Glossary
Abacavir (Ziagen, ABC): A nucleoside like AZT, and the most potent drug in its class. The main side effect is a serious allergic reaction with high fever, gastrointestinal upset, and a rash, usually during the first 30 days of treatment.
If these symptoms occur, the drug should be stopped and should not be taken again. If you think you’re having these reactions, always check with your doctor.ACTU: ACTU stands for AIDS clinical trial unit. ACTUs are a consortium of medical centers throughout the United States that conduct clinical trials of drugs for treating people with HIV infection. Specifically, the drugs are for treating HIV itself, for treating complications (opportunistic infections or tumors), and for stimulating the immune system. The entire consortium of ACTUs is called ACTG; the G stands for group. The ACTG is funded federally, at about $60 million yearly, through the National Institutes of Health. The ACTG has two components: AACTG (adult ACTG) and PACTG (pediatric ACTG). The ACTG is the largest clinical trials group for HIV infection in the world: it has the largest budget, the largest number of investigators, and the largest number of participants.
Acute HIV infection, or acute retroviral syndrome: Acute HIV infection refers to the first illness that occurs after infection with HIV. Symptoms show up about one to three weeks after infection. Typical symptoms are sore throat, fatigue, headache, fever, and a rash. The illness precedes seroconversion, when the standard blood test for antibodies to HIV first turns positive. The illness lasts about one to two weeks. During this period, the risk of transmission is great. Avoid sex and get medical attention.
Acyclovir (Zovirax): A drug used for infections caused by herpes simplex (genital herpes or “fever blisters” or “cold sores”) or herpes zoster (shingles). Acyclovir is available as a cream, a pill, or for intravenous administration.
It has been used in millions of patients since 1982 and has nearly no side effects. Acyclovir not only treats herpes outbreaks, but when taken daily, it also prevents them from recurring.ADAP, or AIDS Drug Assistance Program: A provision in the Ryan White Care Act that makes HIV drugs available to people who can’t afford them with their own income plus assets or with their health care plans.
Adenopathy: Enlargement of lymph nodes, which can be felt in the neck, armpit, or groin; or seen on a CT scan of the chest or abdomen. Enlarged lymph nodes usually mean infection of some sort or, less commonly, a tumor like lymphoma. See Lymphadenopathy.
Adherence: The ability to adhere to or comply with something. In the context of HIV infection, adherence means the ability to stay on the regimen of antiretroviral drugs. Good adherence means taking 70 to 95 percent of HIV drugs at the right time.
Adverse event: Medical term for a complication of a drug—allergic reactions, side effects, toxicities.
AIDS: AIDS stands for acquired immune deficiency syndrome. AIDS is the late stage of an infection caused by the human immunodeficiency virus, or HIV. The virus infects the CD4 cell (also called a T4 cell, a T4 lymphocyte, and a T-helper cell), which is critical to immune defenses. As the numbers of these cells decrease, the immune system weakens until it becomes susceptible to what are called opportunistic infections and opportunistic tumors. These infections and tumors are called opportunistic because the microbes that cause them are opportunists, taking advantage of a weakened immune system. A person with HIV infection has AIDS if he or she has a CD4 cell count below 200 or one or more of certain specific opportunistic infections or tumors, called AIDS-defining diagnoses, that go along with a severely weakened immune system. The list of AIDS-defining diagnoses was drawn up by the Centers for Disease Control and Prevention (CDC) in 1986 and has been modified twice, once in 1987 and again in 1993.
The CDC’s latest definition of AIDS includes all the old criteria and adds a CD4 count of less than 200.AIDS-advocacy organizations: See Community-based organizations.
AIDS-defining diagnosis: A person with an AIDS-defining diagnosis has HIV infection plus any one of a number of common infections that result from a specific defect caused by HIV. According to the Centers for Disease Control and Prevention, the complications included as AIDS-defining diagnoses are, in order of frequency, pneumocystis pneumonia, wasting, candidal esophagitis, tuberculosis, CMV infection, Kaposi’s sarcoma, Mycobacterium avium complex infection, chronic herpes simplex, HIV dementia, toxoplasmosis, and cryptococcal meningitis. These are not the only AIDS-defining diagnoses, but they are the most common. The CD4 count is usually, but not necessarily, below 200. In fact, the average CD4 count for most people with AIDS-defining diagnoses is 50 or less.
AIDS dementia complex: See HIV-associated dementia.
AIDS-related complex: See ARC.
Alprazolam (Xanax): See Benzodiazepines.
Alternative medicine: The alternatives to traditional medicine. Alternative medicine can include use of herbs, acupuncture, Chinese medicine, meditation, and a variety of other approaches to medical care. Complementary medicine is another name for alternative medicine. Alternative medicine generally does not have scientific verification of its effectiveness; if it did, it would be traditional medicine. Most physicians don’t object to their patients using alternative medicine, as long as the alternative medicine is not being used in place of drugs known to work, or causing interactions with those drugs, or causing harm.
Amitriptyline: Amitriptyline hydrochloride (or, e.g., Elavil) is one of a group of drugs called tricyclic antidepressants that are grouped together because of their chemical similarities. Other tricyclic antidepressants include amoxapine (or Asendin), desipramine hydrochloride (or Pertofrane or Norpramin), doxepin hydrochloride (or Adapin or Sinequan), imipramine hydrochloride (or Tofranil), and nortriptyline hydrochloride (or Aventyl Hydrochloride or Pamelor).
Tricyclic antidepressants are used to treat depression and the peripheral neuropathy that causes painful feet. In many cases, the dose is arbitrary: many people start on a low dose and have the dose increased as necessary. Side effects are common, but usually not severe enough to stop treatment. The main side effects are drowsiness, weakness, and fatigue; dry mouth; constipation; and low blood pressure and dizziness. Some people gain weight or have decreased libido. All of these side effects are dose-related, meaning the higher the dose, the more common and severe the side effect. Because the drugs cause drowsiness, they are often given before bedtime.Amphotericin B: The antibiotic amphotericin B is the standard treatment for many infections caused by fungi, including most of the fungi that affect people with HIV infection: Candida, Cryptococcus, Histoplasma, Coccidioides, and Aspergillus. Amphotericin B, which is usually given by vein, is highly effective. Unfortunately, it is also one of the most toxic antibiotics known. The most important side effects include kidney damage, anemia (see below), disturbances in the balance of electrolytes, nausea and vomiting, fever and chills, and phlebitis or inflammation of the vein into which the drug is injected. Many of these side effects can be lessened or eliminated by stopping the drug, or by concurrently taking medicines to combat the side effects, or by taking new preparations of amphotericin that are much more expensive but much easier to take. Because of amphotericin B’s toxicity, other drugs, like ketoconazole, itraconazole, voriconazole, and fluconazole, are given when they are considered to be as effective or sometimes even more effective. Another option to beat the side effects of amphotericin is to use a special formulation called AmBisome, which does everything amphotericin does (in most cases) with a fraction of the side effects. The problem with Am- Bisome is that it costs $1,500 per day, compared to amphotericin’s cost of $16 per day.
Anemia: Anemia means that the number of red cells in the blood is reduced. Red blood cells are responsible for delivering oxygen to all parts of the body. When the reduction is severe, the result is fatigue. Anemia can be caused by HIV infection itself, by a complication, or by several of the drugs commonly taken by people with AIDS. Drugs often responsible include trimethoprim-sulfamethoxazole, other sulfa drugs, pentamidine, amphotericin B, and AZT. When the anemia is severe, it can be corrected with transfusions or a drug called erythropoietin (EPO). When drugs are responsible, the drugs can be reduced in dose or discontinued.
Antibiotics: Antibiotics are drugs made from natural substances (as opposed to drugs made artificially) that inhibit the growth of certain microbes. Antibiotics may be effective against any of the classes of microbes—including bacteria, fungi, parasites, and viruses—that cause infections.
Antibody: Antibodies are proteins and are the part of the complex immune system that attacks any substance—protein or microbe—that is foreign to the body. Certain cells called B lymphocytes recognize these substances as foreign and manufacture antibodies that inactivate or eliminate the foreign substance. The foreign substance that the antibodies attack is called an antigen (see below). For most antigens, the B lymphocytes take one or two weeks to produce antibodies; for HIV, however, the time required may be months. Antibodies are the means by which vaccines work.
Antigen: Antigens are foreign material, including microbes or vaccines, that the immune system responds to by manufacturing antibodies.
Antiretroviral: HIV is a retrovirus, and drugs that inhibit it are antiretroviral drugs. These drugs come in four classes: two reverse transcriptase inhibitors (nucleosides and nonnucleosides), protease inhibitors, and entry inhibitors. Examples of nucleoside reverse transcriptase inhibitors are AZT, ddI, ddC, d4T, 3TC, TDF, FTC, and ABC.
Examples of nonnucleoside reverse transcriptase inhibitors are efavirenz and nevirapine. Examples of protease inhibitors are saquinavir, ritonavir, nelfinavir, indinavir, fosamprenavir, lopinavir, atazanavir, and tipranavir. The entry inhibitors include enfuvirtide and several others still in development. See table 4 in chapter 3.Aphthous ulcer: Aphthous ulcers are ulcers or sores in the mouth and occasionally in the esophagus. They are often extremely painful, they have no clear cause, and they are often cleared up by corticosteroids (see below) or other medications.
ARC: ARC stands for AIDS-related complex. ARC is a collection of conditions associated with HIV infection that do not meet the diagnostic definition of AIDS. There is no official definition of ARC, and most people in the field no longer use the term.
Aspergillus: A fungus found in nature that occasionally causes a chronic infection of the lungs in late symptomatic HIV infection. Treatment is amphotericin B or itraconazole.
Asymptomatic: Asymptomatic means the absence of symptoms. The asymptomatic person feels healthy.
Atazanavir (ATV, Reyataz): A protease inhibitor, or PI, that may or may not be taken with ritonavir to boost its levels in the body. Atazanavir is highly active against HIV but, like all HIV drugs, needs to be combined with at least two other drugs. One of its special advantages is that, unlike other PIs, it doesn’t increase levels of blood lipids like cholesterol. Another of its advantages is that it can be taken once daily. Its disadvantages are that it needs to be taken with food and that it needs stomach acid. So always take it with a meal and never take it with drugs—like prilosec, omeprazole, Maalox, Pepto- Bismol—that neutralize stomach acid.
Atovaquone (Mepron): A drug to prevent or treat pneumocystis pneumonia. The drug is a liquid with a bad taste. It is taken twice daily and must be taken with food.
B lymphocytes: B lymphocytes are the white blood cells—called lymphocytes—responsible for producing antibodies. B lymphocytes are distinct from T lymphocytes (including CD4 cells, also called T4 cells), which are also part of the immune system, but which work against a different group of microbes using different mechanisms.
Baclofen: Baclofen is a drug used to control muscle spasms. The most common side effect is drowsiness and, in large doses, severe sedation, lack of coordination, and lowered functioning of the heart and lungs.
Bactrim: See Trimethoprim-Sulfamethoxazole.
Barbiturates: Barbiturates are drugs commonly used to treat insomnia, anxiety, and seizures. Examples of barbiturates are amobarbital (or Amytal), pentobarbital (or Nembutal), phenobarbital, and secobarbital. All barbiturates affect the central nervous system: low doses cause mild sedation, and high doses can lead to deep coma. When barbiturates are used for sedation, they remain effective for only about two weeks. As a result, alternative drugs are generally preferred to treat insomnia. Barbiturates’ most important role may be for controlling anxiety.
The major side effects are symptoms of central nervous system depression, including drowsiness, depression, lethargy, and hangovers. People who take barbiturates should be aware that the drug may impair their ability to perform hazardous activities. Prolonged use of high doses of the drug can cause physical dependence, psychological dependence, and tolerance (that is, higher doses of the drug are required to produce a similar effect). Discontinuing barbiturates can cause withdrawal symptoms that are similar to the withdrawal symptoms an alcoholic has when abruptly discontinuing alcohol. Other side effects include stomach pain, allergic reactions, and fever.
Benzodiazepines: Benzodiazepines are a class of drugs commonly used to treat anxiety, insomnia, seizures, and painful muscles. Examples of benzodiazepines include alprazolam (or Xanax), diazepam, flurazepam hydrochloride (or Dalmane), lorazepam (or Ativan), midazolam maleate, oxazepam (or Serax), prazepam (or Centrax), temazepam (or Restoril), and triazolam (or Halcion). In general, all benzodiazepines act in similar ways and seem to be equally effective.
Most physicians prefer benzodiazepines for treating anxiety and tension. Compared to barbiturates and meprobamate, and when given at the doses that relieve anxiety, they are less addictive and produce less sedation. The major side effects are drowsiness, loss of coordination, confusion, dizziness, hangover, and fainting. People taking benzodiazepines should be aware that the drug may impair their ability to perform activities that require mental alertness and physical coordination. Using alcohol and other mind-altering drugs will make these symptoms worse. Benzodiazepines can also cause physical dependence and symptoms of severe withdrawal if the drug is stopped suddenly after being used regularly for a long time. If taken in high doses for long periods, it should be withdrawn slowly under a physician’s guidance.
