Aortic Stenosis
• Aortic stenosis (AS) is the most common cause of LV outflow tract obstruction.
• Other causes of obstruction occur above the valve (supravalvular) and below the valve (subvalvular), both fixed (i.e., subaortic membrane) and dynamic (i.e., hypertrophic cardiomyopathy with obstruction).
Etiology
• Calcific/de generative
î Most common cause in the US
î Trileaflet calcific AS usually presents in the seventh to ninth decades of life
• Bicuspid
î Occurs in 1%-2% of population (congenital lesion)
° AS in this population occurs in much younger patients
î Can be associated with aortopathies (i.e., dissection, aneurysm)
• Rheumatic
î More common cause worldwide; much less common in the US
î Almost always accompanied by MV disease
• Radiationinduced
Pathophysiology
The pathophysiology for calcific AS involves both the valve and the ventricular adaptation to the stenosis (Figure 6-1).
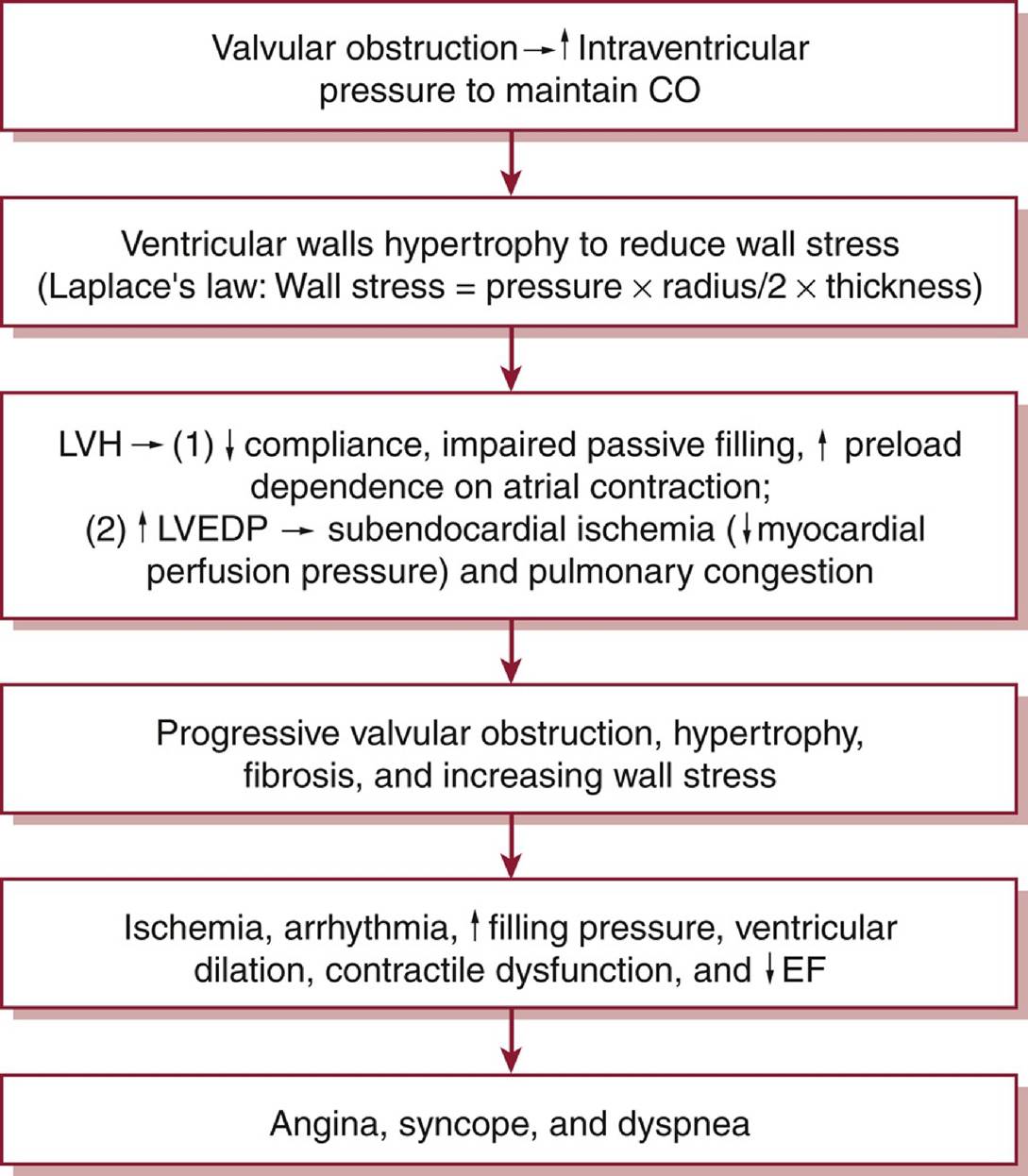
Figure 6-1 Pathophysiology of aortic stenosis.CO, cardiac output; EF, ejection fraction; LVEDP, left ventricular end-diastolic pressure; LVH, left ventricular hypertrophy.
