Protozoal infections
Pneumocystis carinii pneumonia (PCP) Although recently recognised as being more like a fungus,
P. carinii is considered under protozoa here. Nowadays PCP most commonly occurs in those at risk who fail to take adequate prophylaxis or who are newly diagnosed with HIV infection in advanced disease where it is frequently the presenting illness.
Clinical suspicion is aroused early in patients who are under regular medical supervision, leading to earlier diagnosis. Later diagnosis is asssociated with more severe disease and poorer treatment outcome. Techniques of diagnosis include sputum induction with nebulised saline; this obviates the need for bronchoscopy but the diagnostic sensitivity is lower. The use of lavage alone at bronchoscopy avoids transbronchial biopsy with its complications of haemorrhage and pneumothorax. Exercise oximetry and alternative imaging techniques with radiolabelled compounds are also being used in diagnosis. Monoclonal antibodies to pneumocystis proteins and sensitive DNA probes have been developed but have yet to reach the bedside. In the absence of a confirmatory test, a presumptive diagnosis may be made based on the clinical presentation and chest x ray appearances in a patient severely immunosuppressed and at risk.
High-dose intravenous co-trimoxazole for two to three weeks remains a standard first-choice regimen for severe PCP, but once fevers and symptoms have settled and blood gas values have improved the drug can be given by mouth. Side-effects are common, typically after 7—10 days. If co-trimoxazole treatment is not tolerated, alternative treatment regimens include either intravenous pentamidine or a combination of clindamycin and primaquine. Pentamidine is as effective as co-trimoxazole but has side-effects that can be life threatening and should be given by slow intravenous infusion with careful monitoring.
In patients with moderate or mild PCP a combination of clindamycin and primaquine has proven clinical efficacy and is an alternative first choice for those patients who have a previous history of severe co-trimoxazole hypersensitivity. Side-effects of rash and diarrhoea are frequent.
Figure 9.1 Chest x ray appearance of Pneumocystis carinii pneumonia showing interstitial infiltrates
In patients presenting with severe hypoxaemia high-dose adjunctive corticosteroid therapy is indicated and has been shown in clinical studies to reduce both mortality and morbidity
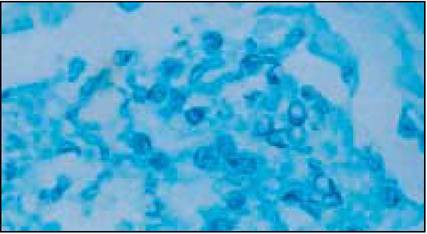
Figure 9.2 Cysts of Pneumocystis carinii in broncho lavage specimen
Alternative second-line therapies include dapsone with trimethoprim, trimetrexate with folinic acid or Atovaquone, a hydroxy-naphthoquinone. The efficacy of atovaquone has only been established in mild to moderate P. carinii infection. Like trimetrexate it is probably less effective than co-trimoxazole but it is less toxic. New formulations have improved atovaquone's bioavailability but it still should not be given to patients with malabsorbtion conditions, previous severe diarrhoea or those not taking oral nutrition. Due to acquired resistance, where possible atovaquone should not be given as single-agent therapy. It is commonly combined with intravenous pentamidine as an effective second-line treatment.
Prophylaxis for PCP pneumonia is essential after a first attack (secondary prophylaxis) but is also recommended for all patients once their CD4 cell counts falls below 200 X 106∕l (primary prophylaxis). The risk of a first episode PCP below this CD4 count level in patients not on antiretroviral therapy is estimated to be 18% at 12 months for those who are asymptomatic, rising to 44% for those who have early symptomatic disease (for example, oral candida, fever).
