Approach to Venous Thromboembolism
GENERAL PRINCIPLES
Definition
• Thrombosis refers to a blood clot that occur in veins, arteries, or chambers of the heart.
• VTE refers to deep vein thrombosis (DVT) and/or pulmonary embolism (PE).
• Thrombophlebitis consists of inflammation in a vein due to a blood clot.
• Superficial venous thrombophlebitis refers to thrombosis in a nondeep vein.
Classification
• The anatomic location of DVT/PE, clot burden, and sequelae may affect prognosis and treatment recommendations.
• DVT can be proximal or distal.
î Proximal lower extremity DVTs occur in the deep venous system at or more proximal to the popliteal vein (or the confluence of tibial and peroneal veins); distal lower extremity DVTs occur more distally in the tibial or peroneal veins.
î Proximal upper extremity DVTs occur in the subclavian, brachiocephalic, axillary, and brachial veins, whereas distal upper extremity DVTs occur in the cephalic or basilic veins.
î Other important venous thromboses sites include the vena cava (superior and inferior), abdominal veins (hepatic, portal, superior mesenteric, and splenic), pelvic veins (iliac, ovarian, penile), retinal veins, and cerebral veins, and cavernous sinus.
• The anatomic location of a PE in the pulmonary arterial system characterizes it as central/proximal (main, lobar, or segmental) or distal (subsegmental or smaller).
• PE severity classification may refer to cardiovascular dysfunction variables that define submassive PE (e.g., right ventricular [RV] strain, RV dysfunction, elevated troponin, elevated NT-proBNP) or massive PE (systemic hypotension). Severity classification may also include a risk (of short-term mortality or poor outcome) score that incorporates clinical variables (Table 20-5).
TABLE 20-5
EUROPEAN SOCIETY OF CARDIOLOGY MORTALITY RISK CLASSIFICATION OF PATIENTS WHO HAVE ACUTE PULMONARY EMBOLISM
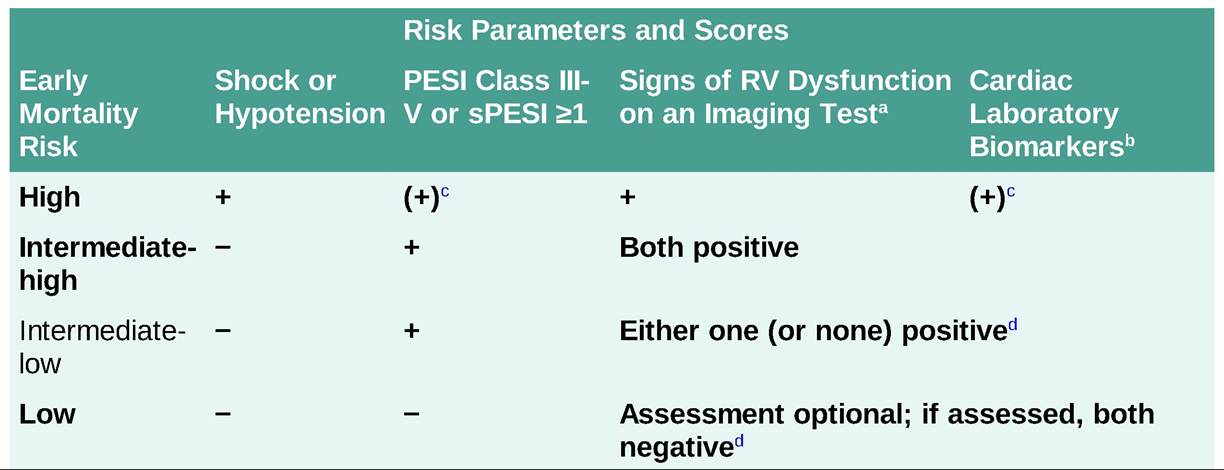
sPESI, Simplified Pulmonary Embolism Severity Index, which assigns 1 point each for: age gt; 80 years, cancer, chronic cardiopulmonary disease, HR #8805; 110, systolic BP lt; 100, and O2 saturation lt; 90%.50
LV, left ventricle; RV, right ventricle.
