Anemia of Chronic Renal Insufficiency
GENERAL PRINCIPLES
Anemia of chronic renal insufficiency is attributed primarily to decreased endogenous erythropoietin (EPO) production and may occur as the creatinine clearance declines to below 50 mL/min.
Other causes including a functional iron deficiency may contribute to the etiology (see the previous description).DIAGNOSIS
• RBCs are often normocytic and hypochromic, with the occasional presence of echinocytes (burr cells).
• Iron status should be evaluated in patients who are undergoing dialysis by obtaining levels of ferritin and transferrin saturation. Oral iron supplementation is not considered effective in CKD; therefore, parenteral iron to maintain a ferritin level of gt;500 ng/mL is recommended.
TREATMENT
• Treatment has been revolutionized by erythropoiesis-stimulating agents (ESAs) including EPO and darbepoetin alfa (Table 21-4).
TABLE 21-4
ERYTHROPOIETIN DOSING
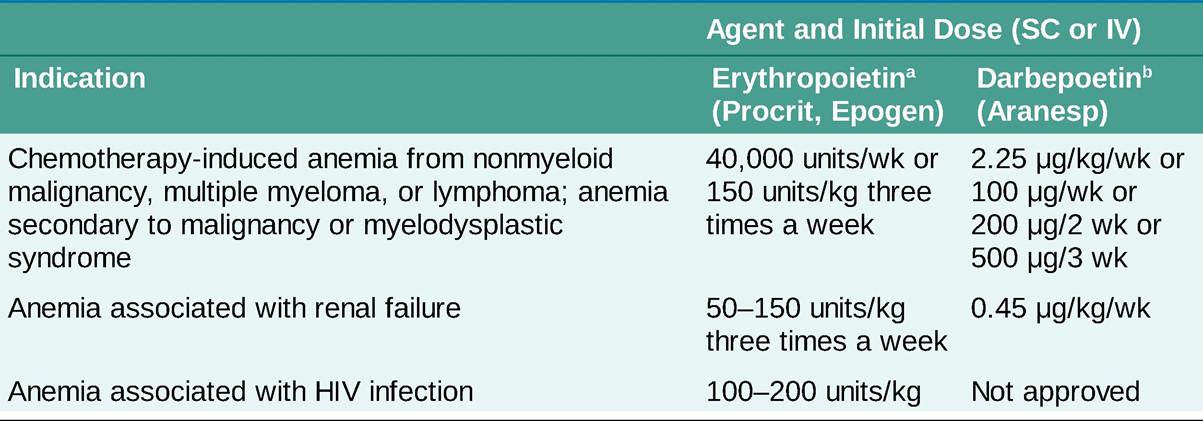
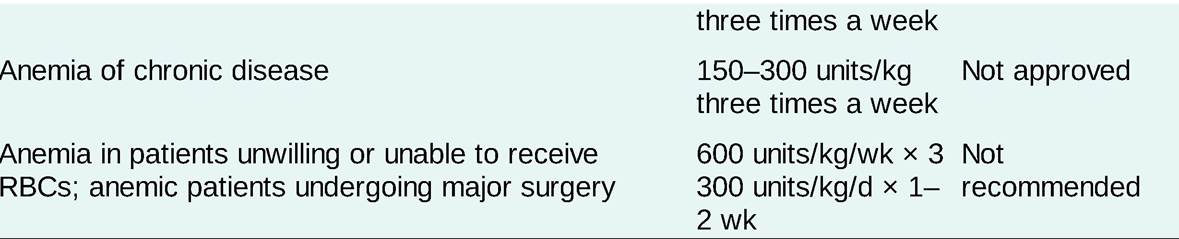
RBC, red blood cell.
aDose increase after 48 weeks up to 900 units/kg/wk or 60,000 units/wk; discontinue if hematocrit (Hct) is gt;40%; resume when Hct is lt;36% at 75% of previous dose.
bDose increase after 6 weeks up to 4.5 mg/kg/wk or 150 mg/wk or 300 mg/2 weeks; hold dose if Hct is gt;36%, then resume when Hct is lt;36% at 75% of previous dose.
• Therapy is initiated in predialysis patients who are symptomatic.
• Administration of ESAs can be IV (hemodialysis patients) or SC (predialysis or peritoneal dialysis patients). In dialysis and predialysis patients with CKD, the target Hgb should not exceed 11 g/dL due to the increased risk for cardiovascular events, stroke, and venous thromboembolism.7 A rapid rise in Hb of gt; 1g/dL over 2 weeks may also be associated with these risks.
Hgb and Hct should be measured at least monthly while receiving an ESA. Dose adjustments should be made to maintain the target Hgb.• Suboptimal responses to ESA therapy are most often due to iron deficiency, inflammation, bleeding, infection, malignancy, malnutrition, and aluminum toxicity.
î IV iron administration has become first-line therapy for individuals with transferrin saturation lt;20% and/or ferritin lt;500 ng/mL. It has also been shown to reduce the ESA dosage required to correct anemia.
î A ferritin level and transferrin saturation should be tested at least monthly during the initiation of ESA therapy with a goal ferritin level of gt;200 ng/mL and a transferrin saturation of gt;20% in dialysis-dependent patients and a ferritin level of gt;100 ng/mL and a transferrin saturation of gt;20% in predialysis or peritoneal dialysis patients.
î Iron therapy is unlikely to be useful if the ferritin level is gt;500 ng/mL.
î Secondary hyperparathyroidism that causes BM fibrosis and relative ESA resistance may also occur.
• Roxadustat, an oral hypoxia-inducible factor inhibitor, has been approved for the treatment of anemia in CKD in China and Japan.8 It is currently undergoing evaluation by the Food and Drug Administration (FDA) for approval in the US.