Problems Affecting the Whole Body
Symptoms that affect the whole body, or constitution, are called constitutional symptoms. Constitutional symptoms are the vague, general symptoms that often accompany chronic illnesses.
Included are weight loss, chronic weakness, diarrhea, night sweats, fever, lethargy, malaise, and fatigue. All these symptoms are relatively common both in the general population and in people with HIV infection. Some of these symp- toms—fatigue, lethargy, malaise—are subjective and difficult to measure. Others—fever, severe weight loss (wasting)—are more objective. These symptoms can be considered the constitutional symptoms of HIV infection only when they have been present for at least one month.People with HIV infection tend not to have constitutional symptoms until the CD4 count is below 200, unless they are also depressed or have some unrelated medical problem like influenza. In people with HIV infection, the distinguishing feature of all of these constitutional symptoms is that they are chronic; that is, they don’t go away. Any of these symptoms may also be caused by certain complications. Because some of these complications are treatable, when these symptoms develop, see a physician.
Three of these constitutional symptoms—fatigue, fever, and wasting — deserve additional discussion.
Fatigue
Fatigue is an especially common constitutional symptom. Its severity is often profound and its causes are diverse. Likely explanations are infections, depression, anemia (low red blood cell count), and HIV-associated dementia. Many cases of fatigue, however, have no clear cause and can be blamed on HIV infection itself. This is true only when the CD4 cell count is low. Fatigue from HIV infection is uncommon and not severe when the CD4 count is over 200; it is common and rarely severe when the CD4 count is between 50 and 200; and it is common and often severe when the CD4 count is below 50.
HIV infection causes fatigue partly because it deprives the body of some of its sources of energy. People with HIV infection often have anemia, or lower numbers of red blood cells. Red blood cells, among other things, carry oxygen; oxygen supplies the muscles with energy. People with fewer red blood cells therefore have less energy and tire easily, though the anemia must be severe before people notice symptoms.
In addition, people with HIV infection and fatigue sometimes experience severe weight loss, referred to as “wasting,” because they’re not taking in enough calories. Some of the weight loss of wasting may result from the loss of muscle protein, called protein-calorie malnutrition, and some wasting may be the result of the direct action of cytokines, proteins that regulate the immune system (see below, “Weight Loss or Wasting”). For some people, fatigue is caused by chronic serious infections like MAC or CMV.
Medications can also cause fatigue or sleepiness, which is often interpreted as fatigue. These medications include, among others, narcotics, antihistamines, and antidepressants. AZT may cause fatigue. Fatigue accompanied by nausea, vomiting, and stomach pain may come from lactic acidosis, a potentially serious side effect of the nucleoside drugs like AZT, ddI, and d4T. This can occur after months or years of taking these drugs, and the CD4 count may be high or low.
Fatigue is also an indirect result of HIV infection. In this case, it may be accompanied by weight loss, fever, and night sweats. These symptoms are most likely to occur relatively late in the course of the infection when the CD4 count is low in people who either do not take HAART, or who take it and don’t respond.
A medical evaluation can help sort out the cause of fatigue. A simple blood count will show if the cause is anemia. Blood tests will indicate if the cause is lactic acidosis due to AZT, ddI, or d4T; lactic acidosis is extremely important to recognize because it can be lethal.
Such symptoms as fever, cough, and diarrhea often accompany HIV infection’s complications. Most causes are treatable.For more on dealing with fatigue, see chapter 4, “HIV Infection and Its Effects on the Emotions,” under “Fatigue and Accommodation.”
Fever
Fever, like other constitutional symptoms, is common; it can be caused by a complication of HIV infection, or it can simply be due to HIV.
Most people with fever are aware of it. Rapid rises in body temperature are commonly preceded by chills. Chills are an indication of the body’s attempt to retain heat by constricting the blood vessels of the skin where heat is given off. People with fever cannot tolerate the usual range of heat and cold that most people consider normal room temperature. Along with fever, some people also have “night sweats,” sweating at night that can be severe enough to require changes in bed clothing. In people with HIV infection, fevers often begin gradually, occurring off and on for extended periods of weeks or months.
Temperature is measured on two scales: the Fahrenheit, or F scale, commonly used in the United States, and the centigrade, or C scale, used in the rest of the world and in some hospitals in the United States. A temperature of 98.6 degrees F corresponds to 37 degrees C; 99.6 degrees F corresponds to 37.5 degrees C.
The average temperature is 97 degrees F at 3:00 a.m. and 99.3 degrees F at 5:00 p.m. In general, temperatures are about two degrees higher (on the Fahrenheit scale) in the late afternoon than they are in the morning. This daily fluctuation in temperature is exaggerated during fever. For this reason, people with HIV infection who think they have fever should take their temperatures several times during the day, when they feel feverish, and in the late afternoon.
Physicians always want to know when a person with HIV infection has a fever: fever is an objective indication of a problem that is not just a day-to-day variation in health status. Prolonged fever accompanied by chills in people with low CD4 counts indicate the presence of some infection other than HIV.
