Drug toxicities
The tolerability and side-effects of a combination regimen is very important in determining the antiviral response. In clinical practice 40—50% of patients will not have sustained falls in plasma viral load by one year of therapy and a major factor contributing to this is poor tolerability.
Drug-specific side-effects are listed in Table 9.6.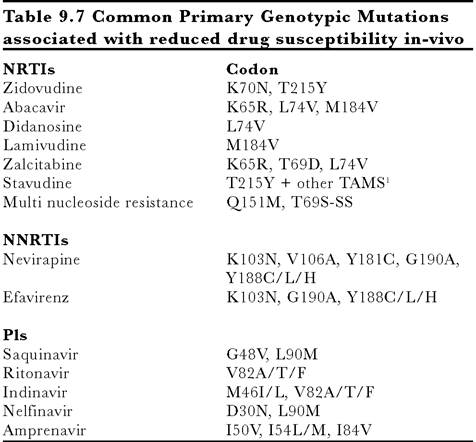
1. TAMS: Thymidine analogue mutations
2. Resistance profile of lopinavir/r in-vivo is uncertain
Clinically relevant phenotypic resistance may require only a single primary mutation or 2 or more primary and secondary mutations. Interpretation of a genotypic test is complex and requires expert advice.
Box 9.9 Role of resistance testing
• detection of transmitted resistance in primary infection
• detection of resistance prior to starting treatment for the first time
• guide choice of new treatment regimen in patients experiencing virological treatment failure on first or subsequent regimens
• guide treatment choice in pregnant mothers for prevention of vertical transmission
The utility of genotypic and phenotypic resistance tests are continuing to be evaluated.
In the last two to three years abnormalities of fat redistribution have been observed in patients on combination regimen. Observational cohort studies suggest that lipodystrophy may occur in up to 50—60% of patients after one to two years on therapy. Patients either present with peripheral fat wasting affecting the buttocks, limbs and face or fat accumulation round internal viscera in the abdomen resulting in a distended abdomen and bloating. The exact pathogenosis of these fat distribution syndromes is unknown but age of patient, antiretroviral drug therapy and time on therapy may all be implicated. They have been reported in both protease inhibitor and NRTI-containing combination regimens, and it is likely that it is a mixed syndrome with a multifactorial cause. The occurrence of lipodystrophy can affect the psychological well being of the patient but as yet we do not know how it is best managed.
It has recently been suggested that mitochondrial toxicity may account for some of the toxcities associated with the NRTIs as a result of inhibition of mitochrondirial gamma DNA polymerase. Severe lacticacidosis is a rare complication of NRTI therapy.