Pericardial Disease
Pericardial Effusion
Pericardial effusion is the most frequent complication in HIV-infected patients. Before the introduction of HAART therapy, its frequency varied from 5 to 46% with an incidence of 11 to 17%/year and was associated with a high mortality rate [5].
Most cases remain of undetermined origin despite an extensive work-up. The cause of pericardial effusion in industrialized countries is idiopathic; in contrast, mycobacterium is the main agent involved in pericardial effusion in Africa (86%) [5] and spontaneous resolution could occur in 42% [6].In the pre-HAART era, pericardial effusion was more common in patients with HIV advanced disease. Clinical manifestation of pericardial disease varies from asymptomatic pericardial effusion to cardiac tamponade.
Echocardiography is the non-invasive reference and accurate tool for the diagnosis of pericardial disease and tamponade. The echocardiographic diagnosis of pericardial effusions is usually based on visualization of a sonolucent circumcardiac space of varying width with or without hemodynamic compromise (Fig. 1).
Heidenreich et al. [6] described the incidence of pericardial effusion and its relation
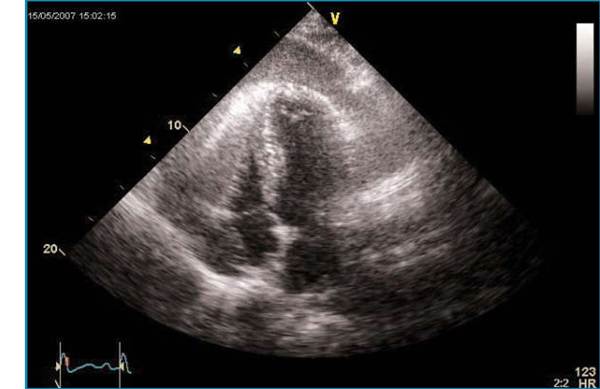
Fig. 1 Apical four-chamber view in an HIV infected patient showing a large and circumferential pericardial effusion
to mortality in HIV-positive subjects. In this study including outpatients, the prevalence of effusion in AIDS subjects was around 5%. The vast majority (80%) were small asymptomatic effusions, without any hemodynamic compromise. Survival of AIDS subjects with pericardial effusions was significantly shorter than AIDS subjects without (36 vs. 93% at 6 months, p32 mm/m2 in diastole) associated with impaired ventricular systolic function, assessed by impaired left ventricular ejection fraction (LVEF stage and no LV systolic dysfunction [21].
In sub-Saharan Africa, dilated cardiomyopathy remains an important issue. Out of 416 HIV-infected patients not receiving HAART, dilated cardiomyopathy was documented by echocardiography in 17.7% of patients. Low socio-economic status, estimated duration of HIV-1 infection, CD4 count, HIV-1 viral load, CDC stage B and C of HIV disease and low plasmatic level of selenium were significant predictors of LV systolic dysfunction [24].
Cardiomyopathy could also be secondary to drug toxicity such as zidovudine, amphotericin B or foscarnet [25]. The exact mechanism and pathogenesis of dilated cardiomyopathy in HIV patients is not unique. Nutritional disorders, direct effect of HIV on the heart, toxic effect of antiretroviral drugs, increased cytokine activity, opportunistic infection, illicit drug abuse, autoimmune reaction have been associated with dilated cardiomyopathy in HIV patients [21]. HAART has significantly decreased the incidence of dilated cardiomyopathy from 8.1 to 1.8% [8].