Immunopathology
CD4 lymphocytes (T helper cells) have been termed “the leader of the immunological orchestra” because of their central role in the immune response, and their destruction accounts at least in part for the immunosuppressive effect of the virus.
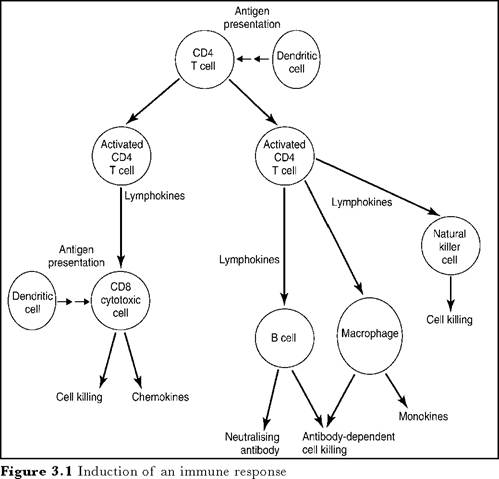
When these cells are stimulated by contact with an antigen they respond by cell division and the production of lymphokines, such as interferons, interleukins, tumour necrosis factor and the chemoattractant chemokines. Lymphokines act as local hormones controlling the growth, maturation and behaviour of other lymphocytes, particularly the cytotoxic/suppressor (CD8) T-cells and antibody-producing B lymphocytes. Lymphokines also affect the maturation and function of monocytes, tissue macrophages and dendritic cells.Macrophages and particularly dendritic cells are important antigen-presenting cells for initiating immune responses of lymphocytes. Not only do they act as a reservoir for the virus
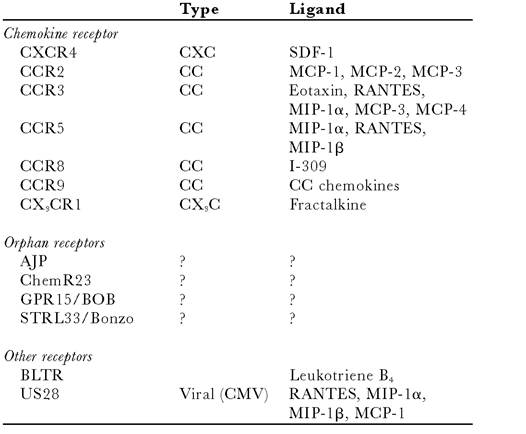
Table 3.1 Co-receptors and their ligands. A large number of seven transmembrane-spanning receptors which can act as co-receptors have been identified. In most cases their importance in vivo remains to be determined. Many are present on some CD4 cells or macrophages
but their antigen-presenting function is impaired, with secondary effects on lymphocytes. Monocytes are the precursors to some glial cells and abnormal lymphokine production after HIV infection may have harmful effects on neural tissue and result in HIV encephalopathy.
Early after HIV infection antibody responses are not impaired; indeed, development of antibodies to the virus envelope and core proteins is the principal evidence for HIV infection and persists until death.
In adults, massive activation of B lymphocytes is manifested by a rise in serum immunoglobulin concentration, perhaps due to direct activation of B cells by HIV. This polyclonal activation explains why a variety of false positive serological tests are seen in HIV infection. In young children, the reverse pattern may be seen, with extremely low levels of immunoglobulin sometimes requiring intravenous replacement therapy.Within days or weeks after infection there may be a transient fall in CD4 lymphocyte numbers and a more sustained rise in the number of CD8 cytotoxic/suppressor cells. Among the CD8 cells, expanded oligoclonal populations are frequently seen and as in other acute virus infections, some of these represent a specific response to HIV. Following this acute reaction, healthy seropositive individuals may have normal numbers of lymphocytes, although the numbers of CD8 cells frequently remain high. Even at this stage, however, in vitro testing may show a lowered response to previously encountered (recall) antigens (tetanus toxoid or purified protein derivative, for example). This seems to be due to poor production of the lymphokine interleukin 2. Individuals may remain healthy for long periods, but a hallmark of disease progression, often prior to the development of new clinical symptoms, is a fall in the number of CD4 lymphocytes. In AIDS the number of CD8 lymphocytes also falls.
Biopsy of the lymph nodes in patients with persistant generalised lymphadenopathy shows many enlarged follicles, often infiltrated by CD8 lymphocytes, with depletion of CD4 cells. Even in clinically silent HIV infection, lymph nodes are the site of remarkably active HIV replication. Uninfected cells may also die by apoptosis, initiated by unexplained mechanisms. In the later stages lymph nodes return to normal size and follicles become “burnt out”, with loss of normal architecture and progressive cellular depletion.
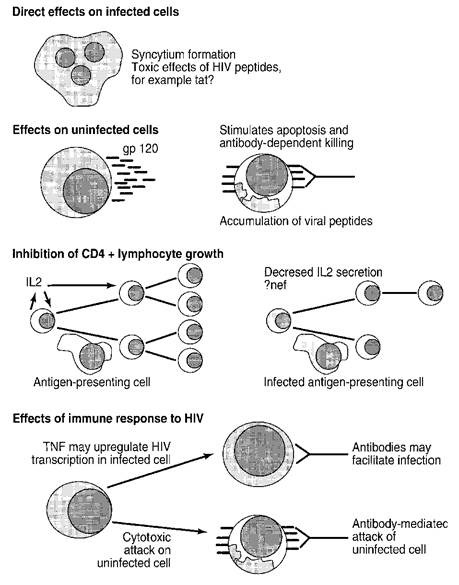
Figure 3.2 Mechanisms of CD4 lymphocyte loss in HIV infection
(b)

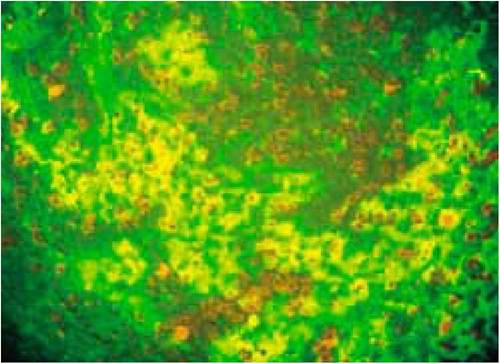
Figure 3.3 (a): Normal lymph node in which B lymphocytes and follicular dendritic cells (green) form a regular network and suppressor/cytotoxic CD8 T- cells (red) populate the paracortical areas. (b): Node from HIV-positive patient with persistent generalised lymphadenopathy which has been infiltrated by many CD8 cells and in which the regular structure has been destroyed.
(c): Same section as middle picture showing complexes of HIV core antigen (orange) and immunoglobulin (red) deposited in germinal centre
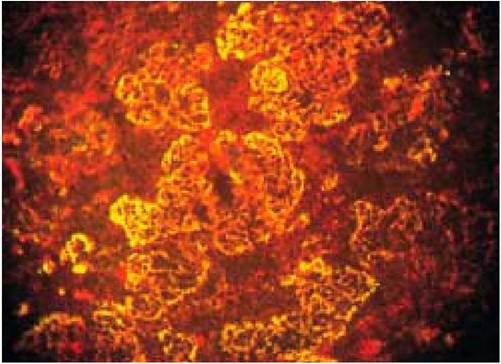
(c)