aEchocardiographic criteria of RV dysfunction include RV dilation and/or an increased end-diastolic RV-LV diameter ratio (e.g., #8805;1), hypokinesis of the free RV wall, or increased velocity of the tricuspid regurgitation jet. CT angiography criterion for RV dysfunction is an increased end-diastolic RV/LV diameter ratio (e.g., #8805;1.0).
bElevations in N-terminal pro-BNP or high-sensitivity troponin I or T.
cClassify shock or hypotension as high risk.
dClassify low-risk PESI (Class I-II) or sPESI patients (score of 0) who have elevated cardiac biomarkers or signs of RV dysfunction on imaging tests.
Adapted from Konstantinides SV, Meyer G, Becattini C, et al.; ESC Scientific Document Group. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur Heart J. 2020;41(4):543-603. doi:10.1093/eurheartj/ehz405. PMID: 31504429.
Epidemiology
• Without treatment, half of patients with proximal lower extremity DVT develop PE.
• DVTs in the upper extremities often occur with an indwelling catheter and may cause PE.
• Untreated acute symptomatic PE has a 10%-30% short-term mortality.51
• Patients who have hemodynamic instability associated with acute PE have a gt;15% risk of death in the subsequent 30 days, despite treatment.
• Patients who have acute PE without shock or hypotension but with signs of right ventricular dysfunction or myocardial injury have a 3%-15% 30-day mortality risk.
• Patients who have acute symptomatic PE with normal blood pressure and RV function have a 30-day mortality risk of lt;1%, low-risk.
• The 3-month mortality after the initiation of anticoagulant therapy in low-risk patients averages around 2%.52
Etiology
• Venous thromboemboli arise under conditions of blood stasis, hypercoagulability (changes in the soluble and formed elements of the blood), or venous endothelial dysfunction/injury (Virchow's triad).
• Hypercoagulable states may have an inherited or acquired etiology (see Risk Factors section).
• VTEs are classified as provoked or unprovoked, where provoked are attributed to an identifiable risk factor (e.g., surgery, oral contraception, pregnancy, immobility) and unprovoked have no identifiable
cause.
• Superficial thrombophlebitis occurs in association with IVs, varicose veins, trauma, infection, and hypercoagulable disorders.
Risk Factors
• Risk factors for VTE can be categorized as inherited, acquired, or unknown.
• Inherited thrombophilia are suggested by spontaneous/unprovoked VTE at a young age (lt;50 years), recurrent (especially unprovoked) VTE, VTE in first-degree relatives, or thrombosis in unusual anatomic locations (i.e., abdominal).
• The most common inherited risk factors for VTE include gene mutations (factor V Leiden and prothrombin gene G20210A) and deficiencies of the natural anticoagulants protein C, protein S, and AT.
• Homocystinuria, a rare autosomal recessive disorder caused by deficiency of cystathionine-#946;- synthase, leads to extremely high plasma homocysteine and causes early-onset arterial and venous thromboembolic events. However, mild elevation of homocysteine may be caused by a mutation in methylenetetrahydrofolate reductase (MTHFR) but does not cause VTE. Therefore, thrombophilia testing should not include MTHFR mutation testing.
• Spontaneous/unprovoked VTE in unusual locations, such as cavernous sinus, mesenteric vein, or portal vein, may be the initial presentation of paroxysmal nocturnal hemoglobinuria (PNH) or myeloproliferative disorders (JAK2 mutation).
• Spontaneous (unprovoked) VTEs have a high risk of recurrence (8%-10% per year) after stopping anticoagulant therapy, regardless of the presence of an inherited thrombophilia.
• Acquired hypercoagulable states may arise secondary to malignancy, immobilization, infection, trauma, surgery, collagen vascular diseases, nephrotic syndrome, HIT, DIC, medications (e.g., estrogen), and pregnancy.
• Acquired autoantibodies associated with HIT and antiphospholipid syndrome (APS) can cause arterial or venous thrombi.