If you have such a fever, see a physician; at least 80 percent of fevers in people with HIV infection occur with an infection that can be diagnosed and treated. Fever with a low white blood count (neutropenia) or a line inserted in a vein for receiving intravenous antibiotics can indicate a serious bacterial infection that requires immediate medical attention.In people in the late stages of HIV infection, the conditions that are most likely to cause persistent fever are tuberculosis, Mycobacterium avium complex infection, cytomegalovirus infection, fungal infection, pneumocystis pneumonia, toxoplasmosis, cryptococcosis, and pneumonia. In people with CD4 counts over 200, the common causes of fever are the same conditions that cause fever in anyone—flu, pneumonia, or gastroenteritis. Drugs may also cause fever. Nearly all drugs may do this, but those that do it most commonly are sulfa drugs like trimethoprimsulfamethoxazole (Bactrim or Septra) and dapsone. Other drugs that can cause fever include amphotericin B, phenytoin (Dilantin), barbiturates, thalidomide, pentamidine, clindamycin, and penicillin. One drug, aba- cavir (Ziagen) may cause fever that is especially important to recognize because it may be a particularly serious side effect requiring discontinuance and careful avoidance in the future. When a drug causes fever, the fever is almost always accompanied by a rash: exceptions are amphotericin B and pentamidine. The best way to tell if the drug is the cause is to stop suspected drugs and see if the fever disappears, which usually occurs within 24 to 48 hours.
Fever is basically treated by treating whatever is causing it. Treating fever itself is a little controversial. Fever actually has advantages: the immune system works better at higher temperatures, and fever is an important indicator of the course of the disease and of the effectiveness of treatment. But fever is also unpleasant for the person who has it and increases the metabolic rate, burning more calories and making good nutrition more difficult.
Otherwise, there is little evidence that fever is harmful.When the decision is made to reduce fever, the usual drugs are aspirin, acetaminophen, or ibuprofen. Acetaminophen carries on the label a warning that it causes liver or kidney damage; although the probability of this is low, it might be best to limit the amount of acetaminophen you take. The maximum adult dose is 0.6 to 0.9 mg (usually two or three pills) taken every four to six hours. The fever decreases or disappears when people take one of these drugs, but returns when the effect of the drug wears off. For people with persistent fever, these fluctuations in temperature can be more unpleasant than a steady, if high, temperature. For this reason, people with persistent fevers are often advised to take these drugs regularly, every four to six hours, without waiting for the fever to recur.
Weight Loss or Wasting
Wasting is the somewhat unfortunate term given to unintentional loss of 10 percent of the body weight, with no explanation other than HIV infection. Wasting once accounted for 20 percent of AIDS diagnoses, but now in the HAART era, it is rare. In general, wasting is seen only in the late stages of HIV infection, in people whose CD4 counts are less than 100 and whose response to HAART is poor. The exceptions to this are wasting due to depression, medications, health conditions unrelated to HIV infection, or early complications of HIV infection like TB or lymphoma. Wasting accompanied by a 25 to 30 percent loss of body weight is considered a medical emergency requiring immediate evaluation and treatment.
Wasting results from one of two problems: inadequate nutrition or metabolic changes. Inadequate nutrition simply means starvation: the body does not get enough nutrients because the person is not eating enough nutrients or is losing too many nutrients. The cause might be loss of appetite, depression, sores in the mouth or esophagus, loss of the sense of taste, or the side effects of drugs.
Some people lose weight because of vomiting or severe diarrhea: the food goes through the digestive system without being absorbed.Metabolic changes can be caused by fever, by an imbalance in hormones called cytokines, by any active complication, and by HIV infection itself. All increase the body’s metabolic rate: the motor runs more quickly and calories are burned at a faster clip. For instance, fever increases the rate at which the body metabolizes food by 7 percent for each degree F. So a person with a temperature of 103 degrees F through the day will increase the calories needed by 30 percent. People with increased metabolic rates may eat voraciously and still lose weight. The average 160-pound man requires 1,700 to 2,100 kilocalories to maintain basal metabolism, but a person with untreated HIV infection requires 2,700 to 3,600. People with HIV infection consequently need to eat more.
Many men with HIV infection, especially in the late stages, produce low amounts of testosterone, which can cause fatigue, loss of libido, and wasting. The test is a measurement of the level of testosterone in the blood. The treatment is the hormone, given as an injection, a skin patch, a pill, or an ointment.
The weight loss associated with wasting is different from the weight loss that accompanies dieting. People who are dieting lose fat but preserve muscle and protein. People who have wasting lose muscle pro- tein—a condition known in medicine as protein-calorie malnutrition. For many people, the weight loss is a stair-step phenomenon—an infection with weight lost, then control of the infection with weight stabilized at a lower level, then another infection with weight lost, and the same process over again.