Co- trimoxazole 960mg given by mouth daily or three times per week is the most effective agent. In patients who are intolerant, alternative regimens include oral dapsone 100 mg with pyrimethamine 25mg daily or three times per week, atovaquone 1500 mg daily or nebulised pentamidine. Dose of the latter depends on the nebuliser system: with a Respirgard II nebuliser the recommended regimen is 300mg every four weeks. In patients with more advanced disease and CD4 counts less than 100 ? 106∕l, 300mg given every two weeks should be considered in view of the high failure rate of the monthly regimen.| Table 9.l Pneumocystis carinii pneumonia treatment | Comments | ||
| Drug | Duration | Side-effects | |
| First choice: Co-trimoxazole (trimethoprim component | 21 days | Nausea, vomiting, fever, rash, | Intolerance common (25-50% of treated |
| 15-20mg∕kg per day p.o./i.v. in | marrow suppression, raised | patients) | |
| divided doses). Alternative regimens: | transaminases | ||
| 1. Severe disease: | 21 days | Hypotension, hyper- and | 80% of patients will respond to treatment |
| Pentamidine isethionate 4 mg/kg per | hypoglycaemia, renal failure, | ||
| day as slow intravenous infusion | marrow suppression, nausea, vomiting, cardiac arrest | ||
| Trimetrexate 45 mg∕m2 i.v. and folinic | 21 days | Marrow suppression, raised | Should only be used as third or fourth line |
| acid 80 mg∕m2 | transaminases rash, anaphylaxis | treatment | |
| 2. Mild to moderate disease: | 21 days | Diarrhoea, rash, nausea, | Clostridium difficile toxin associated diarrhoea is |
| Clindamycin 600mg 6 hourly p.o./i.v. | vomiting, marrow suppression, | a frequent complication of clindamycin therapy | |
| and primaquine 15 mg daily p.o. | methaemoglobinaemia, haemolysis | ||
| Trimethoprim 20mg per kg/day p.o./i.v. | 21 days | Rash, nausea, | Alternative regimens should be used in patients |
| in 2-3 divided doses and dapsone | methaemoglobinaemia, | with G6PD deficiency | |
| 100 mg daily p.o. | marrow suppression | ||
| Atovaquone suspension 750mg | 21 days | Rash, raised transaminases | Must be taken with food. Consider combination |
| twice daily | and neutropenia | with i.v. pantamidine as resistance reported with monotherapy | |
| Adjuvant high-dose steroids | 5 days | ||
| (for example, prednisolone 40-60 mg daily p.o.) | tapering over | Indicated in severe disease. Optimal dose not | |
| 14-21 days | determined | ||
Although clinical trials have shown greater efficacy for co- trimoxazole compared to other regimens, there is a high rate of discontinuation due to side-effects. Desensitisation regimens are used with the aim of reducing the rate of intolerance but there is uncertainty about their efficacy and which regimen is best.
In patients responding to antiretroviral therapy, primary or secondary prophylaxis can be safely discontinued once the CD4 count has increased to levels persistently above 200 ? 106∕l.
Toxoplasmosis
Cerebral toxoplasmosis is the commonest manifestation of toxoplasma infection. As toxoplasmosis is the most common cause of ring-enhancing lesions on contrast CT brain scans a presumptive diagnosis is usually made and treatment started. T he condition responds well if treatment is started early, and a combination of sulphadiazine 4—6 g/day and pyrimethamine 50-100mg a day (both by mouth in divided doses with folinic acid 15mg daily) is the treatment of choice. Side-effects may prevent continued use of sulphadiazine, and clindamycin 600-1200mg four times a day has been shown to be an effective alternative in controlled studies.
Corticosteroids are sometimes used in addition to first-line treatment to reduce symptomatic cerebral oedema, but a clinical and radiological response seen after two weeks of treatment may be due solely to the corticosteroid effect rather than the anti-toxoplasma treatment. A presumptive diagnosis of toxoplasma may therefore be made, although the underlying lesion may be due to something else, such as lymphoma or another infection. Relapse is common after treatment is stopped, and maintenance treatment is therefore necessary. In patients responding to antiretroviral therapy with sustained increases in CD4 count, discontinuation of prophylaxis is safe but there is limited current data to make definite recommendations.
Atovaquone 750mg four times a day with or without pyrimethamine may be considered an alternative and the new macrolides clarithromycin 2 g daily and azithromycin, both given with pyrimethamine 75 mg/day, have also been effective in small uncontrolled studies. The most appropriate regimen for secondary prophylaxis has not been determined but treatment doses of either sulphadiazine and pyrimethamine or clindamycin and pyrimethamine are usually halved.
Of patients with positive toxoplasma serology and a CD4 count of less than 100 ? 106∕l, approximately 1 in 3 will develop cerebral toxoplasmosis within 12 month without prophylaxis. Primary prophylaxis in patients with positive serology with a CD4 count of less than 100 ? 106∕l is therefore recommended. Co-trimoxazole or dapsone with pyrimethamine have been shown to reduce the incidence of toxoplasmosis compared to patients taking nebulised pentamidine for prophylaxis against PCP. Atovaquone with or without pryrimethamine may also be considered but this is based on more limited data. T he macrolides clarithromycin and azithromycin might be anticipated to provide broad-spectrum prophylaxis for toxoplasmosis, atypical mycobacterial and bacterial infections, but bacterial resistance might limit their use in this situation.
Patients who are toxoplasma serology negative should be given advice to prevent exposure in primary infection with toxoplasmosis. They should be advised not to eat raw or undercooked meat and avoid directly handling cats' faeces.
Cryptosporidiosis and other protozoa
In patients with less advanced HIV disease (CD4 counts >200 ? 106∕l) cryptosporridial infection usually causes a self-limiting gastrointestinal illness and symptomatic treatment with
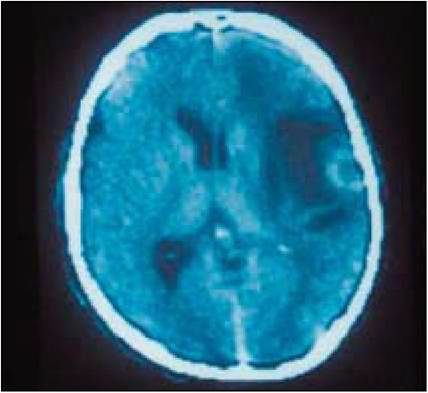
Figure 9.3 CT scan showing ring-enhancing lesions of cerebral toxoplasmosis surrounded by cerebral oedema (dark area)
Box 9.2 Treatment of toxoplasmosis
First line
Sulphadiazine 4—6 g per day or clindamycin 600—1200 mg ? 4 per day
+
Pyrimethamine 50-100mg per day
+
Folinic acid 15mg per day
Alternatives
• Clarithromycin 2g per day or
• Atovaquone 750mgs 4 ?per day p.o.