• APS is a hypercoagulable disorder that requires the presence of at least one clinical and one laboratory criterion.53
î APS clinical criteria:
#9632; Unprovoked arterial or venous thrombosis in any tissue or organ or
#9632; Pregnancy morbidity of (1) unexplained late fetal death, (2) premature birth complicated by eclampsia, preeclampsia, placental insufficiency, or (3) #8805; three unexplained consecutive spontaneous abortions at lt;10 weeks of gestation or one at #8805;10 weeks.
î APS laboratory criteria:
#9632; Presence of autoantibodies such as lupus anticoagulant (LA), anticardiolipin, or #946;2-glycoprotein- 1 antibodies. Do not test for LA while the patient is on a DOAC because of the high risk of a false negative test result.54
î LAs may prolong the aPTT or PT/INR without predisposing to bleeding.
#9632; Approximately 10% of patients with SLE have an LA; however, most patients with an LA do not have SLE.
#9632; Confirmation of positive autoantibody tests (must be done at least 12 weeks apart).
î APS may include other features, such as thrombocytopenia, valvular heart disease, livedo reticularis, neurologic manifestations, and nephropathy.
Prevention
Identifying patients at high risk for VTE and instituting prophylactic measures should remain a high priority (see Chapter 1, Inpatient Care in Internal Medicine).
DIAGNOSIS
Clinical Presentation
• Lower or upper extremity DVT symptoms commonly include pain, edema, redness, and warmth.
• Superficial thrombophlebitis presents as a tender, warm, erythematous, and palpable thrombosed vein. An accompanying DVT may produce pain and swelling.
• Likelihood of a PE increases in a patient suspected of having it in the setting of: history of VTE, active cancer, surgery or immobility in the past 4 weeks, certain medications (e.g., estrogen), hemoptysis, older age, abnormal vital signs (tachycardia and hypoxia), signs and symptoms of DVT, or high suspicion of PE by the clinician (e.g., sudden onset of shortness of breath, hemoptysis, and pleuritic chest pain).55,56
Differential Diagnosis
• The differential diagnoses of lower extremity DVT include cellulitis, Baker cyst (behind knee), hematoma, venous insufficiency, postphlebitic syndrome, lymphedema, sarcoma, arterial aneurysm, myositis, rupture of the gastrocnemius, and abscess.
• Symmetric, bilateral lower extremity edema suggests heart, renal, or liver failure as the cause of the signs and symptoms, but it does not exclude the presence of DVT.
• The differential diagnosis of PE based on the presenting symptoms (e.g., chest pain, dyspnea, hemoptysis) or signs (e.g., hypoxemia, pleural effusion, pulmonary infiltrate) includes dissecting aortic aneurysm, pneumonia, acute bronchitis, pericardial or pleural disease, heart failure, costochondritis, rib fracture, and myocardial ischemia.
Diagnostic Testing
CLINICAL PROBABILITY ASSESSMENT
• Clinical decision rules help to exclude VTE when used in combination with other diagnostic tests (such as normal d-dimer).
î Clinical predictors of DVT from Wells criteria include: history of DVT, paralysis/paresis/immobilization of the leg, recently bedridden, major surgery within 4 weeks, active cancer, leg vein tenderness, swelling of entire leg, calf diameter gt; 3 cm larger than other calf, pitting edema confined to symptomatic leg, dilated collateral superficial leg veins, and alternative diagnoses less likely than DVT. Outpatients who have one or fewer of these predictors (i.e., low Wells score) are unlikely to have a DVT.57
î Pretest assessment of the probability of a DVT provides useful information when combined with the results of a venous compression ultrasound, a d-dimer test, or both, in determining whether to exclude or accept the diagnosis of DVT or to perform additional imaging studies.57
• Validated clinical risk factors for a PE in outpatients who present to an emergency department include signs and symptoms of DVT, high clinical suspicion of PE (e.g., recent surgery or COVID-19 infection), tachycardia, immobility in the past 4 weeks, history of VTE, active cancer, hemoptysis,58 and lack of an alternative diagnosis that is at least as likely as PE. Patients who have one or fewer of these predictors (i.e., a low simplified Wells score) are unlikely to have a PE.
