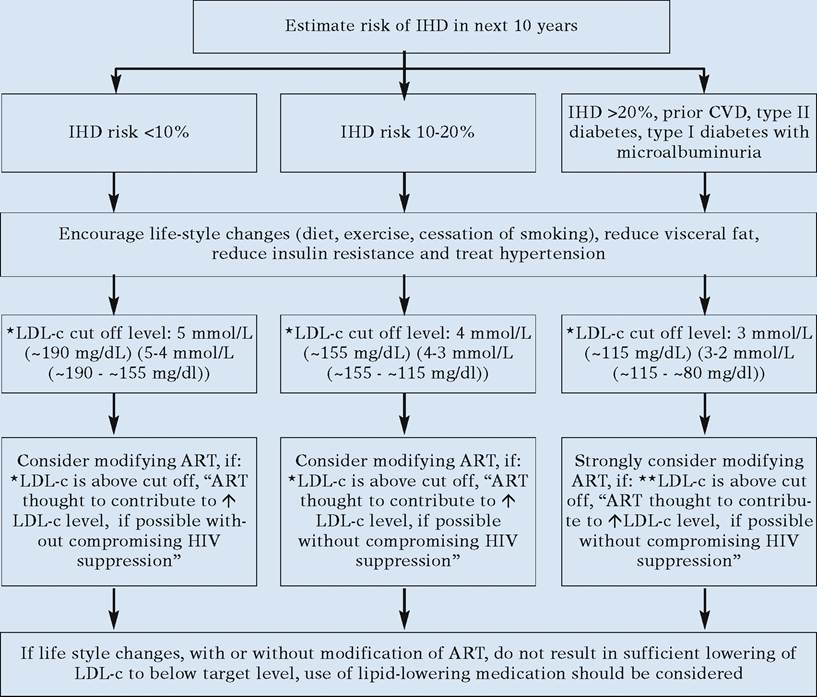
*LDL-c cut off levels (unit: mmol/L (mg/dL)) are higher than in guidelines for the general population (more stringent levels where some experts would consider intervention also indicated in parenthesis below). In cases where LDL-c cannot be reliably calculated because of high triglyceride levels, the non- HDL-c target level should be used which is 0.8 mmol/L (30 mg/dl) higher than the corresponding LDL-c target
**Options for ART modification include: (1) replacing PI(/r) by NNRTI, by another PI(/r) known to cause less metabolic disturbances or by abacavir; should not be done if patient is known or suspected to harbour archived virus containing drug-related mutations against the new drug the patient is switched to (switch to abacavir should not be done in case (archived) thymidine analogue mutations are known or suspected to be present (e.g. due to prior use of suboptimal mono- or dual NRTI therapy); (2) replacing d4T or ZDV by ABC or TDF. In patients with >20% 10 year risk or with prior CVD, the risk of CVD events and cardiac death will usually be higher than risk of progression to AIDS or death and in such patients a strategy to reduce risk of CVD by switching ART is hence most appropriate
Algorithm 9.
Switch Strategies of Antiretroviral Therapy: Rationale and Requirements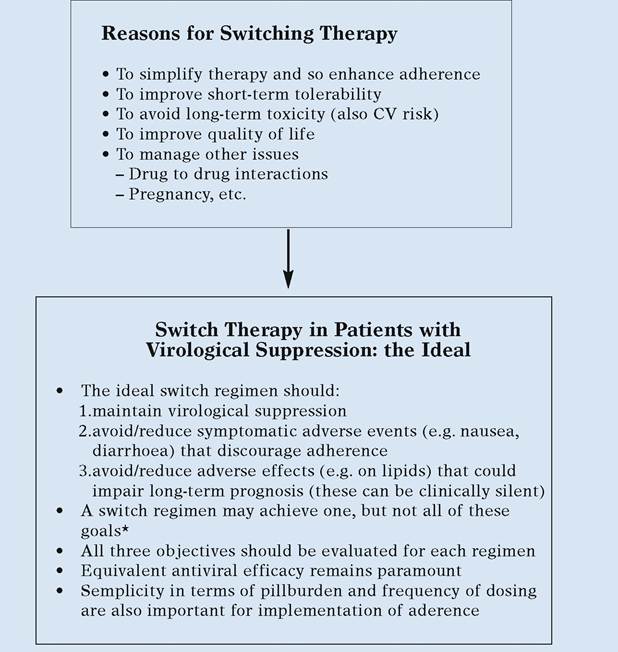
[1] HAART including Atazanavir schemes have been shown to possess all three requirements above
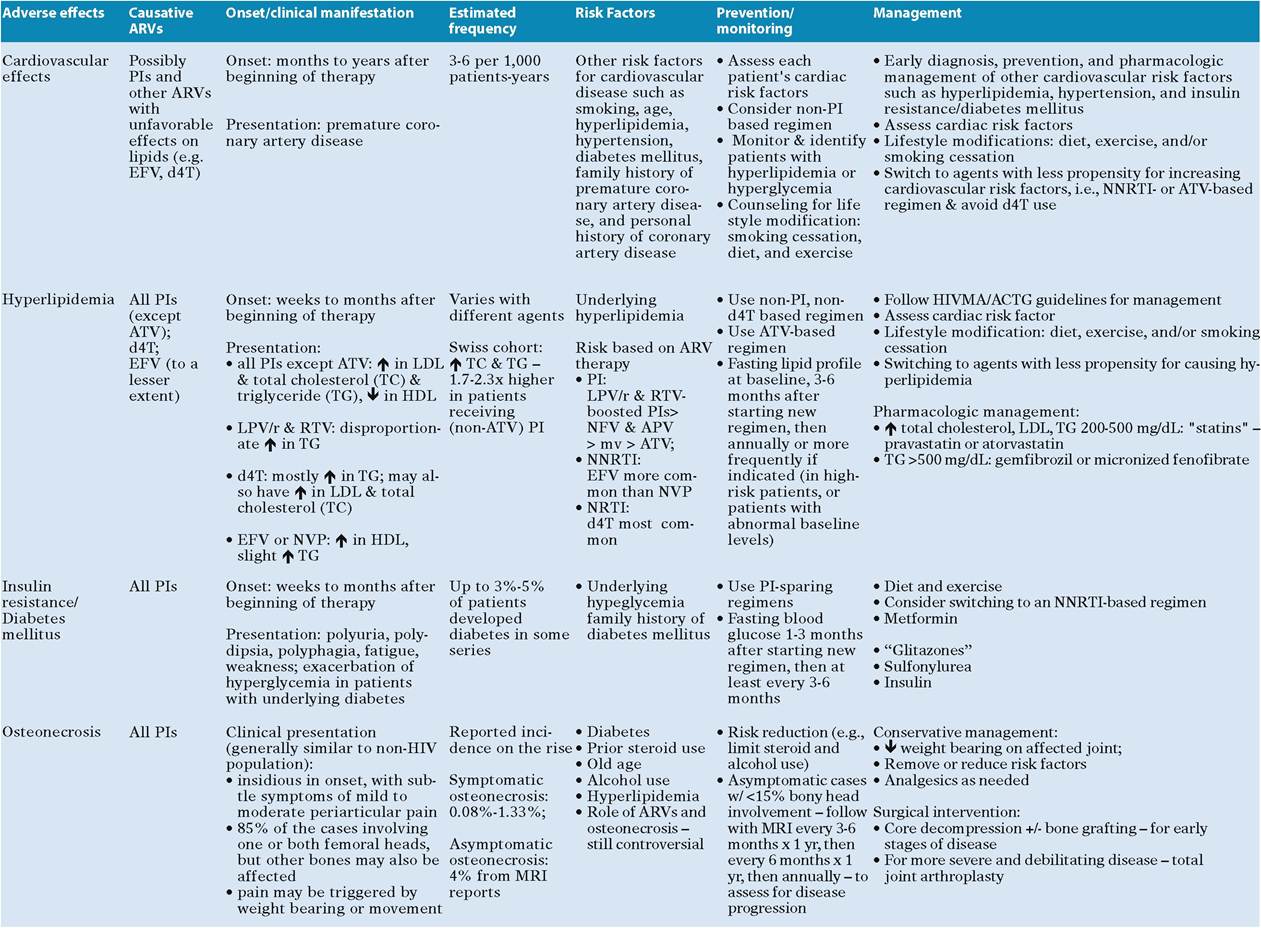
Table 1 Antiretroviral therapy-associated adverse effects and management recommendations [9]
References
1. Volberding P, Murphy R, Barbaro G et al (2003) The Pavia Consensus Statement. AIDS 17(S1):S170-S179
