Box 1.1 Early history of the epidemic
1981 Cases of Pneumocystis carinii pneumonia and Kaposi's sarcoma in the USA
1983 Discovery of the virus. First cases of AIDS in the UK
1984 Development of antibody test
The first recognised cases of the acquired immune deficiency syndrome (AIDS) occurred in the summer of 1981 in America.
Reports began to appear of Pneumocystis carinii pneumonia and Kaposi’s sarcoma in young men, who it was subsequently realised were both homosexual and immunocompromised. Even though the condition became known early on as AIDS, its cause and modes of transmission were not immediately obvious. The virus now known to cause AIDS in a proportion of those infected was discovered in 1983 and given various names. The internationally accepted term is now the human immunodeficiency virus (HIV). Subsequently a new variant has been isolated in patients with West African connections — HIV-2.The definition of AIDS has changed over the years as a result of an increasing appreciation of the wide spectrum of clinical manifestations of infection with HIV. Currently, AIDS is defined as an illness characterised by one or more indicator diseases. In the absence of another cause of immune deficiency and without laboratory evidence of HIV infection (if the patient has not been tested or the results are inconclusive), certain diseases when definitively diagnosed are indicative of AIDS. Also, regardless of the presence of other causes of immune deficiency, if there is laboratory evidence of HIV infection, other indicator diseases that require a definitive, or in some cases only a presumptive, diagnosis also constitute a diagnosis of AIDS.
In 1993 the Centers for Disease Control (CDC) in the USA extended the definition of AIDS to include all persons who are severely immunosuppressed (a CD4 count 1 month
• Cytomegalovirus disease other than in liver, spleen, nodes
• Herpes simplex virus (HSV) infection
• mucocutaneous ulceration lasting >1 month
• pulmonary, oesophageal involvement
• Kaposi’s sarcoma in patient bgcolor=white>(anal)
The advent of an effective antibody test in 1984 has allowed for a clearer understanding of the changing prevalence and natural history of HIV infection. Surveys show that the proportion of individuals infected needs to be high before cases of AIDS start to become apparent. It also underlines the importance of health education campaigns early in the epidemic, when the seroprevalence of HIV is low. Once cases of AIDS start to appear the epidemic drives itself and a much greater effort is required in terms of control and medical care.
Within countries one finds considerable variation in seroprevalence levels for HIV. Over 70% of cases of AIDS and HIV infection within the UK occur and are seen in the Thames regions (London and the surrounding area). Among different groups one also finds geographical differences. For example, the rates among drug users is higher in Edinburgh than London, and for gay men higher in London than anywhere else in the UK. This is also found in the developing world; for example, in Tanzania and Uganda, the urban level of HIV infection in men and women can be five times higher than rural rates.
T he use of highly active antiretroviral therapy (HAART) in resource-rich countries has resulted in an increase in life expectancy. This, in combination with the increase in new HIV infections, means that the prevalent pool of those infected, and potentially infectious, is increasing. This presents a continuing challenge for health promotion and a re-statement of the importance of safe sex techniques, particularly condom use (see chapter 16).
Table 1.4 AIDS: adult patient groups in the USA and UK
USA (June 99) UK (Dec. 00)
| Patient groups | n | % | n | % |
| Men who have sex with men | 334073 | 48 | 11 345 | 66 |
| Intravenous drug user | 179 228 | 26 | 1095 | 6 |
| Men who have sex with men | 45 266 | 6 | 307 | 2 |
| and IV drug user | ||||
| Received blood/haemophilia | 13 440 | 2 | 828 | 5 |
| Heterosexual contact | 70 582 | 10 | 3391 | 20 |
| Other/undetermined | 60 159 | 8 | 185 | 1 |
| Total | 702748 | 100 | 17 151 | 100 |
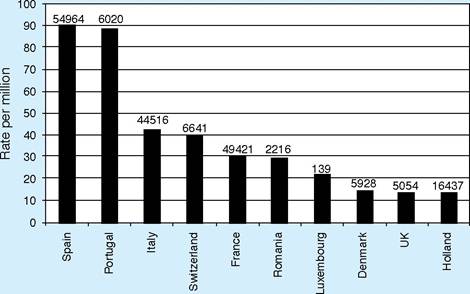
Figure 1.3 AIDS in Europe — top ten countries 1999
Table 1.5 Three main exposure categories (AIDS): % total for various countries in Europe, 1999
Homosexual/Injecting drug
Heterosexual
| bisexual men | users | exposure | |
| Spain | 14.0 | 65.0 | 13.0 |
| Italy | 14.0 | 61.0 | 15.0 |
| Portugal | 20.0 | 47.0 | 26.0 |
| France | 45.0 | 24.0 | 20.0 |
| UK | 68.0 | 6.5 | 18.0 |
| Denmark | 67.0 | 8.0 | 17.0 |
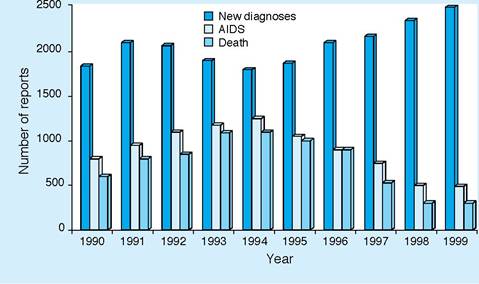
Figure 1.4 New diagnoses, AIDS cases and deaths reported in the year in which they occurred — United Kingdom
AIDS results in a considerable cost not only in human suffering also to health services.
Other costs include time off work and the effect of the deaths of young people on national productivity. AIDS represents a major public health problem in the world. A clear understanding of the epidemiology forms the basis of developing a strategy of control ranging from health education to research.The data on AIDS/HIV in the UK is reproduced with permission from the Communicable Disease Surveillance Centre (CDSC) and the United Nations AIDS Programme.
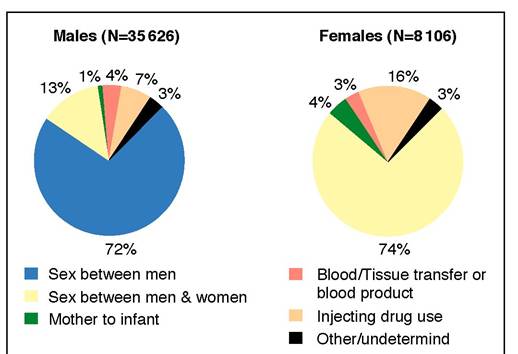
Figure 1.5 HIV-infected individuals diagnosed in the UK by exposure category: to December 2000
2