î The combination of a low (simplified) Wells score and a normal d-dimer essentially rules out a
PE.
59
o A normal d-dimer and a negative chest CT essentially rule out PE, and a lower extremity compression ultrasound does not typically assist further with ruling in or out the presence of a PE.60
LABORATORIES
• d-dimer and fibrin degradation products may increase during VTE.
î Since multiple conditions may elevate d-dimer, it has a low positive predictive value (PPV) and specificity for VTE; patients with suspected VTE and an elevated d-dimer require further diagnostic testing.
î A sensitive quantitative d-dimer assay has a high enough NPV to exclude a DVT when the objectively defined clinical probability is low and/or a noninvasive test is negative.61,62 In the setting of a moderate to high clinical pretest probability (e.g., patients with cancer or COVID-19), a negative d-dimer does not have sufficient NPV to exclude a DVT or PE,63,64 so d-dimer testing is not useful in this setting.
î Compared to a fixed d-dimer cutoff of 500 #956;g#8725;L, an upward age adjustment of the cutoff (age ? 10 in patients at least age 50 years) will increase the number of patients who can have PE excluded based on the combination of nonelevated d-dimer and objective clinical probability assessment (i.e., low-intermediate or unlikely pretest probability).65
• In the setting of spontaneous VTE in unusual sites and hemolytic anemia, use peripheral blood flow cytometry to assess for PNH.
IMAGING
• DVT-specific testing
° Initial diagnostic imaging for suspected acute DVT almost exclusively consists of venous compression ultrasound (CUS),66 called duplex examination when performed with Doppler testing,67 although some other diagnostic options include magnetic resonance venography, CT venography, and venography.
#9632; CUS has a high sensitivity in symptomatic patients and a low sensitivity in asymptomatic patients.
#9632; CUS has a low sensitivity for detecting distal DVT, and it may fail to visualize parts of the upper extremity venous system, iliac veins, or pelvic veins.
#9632; CUS may have difficulty distinguishing between acute and chronic DVT.
#9632; Lower extremity venous CUS may help diagnose or exclude VTE in patients who have suspected PE and a nondiagnostic ventilation/perfusion (V#8725;Q) scan, a nondiagnostic or negative chest CT with high suspicion of PE, or a contraindication to or difficulty completing imaging for PE (see PE-specific testing section).
î Serial testing can improve the diagnostic yield of CUS. If a patient with a clinically suspected lower extremity DVT has a negative initial ultrasound and no satisfactory alternative explanation, one can withhold anticoagulant therapy and repeat testing at least once 3-14 days later.
° Patients who have superficial venous thrombosis should undergo venous CUS testing because of the high risk of having concomitant DVT.68
• Acute PE-specific testing
î CT pulmonary angiogram
#9632; Chest CT pulmonary angiography requires IV administration of iodinated contrast. Thus, contraindications to CT angiogram include renal dysfunction and dye allergy. For patients with a
contraindication to CT, consider using MR pulmonary angiography or V/Q scan.69
#9632; The sensitivity of CT pulmonary angiography for PE improves by combining CT results with objective grading of clinical suspicion.
#9632; Clinical suspicion discordant with the objective test finding (e.g., high suspicion with a negative CT scan or low suspicion with a positive CT scan) should lead to further testing.
#9632; Advantages of CT scan over V/Q scan when assessing for PE include fewer indeterminate studies and the ability to assess for alternative or concomitant diagnoses, such as dissecting aortic aneurysm, pneumonia, and malignancy.70
#9632; For patients who have a contraindication to CT, a lower extremity venous compression ultrasound can be helpful, because proximal DVT may serve as a surrogate for the diagnosis of PE.
î V/Q scan
#9632; V/Q scans administer radioactive material (via inhaled and IV routes).
#9632; V/Q scans are classified as normal, nondiagnostic (i.e., very low probability, low probability, intermediate probability), or high probability for PE.