2. Chobanian AV, Bakris GL, Black HR et al (2003) The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA 289:2560-2572
3. Hadigan C, Yawetz S,Thomas A, Havers F, Sax PE, Grinspoon S (2004) Metabolic effects of rosiglita- zone in HIV lipodystrophy: a randomized, controlled trial. Ann Intern Med 140:786-794
4. Carr A, Workman C, Carey D et al (2004) No effect of rosiglitazone for treatment of HIV-1 lipoatrophy: randomised, double-blind, placebo- controlled trial. Lancet 363:429-438
5. European AIDS Clinical Society (EACS). Guidelines on the prevention and management of metabolic diseases in HIV. http://www.eacs.- eu7c_acceuil.htm
6. Gatell J, Salmon-Ceron D, Lazzarin A et al (2007) Efficacy and safety of atazanavir-based highly active antiretroviral therapy in patients with virologic suppression switched from a stable, boosted or unboosted protease inhibitor treatment regimen: the SWAN study (AI424- 097) 48-week results. CID 44 (1 June)
7. Mallolas J, Podzamczer D, Domingo P et al (2007) Efficacy and safety of switching from boosted lopinavir to boosted atazanavir in patients with virologic suppression receiving a LPV/r-containing HAART: the ATAZIP study, - IAS - Poster WEPEB117LB
8. Rubio R, Carmena J, Asensi et al (2007) Effect of simplification from protease inhibitor to boosted atazanavir -based regimens in real-life conditions: Preliminary results of GESIDA 44/04 SIMPATAZ study EACS Poster P7.5/03
9. Panel on Antiretroviral Guidelines for Adult and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Department of Health and Human Services. January 29, 2008; 1-128. Available at http://www.aidsinfo.nih.gov/ContentFiles/Adul- tandAdolescentGL.pdf. Accessed 18/02/2008 [page 82, table 18b]