People with uncontrolled HIV infection often worry about wasting, and want advice on preventing it. The best ways are to control HIV with antiretroviral therapy, use the appropriate preventive antibiotics when the CD4 cell count is low, and take in enough calories. Beyond that, we don’t know how to prevent wasting. The usual advice is to do what is most logical to preserve muscle protein: eat a balanced diet with adequate amounts of protein, and exercise moderately to maintain or build muscles. Foods that contain protein include meat, fish, poultry, eggs, nuts, and peanut butter. The preferred exercises are activities that both build endurance and maintain muscle: walking, jogging, swimming, or bicycling. Strenuous exercise, like Olympic-type training or marathons, is unnecessary and may even harm the immune defenses. Resistance exercise—weight-lifting exercises that require you to resist the pull of gravity—for 20 minutes three or four times a week will maintain strength and preserve or increase weight.
Otherwise, the treatment of wasting depends on the cause: no single treatment is universally effective. Loss of appetite may be treated with drugs like Megace or Marinol; much of the weight added with these drugs, however, is simply fat, and not protein. Cytokine imbalance requires drugs like growth hormone or thalidomide; growth hormone costs over $200 a day and thalidomide is hard to get. Depression requires antidepressive drugs, which are usually effective. Men with wasting often have low testosterone levels and benefit from treatment with testosterone or anabolic steroids; some women do also.
Sores in the mouth or esophagus—like thrush, oral hairy leukoplakia, or herpes—should be treated with antibiotics, and the person should eat foods that are soft, easy to swallow, and bland. Diarrhea requires drugs like Lomotil, loperamide, or paregoric to slow the intestine, antibiotics to treat infections, or dietary modification. Nausea and vomiting require small frequent meals of food that is not aromatic and is easily digested; nausea and vomiting can also be treated with drugs. Fever requires aspirin, acetaminophen, or ibuprofen and drugs to eliminate the cause of the fever. Rapid weight loss during late-stage AIDS often indicates a chronic infection, like CMV, herpes simplex, tuberculosis, or Mycobacterium avium. In these cases, the most important treatment is to control the underlying infection.
Many people have difficulty maintaining nutrition because of the demands of the drugs of HAART and their side effects. For instance, indinavir (Crixivan) and ddI both must be taken on an empty stomach, but they can’t be taken together, so deciding when to eat can be a problem. Some of these drugs cause nausea, which also confounds nutrition. The key is to discuss these issues with your physician, since an alternative schedule or an alternative regimen may be possible. For more about all these treatments for wasting, see above, “Problems of the Digestive System.”
In general, cater to individual tastes, eat small and frequent meals, and eat foods that contain a lot of calories and protein. For the short term, anyway, don’t worry too much about a balanced diet and eat snack foods that carry large numbers of calories: peanuts, peanut butter, nuts, raisins, sunflower seeds, M&Ms, Oreo cookies, pizza, milkshakes, potato chips, Fritos, macaroni and cheese, Big Macs, most candy bars, fudge sundaes, marshmallows, and many others. Try asking a licensed dietitian. Also ask about exercise training. Men should ask about testosterone.
When people cannot eat enough to compensate for losses, supplements will help. Supplements like Ensure, Ensure Plus, Jevity, Criticare, Peptamen, or Perative, which can be obtained in grocery stores and pharmacies, provide a rich source of calories and protein. The various supplements are similar in nutritional value. These supplements are commonly recommended for wasting, but some—Ensure Plus, Criticare, and Peptamen—actually cause diarrhea and should be diluted before using. If the supplements are taken in addition to meals, the person will need a few cans a day. If the supplements are the only nutrition the person is getting, the person will need about ten cans a day. Most people don’t try to get all of their nutritional needs with these supplements, but they use them to supplement a diet of foods that are more pleasurable and diverse.
When people have problems that prevent the small intestine from absorbing food, different supplements, which are predigested and ready to absorb, will help. Supplements like Vivonex T.E.N. cost about $6 to $8 per can. If these supplements are taken in addition to meals, people will use three to six cans a day; if the supplement is the only source of nutrition, the person will need six to nine cans a day.
All nutritional supplements are available without prescription. But if a prescription is written nevertheless, Medicaid and some insurance plans will cover the supplement’s cost.
On the rare occasions when the intestines quit digesting and absorbing food, nutrients might need to be provided by vein—a procedure called parenteral (meaning by vein) hyperalimentation. This is expensive—in fact, extraordinarily expensive—and costs over $10,000 per month. Most physicians prefer to use parenteral hyperalimentation for only a week or two to get past a temporary problem, though occasionally they use it for longer periods for uncontrollable diarrhea caused by cryptosporidiosis.
Causes of Constitutional Symptoms
The causes of constitutional symptoms are diverse. Sometimes the cause is anxiety and depression (see chapter 4). Sometimes it’s the medicines. Sometimes it’s the common aches and pains—colds, influenza, gastroenteritis, nervous stomach, headaches—that affect everyone.