#9632; V/Q scans are most useful in patients who have a normal CXR because nondiagnostic V/Q scans commonly occur in the setting of an abnormal CXR.
#9632; Use of clinical suspicion improves the accuracy of V/Q scanning, resulting in a NPV of 96% for low pretest clinical suspicion of PE and a normal V/Q scan result, and a PPV of 96% for high pretest suspicion of PE and a high-probability V/Q scan result.71
î Pulmonary angiography
#9632; Angiography requires placement of a pulmonary artery catheter, infusion of IV contrast, and exposure to radiation.
#9632; Contraindications to angiography include renal dysfunction and dye allergy.
#9632; Less invasive tests (i.e., CT angiography) with similar or better diagnostic accuracy have mostly replaced pulmonary angiography for acute PE diagnostic testing.
#9632; Electrocardiogram, troponin and brain natriuretic peptide (BNP) levels, arterial blood gas, CXR, and echocardiogram may to help assess clinical probability of PE, cardiopulmonary reserve, and potential to benefit from thrombolysis (see thrombolytic therapy in Medications section), but these tests do not rule out or rule in PE, with the exception of seeing an intracardiac clot with echocardiography.
#9632; Studies do not support extensive screening for an associated occult malignancy in patients with a first, unprovoked VTE.72 However, such patients should undergo a comprehensive history and physical examination, routine blood work, age- and gender-appropriate cancer screening, and specific cancer screening tests indicated for distinct populations (e.g., chest CT to search for lung cancer in those age 50 or older with a history of smoking).
TREATMENT
• VTE therapy should aim to prevent recurrent VTE, consequences of VTE (i.e., postphlebitic syndrome [i.e., pain, edema, and ulceration], pulmonary arterial hypertension, and death), and complications of therapy (e.g., bleeding).
• Clinicians should perform standard laboratory tests (i.e., CBC, PT/INR, and aPTT) and assess bleeding risk before starting an anticoagulant.
• Unless contraindications exist, initial treatment of VTE should consist of anticoagulation with IV UFH, SC LMWH, SC pentasaccharide (fondaparinux), or a rapid-onset DOAC (see Medications).
Medications
• Anticoagulants, oral
î Direct oral anticoagulants (DOACs) (Table 20-6) have one of two primary mechanisms of action: thrombin inhibition (dabigatran) or Xa inhibition (rivaroxaban, apixaban, edoxaban, and betrixaban).
#9632; As compared to warfarin, DOACs have more rapid onset, wider therapeutic window, and more predictable pharmacokinetics. These features allow patients with a new VTE to begin apixaban or rivaroxaban immediately, without the need for an overlapping parenteral agent. In contrast, dabigatran and edoxaban require at least 5 days of initial parenteral anticoagulation if prescribed for a new VTE. None of the DOACs need INR monitoring or dose adjustments in patients with normal renal function, but the initial dose of some DOACs for a new VTE is higher than the maintenance dose (rivaroxaban 15 mg twice daily for 3 weeks then 20 mg daily, or apixaban 10 mg daily twice daily then 5 mg twice daily).