Biopsy: Biopsy is a procedure for obtaining a piece of tissue for examination under the microscope. The microscopic changes in tissue often provide a diagnosis, and stains and cultures for microbes will often reveal the infecting organism. The biopsy may be obtained using lidocaine to deaden the skin to avoid pain. The biopsy may be performed on an outpatient basis when the area to be biopsied is near the surface or when it is in the lungs or gastrointestinal tract and can be reached through an endoscope, an instrument passed through the mouth or anus. Alternatively, the biopsy of organs deep within the body may require an operating room procedure.
Bleach: Chlorine bleach is highly effective in killing HIV within minutes. It is available at most grocery stores and is commonly recommended for killing any virus or other microbe that may be in such body fluids as blood or saliva, or in stool. Bleach is usually diluted 1:10, or one part of bleach in ten parts of water. This dilution can be applied to surfaces or in the washing machine for clothes.
Blood count: Blood is composed of red blood cells (erythrocytes), which carry oxygen to all parts of the body; white blood cells (leukocytes), which help make up the immune system; and platelets (or thrombocytes), which are required for blood clotting. All three kinds of cells can be counted under a microscope. A low red blood cell count is called anemia (see above), a low white blood cell count is called leukopenia (see below), and a low platelet count is called thrombocytopenia (see below). People with HIV infection commonly have low red counts, low white counts, and low platelet counts. A blood count is a routine procedure for clinical laboratories; it is a relatively simple, inexpensive, and standard test to evaluate people with HIV infection.
Bone marrow: Bone marrow is the tissue in the central portion of many bones where blood is manufactured. Bone marrow can be withdrawn (by placing a needle in the hip bone) and analyzed to detect abnormalities in the production of red blood cells, white blood cells, or platelets. Either HIV infection or drugs can suppress the bone marrow, causing anemia, neutropenia (low white blood cell count), or thrombocytopenia (low platelet count).
Branched chain DNA (bDNA): See Quantitative virology.
Bronchoscopy: A procedure done by a lung specialist to look at and collect specimens from the lung. The procedure is done with a long tube that is passed through the nose or mouth and down the bronchus (the breathing tube), using an anesthetic on the surfaces. This is the best method for diagnosing Pneumocystis jiroveci pneumonia and other lung conditions.
Buffalo hump: The common term for a collection of fat at the base of the neck or on the upper back. The fat is part of the lipodystrophy syndrome and may be difficult to reverse. Occasionally it occurs with pain. Sometimes it is removed with surgery.
Candida: See Candidiasis.
Candidiasis: Candidiasis is an infection caused by the fungus Candida albicans. People with HIV infection commonly have candidiasis in the mouth (thrush), in the esophagus (candidal esophagitis), or in the vagina (vaginal candidiasis). Thrush occurs in about 80 percent of the people with CD4 counts less than 200. Candidal esophagitis is the most common cause of difficulty swallowing in the late stages of HIV infection. Vaginal candidiasis, or “yeast infection,” is common in women with or without HIV infection. Treatment is with topical drugs (drugs placed in contact with the infection, such as nystatin or clotrimazole) or pills such as ketoconazole, fluconazole, or itraconazole.
CD4 cells: The blood contains several kinds of white cells, each of which plays a specific role in the immune system. CD4 cells (other names are T4 cells and T-helper cells) are the cells that HIV selectively infects. The number of CD4 cells frequently indicates the stage of HIV infection. Healthy people without HIV infection usually have around 1,000 CD4 cells in every milliliter of blood; counts of 200 to 500 are considered abnormally low, but not alarming. People with AIDS usually have counts of less than 200, and this is now considered the threshold for the definition of AIDS. Most people with CD4 counts of 50 to 200 feel well, and many have no complications. Nevertheless, counts of less than 200 suggest severe weakening of the immune system.
In any one person the count varies considerably: the same laboratory performing the test on the same specimen can show counts that vary by as much as 20 percent. This means that if the true count is 500, the lab may report any value between 400 and 600. The CD4 count is also influenced by the time of day it is measured and by other medical conditions independent of HIV infection. As a result, although the CD4 count is frequently used to assess progressive disease, changes in the count are sometimes difficult to interpret, and it is advisable not to attach too much credibility to a single test. The test should be repeated if there are big changes that are not readily explained.
The CD4 count is a relatively expensive test (usually $50 to $100), but it is an important way of monitoring the state of the immune system. Most medical authorities base their recommendations of HIV treatment primarily on the CD4 cell count, and monitor the response to that treatment with the viral load and CD4 cell count together. An average person with HIV infection who is not taking treatments has a decrease in CD4 cell counts of about 50 per year. The same person with a robust response to HAART has an increase in CD4 cell count of 50 to 100 per year.
Centers for Disease Control and Prevention (CDC): The Centers for Disease Control and Prevention is a federally funded institution located in Atlanta, Georgia. It has three responsibilities: to serve as an epidemiologic and public health resource for state and local health departments; to investigate epidemics; and to keep track of contagious diseases and other diseases important to public health. The CDC has about 4,000 employees, including 800 physicians and Ph.D.’s. In the past, the CDC has been responsible for much of what we know about Lyme disease, tuberculosis, Legionnaires’ disease, Ebola, and toxic shock syndrome. More to the point, the CDC provided much of the early epidemiologic data that identified the symptoms of HIV infection, the kinds of behavior that risked infection, and how HIV was transmitted—in fact, the CDC was responsible for the name AIDS. At present, the CDC is the storehouse for all reported cases of AIDS in the United States. It provides guidelines for disease prevention and gives advice on safety for health care providers. It is responsible for funding state and local agencies that test for HIV, counsel, and collect data.
Chloral hydrate: Chloral hydrate is a sedative used to treat insomnia. It is usually taken fifteen to thirty minutes before bedtime. Using chloral hydrate regularly for more than two weeks often reduces its effectiveness. Major side effects include stomach irritation, residual sedation, or a hangover. Chloral hydrate should be used with great caution in people who are depressed, who may commit suicide, or who have a history of drug abuse.
Chlorhexidine: A mouthwash available without prescription for treating gingivitis, an inflammation of the gums.
Cholesterol: A steroid found in the blood along with its carrier protein, called a lipoprotein. The low-density lipoproteins (LDLs) carry cholesterol from the liver to body tissue. The high-density lipoproteins (HDLs) carry cholesterol to be eliminated. Heart disease is associated with high levels of LDL (“bad cholesterol”) and low levels of HDL (“good cholesterol”).
Ciprofloxacin (Cipro): An antibiotic with a broad spectrum of uses. It can be taken by mouth or intravenously.
Clarithromycin (Biaxin): An antibiotic used to treat sinusitis, Mycobacterium avium complex (MAC) infection, and other infections. It is the best drug for MAC, but must be used with other antibiotics because MAC can become resistant when treated with only one antibiotic. The major side effect is nausea and vomiting.
Clostridium difficile: People who take antibiotics often develop diarrhea as a side effect. A relatively common and sometimes severe cause of this diarrhea is a microbe called Clostridium difficile. Almost any antibiotic can cause this complication, but the most frequent causes are ampicillin, amoxicillin, clindamycin; a group of drugs called cephalosporins that includes cefixime (or Suprex), cefotaxime, ceftriaxone, cefuroxime, cephalexin (or Keflex), and cefaclor (or Ceclor); and fluoroquinolones such as ciprofloxacin (Cipro), levofloxacin (Levoquin), moxifloxacin (Avelox), and gati- floxicin (Tequin). People who have diarrhea while taking these or any other antibiotics should stop taking the antibiotics and call their physicians. A test of stool will determine if Clostridium difficile is the cause. If it is, it can be treated with metronidazole or vancomycin. Vancomycin is preferred for serious cases of diarrhea, but it costs about $50 to $100. Metronidazole is less expensive—$10 to $20—and equally effective. The authors are fond of Clostridium difficile and its connection to antibiotic-associated diarrhea because one of us (J.B.) discovered that connection.
CMV: CMV, which is short for cytomegalovirus, is a virus commonly found in people without HIV infection. Usually the immune system holds CMV in check, and it remains dormant in the body without causing any serious disease. With a severely weakened immune system, however, CMV may cause serious infection. The site of the infection can be in the eye, lung, liver, gastrointestinal tract, bone marrow, brain, or widespread in many of these areas. The virus can be detected by examining tissue and culturing the virus. CMV retinitis, a vision-threatening infection of the eye, was initially a common HIV-associated complication but has now become relatively rare in this era of HAART. Treatment of CMV retinitis and other forms of CMV infection is with valganciclovir, ganciclovir, foscarnet, or cido- fovir. The most important treatment, however, is HAART: the immune system, if it is reconstituted, will control CMV itself.
Colon: The gastrointestinal tract—which starts at the mouth and ends at the rectum—includes the esophagus, stomach, small intestine, colon, and rectum. The colon and the small intestine are commonly the sites of infections that cause diarrhea. To diagnose problems in the colon, common procedures are colonoscopy and sigmoidoscopy. These procedures permit visualization and biopsy of the colon by passing a tube through the rectum. Colonoscopy is expensive ($1,200 to $1,800) and is usually done by a specialist called a gastroenterologist.
Combination treatment: Combination treatment means taking two or more drugs against HIV. The goals of combination treatment are to “gang up” on HIV with a double whammy attack; and to prevent resistance, since a microbe can develop resistance most easily to one drug at a time. The downside to combination treatment is that it may be more toxic, and microbes may develop resistance to both drugs and leave fewer options for treatment. All HIV treatment is now combination treatment, usually using three or four different drugs.
Combivir (AZT + 3TC): One of the combinations of nucleoside analogs (see below) that are taken as one pill twice daily. The advantage is the reduction in “pill burden,” which makes adhering to the drug regimen easier.
Community-based organizations (CBOs): Community-based organizations are also called AIDS-advocacy organizations and AIDS service organizations (ASOs). They are organizations and agencies that provide services to people with HIV infection, as well as education and prevention programs for the whole community. The leaders of community-based organizations are lay people, ordinary people who do not come from the government or from organized medi- cine—although many community-based organizations have physicians as advisers, and most receive public funds.
Examples of community-based organizations dealing with other diseases are the American Lung Association, the American Heart Association, and the American Cancer Society. There is no similar nationwide organization for people with HIV infection or AIDS. Nevertheless, most cities have one or sometimes several such organizations: examples include Shanti in San Francisco, the Gay Men’s Health Clinic in New York City, and HERO in Baltimore. The types of services offered vary but may include counseling, crisis support, financial assistance, case management, a buddy system, transportation, meals, housing, support groups, legal aid, social services, education, psychological support, hotlines, buyers’ clubs, and medical services (see Appendix A, “Resources”). Most of these organizations have a paid professional staff but rely heavily on volunteers. Funding usually comes from state governments, corporations, foundations, and local fund-raising events.
Complete blood count (CBC): An inexpensive blood test to measure the numbers of white blood cells, red blood cells, and platelets.
Computerized tomography scan (CT scan): CT scans are a particular kind of X-ray that provide a three-dimensional view of the body. Conventional X-ray tests provide a two-dimensional view of the body; CT scans use computers to stack a series of two-dimensional X-rays together to form a three-dimensional image of the body. CT scans can be done of the entire body or of parts of it. The person receiving a CT scan often receives an injection of what is called contrast material—material that shows up under X-rays. Some people have allergic reactions to contrast materials and should not receive them again. The person receiving the CT scan is next put into a chamber with a scanner that circulates around the body, producing three-dimensional images in parallel sections of about an inch or less. CT scans, first developed in the 1970s, are an excellent method for detecting tumors, infections, or other changes in the anatomy of the brain, chest, abdomen, or other parts of the body. They are also expensive, usually costing around $300 to $800.
Constitutional symptoms: Symptoms caused by the impact of an illness on the entire body or constitution are frequently referred to as constitutional symptoms. Included are fatigue, achiness, weight loss, fever, and night sweats. Constitutional symptoms are present in many types of infectious diseases, tumors, and other medical conditions ranging from the serious to the trivial. For people with HIV infection, constitutional symptoms may be a result of HIV infection itself or the result of such complications as pneumocystis pneumonia, tuberculosis, or widespread CMV infection.
Contagious: A disease that is contagious can be passed from one person to another. A disease that is infectious is caused by a microbe. All diseases that are contagious are also infectious; but some diseases, like toxic shock syndrome, are infectious and not contagious. HIV is both infectious and contagious, but is contagious only with specific types of contact.
Corticosteroids (also known as steroids, glucocorticosteroids, prednisone, and cortisone): Corticosteroids are drugs used to reduce the immune response. Numerous preparations are available that can be taken intravenously, by mouth, or in an ointment applied to the skin. Using high doses of corticosteroids for a long time can be dangerous: they reduce the immune system’s defenses against certain infections. Corticosteroids are sometimes considered especially dangerous for people with HIV infection, whose immune defenses are already weakened. Nevertheless, many of the complications of HIV infection appear to result from an overly abundant but misdirected immune response. As a result, these complications of HIV infection respond well to corticosteroids, though the drug should be taken at the lowest doses for the shortest period.
Crixivan: See Indinavir.
