Antipsychotics
GENERAL PRINCIPLES
Pathophysiology
• Antipsychotic agents exert their therapeutic effect largely by antagonizing dopamine receptors in the central nervous system. Newer antipsychotic agents also modulate serotonergic tone.
î Dopamine antagonism unbalanced by muscarinic antagonism leads to extrapyramidal neuromuscular effects, such as acute dystonia, torticollis, oculogyric crisis, drug-induced Parkinsonism, and tardive dyskinesia.
î Generally speaking, the atypical or second-generation antipsychotics have significant antimuscarinic effects that mitigate (but do not eliminate) the risk of extrapyramidal symptoms.
î Dopamine antagonism in the tuberoinfundibular system may lead to gynecomastia and galactorrhea; risperidone is particularly problematic in this regard.
• The antipsychotics also have several well-known “off-target” effects on other receptors and ion channels that are relevant in therapeutic use and overdose.
î Muscarinic antagonism may produce sedation and an antimuscarinic toxidrome in overdose. Quetiapine is particularly antimuscarinic.
î Alpha-1 adrenoceptor antagonism may produce orthostasis and reflex tachycardia.
î Blockade of the cardiac sodium and potassium channels may produce prolongation of the QRS and QT intervals and predispose to dysrhythmias.
• Although each antipsychotic has its own unique pharmacologic profile, in general, first-generation agents (neuroleptics, e.g., haloperidol, droperidol, chlorpromazine) cause more cardiac toxicity and extrapyramidal symptoms than second-generation agents (atypicals, e.g., quetiapine, olanzapine, risperidone).
• Clozapine has unique adverse effects, including profound sialorrhea and agranulocytosis. Its use is closely monitored and restricted.
DIAGNOSIS
Clinical Presentation
• The predominant feature of an acute antipsychotic overdose is profound sedation.
• Other features of acute toxicity depend on the pharmacologic profile of the agent involved (Table 286): for example, quetiapine overdose will produce an antimuscarinic toxidrome.
TABLE 28-6
EFFECTS OF SELECTED ANTIPSYCHOTICS
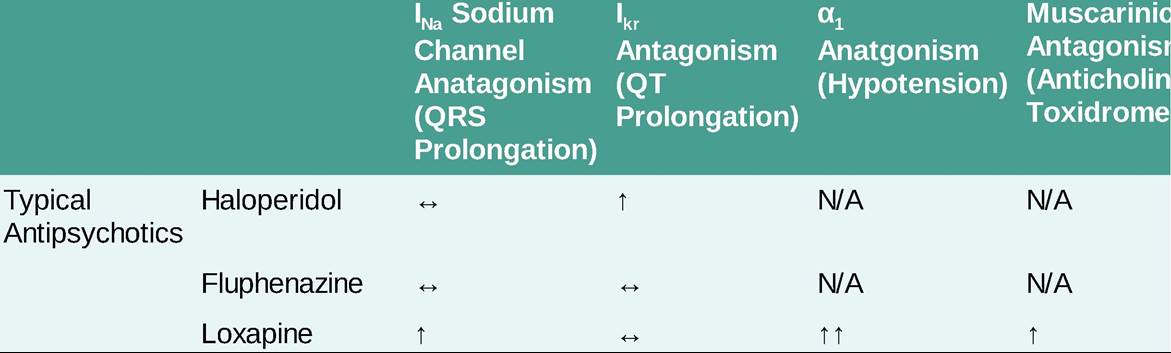
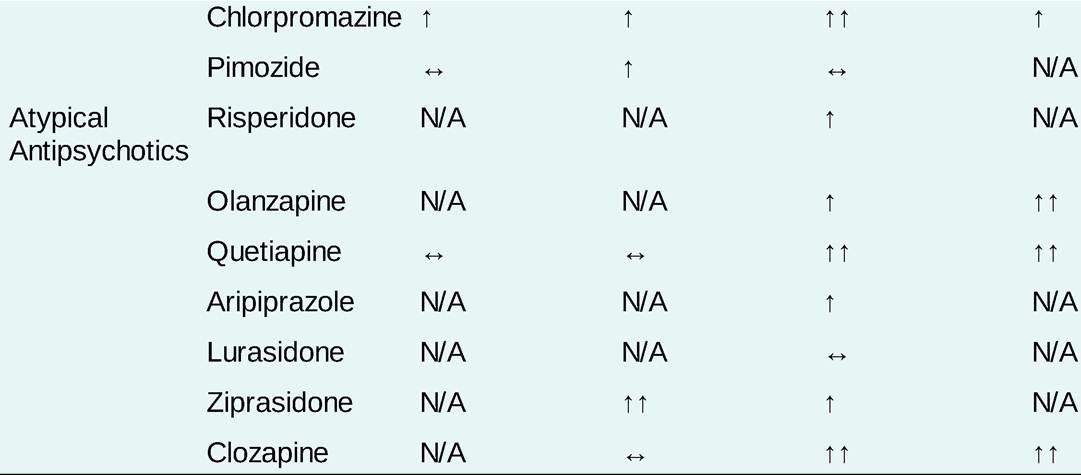
N/A, no significant effect in therapeutic dosing; «, may have effect in Supratherapeutic dosing/overdose; #8593;, antagonism; #8593;#8593;, substantial antagonism.