TABLE 20-6
| ANTICOAGULANTS FOR TREATMENT OF VENOUS 1 | #915;HROMBOEMBOLISM (VTE) | |||
| Anticoagulant | Mechanism of Action | Initial Treatment Dose(s) | Extended Duration Dose | Contraindications' |
| Parental Agents | ||||
| Dalteparinb | FXa gt; FIIa inhibition | 200 IU/kg SC daily | 150 IU/kg SC daily | HIT; sensitivity to pork |
| Enoxaparin | FXa gt; FIIa inhibition | 1 mg/kg SC q12h or 1.5 mg/kg SC q24h; lower dose if CrCl lt; 30 mL/min | 1 mg/kg SC q12h or 1.5 mg/kg SC q24h; lower doses if CrCl lt;30 mL/min | HIT; sensitivity to pork |
| Fondaparinux | Binds to antithrombin, primarily inhibiting FXa | Weight lt; 50 kg: 5 mg SC daily Weight 50-100 kg: 7.5 mg SC daily Weight gt; 100 kg: 10 mg SC daily | NA | CrCl lt; 30 mL/min |
| Heparin (UFH) | Binds to antithrombin | Continuous IV: Goal aPTT 2.0-2.5? normal range | NA | HIT; sensitivity to pork |
| Tinzaparinc | FXa gt; FIIa inhibition | 175 IU/kg SC daily | NA | HIT, not available in US |
| Oral Agents | ||||
| Apixaban | Direct FXa inhibitor | 10 mg bid ? 7 d, then 5 mg daily | 2.5 or 5 mg bid | Pregnancy |
| Dabigatran | Direct thrombin (FIIa) inhibitor | Initially treat with parenteral anticoagulant for #8805;5 | 150 mg bid (CrCl gt; 30 mL/min) | Pregnancy, CrCl lt; 30 mL/min |
| Edoxaban | Direct FXa inhibitor | Initially treat with parenteral anticoagulant for #8805;5 d | 30 or 60 mg daily (depending on CrCl, body weight, and use of P-gp inhibitor) | Pregnancy |
| Rivaroxaban | Direct FXa inhibitor | 15 mg bid ? 21 d, then 20 mg daily | 10 or 20 mg daily; | Pregnancy, CrCl lt; 30 mL/min |
| Warfarin | Vitamin K antagonist | 2-10 mg (see www.warfarindosing. org); overlapped for #8805;5 d with a faster-acting anticoagulant | Adjusted per INR | 1st trimester of pregnancy |
aPTT, activated partial thromboplastin time; CrCl, creatinine clearance; FIIa, factor IIa; FXa, factor Xa; HIT, heparin-induced thrombocytopenia; INR, international normalized ratio; P-gp, P-glycoprotein.
aInvasive procedures (e.g., neuraxial anesthesia), bleeding, and bleeding diathesis (e.g., thrombocytopenia) are contraindications to all anticoagulants.
bFDA-approved only for VTE in cancer patients.
cNot available in the United States.
#9632; Compared to warfarin, DOACs have a lower risk of intracranial hemrrhage.73
#9632; Issues of concern include the risk of thrombosis due to missed doses and increased bleeding risk due to severe renal dysfunction. DOACs are not recommended in patients who have triple positive APS given their increased risk of arterial thromboses when compared to warfarin.
î Warfarin, an oral anticoagulant, inhibits reduction of vitamin K to its active form, which leads to decreased synthesis of and subsequent depletion of the vitamin K-dependent clotting factors II, VII, IX, and X, and proteins C, S, and Z.
#9632; Treatment of DVT/PE with warfarin requires overlap therapy with a parenteral anticoagulant (UFH, LMWH, or pentasaccharide) for at least 4-5 days and until the INR reaches 2.0 or higher.74 For DVT/PE, use a target INR range of 2-3.
#9632; The starting dose of warfarin depends on many factors and ranges from 2 to 4 mg in older or petite patients to 10 mg in young, robust patients (www.warfarindosing.org). Patients with known polymorphisms in genes for cytochrome P450 2C9 or vitamin K epoxide reductase (VKORCl) benefit from lower-dose warfarin initiation.75
#9632; Warfarin dosing adjustments depend on INR results.
#9632; Warfarin is teratogenic during the first trimester.
#9632; For outpatients starting warfarin, INR monitoring can be once or twice weekly initially with the interval between INRs gradually lengthening to monthly once the dose is stable.
#9632; Warfarin dose adjustments after the first few weeks of therapy typically change the weekly dose by 10%-25%.
#9632; Starting or discontinuing medications that affect warfarin metabolism or binding, especially amiodarone, certain antibiotics (e.g., rifampin, sulfamethoxazole), or antifungal drugs (e.g., fluconazole), should trigger more frequent INR monitoring and may require dose adjustments.
#9632; In eligible patients, home INR monitoring may improve INR control and patient satisfaction.76
• Anticoagulants, parenteral
î UFH indirectly inactivates thrombin and factor Xa via AT.
