Preventing Transmission during Home Care
Home care means living with or caring for someone with HIV infection. It does not include sexual contact. These guidelines are based on recommendations by the CDC and on extensive experience with home care and hospital care.
You should know that these recommendations are intentionally overcautious.Reality of the Risk
There is no risk associated with simply living in the same household or working in the same office with a person who has HIV infection. This generally involves the types of nonintimate contact previously referred to as “casual contact” (see above, under “Types of Contact”). The type of contact that might involve the risk of transmitting HIV nonsexually usually takes place during medical care in the more advanced stages of disease. Every health care worker who has acquired HIV infection non- sexually has been exposed to the blood or bloody fluids of a person with HIV infection; transmission usually occurs after health care workers inadvertently inject infected blood into themselves.
The type of contact involved in home care of a person with HIV infection carries, in CDC’s extensive experience, almost no risk. Only about eight of the tens of thousands of people who provide home care for people with HIV infection have acquired HIV as a result of nonsex- ual contact. Most of the people who did not become infected provided complete care of people with HIV infection for many months or even years without the benefit of any special training and without any special precautions to prevent HIV infection. Nevertheless, we recommend that caregivers use some simple precautions to be extra safe.
How can we be sure these are the only eight exceptions? We obviously cannot, although most physicians question people with HIV infection for type of contact, and any physician would promptly report contact through home care because of its importance as a public health issue.
Testing the blood of people who are caregivers of people with HIV infection answers the question more formally: fourteen studies of well over one thousand caregivers have not identified any additional people who acquired HIV infection by nonsexual contact.In short, for those who live in the same household and do things that are common for friends and relatives to do, the risk is nil. For those who care daily for people who are seriously ill, the risk is very low, but not zero.
Guidelines for Preventing Transmission of HIV during Home Care
People with HIV infection and those involved in their care will want to lower the already low risk of transmission. This is easily accomplished by using the basic and simple guidelines described below.
Handwashing. Handwashing is an important way to prevent the spread of most infectious microbes, not just HIV. Nevertheless, alcohol wipes are more effective than soap at killing viruses.
Table 2. Sources of HIV Infection in the Estimated 1.5 Million Americans Thought to Have This Disease
| How Transmitted | Est. No. in U.S. | Body Fluid | Comments |
| Sexual contact | 1,000,000 | Genital secretion | Gay men account for 40% of all AIDS cases, although heterosexual transmission accounts for 29% of new cases in 2002 |
| Injecting drugs | 400,000 | Blood on shared needles | 95% are regular users (more than 1 time/week); 5% are occasional users; together they account for 27% of all new cases reported in 2002 |
| Blood transfusions | 40,000 | Blood | Largely stopped in 1985 due to screening of blood donors; accounted for 0.2% of new cases in 2001, most of which were infected before 1985 |
| Hemophilia | 10,000 | Blood products | As above; about 20 documented cases since April 1985 (less than 1/1,000/year) |
| Infants | 8,700 | Mother to fetus | Rates substantially reduced due to HIV drugs given to pregnant women; accounted for 90 (0.2%) new cases reported in 2002 |
| Health care workers with exposures in the workplace | 57 | Blood | These are the only well- established cases reported through 2005; about 130 additional cases are less well established |
| Organ transplant recipients | 38 | Blood or organ tissue from donor | This group largely stopped due to screening of donors; the exception is 7 cases from |
(continued)
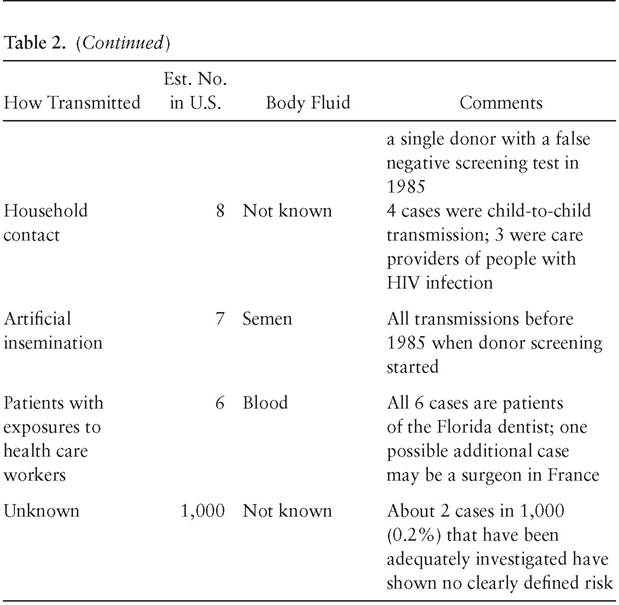
Note: Data are based in part on estimates by the U.S.