+
Pyrimethamine 50-100 mg per day p.o.
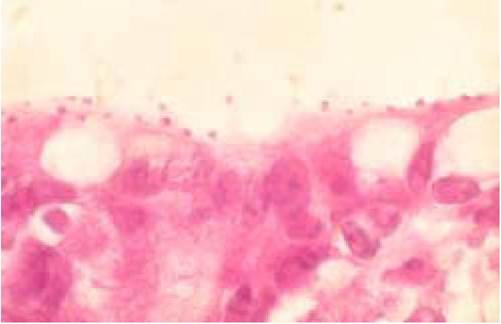
Figure 9.4 Cryptosporridial infection of the small bowel
anti-diarrhoeal agents is all that maybe needed. In those with more severe immunosuppression and persistent symptoms treatment is more difficult and reported successes with a variety of agents are still anecdotal. Symptoms and excretion of cysts may be intermittent. Responses have been described after treatment with a variety of agents, including spiramycin, erythromycin, diclazuril, letrazuril, hyperimmune bovine colostrum, paromamycin, azithromycin and subcutaneous somatostatin.
Symptomatic treatment with antidiarrhoeal and antiemetic agents together with fluid, electrolyte and nutritional support should be provided. Case reports suggest that immune reconstitution is likely to result in improvement and resolution of both symptoms and infection. Thus in the absence of an effective specific treatment against cryptosporidium, infected patients should be started on antiretroviral therapy to increase the CD4 count.
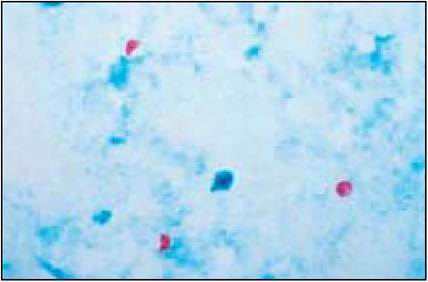
Figure 9.5 Cryptosporidium
Patients at risk of infection should be advised to avoid possible exposure in water supplies particularly at times of documented outbreaks. Although unproven, measures that may be considered for patients with CD4 counts less than 200 ? 106∕l include using bottled water, point of use filters or boiling water for more than one minute.
For microsporidiosis there have been anecdotal reports of symptomatic improvement with albendazole 400 mg twice a day or metronidazole 500mg three times a day.
Isosporiasis is less common and appears to respond to co- trimoxazole 960 mg four times a day, but relapses occur in half of all cases.
Diarrhoea often occurs in the absence of recognised pathogens in the stool, and metronidazole has relieved symptoms in some cases.
| Table 9.2 Viral opportunistic infections | |||||
| Infection | Drug | Duration | Side-effects | Comments | |
| Herpes simplex Treatment | Aciclovir 200 mg 5 ? a day | 5-7 days | Duration may be extended in severe | ||
| orally or 10mg/kg 8 hourly i.v. | infections | ||||
| Prophylaxis | Aciclovir 200 mg 4 ? a day or 400 mg 2 x day | Indefinite | |||
| Cytomegalovirus Treatment | Ganciclovir 5 mg/kg twice a day i.v. | 14-21 days | Neutropenia, anaemia | GCSF support may be required | |
| Cidofovir 5 mg/kg i.v. | 2 weeks | Nephrotoxicity: impaired | Co-administer with probenecid and | ||
| once a week | creatine clearance, proteinuria, | adequate hydration to reduce risk of | |||
| hypophosphataemia Neutropenia Ocular toxicity | nephrotoxicity | ||||
| Foscarnet 180 mg/kg | 14-21 days | Nephrotoxicity, hypomagnesaemia, Dose must be adjusted according to | |||
| daily i.v. | hyper- and hypocalcaemia, | hyper- | renal function | ||
| and hypophosphataemia, hypokalaemia, nausea vom genital ulceration | iting, | ||||
| Maintenance | Ganciclovir 3gr daily | Until CD4 | As above | May be combined with intraoccular | |
| ganciclovir | orally | count > | implants | ||
| 100 ? 106∕l on | Avoid in patients with diarrhoea | ||||
| HAART | Increases levels of didanosine | ||||
| Cidofovir 5 mg/kg once | Until CD4 | As above | As above | ||
| every 2 weeks | count > 100 ? 106∕l on HAART | ||||
Alternative secondary prophylaxis regimens include daily intravenous foscarnet or ganciclovir, intravitreal injections of ganciclovir or foscarnet and intraoccular ganciclovir implants