DIAGNOSIS
History
• The classic triad of symptoms includes angina, syncope, and heart failure.
Symptoms may be masked by a progressive decline in functional capacity as patients modify their activities to suit their symptoms.
Physical Examination
• Harsh systolic crescendo-decrescendo murmur heard best at the right upper sternal border and radiating to both carotids; time to peak intensity correlates with severity (later peak = more severe).
• Diminished or absent A2 (soft S2) suggests severe AS.
• Pulsus parvus et tardus: late-peaking and diminished carotid upstroke in severe AS.
Diagnostic Testing
• ECG: LAE, left ventricular hypertrophy (LVH).
• CXR: cardiomegaly, calcification of the aorta and/or aortic valve.
• TTE
î Determine valve morphology (tricuspid vs. bicuspid), calculate valve area using continuity equation, and measure transvalvular mean and peak gradients.
î Severe AS: peak jet velocity ≥4.0 m/s, mean gradient ≥40 mm Hg, valve area Cardiac catheterization
î Hemodynamic assessment of severity of AS in patients for whom noninvasive tests are inconclusive or when there is discrepancy between noninvasive tests and clinical findings regarding AS severity.
î Gorlin equation: used to calculate aortic valve area during invasive hemodynamic assessment; based on principle that aortic valve area is equal to systolic flow across valve divided by systolic pressure gradient times a constant.
TREATMENT
• Severe symptomatic AS requires surgery or percutaneous aortic valve replacement (AVR); currently, there are no medical treatments proven to decrease mortality or to delay surgery.
• Hypertension should be addressed, and diuretics used for volume overload symptoms.
• Severe AS with decompensated HF or shock: Several options may help bridge the patient to definitive surgery or percutaneous procedure: intra-aortic balloon pump (IABP) (contraindicated in patients with moderate to severe aortic regurgitation [AR]), sodium nitroprusside, balloon aortic valvuloplasty.
• AHA/ACC guideline indications for surgical or percutaneous AVR2
î Symptomatic patients with severe AS (Class I).
î Asymptomatic patients with severe AS and an LVEF 5 m/s), asymptomatic patients with elevated BNP, or increase in aortic velocity ≥0.3 m/s per year on serial examinations.
• Decision for mechanical versus bioprosthetic AVR involves shared decision-making with the patient regarding risks of anticoagulant therapy and expected longevity of new valve. In general, it is reasonable to recommend a mechanical prosthesis in patients 65 years of age (Class IIa).2
• Transcatheter aortic valve implantation (TAVI) is an option for patients who are considering bioprosthetic AVR.
î Requires evaluation by a team of cardiologists and cardiac surgeons. TAVI procedure uses fluoroscopic and echocardiographic guidance to place a stented bioprosthetic valve within the stenotic valve. This can be performed via a transfemoral, transaortic, subclavian, transcaval, or transapical approach.
î To date, clinical trials have demonstrated that in patients at prohibitive risk for surgery, TAVI reduces mortality compared with medical therapy3; for high-risk patients and intermediate-risk patients, TAVI and surgical valve replacement have similar outcomes.4-6
o ACC/AHA guidelines for decision for surgical aortic valve replacement (SAVR) versus TAVI2
■ Class I indication for TAVI in patients who are at prohibitive risk for surgery if expected survival is >12 months with an acceptable quality of life.
■ SAVR is recommended for patients with severe AS who are 20 years (Class I).
■ In patients who are 65-80 years of age, either SAVR or transfemoral TAVI are options (Class I).
■ For symptomatic patients with severe AS who are >80 years of age or for younger patients with a life expectancy on the etiology of MR and timing of presentation.