Cryptococcosis: Cryptococcosis is an infection caused by the fungus Cryptococcus neoformans. This fungus can cause infection in otherwise healthy people. In people with HIV infection, however, it is especially severe, frequently causing meningitis. Common symptoms include headaches, fevers, vision problems, and seizures. The diagnosis is usually made by analyzing blood and cerebrospinal fluid obtained with a spinal tap (see below). The disease is treated with amphotericin B given by vein or fluconazole given by mouth; when treatment is stopped, the disease tends to recur so that long-term treatment is generally necessary.
Cryptosporidiosis: Cryptosporidia are parasites that infect the intestine and cause diarrhea. This infection, called cryptosporidiosis, can occur in otherwise healthy persons, but the diarrhea generally does not last long and is not severe. Cryptosporidiosis in people with HIV infection often causes devastating diarrhea that persists for months. People with cryptosporidiosis may lose large amounts of fluid and nutrients and, consequently, become severely malnourished. The diagnosis is usually established by simply examining the stool under a microscope to detect the parasite. There is no universally accepted form of treatment except to replace the lost fluids and nutrients. The best treatment is to recover the immune system with HIV treatments; the immune system then controls Cryptosporidium and may eliminate it.
Culture: A culture, in medical terms, is a medium in which microbes can grow. Most cultures in medicine are done to detect bacteria like strep and staph. Cultures have been done for over 100 years. A culture usually takes 24 to 48 hours, the methods are standard, and the cost is low. Viruses like HIV, however, are much more difficult to grow in culture and most labs don’t offer this service. When necessary, specialized or research labs can get HIV to grow using cultures containing lymphocytes. The blood test to detect HIV antibody is a better, simpler, faster, and cheaper method of detecting HIV.
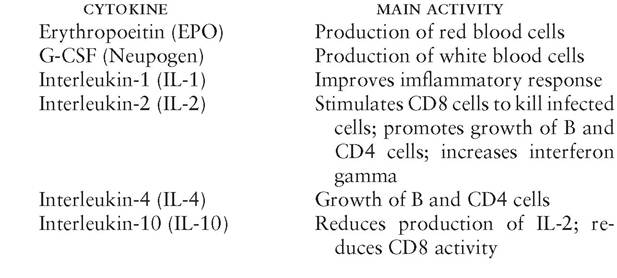
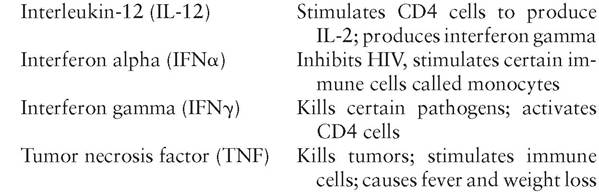
Cytokines: Cytokines are proteins secreted by cells of the immune system. They are the means by which these cells communicate with other cells of the immune system. They may stimulate (up-regulate) or suppress (down-regulate) various immune responses. For instance, a cytokine called IL-2 activates CD8 cells to attack infections. Most cytokines have multiple activities. For instance, IL-2 also up-regulates another cytokine called interferon gamma, and down-regulates still other cytokines called IL-10 and IL-4. Some of the activities are beneficial, some possibly harmful. Many cytokines can be produced in the laboratory and can be given as therapeutic agents. All must be injected because the digestive enzymes in the small intestine break them down. There are at least twenty-six cytokines known so far and probably a lot more to be discovered. Some of the main cytokines are the following:
Cytomegalovirus: See CMV.
d4T (stavudine, Zerit): A popular nucleoside analog (see below) that has few short-term side effects. Long-term side effects, however, include peripheral neuropathy (see below, Neuropathy), pancreatitis (inflammation of the pancreas with severe abdominal pain), lactic acidosis (see below), increased triglycerides, and the sunken-face look.
ddC (zalcitabine, HIVID): A nucleoside (see below) that seems to be relatively weak and toxic. Many physicians have stopped using it except in situations where no alternatives are available.
ddI (didanosine, Videx): A nucleoside (see below) that must be taken on an empty stomach. In many people, it causes stomach problems. Long-term use may cause pancreatitis (inflammation of the pancreas with severe abdominal pain), peripheral neuropathy (see below, Neuropathy), and lactic acidosis (see below).
Delavirdine (Rescriptor): An infrequently used NNRTI (see below)— infrequent because it is not very strong and must be taken 3 times daily.
Dementia: See HIV-associated dementia.
Diabetes: A common, sometimes inherited condition that is characterized by abnormal control of blood glucose, or sugar. Diabetes is relevant to people with HIV infection because protease inhibitors may cause it. The standard methods of controlling diabetes are diet, exercise, and weight loss. When these aren’t enough, diabetes needs to be controlled with pills called oral hypoglycemics; and when pills aren’t enough, you need injections of insulin.
Diarrhea: Loose and/or frequent stools that are a common medical condition in all people, but may be particularly common in people in advanced stages of HIV infection with CD4 counts below 200. It is important to tell your physician when the diarrhea is severe, persistent, or accompanied by weight loss, fever, or cramps. The cause may be side effects of medications, food poisoning, anxiety, gastroenteritis, or some complication of HIV infection.
Dormant: See Latency.
Drug interactions: A drug interaction is the effect one drug has on another. Drug A might interfere with absorption of drug B, so that the levels of drug B in the body are lower than they ought to be. Or drug A might slow the body’s metabolism of drug B, so that drug B lasts longer at higher concentrations and causes toxicity. Drug interactions are a big issue with most protease inhibitors. Make sure your doctor knows all the drugs you are taking.
Dysphagia: Dysphagia means difficulty with swallowing. The most common cause of dysphagia is an infection by Candida albicans, a fungus that can be easily treated (see Candidiasis). Less frequent causes are infections with herpes or CMV. In some people dysphagia has no readily apparent cause. For people with HIV infection and CD4 counts above 200, dysphagia is caused by the same things that cause it in people without HIV infection—the most common being gas- tro-esophagus reflux disease or GERD, treated with drugs to reduce stomach acid. The usual method of finding the cause of dysphagia is endoscopy, a procedure in which a tube is placed in the esophagus to visualize and biopsy the lesions. X-ray examinations are another means of viewing the esophagus. In many cases, neither of these tests is done, and the person is presumed to have a Candida infection if he or she also has thrush (see below) and if swallowing is painful.
Efavirenz (Sustiva): This is a nonnucleoside reverse transcriptase inhibitor that is highly effective against HIV when combined with two nucleosides. The main side effect is that it plays tricks on the brain, causing confusion, bad dreams, and a feeling of being disconnected. These side effects usually disappear after 2 to 3 weeks, but people must be aware of them and their effect on jobs, driving, etc. The drug is taken once daily, usually at sleep time so the person is not aware of the side effects when they are most severe. This drug, when taken in the first trimester of pregnancy, might cause birth defects. It should not be taken by pregnant women or women who may become pregnant. It is the only drug for HIV infection that clearly causes birth defects.
ELISA test: The ELISA (pronounced eelissa) is a blood test done to detect antibodies to certain microbes, among which is HIV. The ELISA is the first of two standard tests done together to detect antibodies to HIV. The test is extremely sensitive but not very specific. Sensitivity means that the test is able to detect HIV infection; specificity means that the test specifically detects a particular infection and no other. In other words, with ELISA, people who have HIV infection will rarely have a falsely negative test, but people who do not have HIV infection will commonly have a falsely positive test. As a result, the ELISA is used as a screening test, and those who are positive have a second test on the same blood sample called a Western blot.
The Western blot test, combined with an ELISA, is over 99.9 percent accurate in both sensitivity and specificity. The combination of tests is generally offered free of charge by most health departments and at a cost of $50 to $150 by commercial laboratories. The test offered may be anonymous, meaning that the person receiving the test cannot be identified, or confidential, meaning that privacy is honored but a record is kept identifying a specific person with the test result. The ELISA is easily performed, but the Western blot is more complicated and often done only by reference laboratories or on certain days of the week. For this reason, the results may not be available for several days. The test results are usually either positive or negative, but occasionally people have Western blots that cannot be clearly interpreted and the test results are considered indeterminate. The usual recommendation for people with indeterminate results is to have the test repeated in two or three months. People at a low risk for HIV and with indeterminate results almost never have HIV infection, and the cause of the indeterminate results is not known.
Emtricitabine (FTC, Emtriva): A nucleoside analog very similar to lamivudine. See Lamivudine.
Emtriva: See Emtricitabine.
Encephalitis: Encephalitis is an infection of the brain. (Meningitis, by contrast, is an infection of the meninges, the membrane surrounding the brain and spinal cord—see Meningitis.) Encephalitis commonly causes headaches, fever, seizures, and neurologic problems. The diagnosis is frequently made on the basis of the person’s symptoms, combined with procedures to examine the brain such as computerized tomography scan (CT scan) (see above); magnetic resonance imaging (MRI) (see below); or electroencephalogram (EEG). Diagnosis can also be made by analyzing the cerebrospinal fluid obtained by a spinal tap (see below). In people with HIV infection, the usual causes of encephalitis are infection with HIV itself or such complications as CMV or toxoplasmosis.
Endoscopy: Endoscopy is a diagnostic procedure in which an instrument is passed through the mouth or rectum to examine an internal organ or to obtain a biopsy (see above). In people with HIV infection, the most common types of endoscopy are bronchoscopy (see above) to examine the lungs and endoscopies to examine the digestive system. Upper endoscopy of the intestine involves passing an endoscope through the mouth to examine the esophagus, stomach, or upper small intestine. Lower endoscopy of the intestine involves passing an endoscope through the rectum to examine the large intestine or colon. Endoscopes are flexible and can turn corners. Endoscopy requires the expertise of a specialist, can be done on an outpatient basis, and usually costs $1,200 to $1,800, except in New York City, where everything costs more.
Enfuvirtide (T20, Fuzeon): A drug that works against HIV by preventing it from attaching to and entering the CD4 cell. It is the first of a whole class of drugs that will work this way. It is used only when the standard drugs for HIV no longer work, usually because of resistance. It needs to be injected twice daily; the injections cause a predictable reaction with painful or itchy bumps. Most people learn to do their own injections with proper training. Adherence to this drug is actually better than to the drugs that are swallowed. But taking this drug also requires commitment. It must be taken with another drug or drugs against HIV; it can’t succeed alone. It is also expensive—over $20,000 per year.
Enteritis: Enteritis is an inflammation of the small intestine; the most common symptom is diarrhea. In people with advanced HIV infection and CD4 counts of less than 200 and usually less than 50, the microbes that usually cause enteritis are Cryptosporidium, Microsporidium, Mycobacterium avium complex, and CMV. These microbes can be detected by examining stools under a microscope or with a biopsy of the small intestine done with an endoscope (see above, Endoscopy), a tube that is placed through the mouth and into the small intestine. Diarrhea in people with HIV infection and a CD4 count over 200 will often be due to medications, gastroenteritis (a self-limiting viral infection), anxiety, or food poisoning.
Epidemic: An epidemic is a disease that occurs in many more people than would be expected during a given time. Epidemiology is the study of the factors that determine the frequency and distribution of diseases.
Epivir: See Lamivudine.
Epzicom: A combination pill containing abacavir and lamivudine.
Erythropoeitin (EPO): A cytokine made in the body that stimulates production of red blood cells. EPO has been synthesized and can be taken as a drug. It has to be injected, it is expensive, and it has almost no side effects.
Esophagitis: Inflammation of a portion of the esophagus (the swallowing tube), which runs from the throat to the stomach. Common causes are Candida albicans, herpes simplex, CMV, and aphthous ulcers.
FDA: See Food and Drug Administration.
Fluconazole (or Diflucan): Fluconazole is used to treat fungal infections, primarily those caused by Candida albicans (thrush or candidal esophagitis) and Cryptococcus neoformans (cryptococcal meningitis). Fluconazole can be taken by mouth or by vein. Side effects are unusual; occasional problems are nausea, rash, or hepatitis.
Food and Drug Administration (FDA): The U.S. Food and Drug Administration, located in Rockville, Maryland, is the federal agency responsible for assuring that drugs (like penicillin and AZT), vaccines (like tetanus toxoid and the chickenpox vaccine), and devices (like artificial heart valves) are both safe and effective. Drugs cannot be sold in the United States unless the FDA has approved them. Approval is based on the drug’s success or failure in clinical trials, which evaluate the drug’s toxicity and effectiveness for a particular condition. The FDA also decides whether the drug can be sold over the counter (like aspirin), whether it requires a prescription from a physician (like all antibiotics), or whether it should be a controlled substance requiring a narcotic license (like morphine). In short, the FDA has broad regulatory powers. Some consider the FDA to be a bureaucratic nightmare—slow, demanding, and unresponsive to such critical needs as new drugs for HIV infection. Others consider that the FDA’s awesome responsibility justifies its tedious but painstaking approval process. The FDA has always given a high priority to drugs for HIV, granting these drugs what is called an “expedited review.” With expedited reviews, the requirements for approval are less stringent and after the studies are done, the review process is completed in a short time, often two to four months. The good news is that we get access to the drugs fast; the bad news is that we know less about them.
Fosamprenavir (FPV, Lexiva): A protease inhibitor that is usually boosted with ritonavir. Possible advantages compared to other PIs are that it can be taken once daily (though many take it twice daily), it can be taken with or without food, and it may have less effect on blood cholesterol than other PIs.