Public Health Service for 2004. The Comments column refers to cases reported since April 1985, the date when the blood test first became available for screening blood and organ donors. The estimated total in the U.S. is 1.5 million people infected with HIV, including 1 million living with HIV infection and 500,000 who have died with AIDS.Gloves. Wear latex gloves if your hands have any cuts, sores, or torn cuticles. Wear gloves to handle blood or feces or urine, or to clean open sores. Wear gloves for cleaning surfaces that have been soiled by blood or feces or urine. Following use, soiled gloves should be washed with soap and water, then dried, and then discarded in a plastic container such as a trash can lined with a plastic bag.
Disinfectants. No one is known to have become infected from contacting HIV on a surface outside the body. Nevertheless, this virus has been shown to survive on a surface for several days, and it is probably wise to clean up blood or other body secretions on clothing or hard surfaces. Studies show that HIV is killed by heat and by nearly all chemical disinfectants.
The most commonly used disinfectants include household bleach and alcohol (70% isopropyl). Other disinfectants that are effective include hydrogen peroxide, iodophors, phenolics, and quaternary ammonium compounds. These disinfectants are readily available in pharmacies and grocery stores. They are registered with the Environmental Protection Agency (EPA) with directions for use and precautionary information.
The most common disinfectant used is sodium hypochlorite, commonly known as household bleach (the most common brand is Clorox). This is available as a 5.25 percent solution wherever household cleaning products are sold. Household bleach kills a broad range of microbes, including HIV. To clean surfaces contaminated by blood or secretions, use a 1:10 dilution. A 1:10 dilution contains one part of 5.25 percent household bleach and nine parts of tap water (for example, one-fourth cup bleach and two and one-fourth cups water).
Leave the 1:10 dilution on the surface for ten minutes, then wipe it off.If the surface is cleaned before using the bleach, a 1:100 dilution may be used. Some people find it convenient to use the 1:100 dilution of bleach in a spray bottle, to spray on surfaces after they have been wiped clean. Bleach may corrode metals. It may also damage electrical and electronic equipment. Undiluted, it can leave white spots on fabric or eat holes in fabric. Contact with the skin and especially the eyes should be avoided. Use gloves to protect the skin when cleaning and disinfecting with bleach. If bleach comes in contact with skin, eyes, or mouth, the area should be washed or rinsed thoroughly with water. This applies to undiluted bleach and to the 1:10 dilution. Inhaling bleach fumes should also be avoided.
Household bleach may be stored in the original container (or in any opaque container) in a cool area, for up to a year. Bleach in solution is unstable and loses potency when exposed to sunlight, heat, or metal. Diluted bleach solutions should be used within a day or discarded.
Seventy percent isopropyl alcohol is also a very effective disinfectant. One problem with its use on surfaces is that it evaporates quickly. It may also cause skin irritation. This is the usual disinfectant ingredient in waterless handwashing products that are marketed in sealed packets. Isopropyl alcohol need not be diluted before use. Undiluted isopropyl alcohol kills high concentrations of HIV in less than one minute.
Hydrogen peroxide is usually sold in a 3 percent solution, which is too weak to disinfect. Iodine is an adequate skin disinfectant, but it must be used carefully, since it stains fabrics, corrodes metal, cracks plastics, and dissolves rubber.