î In primary MR (usually degenerative MR) that has gradually progressed, the patient may be asymptomatic even when the MR is severe. As compensatory mechanisms fail, patients may note dyspnea on exertion (may be because of PH and/or pulmonary edema), palpitations (from an atrial arrhythmia), fatigue, and volume overload.
Physical Examination
• Acute MR
î Tachypnea with respiratory distress, tachycardia, hypotension.
î Systolic murmur, usually at the apex (may not be holosystolic and may be absent).
• Chronic MR
î Apical holosystolic murmur that radiates to the axilla.
î In MV prolapse, there is a midsystolic click heard before the murmur.
î S2 may be widely split because of an early A2.
î Other signs of heart failure (lower extremity edema, increased JVP, rales, etc.).
Diagnostic Testing
• ECG: LAE, LVH, AF.
• CXR: enlarged LA, pulmonary edema, enlarged pulmonary arteries, and cardiomegaly.
• TTE: assess etiology of MR, LA size and LV dimensions (dilated in chronic severe MR), EF (LV dysfunction is present if EF ≤55%), qualitative and quantitative measures of MR severity.
• TEE
î Provides better visualization of the valve to help define anatomy, presence of endocarditis (valvular vegetations), and feasibility of repair.
î May help determine severity of MR when TTE is nondiagnostic, particularly in the setting of an eccentric jet.
• Right heart catheterization
î Better characterize PH in patients with chronic severe MR and determine LA filling pressure in patients with unclear symptoms.
î Giant “V” waves on pulmonary capillary wedge pressure tracing may suggest severe MR.
• Left heart catheterization
î May influence therapeutic strategy in ischemic MR.
î Evaluation of CAD in patients with risk factors undergoing MV surgery.
• MRI/nuclear testing
î Assess EF in patients with severe MR but with an inadequate assessment of EF by echocardiography.
î Assess quantitative measure of MR severity when echocardiography is nondiagnostic.
î Viability assessment may play a role in considering therapeutic strategy in ischemic MR.
TREATMENT
Acute Mitral Regurgitation
• While awaiting surgery, aggressive afterload reduction with IV nitroprusside or an IABP can diminish the amount of MR and stabilize the patient by promoting forward flow and reducing pulmonary edema.
• These patients are usually tachycardic, but attempts to slow down their heart rate should be avoided because they are often heart rate dependent for an adequate forward CO.
Chronic Mitral Regurgitation
• Chronic primary MR
î Medical therapy is reasonable in patients with chronic primary MR and LVEF less than 60% not undergoing surgery.
î Angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor blockers have been shown to reduce the regurgitant fraction and aid with ventricular remodeling.
β-Blockers have also been shown to reduce severity of MR in asymptomatic patients.î There is no benefit of vasodilator therapy in the asymptomatic patient with normal LV function and chronic severe MR.
• Chronic secondary MR
î Treat symptoms related to LV dysfunction.
î Guideline-directed medical therapy (GDMT) for LV systolic dysfunction, including ACE inhibitors and β-blockers, is indicated and has been shown to reduce mortality and the severity of MR.
î Some patients may also qualify for cardiac resynchronization therapy, which can favorably remodel the LV and reduce the severity of MR.
Percutaneous Intervention2
• Transcatheter edge to edge repair (TEER) (i.e., MitraClip) pinches the leaflets together in an attempt to enhance coaptation (a percutaneous treatment analogous to the surgical Alfieri stitch), creating a double-orifice valve.
î This procedure is performed via femoral venous access, and a transseptal puncture is used to position the delivery system in the LA.
î Using fluoroscopy and TEE guidance, the clip is advanced and attempts are made to grasp the leaflet tips of the anterior and posterior MV leaflets and clip them together.
î Indicated for chronic severe secondary MR with LVEF between 20% and 50% for patients with persistent symptoms despite GDMT and appropriate anatomy (Class IIa).
This recommendation comes from results of the COAPT trial demonstrating improvement in survival, symptoms, and quality of life in selected patients with moderate to severe secondary MR who underwent TEER as compared to medical therapy alone.7,8
î TEER is also an option for patients with severely symptomatic with primary severe MR at high or prohibitive surgical risk who have favorable anatomy (Class IIa).