Ganciclovir (Cytovene): Ganciclovir is used to treat infections caused by cytomegalovirus and occasionally for infections caused by herpes simplex and other viruses. It is given intravenously. The most important side effect is a low blood count, especially neutropenia, which predisposes the person to bacterial infections (see Blood count, and neutropenia, under Leukopenia). If neutropenia is severe enough, the dose of the drug should be reduced, or the drug should be temporarily stopped. The drug is expensive.
G-CSF (Neupogen): A cytokine made in the body that stimulates the bone marrow to make white blood cells that fight infections. The drug must be taken by injection. Side effects are nil. The price is high.
Generic names: Most drugs have two names: a drug name and a trade name. For instance, atazanavir is the same as Reyataz: the first is the drug name, the second is the trade name from one drug company. Trade names are usually capitalized; generic drug names are not. When new drugs are discovered, they are patented, meaning that no one else can make them. So the company that made the discovery or owns the patent can charge whatever it can get. This arrangement can actually be good, because it keeps the pharmaceutical industry interested in discovering new drugs; it is the reason we now have more than twenty drugs for HIV. After seventeen years, patents run out and the drugs become generic. That’s good too, because the drugs can then be manufactured by anyone and the price drops, sometimes to a small fraction of the original price. This decrease in price happened with ddI and AZT. The generic drugs must satisfy production requirements in order to be sold, providing assurance that the generic drug is as safe and as potent as the patented drug. We emphasize this point because some people think that generics are lesser drugs; they aren’t. You should have no reservation about using them, providing they are licensed for sale in North America, Europe, or Australia. Many health insurance companies and managed care organizations or HMOs require that generic drugs be used when available. Physicians and medical journals tend to refer to drugs by generic names; patients tend to refer to them by trade names.
Gynecomastia: The medical term for breast enlargement in men that, in people with HIV infection, results from the redistribution of fat that is a side effect of long-term use of protease inhibitors. The enlargement may be generalized or nodular, and may be painful. Standard treatment when it is painful or cosmetically unpleasing is surgical reduction.
HAART (highly active antiretroviral therapy): HAART refers to the complex medical regimens of therapies directed against HIV that are likely to stop its replication and mutation. The goal of HAART is no progression of disease and no resistance to the virus. The progress in HIV therapy in the late 1990s is ascribed to the widespread use of HAART. The progress includes decreases in mortality, in the number of people with AIDS, in hospitalizations, in HIV- associated complications. HAART is also implicated in some of the newly recognized side effects, like lipodystrophy (see below).
HAD: See HIV-associated dementia.
Hemophilia: A person with hemophilia lacks a protein that helps the blood to clot. People with hemophilia bleed easily, even with a trivial cut; many have severe hemorrhaging into the joints and eventually get joint disease. Hemophilia is inherited, and only by men; the gene for hemophilia is carried by women, who do not get the disease but who can pass the gene on to their sons. Hemophilia has two forms, hemophilia A and hemophilia B; each form lacks a different clotting protein, called a clotting factor. Hemophilia is treated by substituting a commercial clotting factor for the clotting factor the blood lacks. The commercial clotting factor is extracted chemically from blood donated by hundreds or thousands of people. As a result, people with hemophilia are exposed to the blood of thousands of donors. Between 1978 and 1985, from the time HIV was introduced into the United States until the time the blood banks screened for HIV, people with hemophilia had a high risk of being infected with HIV. Approximately 70 percent of men with hemophilia A and 30 percent of men with hemophilia B acquired HIV infection from infected commercial clotting factors.
Since 1985, the risk of being exposed to HIV through clotting factors has dropped to practically nil. One reason is that donated blood is now screened for HIV; another reason is that clotting factors are heated and purified by detergents and biochemicals that kill HIV.
Hepatitis: Hepatitis is an inflammation of the liver. Many people have no symptoms and are unaware of having hepatitis. The symptoms, when people do have them, are loss of appetite, vomiting, yellow discoloration of the skin and eyes (jaundice), dark urine, sore stomach, and fever. Hepatitis is usually caused by viruses that are named alphabetically in their order of discovery, that is, hepatitis A through hepatitis E. Most important are hepatitis A, B, and C. Hepatitis A is caused by food poisoning; though it may be severe, it is always temporary. Hepatitis B and C are common in the general population, but more common in people with HIV infection. The reason is that HIV, hepatitis B, and hepatitis C are all transmitted by the same mechanisms: sex and blood. Both hepatitis B and C may cause persistent infection that lasts years or decades, cause chronic hepatitis, and may cause cirrhosis. The diagnosis of hepatitis is easily made with blood tests to determine liver function and to detect specific microbes, including hepatitis B, hepatitis C, and hepatitis A viruses. When the cause is unclear, it is sometimes helpful to obtain a biopsy of the liver.
For people with HIV infection who are also trying to manage chronic infections with the hepatitis B virus or the hepatitis C virus (two simultaneous infections referred to as coinfections), the following facts are important:
• All people with HIV and chronic liver infection need to avoid excessive alcohol, get vaccinated for hepatitis A, and avoid the drugs that are likely to injure the liver. If they haven’t had hepatitis B, they need the vaccine to prevent it.
• All HIV drugs can cause liver disease; some are more likely to do so than others. Many HIV drugs are most likely to cause liver disease when the liver is already injured by chronic infection with, say, the hepatitis B or hepatitis C virus. We can’t avoid the HIV drugs, but we can watch the liver closely by getting liver tests frequently and changing the drugs when necessary.
• Hepatitis B and hepatitis C are now treatable. The treatment for hepatitis C is a weekly injection with interferon (peg-interferon), which has substantial side effects; treatment usually continues for one year. Hepatitis C can actually be cured, but the rate of cure with an HIV coinfection is substantially lower. The treatment for hepatitis B will not cure it but will reduce its progression. Of the five drugs used for hepatitis B infection, three are also used for HIV. Coinfection with HIV and both forms of hepatitis makes treatment complicated. One reason is that the drugs used for HIV commonly cause liver disease. So before you can be treated for liver disease, your doctor must figure out whether the cause is hepatitis or the HIV drugs. Decisions about how to use these drugs with coinfection are tricky and best made by experts.
Hepatitis B virus: The hepatitis B virus is one of the microbes that causes hepatitis. Hepatitis B infection may be acute and cause serious symptoms that last up to a few weeks (see above, Hepatitis); it may be chronic with occasional symptoms and abnormal liver tests that last for months or years; or it may cause no symptoms at all and may only show up on a blood test. The tests for the hepatitis B virus are a little complicated:
1. The test might show that you have antibodies to the virus, which means either that you have been infected (but usually don’t know it) or that you have already responded to the vaccine. In this case, you don’t need the vaccine and you don’t need to worry about hepatitis B.
2. The test might be negative, which means you have not been exposed to the hepatitis B virus. Most people with this test result and with HIV infection should get vaccinated.
3. The test might show that you have chronic infection with hepatitis B virus. This means you need to be evaluated for treatment for the virus.
About 5 to 10 percent of people with hepatitis B infection become chronic carriers of hepatitis B virus; they continue to carry the virus and can transmit it to others for years. People who are persistent carriers of hepatitis B virus may develop chronic hepatitis that over many years could eventually lead to cirrhosis or in rare cases, liver cancer. The frequency of chronic hepatitis B carriers is higher among people with HIV infection. The hepatitis B virus is transmitted the same way HIV is, by sexual contact or blood-to-blood transmission. The blood supply used for transfusions is screened for the hepatitis B virus and is therefore an unlikely source of this infection.
There is little evidence that chronic hepatitis B infection is worse in people with HIV infection than in people without HIV infection. In addition, the presence of liver damage or ongoing inflammation may complicate the use of certain drugs that require the liver for metabolism or that may occasionally cause further liver damage (see Hepatitis, above). Once infection takes place, treatment with interferon, lamivudine (3TC), adofovir, entecavir, or tenofovir can slow the hepatitis B virus, but the results are variable. Interferon has harsh side effects and the virus usually becomes resistant to lamivu- dine. It’s better to prevent the infection with a vaccine. The vaccine is recommended for the people at risk for this infection: people who share needles to inject drugs, people who practice unsafe sex with gay men, family members who live in the same household, sex partners of people known to be hepatitis B carriers, and health care workers. Three injections are required, at a cost of about $150 to $200 for all three doses.
Hepatitis C virus: The hepatitis C virus, like hepatitis B, causes hepatitis. Hepatitis C is transmitted by blood, and far less frequently by sexual contact. The diagnosis is made by a blood test and sometimes by a biopsy of the liver. Unlike hepatitis B, hepatitis C cannot be prevented by vaccine. Most injection drug users and people with hemophilia have hepatitis C. Hepatitis C is quite different from hepatitis B in several ways: about 85 percent of the people with hepatitis C get chronic infection, meaning they carry this virus forever. Of the chronic carriers, about 20 percent develop cirrhosis over a period of 20 years, and about 4 to 10 percent die of liver failure or get a liver transplant. These odds are made much worse by alcohol abuse and by concurrent HIV infection. In fact, now that the prognosis with HIV infection is so much better, many people with both HIV and hepatitis C usually live long enough to get serious liver disease from hepatitis C. Hepatitis C can be treated with interferon and ribivirin. The treatment has many side effects, but about 30 to 50 percent of the people who get through the full 6- to 12-month course are cured of hepatitis C.
Herpes simplex virus: Herpes simplex is a virus that commonly causes infections of the mouth (“fever blisters” or “cold sores”) and genitals (“genital herpes”). There are actually two different viruses: though similar in many respects, one kind (called herpes simplex no. 1) is most likely to infect the mouth and the other (called herpes simplex no. 2), the genitals. The symptoms of both infections are blisters on the mouth or genital area that first contain clear fluid, then become filled with pus, finally form scabs, and eventually disappear. Herpes simplex is a persistent virus: the virus remains dormant most of the time and then causes recurrent symptoms intermittently over a period of years. The initial infection with herpes simplex virus is often severe with large areas of blisters, occasional fevers, and pain and tingling in the area involved. Subsequent attacks are usually milder. The virus is transmitted to others by contact with the mouth or genitals, especially when the blisters are present.
Both the oral and the genital form of herpes are common infections in the general population; in people with advanced HIV infection, however, the blisters are more common, more severe, less likely to respond to standard therapy, more widespread over relatively larger areas, and persist for longer periods of time. Treatment with drugs like acyclovir, famciclovir, or valacyclovir makes the lesions heal faster, especially if taken early in the course of the infection. These drugs can also be taken continuously to prevent outbreaks. In addition, treatment reduces the risk of transmitting the virus to others. In people with HIV infection who have severe herpes infections, acyclovir may be given intravenously; once the infection is under control, the tablets are often given for extended periods to prevent recurrences.
Herpes zoster: Herpes zoster is caused by the same virus that causes chickenpox. The virus persists in the body and may cause symptoms decades after the original infection. Attacks after the first infection are called shingles, or herpes zoster. The skin sores with herpes zoster are similar to those of chickenpox and those of herpes simplex. With herpes simplex, the sores are on both sides of the body and usually on the genitals or mouth. With chickenpox, the sores are all over the body and don’t hurt; with shingles, a crop of sores forms on one side of the body and hurts. The sores begin as red spots that become blisters filled with water; the blisters break down into sores with pus, finally scab over, and eventually disappear. Unlike herpes simplex infections or chickenpox, however, the later recurrences of herpes zoster are usually restricted to the area served by a single nerve. In other words, the blisters are restricted to one side of the body, usually in a band across the face, chest, abdomen, back, or leg.
In older people, herpes zoster is followed by post-herpetic neuralgia, a pain at the site of blisters that may persist for months after the blisters are gone. Post-herpetic neuralgia is fortunately infrequent among people with HIV infection. Herpes zoster is more common and more severe in people with HIV infection. It does not, however, necessarily mean that the immune system is weakening, and it clearly does not indicate AIDS. The diagnosis is generally made with a microscopic examination and culture of blisters, but the appearance of the blisters is usually all a physician needs to make a diagnosis. Acyclovir, famciclovir, or valacyclovir can hasten healing and reduce the most common complication of herpes zoster—severe pain.
Hickman catheter: People who require long courses of drugs given by vein will often have a tubing called a Hickman catheter. The catheter is inserted by a specialist, usually a surgeon, through the skin of the chest, and then tunneled under the skin to a vein in the chest. The end of the catheter comes out the chest wall above the breast. Drugs can be injected into the catheter as necessary. The advantage of a Hickman catheter is that it permits access to the vein without repeated needlesticks in the arms. Other devices are also available, including a type that is placed below the skin so that no tube comes out the chest wall.
It is important to know that the area around any catheter in a vein can become infected. Symptoms of infection of the area where the catheter is located are redness and pain, and sometimes pus. Symptoms of infection around the catheter inside the body are fever and chills; in most cases, the infection is inside the body and the skin around the catheter appears normal or feels slightly tender. Anyone with a Hickman catheter and these symptoms should tell a physician right away. Antibiotics should be given immediately, and sometimes the catheter needs to be removed.