Sometimes the cause is one of the medical complications. When
Table 6. Nonmedicinal Treatment of Wasting
| Cause | Do’s | Don’t’s |
| Mouth sores | Treat the cause—usually thrush, OHL, esophagitis, herpes, aphthous ulcers | Food that is hot, spicy, sour, or sticky |
| Loss of taste | Eat the foods you like; use herbs, spices, and additives as desired | Food you don’t like |
| Nausea | Eat small portions; eat saltines, pretzels, toast; drink liquids and eat food separately | Food that is fatty, spicy, or has strong aromas; drugs that cause nausea—use substitutes |
| Depression | Ask the assistance of a mental health professional | |
| Dementia | Encouragement by caregiver; may require feeding | |
| Diarrhea | Small, frequent meals; eat food high in soluble fiber, like oatmeal, pears, bananas, peaches | Caffeine, milk and milk products, fruit juices, fatty food, alcohol; food high in insoluble fiber like whole grain breads and cereals |
constitutional symptoms are accompanied by cough and shortness of breath, the cause may be pneumocystis pneumonia. When constitutional symptoms are accompanied by headache or other symptoms of central nervous system infection (see above, “Head and Nerve Problems”), the cause is probably toxoplasma encephalitis or cryptococcal meningitis. When constitutional symptoms last for weeks or months, the cause is probably pneumocystis pneumonia, tuberculosis, Mycobacterium avium complex, cytomegalovirus, lymphoma, fungal infections, drugs, or HIV itself.
Tuberculosis. Tuberculosis (TB) is an infection of the lungs by a bacterium called Mycobacterium tuberculosis. (See “Tuberculosis,” under “Productive Cough, Shortness of Breath, Fever,” in this chapter.)
Mycobacterium avium complex (MAC). Mycobacteria are special types of bacteria; the best known, Mycobacterium tuberculosis, causes tuber-
Table 7. Drugs Used to Treat or Prevent Wasting
| Drug | Cost/Week* | Comment |
| Megesterol (Megace) | $70-140 | Most of the weight gain is fat. Side effects: impotence, reduced testosterone levels, high blood sugar. |
| Dronabinol (Marinol) | $140-210 | Most of the weight gain is fat. Psychoactive component of marijuana, so may cause “high.” |
| Serostim (growth hormone) | $1,750-2,300 | Most of weight gain is lean body mass. Requires injection daily. |
| Testosterone injection | $10 | Causes muscle building and masculinizing effects; used by men only. Injected every two weeks. |
| Testosterone patch | $35 | Same as testosterone injection, but applied as a patch to skin daily. Men only. |
| Oxandrolone | $250 | Causes muscle building with fewer masculinizing effects. May be used in low dose by women. |
| Nandrolone | $15 | As above |
| Testosterone plus Megace | around $30 | Popular combinations |
*Cost based on average wholesale price.
culosis (TB). TB is the most common complication of HIV infection in developing countries. But in Europe and North America, the most common mycobacterial infection in HIV infection is Mycobacterium avium complex, or MAC. In people with HIV infection, MAC is usually widespread and can be cultured in the blood. People who do not have HIV infection also get infections with MAC, but only in the lungs. Before HAART, 30 to 50 percent of people with advanced HIV infection and a CD4 cell count of less than 50 developed MAC infection. MAC is now relatively unusual but still occurs in those with low CD4 counts who don’t take drugs to prevent MAC.
MAC may spread widely throughout the body. In the liver, MAC can cause hepatitis; in the lung, pneumonia; in the bone marrow, it can cause a lowered blood count (further lowered from the effect of HIV); in the lymph glands, it can cause enlargements; in the intestines, stomach pain and diarrhea. Accompanying all of these infections are constitutional symptoms; the most common are chronic fever, weight loss, abdominal pain, and diarrhea.
MAC is easy to diagnose because it can be detected in the blood, but labs take at least a week to grow and identify it. MAC is somewhat difficult to treat, however, since many standard drugs don’t work well and since, during the course of therapy, MAC often becomes resistant. Physicians have two approaches to this infection. To prevent MAC, the recommendation is to take clarithromycin (Biaxin) once a day, or azithromycin once a week. Preventive treatment is begun when the CD4 count is below 50, and can be discontinued when the CD4 count is above 100. To eliminate or reduce the numbers of mycobacteria, the standard treatment is to give two or more drugs. The most important are clarithromycin (Biaxin) and ethambutol given together. Sometimes these two are combined with a third drug: ciprofloxacin (Cipro), rifabutin (Mycobutin), azithromycin (Zithromax), or amikacin (Amikin). Most people respond to the drugs, though the response is slow, often requiring weeks for fever, fatigue, and positive blood cultures to resolve. In addition, many people have trouble tolerating the drugs, and some develop resistance to the drugs, after which the infection breaks through. Most important is to raise CD4 cell counts, which will help control MAC, prevent resistance, and simplify treatment.
Successful treatment of MAC has one curious and common complication, called “immune reconstitution syndrome,” or IRS. IRS is described below but is emphasized here because it seems to complicate treatment of mycobacterial infection far more than treatment of other infectious disease complications. In Africa, the most common form of IRS is immune reconstitution TB; in the United States and Europe, it is immune reconstitution MAC. To understand the mechanism of this reaction, see “Immune reconstitution syndrome,” below.