• Transcatheter mitral valve replacement is an emerging structural intervention and currently being investigated in a number of clinical trials. Currently, this technology is only reserved for degenerative MR.
Surgical Management
• Primary MR2
î Symptomatic with chronic severe primary MR (stage D) (Class I).
î Asymptomatic with chronic severe primary MR with EF ≤60% or LV end-systolic dimension ≥40 mm (stage C2; Class I).
î Chronic severe primary MR undergoing cardiac surgery for other indications (Class I).
î Repair is recommended over replacement (Class I).
î Asymptomatic patients with chronic severe primary MR (stage C1) in whom repair is highly likely (>95%) and operative mortality is low (Other presenting symptoms may be related to the cause of acute AR.
• Chronic AR: symptoms depend on the presence of LV dysfunction and whether the patient is in the compensated versus decompensated stage. Compensated patients are typically asymptomatic, whereas those in the decompensated stage may note decreased exercise tolerance, dyspnea, fatigue, and/or angina.
Physical Examination
• Acute AR
î Widened pulse pressure may be present, but it is often not present because forward SV (and therefore systolic blood pressure) is reduced.
î May hear brief soft diastolic murmur or systolic flow murmur.
î Look for evidence of aortic dissection, infective endocarditis, and characteristics associated with Marfan disease.
• Chronic AR
î LV heave; point of maximal impulse is laterally displaced.
î Diastolic decrescendo murmur heard best at left sternal border leaning forward at end-expiration (severity of AR correlates with duration, not intensity, of the murmur).
î Systolic flow murmur (mostly because of volume overload; concomitant AS may also be present).
î Widened pulse pressure (often >100 mm Hg) with a low diastolic pressure; there are numerous eponyms for the characteristic signs related to a wide pulse pressure.
Diagnostic Testing
• ECG: tachycardia, LVH, and LAE (more common in chronic AR).
• CXR: pulmonary edema, widened mediastinum, and cardiomegaly.
• TTE
î Assess LV systolic function, LV dimensions at end systole and diastole, leaflet number and morphology, assessment of the severity of AR.
î Look for evidence of endocarditis or aortic dissection, dimension of aortic root.
• TEE
î Clarify whether there is a bicuspid valve if unclear on TTE.
î Better sensitivity and specificity for aortic dissection than TTE.
î Clarify whether there is endocarditis with or without root abscess if unclear on TTE.
î Better visualization of aortic valve in patients with a prosthetic aortic valve.
• Cardiac catheterization: assessment of LV pressure, LV function, and severity of AR (via aortic root angiography) is indicated in symptomatic patients in whom the severity of AR is unclear on noninvasive imaging or discordant with clinical findings.
• MRI/CT
î Either of these may be the imaging modality of choice for evaluating aortic dimensions and/or for evaluation of aortic dissection.
î If echocardiography assessment of the severity of AR is inadequate, MRI is useful for assessing the severity of AR.
TREATMENT
The role of medical therapy in patients with AR is limited.
• Vasodilator therapy (i.e., nifedipine, ACE inhibitor, hydralazine) is indicated to reduce systolic blood pressure in hypertensive patients with AR.
• When endocarditis is suspected or confirmed, appropriate antibiotic coverage is critical.
Surgical Management
• AHA/ACC recommendations for intervention2
î Symptomatic patients with severe AR (stage D) regardless of LV systolic function (Class I).
î Asymptomatic patients with chronic severe AR and LV systolic dysfunction (EF ≤55%) (stage C2; Class I).
î Patients with severe AR (stage C or D) undergoing cardiac surgery for other indications (Class I). î Asymptomatic patients with severe AR and normal LV systolic function (EF >55%) but with severe LV dilation (LV end-systolic dimension >50 mm) (stage C2; Class IIa).
• Acute, severe AR is almost universally symptomatic and is treated surgically.
• If the aortic root is dilated, it may be repaired or replaced at the time of AVR. For patients with a bicuspid valve, Marfan syndrome, or a related genetically triggered aortopathy, surgery on the aorta should be considered at the time of AVR.
OutcomeZPrognosis
• Asymptomatic patients with normal LV systolic function (LVEF ≥55%): progression to symptoms and/or LV dysfunction approximately 6% per year.9
• Asymptomatic patients with LV dysfunction (LVEF 25% per year.9,10
• Symptomatic patients: mortality rate approximately 9.4% per year.9