• Extrapyramidal symptoms usually develop after therapeutic use, typically (although not invariably) following initiation or dose escalation.
î Acute dystonia may cause spasm of any muscle group, including the neck (torticollis) or extraocular muscles (oculogyric crisis). It may be life-threatening when it involves the laryngeal musculature.
î Akathisia is a clinical syndrome of restlessness, anxiety, psychomotor agitation, and a compulsion to move.
î Drug-induced Parkinsonism presents with bradykinesia and rigidity.
î Tardive dyskinesia, a pattern of stereotyped movements of the lips, face, and tongue, usually develops later (sometimes after years of therapy) and may be irreversible.
Diagnostic Testing
LABORATORIES
Routine laboratory testing is not generally helpful.
Target laboratory testing based on the patient's clinical presentation and the agent ingested.
ELECTROCARDIOGRAPHY
• All antipsychotics prolong the QT interval; the degree of prolongation varies among the available agents.
• Some antipsychotics, including first-generation agents and quetiapine, may prolong the QRS interval in overdose. The most problematic agents have been withdrawn from the market.
TREATMENT
• Treatment of acute overdose is generally supportive and symptom-targeted.
î Intubation and mechanical ventilation are not typically required.
î Treat seizures with benzodiazepines or other directly GABAergic agents.
î Hypotension is unusual; if it occurs, treat with fluid resuscitation and vasopressors.
• In patients with QT prolongation, supplement magnesium, potassium, and calcium, and avoid other QT prolonging agents. If torsades de pointes develops, magnesium or overdrive pacing may be required.
• In patients with QRS prolongation, administer sodium bicarbonate as discussed above under tricyclic antidepressant poisoning.
• Treat extrapyramidal symptoms with antimuscarinic agents, typically diphenhydramine or benztropine.
î Patients who require continued therapy with antipsychotics may require initiation of scheduled antimuscarinic agents to prevent extrapyramidal symptoms.
î Tardive dyskinesia may be resistant to treatment.
SPECIAL CONSIDERATIONS: NEUROLEPTIC MALIGNANT SYNDROME
• NMS is a severe, life-threatening adverse effect of antipsychotics that is thought to be mediated by dopamine antagonism. NMS is rare.
• NMS may occur with exposure to any antipsychotic agent, not just with first-generation antipsychotics.
• The onset of NMS is subacute (over a period of days). It typically (but not exclusively) occurs in the days to weeks following the initiation of an antipsychotic.
• NMS classically presents with a triad of mental status changes, neuromuscular abnormalities, and hyperthermia.
î Mental status changes may range from mild delirium to coma and catatonia
î Neuromuscular symptoms typically consist of “lead-pipe” rigidity involving all four extremities and bradykinesia.
î Hyperthermia is a late finding and may be accompanied by profound autonomic instability.
• The most important principle of management is to stop the offending agent and avoid all antidopaminergic xenobiotics.
• Aggressive resuscitative care in the intensive care unit is required.
î Administer benzodiazepines or other directly GABAergic sedatives with the goal of eliminating agitation (if present) and improving neuromuscular rigidity. In extreme cases, paralysis with nondepolarizing neuromuscular blockers may be required to control rigidity.
î If hyperthermia is present, aggressive external cooling must be pursued.
î Monitor for and treat rhabdomyolysis and electrolyte derangements.
• The role of putative antidotes such as bromocriptine (a dopamine receptor agonist) or dantrolene is controversial and their efficacy is unproven.