Histoplasmosis: A fungus that is highly prevalent in the Ohio and Mississippi River valleys and is also found in other central, southwestern, and mid-Atlantic states. People with HIV infection are susceptible to it. The infection is often disseminated, that is, widely distributed all over the body. The disseminated form of histoplasmosis occurs in late-stage HIV infection when the CD4 count is under 100. Common symptoms are fever and weight loss. Treatment is with amphotericin B by vein and/or itraconazole by mouth.
HIV: HIV stands for the human immunodeficiency virus. HIV causes AIDS. There are occasional arguments that perhaps HIV does not cause AIDS, but at present, the great majority of scientific authorities accept HIV as the sole cause of AIDS. Several studies show that HIV reproduces rapidly and destroys CD4 cells, suggesting that the entire course of infection is similar to that of most other viral infections. HIV’s uniqueness is that it takes a long time to make the person sick and that it attacks an unusual part of the body, the immune system.
HIV-associated dementia (HAD): HIV-associated dementia is the dementia that appears to result from HIV infecting the brain. Dementia means the loss of intellectual abilities, including the loss of memory, judgment, and concentration. HAD occurs in 20 to 30 percent of people with HIV infection, but usually only in the late stages.
Immune reconstitution: The term used to describe the return of the immune system when HAART (see above, HAART) controls HIV. Immune reconstitution is monitored by the CD4 cell count (see above, CD4 cells). Early studies questioned the competence of the CD4 cells that came back after HAART, but we now know that they work well. Even people with severe immune suppression and CD4 counts near 0 can have complete or near-complete recoveries. This means that people who took PCP prophylaxis for years can stop taking it when the CD4 count is above 250 for 3 months.
Immune reconstitution syndrome: In this syndrome, the immune system overresponds, usually to some opportunistic infection that is being treated at the same time HIV is being treated. When HIV is controlled, the immune system comes back and attacks the opportunistic infection with such vigor that the immune response itself causes symptoms. In most cases, the syndrome is managed by continuing to treat HIV, continuing to treat the opportunistic infection, and taking medication like cortisone to quiet the immune reaction.
Immune system: The human body is defended against a multitude of microbes by a complex system called the immune system. The principal components of the immune system are cells called B lymphocytes, neutrophils, and T lymphocytes. B lymphocytes make antibodies, the proteins that attack bacteria and viruses; neutrophils envelop and kill bacteria; and T lymphocytes provide communication between the parts of the immune system. Although these three components are somewhat interdependent, each takes primary responsibility for defense against certain types of microbes. For this reason, people deficient in different components are prone to infections with quite different microbes.
The cell type that is primarily affected in people with HIV infection is a type of T lymphocyte called a CD4 cell (see above). The most common infections encountered in people with few CD4 cells are caused by Pneumocystis jiroveci, cytomegalovirus, Mycobacterium avium complex, herpes simplex virus, herpes zoster, Candida albicans, Toxoplasma gondii, Cryptosporidium, Cryptococcus, Salmonella, and the bacterium that causes tuberculosis. People with immune systems weakened by HIV are not only subject to high rates of infections with these organisms, but the infections also tend to be severe, prolonged, recurrent, and often difficult to treat. At the same time, many other microbes that commonly cause infections in everyone do not appear to be unusually common or severe in people with HIV, presumably because the other components of the immune defenses remain relatively strong.
Incubation period: The incubation period of a disease is the time interval between infection with a microbe and the first symptoms of disease. For influenza and common colds, the incubation period is usually several days; for measles, chickenpox, mumps, and infections caused by many other viruses, the incubation period is two to three weeks. An unusual feature of HIV infection is that the first symptoms of a weakened immune system usually do not occur until several years after the infection takes place. Nevertheless, the acute HIV infection (see above) usually occurs at 2 to 4 weeks after HIV trans-
mission.
Indinavir (Crixivan): A protease inhibitor that is usually taken with ritonavir (Norvir) twice daily. Indinavir may cause kidney stones composed of indinavir; the best way to prevent this is to drink large amounts of fluids.
Infectious: See Contagious.
Influenza vaccine: The influenza vaccine varies in effectiveness, depending on whether the strain of virus in the vaccine is related to the virus that is causing the influenza. The effectiveness of the vaccine changes every year. In most years, however, the vaccine probably prevents about 70 percent of the cases of influenza, and those who become infected despite having been vaccinated usually have less severe symptoms. Influenza is not known to be unusually common or severe in people with HIV infection. The main problem specific to people with HIV infection is that the symptoms of influenza can be confused with the symptoms of pneumonias such as pneumocystis pneumonia, which are caused by other microbes (see Pneumocystis jiroveci), a confusion it would be nice to avoid. Therefore, the CDC’s Advisory Committee on Immunization Practices recommends that people with HIV infection routinely get the influenza vaccine every year.
Informed consent: Informed consent is a form of protection for people considering taking an HIV antibody test or undergoing certain medical procedures (like an operation) or considering participation in a clinical trial. Before taking the test, undergoing the procedure, or participating in the trial, the person or the person’s representative must sign an informed consent form stating that he or she has been informed about the purpose, benefits, risks, and alternatives to the test, procedure, or trial, and that he or she consents to it. In the case of participation in a clinical trial, the informed consent form explains the purpose of the trial, what will be done, the risks of participation, the benefits of participation, what other treatments are available, and the right of the participant to leave the trial at any time.
Inoculum size: Inoculum size is a term used in the field of infectious diseases to describe the number of microbes necessary to cause an infection. In HIV infection, for example, a certain number of viruses is required before infection takes place. The specific number is not known. What is known is that the probability of transmitting HIV with the transfusion of one unit (or 500 milliliters) of infected blood is 80 to 90 percent (80 or 90 chances in 100). The probability of transmitting HIV with a needlestick injury, which injects only a fraction of a milliliter of blood, is 0.3 percent (1 chance in 300). The concentration of HIV in the fluid is another component of the equation. One milliliter of blood with a million HIVs (officially called virus copies) is much more likely to transmit HIV than a milliliter of blood with only 100,000 copies. This difference in the probabilities of transmission is due to differences in inoculum size. The definition of inoculum size actually includes both the volume of fluid and the concentration of viruses in it.
Intensification: The addition of 1 to 2 drugs to an antiviral regimen that’s having a good effect, but not quite good enough.
Interferons: Interferons are proteins that cause cells to resist attack by certain viruses. Interferons are usually produced by the body, but they are also made artificially and used as medications. For people with HIV infection, interferons are mainly used to treat hepatitis B or hepatitis C. The drug works but only when given intravenously in very large doses, and the side effects may be severe. Most doctors now prescribe a special form of interferon, called peg-interferon, which needs to be injected only once a week. The major side effects of injected interferon are the achiness and fever that accompany flu: it is the interferon produced by the body that causes these symptoms during flu. Another important side effect is depression; less common side effects are nausea, vomiting, low white blood cell counts, rash, hair loss, and liver damage.
Invirase: See Saquinavir.
Isoniazid (INH): Isoniazid is the standard drug used to treat and prevent tuberculosis. Isoniazid is usually recommended for any person with HIV infection who has tuberculosis or who has a positive tuberculosis skin test. The usual dose is 300 milligrams, taken once a day by mouth. The most important side effect is hepatitis, including jaundice (yellowish skin and eyes), dark urine, nausea, and abdominal pain. This side effect is more likely in people who already have liver damage for other reasons, and in older people. People taking isoniazid and having these symptoms should stop taking the drug immediately and call their physicians. INH tends to cause a vitamin B6 deficiency, so INH and vitamin B6 are often given at the same time.
Itraconazole: An antifungal drug that is sometimes used to treat infections caused by Candida, Aspergillus, or Histoplasma. It comes as a capsule, a liquid, or in a form for intravenous administration. The capsule needs to be taken when there is food and stomach acid to permit absorption; the liquid form needs to be taken on an empty stomach.
Kaletra: See Lopinavir.
Kaposi’s sarcoma: Kaposi’s (pronounced kaposhee’s) sarcoma is a tumor of blood vessels caused by a virus called Kaposi’s sarcoma herpes virus (KSHV) or herpes virus 8 because the virus is related to herpes. Approximately 20 percent of all people with AIDS have Kaposi’s sarcoma, but the percentage is highest in gay men: for example, it is 20 times more common in gay men than in people with hemophilia. The symptoms of Kaposi’s sarcoma are purplish nodules, usually a quarter of an inch to an inch in diameter, anywhere on the skin. The nodules are new, firm bumps; they aren’t flat like a freckle. The nodules will grow in size and number. They sometimes occur on internal organs like the lung, brain, and gastrointestinal tract, though they often cause no specific symptoms at these sites. Some nodules are painful. The face and legs may swell if the lymph channels nearby are blocked. If Kaposi’s sarcoma becomes extensive, people may have fever, weight loss, and severe fatigue.
The diagnosis can be established by a biopsy of the nodules. Biopsies are easy to do with nodules on the skin, but more difficult when the nodules are on internal organs. The main reason to do the biopsy is that the nodules might possibly turn out to be something other than Kaposi’s sarcoma; and if they are Kaposi’s sarcoma, they are an AIDS-defining diagnosis. Therapy depends on where Kaposi’s is and what problems it causes. Skin bumps may only require coverup makeup. Some lesions are treated with injections or irradiation. The serious form of Kaposi’s is when there are over 25 spots, there is edema, or when the internal organs are involved. These conditions are often treated with chemotherapy like cancer.
Lactic acidosis: This is a complication of treatment with nucleoside analogs, primarily d4T, AZT, or ddI. The cause is toxicity to mitochondria, tiny particles inside cells responsible for the cell’s metabolism. The result is an increase in lactic acid. The diagnosis is made by measuring the level of lactic acid in the blood. The symptoms are nausea, vomiting, stomach pain, weight loss, and shortness of breath. The symptoms occur in the context of taking one of these three drugs, usually for months. Lactic acidosis can be serious and, if advanced, even life threatening. We have no good treatment except to stop the drug responsible and provide support like intravenous fluids, dialysis, or a ventilator. Lactic acidosis takes a long time to clear up—weeks or months. Most people who have it can never use AZT, ddI, or d4T again.
Lamivudine (3TC, Epivir): A nucleoside analog that works powerfully against HIV, can be taken once a day as a single pill, can be taken with or without food, and has almost no side effects. A similar drug is emtricitabine (FTC, Emtriva). Nearly everybody who takes antiretroviral treatment takes one of these two drugs. The two are never taken together because they are too similar. The one problem is that when the virus is not well controlled, it can get a mutation at codon 184 of the reverse transcriptase gene that reduces the action of both 3TC and FTC. This is the most common resistance mutation. After this mutation occurs, many people continue taking the drugs, which are still active against HIV even with the mutation. The two drugs are also effective against the hepatitis B virus (HBV) but for people with both HBV and HIV, taking the drugs can be tricky. For example, if the drugs are stopped for any reason, the hepatitis can flare up. Or the HBV may become resistant to these drugs after several months (as it is prone to do) so that the drugs no longer control it. Experts in hepatitis and HIV know how to deal with these issues.
Latency: Latency and dormancy (which literally means sleeping) mean the same thing: a microbe is in the body but is not actively reproducing, not invading any tissues, and not causing symptoms. Examples of microbes that are latent or dormant in many or most healthy people are: Pneumocystis jiroveci, Toxoplasma gondii, herpes simplex virus, the virus that causes herpes zoster, and cytomegalovirus. Once in the body, these microbes remain in the body. They remain latent or dormant until something tilts the balance in the immune system and permits them to become active.
Leukopenia: Leukopenia means a low number (or penia) of white blood cells (or leukocytes—leuko means white), the cells of the immune system that fight infection. Leukocytes include lymphocytes (cells that recognize foreign material) and neutrophils (cells that gobble up microbes). The normal leukocyte count is 4,000 to 8,000 per milliliter of blood. In people with certain infections, especially with bacterial infections, the leukocyte count is high (leukocytosis). In people with viral infections, including HIV infection, the leukocyte count is low (leukopenia). Having a low count of lymphocytes is called lymphopenia; lymphopenia is the expected result of HIV infection. A low count of neutrophils is called neutropenia; neutropenia can be caused by HIV itself or by some of the drugs—like AZT or trimethoprim-sulfamethoxazole (Bactrim or Septra)—commonly taken during HIV infection. Neutropenia becomes worrisome if the count is less than 750 per milliliter; if the count is less than 500 per milliliter, the person is prone to bacterial infections. Neutropenia is usually not a big problem in people with HIV infection; when it is severe, however, it can often be reversed with G-CSF (Neupogen) (see G-CSF).
Lexiva: See Fosamprenavir.
Lipoatrophy: This is the medical terms for fat loss. It is a side effect of d4T, AZT, and ddI. The fat is lost in the arms and legs, buttocks, and face. In the face, it causes a characteristic “sunken cheek” appearance and is usually a side effect of taking d4T—or, less commonly, AZT—for years. People don’t like the change in the way they look, which they feel is stigmatizing. This fat loss has no medical consequences. When you stop taking d4T or AZT, the side effect may go away, but it may take years or may not happen at all. Some treatments with injections fill out the face. These treatments are often highly effective, but medical insurance does not pay for them.
