Management
The aim of any intervention for HIV-infected children should be to maintain the best possible quality of life for the children as long as possible, with the hope that they will be able to take advantage of potential curative therapy in the future.
This inevitably means balancing the potential benefits of new treatments against the need for increased monitoring, possible toxicities and limiting future therapeutic options.As a result of advances in ART, there has been a shift in focus from diagnosing and managing opportunistic infections (OI) to preventing them by restoring and maintaining cellular immunity. For most established opportunistic infections, the best treatment is HAART.
Antiretroviral therapy
Virus replication in children, as in adults, is occurring at all stages of HIV infection and, as improved drugs and drug combinations become available, treatment is likely to be offered increasingly early. Highly encouraging results have been reported with three or more drug combinations in selected, infected infants, which demonstrate that complete viral suppression and maintenance of entirely normal immune development can be achieved and sustained for at least three years. These observations, and studies of adults treated during primary infection, provide a rationale for early aggressive therapy of infants.
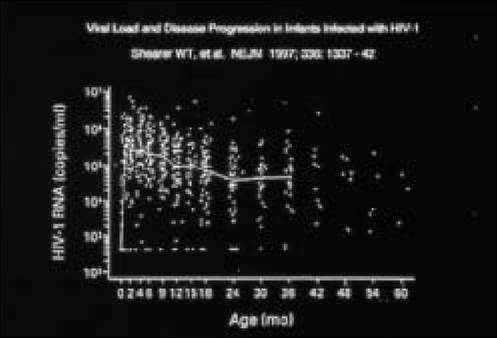
Figure 12.10 Plasma viral load (HIV-l RNA copies/ml) over time in a cohort of perinatally infected, non-breast-fed infants. Solid line represents median values at each time point. Note that median viral load on days 1—3 of life was below the limit of detection (are a potential risk.
It is likely that long-term control of viral replication in children will require adjunctive immune-based treatment, and several approaches are under investigation.
The role of strategic treatment interruptions is also being evaluated. The long-term goal is to restore the child's HIV-specific immune responses to the point where HAART is no longer needed.In view of the many uncertainties regarding optimal treatment, it is strongly recommended that children should be offered treatment as part of a clinical trial. Paediatricians in Europe and Brazil are collaborating in a series of studies coordinated by the Pediatric European Network for the Treatment of AIDS (PENTA). Information about the PENTA studies is available through the Medical Research Council Clinical Trials Centre in London (telephone +44 (0) 20 7670 4791/2, fax +44 (0) 20 7670 4814) or INSERM in Paris (telephone +33 1 4559 5201, fax +33 14559 5180).
Box 12.5 Issues to consider when starting therapy in Children
• Parental (and child) readiness
• Likelihood of good longterm adherence
• What formulations could this child take (taste testing: let child chose)?
• What pharmacokinetic data are available for infants/children/adolescents?
• What experience have other family members had on antiretroviral drugs?
Box 12.6 Drug combinations consider:
• Pill/liquid burden
• Ease of adminstration
• With/without food
• Number of times per day (avoid school hours, ?once daily for adolescents)
• Creative use of drug-drug interactions (boosting with ritonavir)
• Pill-swallowing techniques
• Adherence aids (sticker charts, dosette boxes etc.)
• Gastrostomy tubes to improve quality of life if this is severely eroded by difficulties taking medicines orally
Box 12.7 Recommendations for use of HAART in children (adapted from PENTA, 2001)
• Must start HAART if
Clinical stage C or immunological stage 3 disease (CD4106 RNA copies/ml if age 105 if age over 1 year)
Infant 25%
Low viral load:
the changing needs of infected and affected children and their caregivers. Continuity of care between inpatient and outpatient services, local referring hospitals and the community needs to be developed.
Ideally adults and children should be treated in family-based units. All too often parents will ignore their own health needs because they put their children first.Increasingly the work of the multidisciplinary team has shifted towards ways of helping families achieve long-term adherence to HAART. As children survive longer, meeting the needs of adolescents and planning transition to adult clinics is placing new demands on services.
The decision as to who should be informed should be tailored individually. Families may need help in explaining the diagnosis to older children. This needs to be undertaken at the child's pace, and is frequently most effectively achieved in gradual steps. It is not mandatory to tell staff at schools, as universal precautions should be employed for all children with cuts and abrasions. The risks of transmission from casual contacts in school or day care settings are virtually nil. Ensuring that adolescents are well informed and responsible before they become sexually active themselves is a priority.
The child's developmental needs require careful monitoring and support, with access to a clinical psychologist, a physiotherapist, occupational therapist and speech therapist.
The multidisciplinary team should include a dietician, as nutritional problems and growth faltering are very common complications. Balanced supplements are sometimes required and enteral feeding through gastrostomy tubes and occasionally intravenous parenteral feeding may be necessary. Gastrostomy tubes have been used with success to allow unpalatable medicines to be given, even when they were not required for nutritional supplementation.
Because children below the age of eight years very rarely complain of symptoms of unilateral eye disease, regular monitoring of young children with CD4 counts less than 5% by a paediatric ophthalmologist is desirable. Chorioretinitis due to CMV is usually treated by intravenous induction therapy with ganciclovir followed by regular maintenance intravenous treatment five days per week.
Paediatric formulations of oral ganciclovir are poorly bioavailable. Intravitreous injections and, in older children, implants have been used.Pain management is of critical importance in late-stage disease. Complementary therapies such as therapeutic touch and aromatherapy may be useful and require evaluation. It is a testament to the success of HAART that very few children in industrialised countries are needing palliative or terminal care. However unless new treatment strategies become available, the next few years may see some children running out of therapeutic options.
Prevention remains the top priority in managing HIV infection in children. Reducing national perinatal transmission rates to below 2% is an achievable target that can only be realised if HIV-infected mothers can be identified prenatally and offered appropriate interventions. This will require continued effort by health professionals, public health planners and community organisations.
13