In summary, the most practical disinfectant to keep on hand is household bleach. Bleach should be properly stored and clearly labeled to avoid misuse or accidental drinking. In addition, 70 percent isopropyl alcohol can be used to clean cuts or other open wounds.
Dishwashing. There is no reason to provide separate dishes, glasses, or silverware for people with HIV infection. Washing dishes in a standard dishwasher or in hot soapy water is adequate.
Laundry. Laundry should be washed with detergent, using the hot cycle. Adding one-third cup of household bleach per ten gallons of wash water will assure disinfection, although it is really not necessary and may damage some fabrics. Fabrics that are soaked with blood or other body secretions should be presoaked and then washed separately. Dry cleaning will disinfect any fabric.
Cuts and other injuries. Any fresh bleeding cut or sore on the caregiver or the person with HIV infection should be wiped free of blood and washed with soap and water or with alcohol (70% isopropyl).
Blood spills. Blood, including menstrual blood, spilled on a surface should be cleaned by a person wearing disposable gloves and using disposable cleaning cloths. After wiping up the blood, clean the area with a disinfectant like household bleach in a 1:10 or 1:100 dilution. Sponges, mops, and fabrics that have blood or body fluids on them may be cleaned with soap and water or with bleach in a 1:10 dilution.
Disposal of waste. Liquid waste that may have HIV in it can be poured into the toilet or sink. This will not contaminate the sewer system: sewage is decontaminated using methods that are clearly adequate to kill HIV and virtually all other microbes as well.
Soiled materials such as bandages, sanitary napkins, disposable gloves, soiled cleaning cloths, and the like should be placed in plastic bags for disposal. This is important primarily when they are soiled with blood. Sharp instruments such as needles, syringes, used razor blades, and broken glass should be placed in containers such as a metal coffee can for disposal. To be extra cautious, some health departments recommend also adding bleach to the container.
To summarize: Caregivers should be cautious and sensible but should not worry excessively.
In fourteen years, of all the people who are and have been caregivers, only eight are thought to have become infected by nonsexual contact.Preventing Transmission of Infections Other Than HIV
People with HIV infection are susceptible to infection by a multitude of other microbes. These microbes cause what are called opportunistic infections or more simply, complications. The most common complications are pneumocystis pneumonia, thrush, infection disseminated throughout the body caused by either cytomegalovirus or Mycobacterium avium complex, and a brain infection called toxoplasmosis. (These and other complications are discussed at great length in chapter 6.) People commonly want to know whether the caregiver can also be infected by these complications. The short answer is: with rare exceptions, no.
Most of these complications are caused by microbes that we all come in contact with every day. People with HIV infection usually do not develop complications until relatively late in the disease after their immune systems have become profoundly impaired. The caregiver’s immune system does not permit such organisms to flourish. In other words, none of these complications can be transmitted from the person to the caregiver either in the home or in the hospital.
Pregnant caregivers are sometimes worried about exposure to people with cytomegalovirus, but most authorities believe these concerns are unjustified (see the section on cytomegalovirus in chapter 6).
In fact, the person with HIV infection is not a significant source of complications even for another person with HIV infection. The reason is that most of these microbes are and always have been everywhere around us, and everyone has been exposed to them for a long time.
Exceptions to the rule. Some infections may be transmitted to the caregiver, and to avoid these infections, the caregiver should use special precautions.
The most important exception is tuberculosis, which is caused by a bacterium called Mycobacterium tuberculosis. Mycobacterium tuberculosis is related to another bacterium that people with HIV infection are prone to, Mycobacterium avium complex, or MAC, which causes infections throughout the body. MAC is not contagious—that is, it cannot be spread from person to person. Mycobacterium tuberculosis, however, is contagious.
Tuberculosis has always been recognized as a contagious disease. People with HIV infection are exceptionally vulnerable to infection with tuberculosis, and, once infected, they get the disease severely. Moreover, some of these people are infected with a strain of the TB bacterium called the “multiply drug-resistant strain,” that is, a form of the TB bacterium that does not respond to the usual drugs. The multiply drug-resistant strain was a big problem among people with HIV infection, especially in New York City in the early 1990s, but both TB and multiply drugresistant TB are now much better contained.