Lipodystrophy: A complication of antiretroviral therapy that includes (1) high levels of blood fats, or hyperlipidemia, which predisposes the person to heart disease and stroke; (2) redistribution of fat on the body, resulting in a protuberant abdomen (“crix belly”), a collection of fat on the back of the neck (“buffalo hump”), enlarged breasts in women, thin arms and legs with prominent veins, and sunken cheeks; (3) diabetes; and (4) bone thinning or osteoporosis. Most people have one or two of these symptoms, not all four. The cause is not clear, but appears related to antiretroviral drugs.
Lopinavir/ritonavir (Kaletra): A combination of two FI’s (see below). One is lopinavir, which does the job against HIV, and the other is ritonavir, which is given only to increase the levels of lopinavir.
Lumbar puncture: See Spinal tap.
Lymph glands: The lymphatic system is a widespread network, like the blood circulation, of channels that carry lymph. Lymph is a clear fluid containing lymphocytes, or white blood cells (including CD4 cells), which are a part of the immune system. Lymph is manufactured in the lymph glands, clumps of lymphatic tissue that trap infecting microbes and are distributed widely throughout the body. When lymph glands are near the surface of the skin, they can be felt as bumps below the skin’s surface. The usual locations where they can be felt are the back of the neck, below the jaw, under the armpits, and in the groin. Lymph glands are commonly swollen and sometimes painful and tender when they are infected. Many infections involve the lymph glands. In HIV infection, the lymph glands become infected early. The lymph glands are the sites where HIV concentrates most highly, where much of the destruction of CD4 cells takes place, and where much of the reproduction of HIV also takes place. Swollen lymph glands are likely to occur in three different circumstances: with persistent generalized lymphadenopathy, or PGL (see below), in which many lymph glands are swollen for months early in the course of HIV infection; with infection of the lymph glands by certain complications later in the course of HIV infection; and with lymphomas, which are tumors of the lymphatic system seen more frequently in people with HIV infection than in the general population. Swollen lymph glands may require diagnostic tests: the usual is a biopsy of the lymph gland or removal of the whole gland to permit microscopic examination of the lymphatic tissue.
Lymphadenopathy: Lymphadenopathy means swollen lymph glands. Swollen lymph glands are most common at the back of the neck, along the jaw, in the armpits, and in the groin. The lymph glands may feel like rubbery, discrete nodules that are rarely tender to touch and often pea-sized; glands of this description are common in everyone and in several conditions unrelated to HIV infection. If they are swollen to abnormal size for longer than a month in at least two different areas, they constitute persistent generalized lymphadenopathy (PGL) (see below).
Lymphoma: Lymphoma is a cancer of the lymphatic system. Lymphoma occurs most frequently in people without HIV infection, but people with weakened immune systems, including those with HIV infection, have lymphomas about forty times more frequently than normal. About 5 to 10 percent of people with AIDS have lymphomas, and for people with AIDS, lymphomas are classified as opportunistic tumors. Lymphomas are one of the few complications of HIV infection that appears to be increasing in the era of HAART, presumably because lymphomas are not so dependent on severe immune suppression—so immune reconstitution helps but not as much as with other HIV complications.
There are many types of lymphomas: some progress extremely slowly, cause few symptoms, and require minimal treatment; some are more severe. People with AIDS generally have lymphomas called non-Hodgkin’s lymphomas of B cell origin. These lymphomas tend to be severe, and they also tend to involve unusual areas of the body like the brain, liver, kidneys, intestines, and lungs. The diagnosis is usually established with a biopsy. Treatment is variable and often requires the assistance of a specialist in cancer treatment using cancer chemotherapy or radiation treatment.
MAC: See Mycobacterium avium complex.
Magnetic resonance imaging (MRI): Magnetic resonance imaging is a technique used to make a three-dimensional image of the interior of the body. Though the technique is somewhat different from a CT scan (see Computerized tomography scan), the images are similar. The person getting an MRI is placed inside a large tubular structure and remains motionless for thirty to sixty minutes: the worst problems are boredom, noise, and claustrophobia. During that time, the person’s body is bathed in a magnetic field, which causes the atoms in different tissues to give off tiny radio signals. The signals are different depending on the kind of tissue. An MRI is better than a CT scan at detecting diseases of the brain and spinal cord. MRI is painless, harmless, and does not involve exposure to radiation. MRIs are also expensive, from $500 to $1,000.
Managed care organization: An organization that takes financial and medical responsibility for its subscribers’ health care. The best- known managed care organizations are called health maintenance organizations, or HMOs.
Marinol: The psychoactive component of marijuana. It is used to increase appetite in people with wasting. It is expensive, has psychological side effects, and most of the weight gain is fat, as opposed to a more useful protein. Whether or not marinol works as well as smoking marijuana cigarettes has not been studied.
Megestrol acetate (Megace): Megestrol is a female hormone that stimulates the appetite. The drug may cause reduced libido in men. Most of the weight gained is fat, rather than protein.
Meningitis: Meningitis is an infection of the meninges, the membrane that envelops the brain and spinal cord. The most common cause of meningitis in people with HIV infection is Cryptococcus (see under Cryptococcosis).
Methadone: Methadone is an opiate that is commonly used to control narcotic withdrawal symptoms and to maintain people addicted to morphine-like drugs, particularly heroin. Methadone maintenance is permitted only in programs approved by the Food and Drug Administration and the designated state authority. Methadone can be given by mouth or by vein. Side effects are those shared by all morphine-like drugs, which depress the central nervous system: dizziness, mental clouding, depression, and sedation. Methadone may cause physical dependence. If it is stopped abruptly after prolonged and regular use, it can cause withdrawal symptoms.
Metronidazole (Flagyl): Metronidazole is an antibiotic taken by people with HIV infection for common intestinal infections and common dental problems like gingivitis (inflammation of the gums) and periodontitis (infection of the structures that support the teeth). The drug is given by mouth or by vein. Side effects are unusual, primarily nausea and stomach pain. The side effects can improve if the drug is taken with meals or if the dose is reduced. Taking this drug for periods of months may cause pain in the feet that resembles the pain of HIV neuropathy (see below). The pain usually goes away when the drug is stopped.
Microbes: Microbes are organisms so small they require a microscope to be seen. They can be bacteria, viruses, parasites, or fungi. HIV is one example of a virus. Microbes cause infectious diseases. The microbes that commonly cause the infections that are complications of HIV infection are as follows:
Viruses: Cytomegalovirus, herpes simplex, herpes zoster, molluscum contagiosum
Bacteria: Mycobacterium avium complex, Mycobacterium tuberculosis (the cause of tuberculosis), Salmonella, Nocardia, pneumococcus, Bartonella
Parasites: Toxoplasma gondii, Cryptosporidium, Isospora
Fungi: Pneumocystis jiroveci, Cryptococcus, Histoplasma, Candida albicans, Coccidioides, Aspergillus
Mutation: A change in a gene that can in turn change certain of a microbe’s characteristics: growth, appearance, sensitivity to drugs, ability to invade, and response to antibodies. HIV mutates extensively. Within a few years, the person infected with one strain of HIV has billions of different mutant strains in his or her body. If the person takes AZT, then evolution assures that HIV mutates to become resistant to AZT. Mutated strains of HIV also confound vaccine development because the immune system may not recognize them.
Mycobacterium avium complex (MAC): MAC is related to the bacterium that causes tuberculosis, though it is not contagious and is more difficult to treat. In the late stages of HIV infection, infection with MAC is spread widely throughout many organs in the body. It can cause fever, pneumonia, diarrhea, hepatitis, and many other complications. In a person with a CD4 count under 50, MAC most commonly causes prolonged fever and abdominal pain.
National Institutes of Health (NIH): NIH is a federal organization located in Bethesda, Maryland, that funds scientific research. NIH is the world’s largest research organization. With a budget of over $10 billion a year, NIH is responsible for funding about a third of all research in the biomedical sciences, including research related to HIV infection, in the United States. About $1.8 billion is allocated annually to research on HIV. Some of the research sponsored by NIH is intramural; that is, it is conducted by the approximately one thousand researchers inside NIH; most of the research is extramural, at universities and medical schools throughout the country. Extramural research grants are awarded on the basis of priority, as determined by expert review of proposals. NIH is divided into fifteen different institutes, each with a different scientific specialty: the National Institute for Allergy and Infectious Diseases (NIAID) is responsible for most of the research into HIV infection. NIH is not related to the Centers for Disease Control and Prevention (see above), except that both are federally funded agencies with somewhat different roles in combating HIV and other diseases.
Funding for research into HIV infection from sources other than NIH comes from other federal agencies (Department of Defense, National Science Foundation, Veterans Administration, and the Centers for Disease Control and Prevention), pharmaceutical companies, local governments, and private foundations. Funding for this research escalated rapidly in the late 1980s until the total HIV research budget exceeded the funding for heart disease research at a time when heart disease was responsible for twenty times more deaths than AIDS was. Some view this as inappropriate, given the relative impact of the two; others feel AIDS research is underfunded, given its importance as a public health problem, its role as the major cause of death in Americans aged 24 to 44, and as a prototypic disease for many other conditions—that is, what we learn from HIV may be applied as well to such diseases as cancer, diabetes, and lupus.
Nelfinavir (Viracept): A protease inhibitor taken 2 times a day. The major side effect is diarrhea. This is the only protease inhibitor that is not “boosted” with ritonavir.
Neuropathy: Neuropathy is an illness involving the nerves. Nerves are responsible for (among other things) the movement of muscles and the sensation of touch, including the sensation of pain. The symptoms of a neuropathy can therefore be weakness of a muscle or pain and tingling. In people with HIV infection, the most frequent symptoms of neuropathy are painful feet and legs. There may be tingling as if the foot were asleep. Often the bottom of the foot is most affected, which may interfere with walking or require pain medication. Neuropathy may be the result of HIV infection or a side effect of some drugs, especially ddI, ddC, or d4T.
Nevirapine (Viramune): An NNRTI (see below) taken twice a day. The major side effects are rash and liver disease, usually in the first 8 to 16 weeks of treatment. Rash occurs in 15 to 20 percent of the people taking it and may be severe. A rash in the form of red splotches is usually not serious but should be checked out. Rashes are serious when they show blisters, involve the mouth or eyes, or occur with fever. The liver disease can be very serious; if you have severe stomach problems, a rash, or fever, you need immediate evaluation. You should report to your doctor any sickness during the first 8 to 16 weeks of taking nevirapine.
NNRTIs: Short for nonnucleoside reverse transcriptase inhibitors (see below).
Nonnucleoside reverse transcriptase inhibitors (NNRTIs): A class of drugs that inhibit reverse transcriptase but are not in the same class as nucleosides. Examples of NNRTIs are efavirenz, nevirapine, and delavirdine.
Norvir: See Ritonavir.
Nucleoside analogs: Nucleoside analogs, sometimes called just nucleosides, are a chemically related group of drugs used to inhibit HIV. Examples include the first drugs approved to treat HIV infection: AZT, ddI, ddC, d4T, ABC, 3TC, FTC, and TDF. Often these drugs are combined to reduce the “pill burden,” the total number of pills you need to take. These combinations are AZT/3TC (Combivir), AZT/3TC/ABC (Trizivir), TDF/FTC (Truvada), and 3TC/ABC (Epzicom). They all work by the same mechanism, by inhibiting an enzyme called reverse transcriptase that is critical for HIV’s survival. Nucleoside analogs often seem to have time-limited benefit, that is, after prolonged use they stop working. This happens because HIV develops resistance to a particular nucleoside analog. Nevertheless, HIV often remains sensitive to other nucleoside analogs, which can then be substituted or added.
Nukes or nucs: Shorthand for nucleoside analogs (see above).
Opportunistic infections: In all infectious diseases, the body’s defenses are, for a while, inadequate to control microbial invasion. Many microbes can cause disease in people who are otherwise healthy. Other microbes, however, are fairly harmless and can cause disease only in people whose immune defenses are weakened. These microbes are called opportunistic microbes because the microbe takes the opportunity offered by a weakened immune system to cause disease. The opportunistic microbes that most frequently infect people with HIV infection are listed above, under Microbes.
Opportunistic tumors: Opportunistic tumors, like opportunistic infections, occur primarily in people with weakened immune systems. In people with HIV infection, the major opportunistic tumors are Kaposi’s sarcoma, certain types of lymphoma, and cervical cancer. Two of these tumors and possibly all three are actually caused by viral infections.
Oral hairy leukoplakia (OHL): The symptoms of oral hairy leukoplakia are white (leuko) patches (plakia) on the tongue and elsewhere in the mouth. It usually produces no symptoms, but may distort taste or cause pain. It is caused by the same virus that causes infectious mononucleosis. These patches often appear similar to those of thrush; in fact, oral hairy leukoplakia is often diagnosed when people who appear to have thrush do not respond to the usual treatment. It can also be diagnosed with a biopsy of the patches. Oral hairy leukoplakia seems to occur exclusively in people with HIV infection. It generally indicates progressive weakening of the immune system. Most people have no symptoms, but when they do, the usual treatment is high doses of acyclovir.
