Malignancies
The prevalence of cardiac Kaposi’s sarcoma (KS) in AIDS patients ranged from 12 to 28% in retrospective autopsy studies in the pre-HAART period [3]. Cardiac involvement with KS usually occurs when widespread visceral organ involvement is present.
The lesions are typically less than 1 cm in size and may be pericardial or, less frequently, myocardial, and are only rarely associated with obstruction, dysfunction, morbidity, or mortality [8]. Microscopically, there are atypical spindle cells lining slit-like vascular spaces (Fig. 4).Non-Hodgkin’s lymphoma (NHL) involving the heart is infrequent in AIDS [15]. Most cases are high-grade B-cell (small noncleaved) Burkitt-like lymphomas, with the rest classified as diffuse large B-cell lymphomas (in the REAL classification; Fig. 5). Lymphomatous lesions may appear grossly as either localized or more diffuse nodular to polypoid masses [16, 17]. Most involve the pericardium, with variable myocardial infiltration [16, 17]. There is little or no accompanying inflammation and necrosis. The prognosis of patients with HIV-associated cardiac lymphoma is generally poor because of widespread organ involvement, although some patients treated with combi-
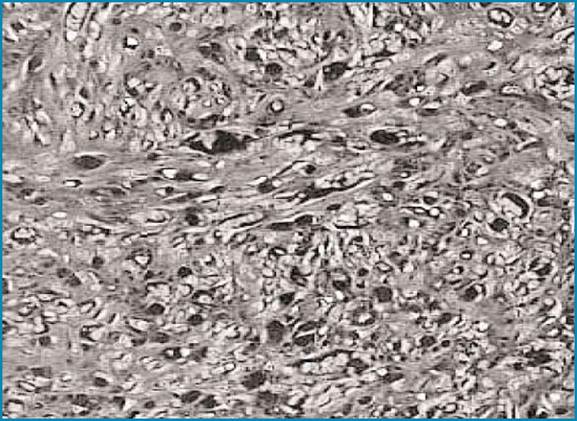
Fig. 4 Myocardial involvement by Kaposi’s sarcoma. Histology shows spindle cells surrounding slit-like capillary vessels. H&E, x40
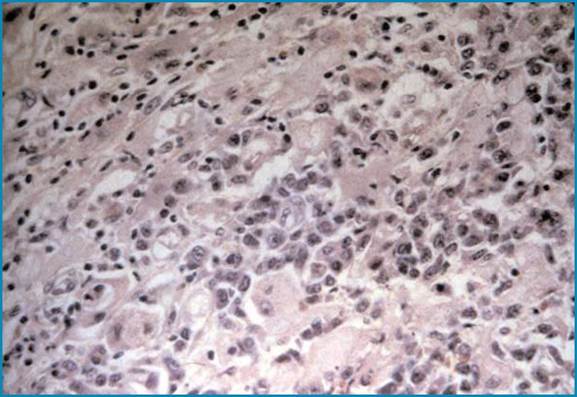
Fig. 5 Myocardial infiltration by large cell non-Hodgkin’s lymphoma, associated with myocardial damage. H&E, x40
nation chemotherapy have experienced clinical remission [18].
The introduction of HAART has reduced the incidence of cardiac involvement by KS and NHL, perhaps attributable to patients’ improved immunologic state and to suppression of opportunistic infections with Human Herpes Virus-8 and Epstein-Barr virus that are known to play an etiologic role in these neoplasms [18].