People with MAC usually take two antibiotics for MAC and three to four drugs for HIV infection. The MAC infection does improve somewhat, and the CD4 cell count rises as the HIV viral load falls. The newly reconstituted immune system recognizes MAC and attacks it aggressively. As a result of the attack, the person may have fever, fatigue, sweats, and local symptoms like enlarged, tender lymph nodes, stomach pain, or back pain, depending on the site of the attack.
It is important to note that MAC is transmitted very differently from the mycobacterium that causes tuberculosis. MAC is in soil and often in water supplies, which are presumably the sources of infection. Unlike tuberculosis, MAC is not transmitted from one person to another, and special precautions to prevent its spread are not necessary.
Cytomegalovirus (CMV). CMV infection, like herpes simplex infection, occurs early in life and remains dormant until a weakened immune system allows it to flourish. About 60 to 90 percent of adults have antibodies to CMV in their blood, meaning they have been infected and continue to harbor the virus. The initial infection is usually associated with either trivial symptoms or no symptoms at all. For most people the presence of the virus in the body continues to cause no symptoms until the immune defenses are lowered. About 30 percent of people with AIDS who are not taking treatment develop CMV disease when their CD4 counts are less than 50.
Like MAC, CMV infections are spread throughout the body. In the liver, CMV causes hepatitis; in the intestines, diarrhea; in the brain, encephalitis; in the nerves, a condition called radiculopathy; in the esophagus, difficulty swallowing; in the lung, pneumonia; on the skin, herpeslike sores; in the eye, retinitis. In many people, CMV infection only causes constitutional symptoms, including fever, fatigue, and wasting. The most common and serious of these infections is CMV retinitis. The diagnosis is made by an ophthalmologist. Treatment is important: it prevents loss of sight that could end up in blindness (see above, under “Eye Problems”).
CMV is transmitted the way HIV is, through sexual contact or contact with blood. CMV is not transmitted from one person to another by casual contact.
CMV infection is difficult to treat although antibiotics like ganciclovir (given intravenously), cidofovir, and foscarnet are at least partially effective against some forms of the disease. CMV retinitis responds well to many different kinds of treatment, but the problem is relapse: that is, symptoms recur, and eye examinations show progressive changes. CMV at other places in the body responds less predictably. The problem with all the treatments is that they work temporarily, then fail. Depending on the type of treatment, the average time to failure is two to twelve months. Then a new treatment is tried.
For people with a low CD4 count, the best treatment is to start CMV therapy and HAART both. HAART increases a low CD4 count and permits the immune system to control CMV. When the CD4 count is over 100, it is possible to stop treatment for CMV.
Lymphoma. Lymphomas are tumors of the lymph glands that can occur in anyone but are more common and more severe in people with HIV
infection. Lymphomas can occur relatively early in HIV infection when the CD4 count is above 200; lymphoma is one complication of HIV infection that has not decreased dramatically with HAART, presumably because lymphomas do not require a major decrease in the CD4 cell count.
In some people, the only symptoms of lymphoma are the constitutional symptoms. In other people, the symptoms of lymphoma are very large lymph glands in the neck, under the arms, or in the groin. In some people, the symptoms of lymphoma differ according to where in the body lymphoma occurs: lymphoma in the intestines causes pain and diarrhea; in the brain, focal neurologic problems (see above, “Head and Nerve Problems”); in the lung, pneumonia. The most common symptoms are fever, weight loss, fatigue, and abdominal pain. A CT scan of the chest and abdomen helps find the lesions if they are not obvious.
In people with HIV infection, lymphomas occur more often and progress more rapidly than they do in other people. Treatment is with radiation and with chemotherapy using the same drugs used for other types of tumors. The treatment is given by specialists, either radiation therapists or oncologists. The success of the treatment is variable; some people do extremely well. Curing lymphoma is increasingly likely, so talk to your physician about the side effects and potential benefits of each treatment.
Fungal infections. Constitutional symptoms can also be caused by fungal infections, including Cryptococcus neoformans, Histoplasma capsu- latum, and Coccidioides immitis.
Cryptococcus neoformans usually causes pneumonia, then spreads to other areas of the body. It spreads most commonly to the meninges, where it causes meningitis (see above, under “Head and Nerve Problems”). It can also cause only constitutional symptoms.
Histoplasma capsulatum is found primarily in the central and eastern parts of the United States, especially in the Mississippi, Ohio, and St. Lawrence River valleys. Most people with histoplasmosis have been in the areas where it is common, but they may have been in those areas years earlier. In most people, it causes infections of the lungs. In people with HIV infection, it causes infections spread throughout the body.
Coccidioides immitis is found in the southwestern United States (California, Arizona, New Mexico, and Texas), where it causes a lung infection called valley fever. As with histoplasmosis, HIV-infected people with coccidioidomycosis have usually visited or lived in the areas where the fungus grows. In people with HIV infection, Coccidioides, like Histoplasma, tends to spread throughout the body.