Pancreatitis: Inflammation of the pancreas, an organ in the abdomen that makes insulin and digestive enzymes. Symptoms are abdominal pain, nausea, and vomiting. Pancreatitis is a potentially serious complication of alcoholism and of some drugs, like ddI or d4T, used to treat HIV infection.
Paromomycin: An antimicrobial drug used to treat cryptosporidiosis. It is taken by mouth and sometimes effectively reduces symptoms.
Pentamidine: Pentamidine is a drug used to treat or prevent pneumocystis pneumonia. Pentamidine is often used only when someone cannot take the best drug, trimethoprim-sulfamethoxazole. To treat pneumocystis pneumonia, pentamidine is given by vein for three weeks. To prevent pneumocystis pneumonia in people whose CD4 count is less than 200, pentamidine is given by aerosol directly into the lungs, at monthly intervals. When given by vein, pentamidine often has severe side effects, such as low blood pressure (causing fainting), low blood sugar, high blood sugar (diabetes), kidney failure, liver disease, low blood counts, or inflammation of the pancreas. These side effects are common when the drug is given by vein. They are rare or don’t occur at all when pentamidine is taken as an aerosol, since so little of the drug gets into the system.
Persistent generalized lymphadenopathy (PGL): A diagnosis of PGL means that lymph glands are swollen for at least one month and at two different sites of the body, not counting the groin area. PGL often occurs early in HIV infection. Lymph glands are the location of HIV multiplication at a time when the patient feels well. (See Lymph glands and Lymphadenopathy.)
PIs: Shorthand for protease inhibitors (see below).
Platelets: Platelets are the component of blood that facilitates clotting. The number of platelets is often low in people with HIV infection— sometimes so extremely low that the person is prone to bleeding. The cause of the low platelet count may be HIV infection itself, or it may be the drugs that are used to treat people with HIV infection. The normal platelet count is over 150,000 per milliliter of blood; a count of 50,000 to 150,000 is low but usually causes no problem; a count of 10,000 to 50,000 is worrisome, and less than 10,000 is serious. These numbers are rough: some people do fine for years with counts of 5,000 to 15,000, while other people with counts of 30,000 have profuse bleeding.
Pneumococcal vaccine: The most common cause of bacterial pneumonia in people without HIV infection is a bacterium called Streptococcus pneumoniae or pneumococcus. Pneumococcus causes pneumonia about 100 times more frequently in people with HIV infection. Pneumococcal vaccine is recommended for people with HIV infection, since they are prone to frequent or severe infections by pneumococcus. It is best to take this vaccine relatively early in the course of the disease when the immune system is strong. This means having a CD4 count of over 200.
Pneumocystis jiroveci (formerly Pneumocystis carinii): This fungus commonly causes lung infection and pneumonia in people with HIV infection. Pneumocystis jiroveci pneumonia (PCP) is the most frequent serious complication in people with HIV infection. Pneumocystis pneumonia is the most common AIDS-defining diagnosis. The symptoms are cough without sputum, shortness of breath, and fever. These symptoms usually evolve over a period of weeks. The diagnosis is generally established by a chest X-ray or studies of lung function, combined with a microscopic examination of respiratory secretions to show the fungus. Treatment is with several drugs— most commonly trimethoprim-sulfamethoxazole, but also pentamidine, dapsone-trimethoprim, atovaquone (Mepron), or clindamycinprimaquine. Treatment is most successful when started relatively early in the course of the infection.
Pneumonia: Pneumonia is an infection of the lungs. The usual symptoms are cough, fever, and shortness of breath. The causes of pneumonia vary, and the treatment depends on the cause.
Polymerase chain reaction (PCR): Polymerase chain reaction is a method for multiplying some part of a microbe’s gene to huge concentrations within hours. It allows for a very sensitive test, developed in the 1980s, for detecting many microbes, including HIV (see Retrovirus). Unlike the standard blood test for HIV infection, which detects antibodies to HIV, the PCR detects HIV itself. This test can now be used to measure the concentration of HIV in the blood, called the HIV viral load (see below, Quantitative virology). Concentrations usually range from 1,000 to 1,000,000 viruses per milliliter of blood. Concentrations are highest in the first few weeks of infection before the immune defenses have responded, and in the late stage of the infection, when the immune defenses have been destroyed.
Progressive multifocal leukoencephalopathy: Progressive multifocal leukoencephalopathy is a viral infection deep in the brain that is found only in people with severely weakened immune systems, including, occasionally, people with HIV infection. Progressive multifocal leukoencephalopathy has a distinctive appearance on CT or MRI scans of the brain, but a diagnosis can be established definitely only with a biopsy. The infection tends to be progressive, and no therapy is known to be effective. Among people with HIV infection, it occurs only in the late stage, when the CD4 count is under 50.
Prophylaxis: Prophylaxis is treatment to prevent a disease, as opposed to treatment to eliminate a disease already present.
Protease inhibitors (PIs): This class of drugs inhibits HIV by interfering with the enzyme protease, which is critical for assembling the complete virus after it has reproduced. Several drugs are in this class, including saquinavir (Invirase), ritonavir (Norvir), indinavir (Crix- ivan), fosamprenavir (Lexiva), lopinavir (Kaletra), atazanavir (Rey- ataz), tipranavir (Aptivus), and nelfinavir (Viracept). Initial tests show that PIs and the NNRTIs are the most potent drugs we have for decreasing the concentration of HIV. The initial effect is a decrease in viral load by 99 percent. To keep the viral load low without also developing resistance, PIs must be combined with nucleosides.
Protease paunch: Slang for the collection of abdominal fat that is a side effect of protease inhibitors. Another term is “crix belly,” referring to Crixivan (indinavir), but the side effect can occur with any PI. It may disappear if treatment with the PI is stopped—for example, changing to efavirenz-based HAART—but the disappearance is very slow.
Pyrimethamine (Daraprim): Pyrimethamine is an antibiotic used to treat or prevent toxoplasmosis (see below). The full treatment usually combines pyrimethamine with a sulfa drug like sulfadiazine or clindamycin. Pyrimethamine is taken by mouth. The major side effect after prolonged use is anemia. To avoid anemia, another drug, leucovorin, is given at the same time. Other side effects include gastric intolerance, allergic reactions, and hepatitis. Many of these reactions are the result of the sulfa drug that is taken with pyrimethamine.
Quantitative virology: Quantitative virology is a method of determining the concentration of a virus in some part of the body, in this case, the concentration of HIV in the blood. “Viral load” and “viral burden” are synonymous terms for quantitative virology. Two different tests are usually used to measure quantitative HIV virology: polymerase chain reaction (quantitative RNA-PCR) (see above) and branched chain DNA (bDNA). In both tests, parts of the virus serve as tags for that particular virus. These tags are multiplied to huge concentrations within hours so that the presence of that virus becomes obvious. Once the virus tags are detected, then the concentration of the tags is extrapolated backward to the original concentration of the virus. The concentration of HIV usually ranges from 1,000 to 1,000,000 viruses per milliliter of blood. Quantitative virology measures the amount of virus and appears to supplement the CD4 count to indicate the stage of disease, or the prognosis. Concentrations over 100,000 per milliliter usually indicate that the disease is progressing. Quantitative virology is also used to measure the response to therapy. Most drugs cause a decrease in viral concentrations within hours.
Randomized trial: A trial or experiment comparing treatments. Participants are assigned to take one treatment or the other. Which treatment they take is a matter of chance; their assignment is random. Random assignment is necessary if the trial is to be scientifically credible. See chapter 8.
Receptor: A docking site on a cell to which a molecule or microbe attaches before entering the cell. The receptor for HIV is the CD4 receptor, for which the CD4 cell is named.
Rescriptor: See Delavirdine.
Research: See National Institutes of Health.
Reservoir: A place, like the genital tract or the central nervous system, where HIV can hide from treatment.
Resistance: Resistance, when used in medicine, means that a drug is not effective because the microbe being treated has been able to change its chemistry so it is no longer susceptible to the drug (see Mutation, above). The result is either that the drug does not work in the test tube against this person’s microbe, or that the person stops getting better; usually both results are found together. Resistance is usually qualitative; that is, HIV may be highly resistant or slightly resistant. Furthermore, the person with HIV infection has billions of genetically different HIVs. Some HIVs may be sensitive to one drug and not to another, some are sensitive to all drugs, and some are resistant to every drug. People with very resistant HIVs have usually had many different courses of antiviral drugs.
There are two methods of measuring resistance. One detects mutations that confer complete or partial resistance. These mutations occur at specific locations, called codons, on the relevant gene—the reverse transcriptase gene for nucleosides and NNRTIs, and the protease gene for PIs. An example: a mutation on codon 184 of the reverse transcriptase gene makes 3TC (lamivudine) ineffective. Many drugs require many mutations before becoming ineffective.
The other method of measuring resistance is with a phenotypic test, which simply measures the amount of the drug required to inhibit a particular strain of HIV. If the amount of drug to inhibit that strain is many times greater than the amount that inhibits untreated strains, then that particular strain is resistant.
Retinitis: Retinitis means an inflammation (itis) of the retina, the layer of cells at the back of the eye that collect and send images to the brain. Retinitis usually causes some loss of vision. The earliest symptoms are pain in the eye, “floaters” across the field of vision, or a blind spot, which is the loss of part of a visual field. In people with HIV infection, the most common cause of retinitis is infection with cytomegalovirus (see above, CMV). CMV retinitis rarely occurs when the CD4 count is above 50.
Retrovirus: Retroviruses are a type of virus. Retroviruses do not have DNA, the molecule that holds the genetic code that cells use to reproduce themselves. Instead, retroviruses have RNA and an enzyme called reverse transcriptase, which turns RNA into DNA. When a retrovirus invades one of the cells of the body, it uses reverse transcriptase to turn its own RNA into DNA. This DNA then becomes part of the cell’s DNA. When properly stimulated, the DNA then makes more retrovirus instead of more cells. Many different kinds of retroviruses infect many different kinds of animals. HIV is the most important retrovirus to infect humans; it causes disease in no other animal species except for certain types of monkeys. On the whole, it is not easy for retroviruses to pass from one species to another.
Reyataz: See Atazanavir.
Risk factor: A risk factor is a condition or behavior that makes it likely that a person with the risk factor will develop a condition—in this case, HIV infection. The major risk factors for HIV infection are needle-sharing with injection drug users and sexual contact with a person who has HIV infection. Another risk factor is having received blood products between 1978—when HIV infection was first known to exist in the United States—and April 1985, when the blood supply was first screened for HIV. Other risks that heighten the probability that HIV will be transmitted through sexual intercourse are multiple sex partners, failure to use condoms, sex with someone in the late stage of the disease (when the viral load is high), anal sex, and sex with someone who has a sexually transmitted disease, especially genital ulcers. The risk to an infant born to a woman with HIV infection is 20 to 35 percent if the mother has not taken drugs to inhibit HIV. A minor risk factor in terms of frequency is needlestick injuries in health care workers who care for people with HIV infection. Less than 1 percent of all people with HIV infection in the United States have no clearly defined risk factor, although many of these people either are too sick to provide adequate information or are providing information that is suspect.
Ritonavir (Norvir): A protease inhibitor commonly used with other protease inhibitors. The reason is that ritonavir increases blood levels of the other PI by inhibiting the enzyme normally responsible for getting the other PI excreted. Ritonavir can be used as a single PI, but many people have trouble tolerating the necessary dose.
Safer sex: Safer sex is a qualitative term. To be absolutely safe, sexual contact cannot involve an exchange of any body fluids—specifically, semen, blood, or vaginal secretions. The term safer sex recognizes the likelihood of human error and the inexactness of human knowledge. Safer sex refers to sexual intercourse using a condom, or sexual practices that do not involve exchange of body fluids.
Salvage therapy: Treatment against HIV after a previous treatment has failed and the viral load has increased.
Saquinavir (Invirase): A protease inhibitor (see above) that comes in two forms. The first form, introduced in 1995, was Invirase. Since the body absorbed only about 4 percent of the drug, it has now been augmented by giving it with ritonavir to “boost” its levels. The main side effect is stomach distress.
Seizure: A seizure is a convulsion, uncontrolled movements of the arms and legs accompanied by unconsciousness and inability to control urine or stool. The usual cause of seizures in people with HIV infection is an opportunistic infection or an opportunistic tumor of the brain, including toxoplasma encephalitis, cryptococcal meningitis, or lymphoma. Less commonly, seizures are caused by HIV itself, or result from an imbalance of electrolytes, or are a side effect of medications. Recurrent seizures can usually be controlled with drugs like Dilantin and phenobarbital. Anyone with recurrent seizures should be careful about his or her physical circumstances: be careful working on ladders, for instance, or driving. In many states it is illegal for a person with seizures to drive until seizures have been controlled for at least one year.
Seroconversion: The immune system usually takes several days or weeks to recognize a foreign substance like a virus and to produce antibodies to it. Six to twelve weeks after HIV enters the body, antibodies to HIV usually appear in the blood. Physicians call the appearance of antibodies in the blood seroconversion. That is, the result of a test for antibodies in the blood serum converts from negative to positive.
Shingles: Synonymous with herpes zoster (see above).
