Arrhythmias
Both tachy- and bradyarrhythmia may be observed in HIV-infected patients in relation to structural alterations of the endocardium (infective endocarditis), of the myocardium (myocarditis, dilated cardiomyopathy), and of the pericardium (infective and neoplastic pericarditis and myopericarditis).
In HIV-infected patients with myocarditis, the most frequent arrhythmias are ventricular ectopic beats. Bradycardias (e.g., left bundle branch block and/or atrioventricular block) may be observed in patients with HIV-associated dilated cardiomyopathy resulting from fibrous degeneration of the conduction system [7].id="Picutre 112" class="lazyload" data-src="/files/uch_group75/uch_pgroup303/uch_uch7204/image/image107.jpg">
Fig.4 Dilated cardiomyopathy in an HIV-infected patient (four-chamber apical view). Left ventriculalr ejection fraction: 25%. Note the dilatation of both left and right cardiac chambers. RA, right atrium; RV, right ventricle; LA, left atrium; LV, left ventricle
Side effects of both antiretroviral drugs or drugs used in the treatment and/or prophylaxis of opportunistic infections and neoplasms. Ganciclovir, amphotericin B, Cotrimoxazole (trimethoprim-sulfamethoxazole), and pentamidine may cause Torsades de pointes (TdP) that can degenerate into ventricular fibrillation and sudden cardiac death (Fig. 5). Torsades de pointes (TdP) is related to prolongation of the ventricular action potential duration (QTc interval of the electrocardiogram >0.45 s) and it has also been described in relation to the administration of macrolide antibiotics (erythromycin, clarithromycin). Uncorrected electrolyte alterations (e.g., hypokalemia, hypomagnesemia, hypocalcemia) related to malnutrition and/or to chronic diarrhea or electrolyte imbalances induced by diuretics are also associated. These alterations, which should be evaluated and treated as early as possible, may further contribute to prolonging the QTc interval.
Use of central nervous system stimulant drugs (e.g., cocaine, amphetamines). Cocaine abuse has been associated with myocarditis, myocardial infarction, and dilated cardiomyopathy even in HIV-negative subjects, possibly because of intermittent microvas- cular spasm resulting from catecholamine surges associated with a high risk of ventricular arrhythmia.
Particularly in the ED, the first line of therapy for TdP is to stop medications suspected of prolonging the QT interval and to correct electrolyte imbalances. Intravenously administered magnesium sulfate is immediately indicated (loading dose of 1-2 g, mixed in 50-100 ml of saline, over 5-10 min followed by a continuous infusion of 1.0-2.0 g/h over 4-6 h), whereas i.v. infusion of isoproterenol (0.01-0.02 mcg/kg per minute) in the absence of known or suspected coronary artery disease may accelerate the heart rate and suppress ventricular arrhythmias while temporary ventricular pacing (overdrive pacing) is initiated [1].
In HIV-infected patients, hemodynami- cally stable sustained monomorphic wide- QRS complex tachycardia is another diagnostic challenge for the emergency physician, as ventricular tachycardia (VT) must be distinguished from supraventricular tachycardia (SVT). In particular, SVT with an accessory pathway, preexisting bundlebranch block, or rate-dependent bundlebranch block should be considered. SVT with aberrant conduction is frequently observed in HIV-infected patients with dilated cardiomyopathy and histological diagnosis of myocarditis [1] (Fig. 6). In patients that are hemodynamically stable with no symptoms or clinical evidence of tissue hypoperfusion or shock, initial management should proceed under the presumption that the arrhythmia is VT, and electric cardioversion is the preferred therapy. If electrical cardioversion is not possible, empiric pharmacological therapy may be necessary with agents such as procainamide or amiodarone, which possess efficacy against VT and SVT and are also acceptable in patients with accessory pathway conduction [1].
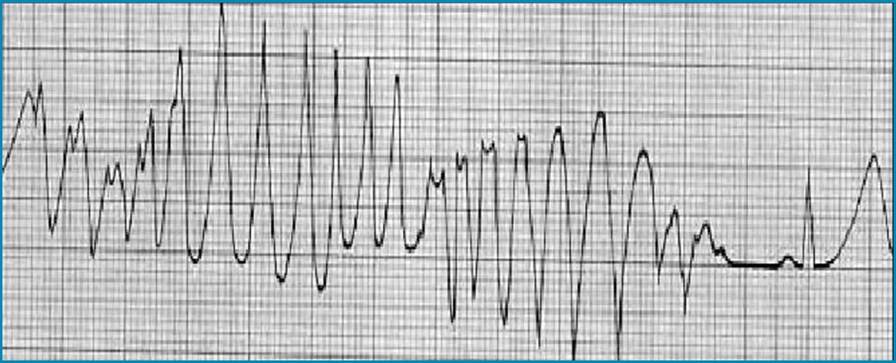
Fig. 5 Run of Torsade de pointes in an HIV-infected subject receiving pentamidine as prophylaxis for Pneumocystis carinii pneumonia during Holter electrocardiographic monitoring (lead CM5). Note the prolongation of the QT interval of the QRS complex following the arrhythmic run (0.50 s). (From [1], with permission from Elsevier)
Procainamide is administered in an infusion of 20 mg/min until the arrhythmia is suppressed or hypotension ensues, or when a total of 17 mg/kg of the drug has been given. Amiodarone is administered as 150 mg over 10 min, followed by 150 mg over the next 30 min, and then 1 mg/min infusion for 6 h followed by 0.5 mg/min, to a maximum daily dose of 2 g. If the patient is in shock or in congestive heart failure (hemodynamically unstable), a wide-QRS complex tachycardia should be presumed to be VT, which requires immediate termination of synchronized cardioversion [1].