All three fungal infections are diagnosed by detecting the fungus. They are usually treated with amphotericin B, given intravenously, or with the azoles—fluconazole (Diflucan) or itraconazole (Sporanox)— both taken by mouth.
Drugs. Constitutional symptoms can also be caused by drugs. People with HIV infection take many drugs either to treat or to prevent infections, and to treat anxiety, depression, fever, aches, and problems with sleep and appetite. Many of these drugs have side effects, ranging in seriousness from drowsiness to kidney damage and anemia. The only side effects of many drugs, however, are constitutional symptoms, particularly fever and rash. Drugs can also commonly cause hepatitis, low counts of white blood cells, nausea, vomiting, diarrhea, and abdominal pain. AZT, d4T, and/or ddI can cause lactic acidosis, which in turn can cause weight loss and weakening; lactic acidosis is important to recognize because it’s progressive and ultimately serious.
For reasons that are unclear, many of these side effects are more common in people with HIV infection. For instance, trimethoprim-sul- famethoxazole (Bactrim or Septra) causes side effects in 10 percent of the people without HIV infection and over 50 percent of those with HIV infection.
Finding out which drugs are causing side effects and stopping the side effects requires the advice of a physician. This advice will depend on the probability for each drug and the necessity of the drug. The physician will either advise what is called a drug holiday—discontinuation of all drugs—or will stop drugs one at a time.