Sinusitis: The sinuses are air sacs next to the passageway from the nose. Sinusitis is an infection of the sinuses, usually as a result of a cold or an allergy. Anyone can get sinusitis, but people with HIV infection have it more often, it is more likely to affect many sinuses, and it is often more difficult to treat. Symptoms are pus drainage from the nose, headache, face pain, and fever. The usual treatment is with antibiotics taken by mouth, such as trimethoprim-sulfamethoxazole, amoxicillin, erythromycin, cephalexin (or Keflex), cefaclor (Ceclor), clarithromycin (Biaxin), azithromycin (Zithromax), ciprofloxacin (Cipro), or tetracycline. Some people do not respond to these drugs, and their sinuses need to be drained, a procedure done by a specialist called an otolaryngologist (ear, nose, and throat specialist).
Spinal tap: A spinal tap, also called a lumbar puncture, is a procedure for obtaining cerebrospinal fluid, the fluid that surrounds the brain and the spinal cord. The procedure involves inserting a needle into the middle of the back and into the meninges, a membrane that contains the cerebrospinal fluid. The cerebrospinal fluid is then analyzed for evidence of infection of the brain or spinal cord. Despite sounding unpleasant and risky, a spinal tap is a well-established medical procedure and is rarely associated with any important complications. The most common complaint is a headache following the spinal tap, a complaint made less likely by lying flat once the spinal tap is completed.
Statins: A class of drugs that lower blood cholesterol. Most protease inhibitors increase cholesterol, and statins are taken to correct the increase. The problem is that most PIs interfere with the metabolism of the statins, so taking the two kinds of drugs together gets complicated. They may cause muscle pain, which can be a serious complication. In general, PIs are never to be taken with lovastatin (Altocor, Mevacor) or simvastatin (Zocor). Other statins, such as atorvastatin (Lipitor) or pravastatin (Pravachol) are less problematic, but we still prescribe low doses and alert the person taking the drug.
Sustiva: See Efavirenz.
3TC (lamivudine): A nucleoside analog, like AZT, ddI, ddC, d4T, and abacavir, that acts against HIV by inhibiting the enzyme reverse transcriptase, which HIV uses to reproduce. 3TC also inhibits the hepatitis B virus. For HIV infections, 3TC is most commonly used in combination with AZT, TDF, or ABC. Side effects are rare.
T-helper cells: Synonymous with T4 cells, T4 lymphocytes, and CD4 lymphocytes. (See above, CD4 cells.)
T-suppressor lymphocytes: T-suppressor lymphocytes are another class of T lymphocytes (see above, Immune system). T-suppressor lymphocytes are synonymous with T8 cells, CD8 cells, and T8 lymphocytes. All T lymphocytes participate in the body’s defenses. A small subset of the CD8 cells targets HIV and is therefore responsible for destroying the CD4 cells that harbor the virus and therefore the virus itself. During the initial illness, called acute HIV infection or acute retroviral syndrome, the concentrations of HIV are high. The CD8 response decreases the HIV concentration precipitously, and the symptoms of the initial illness accordingly disappear. The laboratory test called the T-cell subset analysis is a count of the various types of T lymphocytes.
Tenofovir (TDF, Viread): This drug is closely related to the nucleoside analogs but is a nucleotide. It is highly active against HIV, has few side effects, and can be taken as a single pill once daily. It can cause kidney damage if taken in too high a dose—occurring if someone forgets to lower the dose when, for other reasons, the kidneys don’t work well.
Testosterone: Many men with HIV infection have low levels of testosterone. This is especially true for men who take Megace, which is a female hormone. Testosterone may be important in the prevention and treatment of wasting, primarily in men with low testosterone levels. It is given as a patch or by injection at intervals of 1 to 2 weeks.
Thalidomide: A drug once abandoned because it caused birth defects when given to pregnant women. It is now available for people with HIV infection and is used to treat wasting and aphthous ulcers.
Thrombocytopenia: Thrombocytopenia is a low count (penia) of thrombocytes (or platelets), cells in the blood that facilitate clotting. The usual count of thrombocytes is 150,000 to 300,000 per milliliter of blood. Lower counts of 50,000 to 120,000 per milliliter are common in people with HIV infection. When the count is very low, from 5,000 to 25,000 per milliliter, bleeding problems may occur. People with HIV infection have thrombocytopenia because their bodies produce antibodies against their own platelets. Some people have no symptoms but must still be careful to avoid cuts or anything that could cause bleeding. Other people have excessive nosebleeds, excessive bleeding from cuts, bleeding into the stomach or intestines, and red spots the size of pinheads that come from tiny hemorrhages into the skin. Treatment is with drugs—corticosteroids (see above), HAART (see above), or gamma globulin given intravenously.
Thrush: Thrush is an infection of the mouth caused by the fungus Candida albicans. The symptoms are white patches along the gums, on the inside of the cheeks, on the roof of the mouth, or on the tongue. Thrush is extremely common in people with HIV infection, and is considered part of early symptomatic HIV infection. Thrush is easily treated with nystatin, clotrimazole, ketoconazole, or fluconazole.
Tipranavir (TPV, Aptiva): A protease inhibitor intended for people for whom prior treatment has failed. It must be boosted with ritonavir, and it can’t be used with other protease inhibitors because of some harsh drug interactions. It interacts with many other kinds of drugs as well, and has a high rate of liver toxicity.
Toxoplasmosis: Toxoplasmosis is an infection caused by the parasite Toxoplasma gondii. Toxoplasma gondii is found in cat excrement and in rare meat, both of which are potential sources of infection. About 10 to 30 percent of all adults in the United States have Toxoplasma gondii in their bodies, but the majority are unaware of it. The carriers of Toxoplasma can be identified by a blood test for antibodies to the parasite. The parasite remains dormant (see Latency) and rarely causes disease unless the immune system is weakened. In people with HIV infection, the most common form of toxoplasmosis is an infection of the brain called toxoplasma encephalitis. The usual symptoms are headaches and fever, with a CD4 count below 100; many people have seizures, a weak arm, weak leg, or other neurologic symptoms. An MRI scan (see Magnetic resonance imaging) of the brain usually shows certain specific changes. Treatment is with a combination of pyrimethamine and either a sulfa drug or clindamycin. Toxoplasmosis can be prevented by taking trimethoprim- sulfamethoxazole, the same drug that prevents PCP (see below).
Trimethoprimsulfamethoxazole (Bactrim, Septra): This is an antibiotic used to prevent and treat pneumonia caused by Pneumocystis jiro- veci. Trimethoprim-sulfamethoxazole can be taken by mouth or by vein. Its advantage is that it treats or prevents many other infections as well. Its major disadvantage is that many people develop reactions to it—fever, rash, low white blood cell count, and hepatitis. Many people will tolerate the drug if they stop taking it for a while and then begin taking it again at a lower dose.
Triple therapy: The use of three different drugs to treat HIV, usually two nucleoside analogs and a protease inhibitor, either nevirapine or efavirenz. See HAART.
Trizivir (AZT + 3TC + ABC): One of the combinations of nucleoside analogs (see above) that are taken as one pill twice daily. The advantage is the reduction in “pill burden,” which makes adhering to the drug regimen easier.
Truvada: A combination pill containing tenofovir and emtricitabine.
Tuberculosis (TB): Tuberculosis is an infection, usually in the lungs, that is over 100 times more frequent in people with HIV infection than in the general population. The bacterium that causes TB can either be dormant (inactive TB) or active (active TB). In active TB, the usual symptoms are fever, cough, weight loss, fatigue, and night sweats. People with either active or inactive TB may have skin tests that are positive for TB. In people with HIV infection, the skin test is less reliable, especially in the later stages of HIV infection, when the immune system is weakened. People with HIV infection and inactive TB should receive treatment to prevent active TB. People with HIV infection and active TB should receive a combination of four drugs that include isoniazid (INH), rifampin, pyrazinamide, and either streptomycin or ethambutol (Myambutol). A new form of tuberculosis is resistant to some or all of these drugs. This new tuberculosis occurs most commonly in people who do not complete the standard treatment and in people living in New York City.
Ultrasensitive: Describes a test for HIV that detects concentrations of the virus as small as 20 to 50 copies per milliliter. A newer ultraultrasensitive test will detect concentrations as low as 5 copies per milliliter.
Undetectable: Describes measurements of viral load that fail to detect HIV because HIV is in such low concentrations. What undetectable actually means differs according to the sensitivity of the test (see above, Ultrasensitive). Standard tests detect amounts of virus over 400 to 500 viruses per milliliter of blood; the “ultrasensitive” tests detect amounts over 20 to 50 viruses per milliliter of blood.
Vaccine: A vaccine is a substance, given by mouth or by an injection, that stimulates the immune system to form antibodies to some microbe. The polio vaccine, for instance, stimulates the immune system to form antibodies against the polio virus. These newly formed antibodies now protect the person against any subsequent exposure to that microbe. Some vaccines work better than others: with the polio vaccine, protection is nearly 100 percent; with the influenza vaccine, protection is about 70 percent. Vaccines for HIV infection are being tested in people with and without HIV infection. For people without HIV infection, a vaccine could hopefully work like any other vaccine, that is, it could stimulate antibodies that protect you if you are exposed to HIV. For people with HIV infection, a vaccine could hopefully stimulate the immune system to respond more effectively.
Vaginitis: Vaginitis is infection of the vagina. Symptoms are abnormal vaginal discharge, sometimes with severe itching. Vaginitis has three common infectious causes: (1) “yeast,” or the fungus Candida, which is treated with antifungal drugs like Gyne-Lotrimin or fluconazole; (2) “trick,” short for the parasite Trichomonas vaginalis, which is treated with metronidazole (Flagyl); and (3) certain bacteria also treated with metronidazole. The most common cause of vaginitis in women with HIV infection is yeast infection. This form of vaginitis is more likely to occur if you are taking antibiotics. Vaginitis is common in women without HIV infection, but those with HIV infection have it more frequently and it is more difficult to treat.
Varicella zoster: Varicella zoster is the virus that causes chickenpox (varicella) and herpes zoster (shingles). See above, Herpes zoster.
Vertical transmission: Medical lingo for the transmission of a microbe from a pregnant woman to her newborn baby.
Videx: See ddI.
Viracept: See Nelfinavir.
Viral load: Synonymous with quantitative HIV. Viral load is the concentration of HIV in the blood, which indicates the total amount of HIV in the body. The average viral load for an untreated person is 30,000 to 60,000, meaning 30,000 to 60,000 copies (viruses) per milliliter of blood. The usual goal of therapy is to reduce the viral load to undetectable (see above) levels, meaning less than 50 copies per milliliter.
Viramune: See Nevirapine.
Viread: See Tenofovir.
Virologic failure: Not the failure of the virus, but the failure of the treatment to inhibit the virus. The person taking treatment whose viral load falls only from 100,000 to 10,000 is said to have virologic failure, though this ten-fold decrease is nevertheless a 90 percent decrease in the amount of HIV. The person whose viral load returns to 100,000 despite treatment has complete virologic failure. The first goal of treatment is to decrease the virus ten-fold (or one log) within 1 to 4 weeks. The subsequent goal is to reach a viral load of less than 500 by weeks 8 to 16, and less than 50 at week 24. Despite virologic failure, life is still better than before treatment—presum- ably because the resistant HIV is injured and simply cannot do as much damage.
Virus: A virus is a tiny microbe that, unlike bacteria, can neither survive nor reproduce unless it lives in a cell. HIV is a virus that lives in CD4 lymphocytes in humans.
Wasting: Wasting is the term given—somewhat unfortunately—to the weight loss and malnutrition that often accompany HIV infection. The causes of wasting vary; they may include infections and tumors that are complications of HIV infection. Some people burn more calories because their metabolism increases, usually because of fever and common infections. These people may eat a lot and still lose weight. Other people have malnutrition due to starvation because of sores in their mouths, or depression, or apathy, or side effects of drugs that prevent them from eating. Many people in the late stages of HIV infection seem to have progressive weight loss with what is called protein-calorie malnutrition, which may be the result of the action of cytokines, proteins that regulate the immune system and can cause loss of muscle protein. Wasting can be an AIDS-defining diagnosis: according to the criteria of the Centers for Disease Control and Prevention, an unexplained loss of at least 10 percent of the usual body weight, accompanied by diarrhea or fever for 30 days, is diagnostic of AIDS. Treatment of wasting is varied and is tailored to the cause. Treatments include food supplements such as Ensure, Ensure Plus, Jevity, Criticare, Peptamen, or Perative; appetite stimulants such as Megace, Marinol, and thalidomide; and injections of growth hormone, testosterone, or anabolic steroids. Resistance exercise, like lifting weights, is also helpful.
Western blot: The Western blot is a test for specific antibodies, in this case, for antibodies to HIV. (See above, ELISA test.)
Wild-type HIV: Naturally occurring strain of HIV, that is, HIV with no mutations that may have conferred resistance. Some people use “wild-type” to mean the strain of HIV that’s predominant in a community. In this case, the “wild-type” could conceivably be a resistant strain, if the particular community has extensively used antiretroviral drugs and has had virologic failure (see above).
Xanax: See Benzodiazepines.
Zerit: See d4T.
Ziagen: See Abacavir.
Zovirax: See Acyclovir.