All people in the same household as someone with tuberculosis are at special risk. The risk is highest during the period before diagnosis and treatment. This is equally true for people in the household of someone with tuberculosis and HIV infection. People not in the household—visitors, co-workers, casual friends, golf partners, and the like—are not usually considered to be at risk, but this depends to some extent on the type of contact. In any case, people usually become infected by inhaling the droplets in the air after the infected person has coughed.
Whenever a case of tuberculosis is detected, medical authorities evaluate others in the same household. The evaluation starts with a skin test. Because the skin test can take three months to become positive, sometimes treatment is started immediately. And treatment is often started immediately for any children in the household. If the skin test for tuberculosis is positive, the evaluation proceeds to the next step, a chest X-ray. Once tuberculosis is treated with drugs, the infected person rapidly becomes noncontagious. For this reason, the main threat of tuberculosis comes from the person whose tuberculosis has not yet been detected or treated.
People infected with the resistant strain of tuberculosis, which persists in spite of treatment, are an exception. These people require special care and may need to stay in the hospital for prolonged periods. And because the resistant strain of tuberculosis is a major threat to public health, people may even be kept in the hospital against their wishes.
Another infection that is an exception is hepatitis B. Most people with hepatitis B are not aware they have it; they develop antibodies to it and are subsequently protected from infection. However, about 5 or 10 percent of people with hepatitis B will develop a persistent infection, and therefore may infect others for many years. Some people with persistent hepatitis will develop a liver disease called chronic active hepatitis that may eventually result in cirrhosis.
The virus that causes hepatitis B is transmitted the same way HIV is: by sexual contact, by blood contact, or by passage from mother to infant. Therefore, the activities that carry a risk of infection with HIV also carry a risk of infection with the hepatitis B virus. People at greatest risk for hepatitis B are men who have homosexual sex, people who use drugs by injection, and men who have hemophilia. Like HIV, hepatitis B may be also transmitted to someone exposed to the blood of an infected person.
Hepatitis B has four features worth emphasizing:
1. Hepatitis B virus is transmitted much more efficiently than HIV. A needlestick injury with blood that contains the hepatitis B virus is twenty times more likely to transmit hepatitis B than a needlestick injury with blood that contains HIV is to transmit HIV infection.
2. The same guidelines for preventing transmission of HIV through blood and body fluids apply to preventing transmission of hepatitis B.
3. A vaccine can prevent infection by the hepatitis B virus. The hepatitis vaccine is readily available, though it is expensive; it costs about $160 for three injections. Those people who live in the same house as the person with hepatitis B should take the vaccine if they have not already been infected.
4. Hepatitis B can now be treated with several drugs—interferon, lamivudine, adofovir, and entecavir—which all help control the hepatitis B virus. The results of the treatment, however, are quite variable, the medicines (especially interferon) can cause side effects, and the virus may become resistant.
Outside of tuberculosis and hepatitis, the infections that could conceivably be transmitted from the person with HIV to a caregiver are salmonellosis, herpes simplex infection, herpes zoster infection, and cryptosporidiosis. If the caregiver is otherwise healthy, these infections may cause a temporary disease that is not serious.
Salmonellosis is an infection of the intestine by bacteria called Salmonella. The main symptom of salmonellosis is diarrhea. Salmonellosis is relatively unusual, and transmission to others is relatively infrequent.
Cryptosporidiosis is also an infection of the intestine but is caused by a parasite. The main symptom of cryptosporidiosis is also diarrhea. It is transmitted by lapses in personal hygiene; that is, small amounts of feces on the hand carry the parasite to someone else’s hand, and then to that second person’s mouth.