HIV Infection. Some people have constitutional symptoms that cannot be attributed to a medical complication, or to the side effects of drugs. In such cases, HIV itself might be responsible.
Constitutional symptoms with no causes other than HIV usually occur late in the course of the infection. The treatment is drugs directed at HIV—like HAART—or drugs that simply relieve the constitutional symptoms—aspirin, acetaminophen, ibuprofen, or similar drugs. Sometimes prednisone helps. These drugs are often given on a trial basis, in varying combinations and increasing doses.
Immune Reconstitution Syndrome (IRS). The HAART era brings with it an unexpected development. A rapid decrease in HIV viral load is usually accompanied by a rapid increase in CD4 cells, which means the immune system is being rebuilt, reconstituted—exactly what we want. But when people taking HAART also have complications like CMV or MAC or PCP or cryptococcal meningitis, their newly reconstituted immune systems kick in, recognize those microbes, and aggressively attack. The
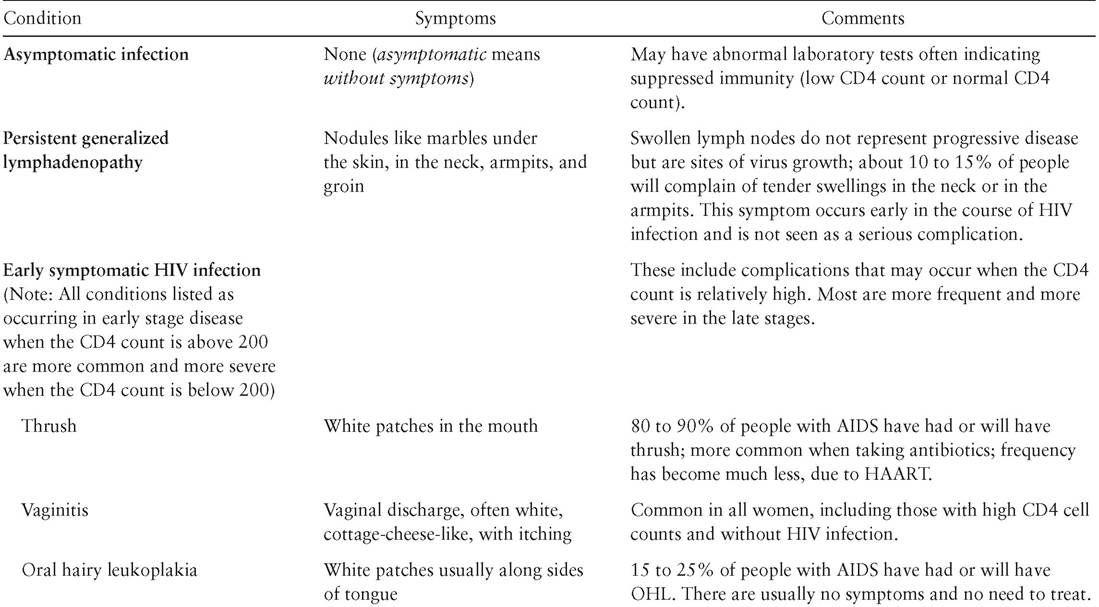
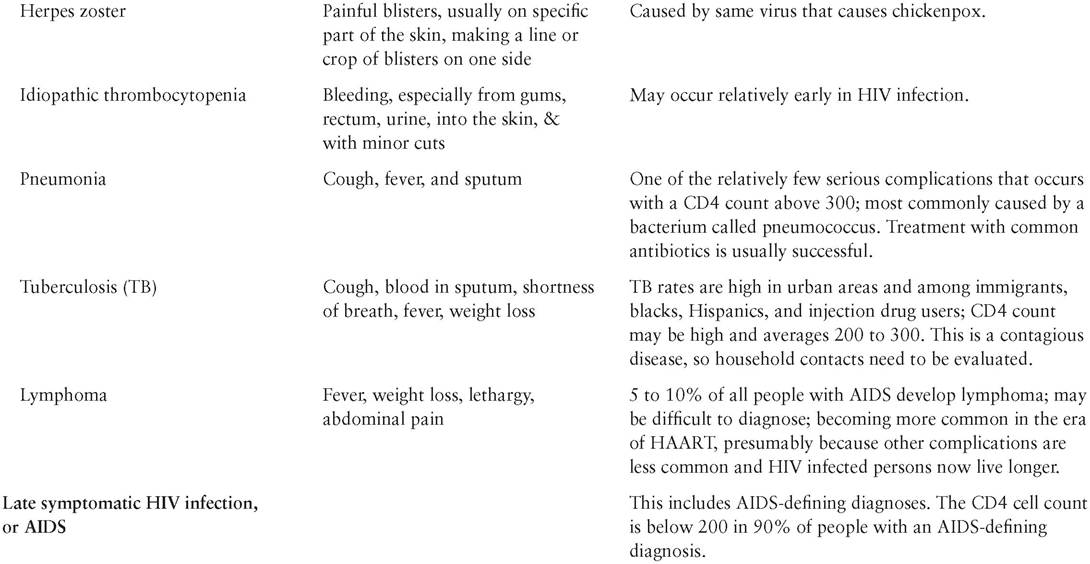
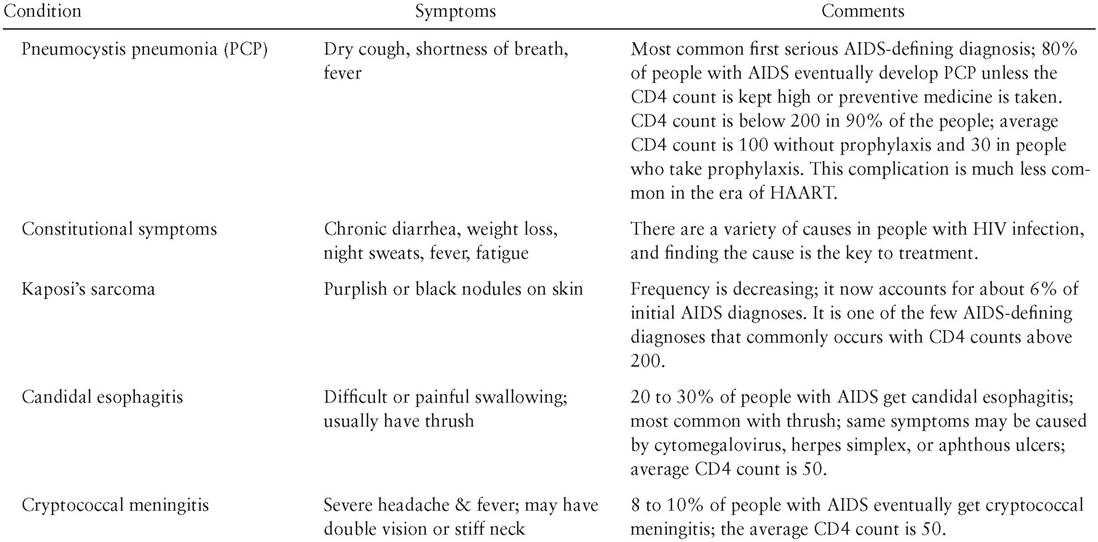
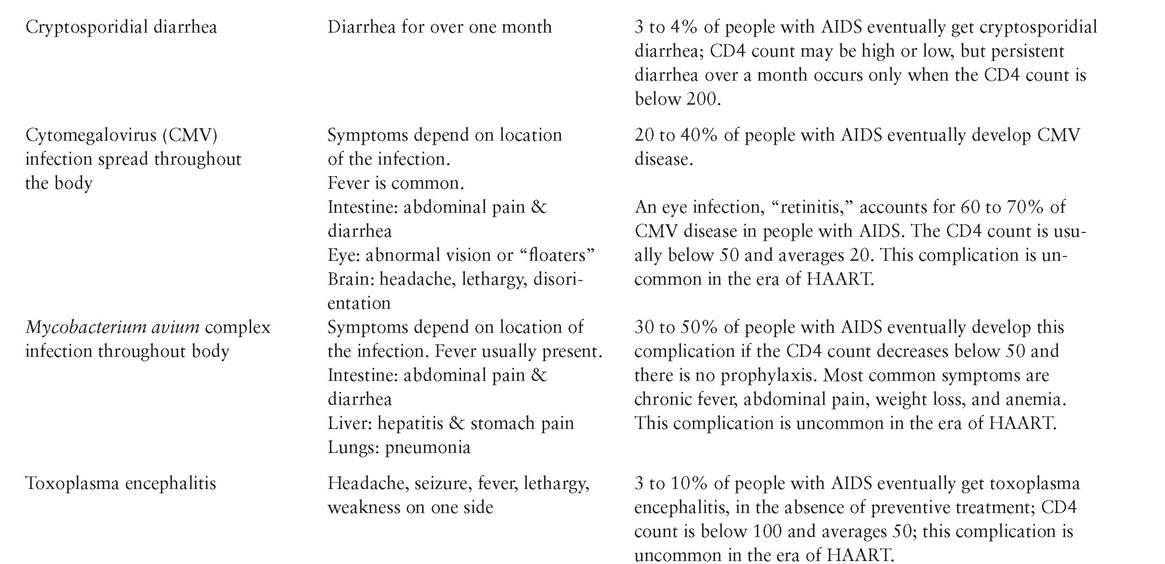
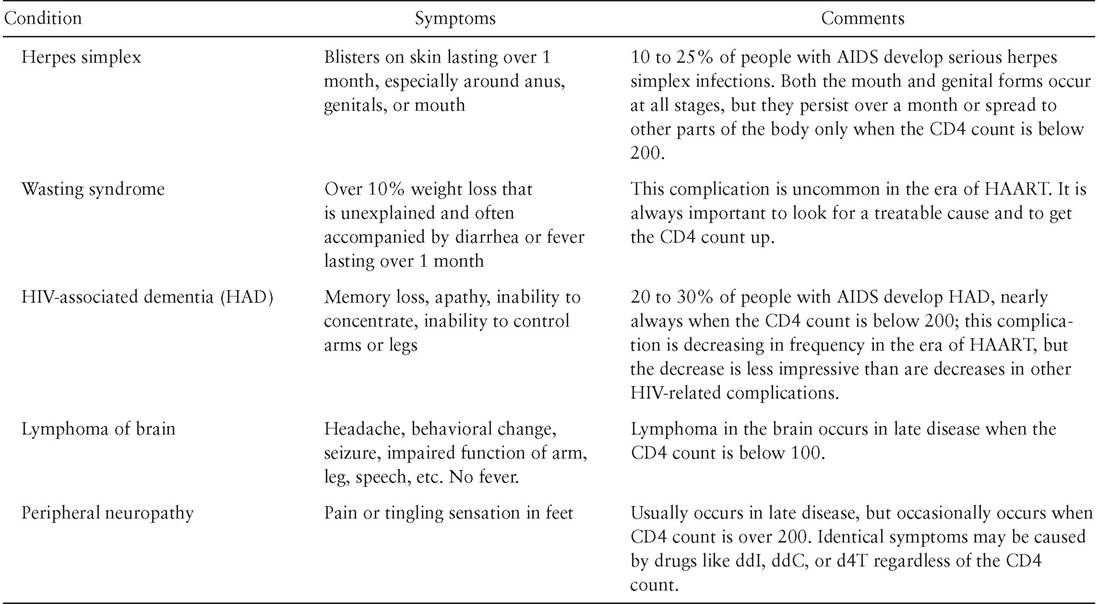
Table 8. Stages of Untreated HIV Infection and Commonly Associated Complications
188
189
190
191
192
immune attack causes general symptoms of fever and fatigue, along with specific symptoms that reveal the site of the attack: a swollen lymph node in the neck for MAC, a sudden worsening of vision for CMV, or a sudden severe headache for cryptococcal meningitis. The health care provider has to decide: Is this a relapse of the infection? Is it a new reaction to one of the many drugs? Is it a new HIV-related complication? It is none of these; it is an immune system now doing its job. The resulting syndrome is called immune reconstitution syndrome or IRS.
IRS usually occurs after HAART is started, when the CD4 cell count is still low (usually less than 100) and the response to HAART is good (the viral load is falling and the CD4 cell count is rising). The new immune response is to an infection, usually one that is newly treated, but sometimes one not known to have existed. Though the symptoms can be pretty awful, the syndrome is a good sign: the immune system is working. IRS is managed by continuing HAART, treating the complicating infection, and quieting down the immune system with ibuprofen or cortisone.
Consider the case of a 42-year-old man who sees a physician because he has fever and weight loss. The physician runs tests and learns that the man has HIV infection, a CD4 count of 50, and a blood culture positive for MAC. The physician treats the man with HAART and for MAC. The man slowly responds, and after four months, his CD4 cell count has increased to 96 and his viral load has decreased from 56,000 to 450. He then develops fever and a large, tender swelling in his neck. This is MAC IRS: his HIV is under control; his CD4 count is on a roll; and his MAC, which used to be disseminated throughout his body, is now isolated in one lymph node, where the immune system is doing its job. The physician doesn’t want to stop treating either HIV or MAC, so to make the man feel better, the physician prescribes corticosteroids to cool down the overactive immune system.