Herpes simplex, usually known as “herpes,” causes a blister on the skin, most commonly on the mouth or genitals, though people with advanced HIV infection can also have herpes over much of their bodies. The caregiver can get herpes by touching the blisters, and can avoid transmission easily by wearing gloves when touching the areas with sores until the sores are crusted over.
Herpes zoster, also called shingles, is caused by the virus that causes chickenpox. The virus is transmitted when people inhale it. However, most older children and adults have had chickenpox, even if they don’t remember it, and thus are protected by antibodies against the virus. Those who are concerned about herpes zoster are urged to have a blood test to see if they have antibodies to herpes zoster; and to be safe, they
should avoid going into the same room as the infected person until the sores are crusted over. They might want to take the new chickenpox vaccine, which is highly effective.
All these infections are discussed in greater detail in chapter 6.
Preventing Transmission of Infections to the HIV-infected Person
Both health care workers and home caregivers are understandably worried that they might transmit infection to the person whose immune system has been damaged by HIV infection. Although this worry sounds rational, in reality it is not much of a problem.
The kinds of infections common in otherwise healthy individuals include upper respiratory tract infections like colds, sinusitis, and pharyngitis; influenza or “flu”; gastroenteritis with diarrhea, vomiting, and fever; and skin infections. Some of these sound like infections, but in reality they are not. Some are infections that are not contagious and cannot be passed from one person to another. And some are contagious diseases in the usual sense. The latter category is the only important one. The most common examples are colds, bronchitis, influenza, and gastroenteritis. Most of these are caused by viruses.
However, people with HIV infection do not get these common contagious diseases any more frequently or any more severely than anyone else. The viruses that cause the common contagious diseases affect a person with HIV the same way they affect other people. The reason seems to be that the part of the immune system that HIV attacks is not the same as the part that defends against colds and flu.
People also worry whether pets can carry infections to people with HIV infection. The most common worry is about the Toxoplasma gondii parasite, which causes a brain infection called toxoplasma encephalitis. The parasite is commonly found in the stool of cats. This worry is probably not justified: Toxoplasma gondii is one of those microbes that 2030 percent of all people have in their bodies, and the person with HIV infection who gets toxoplasmosis has probably had this microbe a long time.
If You Think You Have Been Exposed
Persons who think they have been exposed to HIV infection or any of the infections noted above should seek care at a site that offers a treatment called “nonoccupational exposure prophylaxis.”
Health care workers who have been exposed to HIV are usually offered two nucleosides. Previous experience with one particular nucleoside reduced the risk of transmission by 80 percent, and other nucleosides are thought to be equally good. A third drug is added if the exposure was to a large amount of virus or if the injury was deep. When the drugs are taken for this reason, they must be started as soon as possible, and certainly within 72 hours of exposure.
We usually start treatment within 2 hours of exposure and think that much of the opportunity to prevent HIV transmission is gone when treatment is delayed over 24 hours. The drugs are taken for one month. HIV blood tests are done before treatment and at three months, and again at six months after exposure.We want to see whether the test turns positive and transmission has indeed taken place.
The CDC’s 2005 guidelines for people exposed to HIV by sex or shared needles are based on the experiences of health care workers exposed to HIV occupationally. Basing the guidelines for one group on the experiences of another is not backed by scientific evidence, but it should work anyway. People seeking treatment should have been exposed by sex or needle-sharing with someone who has or probably has HIV infection; and they should be able to begin treatment within 72 hours after the time they were exposed. Treatment begun even sooner is better: health care workers who were exposed occupationally and who received treatment within 2 hours of exposure had an 80 percent reduction in transmission. The treatment regimens recommended are the same as those used for health care workers exposed to HIV. One drug to avoid is nevirapine (Viramune), because of its possible liver toxicity. Another drug, efavirenz (Sustiva), should not be given to pregnant women or women who may become pregnant, because it possibly causes birth defects. People who receive the treatment regimen need to be aware that it has side effects and that it will cost between $500 and $1,200, depending on the regimen. The standard course of treatment takes one month, but the drugs can be stopped immediately if the person who was the source of the exposure is given an HIV test that turns out to be negative.