#9632; At usual doses, UFH prolongs aPTT and thrombin time, and may mildly prolong the PT/INR.
#9632; Because the anticoagulant effects of UFH normalize within hours of discontinuation, and protamine sulfate reverses it even faster, UFH is the anticoagulant of choice during initial therapy for patients with a high risk of bleeding or those who will likely undergo an invasive procedure (e.g., ICU patients).
#9632; For therapeutic anticoagulation for VTE, UFH is usually administered IV with a bolus (e.g., 80 units/kg after a VTE) followed by continuous infusion (e.g., 18 units/kg/h) that has a dose titration based on standard protocols (i.e., heparin nomogram), usually to a goal aPTT of 2- to 2.5-fold of normal range (Table 20-6).
#9632; UFH is the anticoagulant of choice for inpatients with a mechanical heart valve who need bridging of anticoagulation.
î LMWHs, produced by chemical or enzymatic cleavage of UFH, indirectly inactivate thrombin and factor Xa via AT.
#9632; LMWHs minimally prolong the aPTT.
#9632; LMWH treatment does not require Factor Xa monitoring, except in special circumstances: renal dysfunction, morbid obesity, or pregnancy.77 Therapeutic anticoagulation will have a peak factor Xa level, measured 4 hours after a dose, of 0.6-1.0 IU/mL for q12h dosing and 1-2 IU/mL for q24h dosing.78
#9632; Different LMWH preparations have different dosing recommendations (Table 20-6). The usual prophylactic dose of enoxaparin is 40 mg SC daily. However, higher doses are more effective among inpatients with obesity such as BMI gt; 40 kg/m2. Higher doses (e.g., enoxaparin 1 mg/kg twice daily) can be used for thromboprophylaxis among noncritically ill patients with COVID.79
#9632; Given their renal clearance, LMWHs are generally avoided in patients with creatinine clearance (CrCl) lt;10 mL/min, and they should be dose-adjusted in patients who have a CrCl of 10-30 mL/min (e.g., enoxaparin 1 mg/kg daily instead of 1 mg/kg twice daily).
#9632; Pregnant women (without artificial heart valves) who have VTE should be treated with LMWH.
#9632; Patients with cancer and VTE should receive anticoagulation for more than 3 months and until cancer resolution or development of a contraindication.80,81 They can be treated with LMWHs (e.g., with dalteparin (200 IU/kg SC daily ? 1 month, then 150 IU/kg SC daily),82 or a DOAC: apixaban (10 mg twice daily for the first 7 days, followed by 5 mg twice daily),83 edoxaban (60 mg p.o. daily),84 or rivaroxaban (15 mg twice daily for the first 21 days, then 20 mg daily).85 Although warfarin (INR 2-3) has similar mortality to LMWHs and DOACs in patients with cancer and VTE, warfarin has higher rates of recurrent VTE.86
î Fondaparinux, a synthetic pentasaccharide, indirectly inhibits factor Xa via AT.
#9632; The fondaparinux dose for VTE ranges from 5 to 10 mg SC daily.87(Table 20-6).
#9632; Similar to the LMWHs, factor Xa monitoring is not used routinely, and fondaparinux undergoes renal clearance.
#9632; Though not FDA-approved for use with suspected immunologic HIT, fondaparinux also is used in this setting.88
î Argatroban is a synthetic direct thrombin inhibitor used for immunologic HIT therapy.
#9632; Argatroban has a half-life of lt;1 hour, and a reversal agent is not available.
#9632; Argatroban is infused IV at an initial rate of #8804;2 #956;g#8725;kg#8725;min. Special populations require lower initial infusion rates: patients with recent cardiac surgery, heart failure, hepatic dysfunction, or anasarca.89
#9632; aPTT monitoring should occur 2 hours after beginning the infusion, and the infusion rate should undergo adjustment to achieve a therapeutic aPTT (1.5-3.0 times the baseline aPTT).
#9632; Once the platelet count has recovered, before conversion to warfarin, argatroban therapy should be overlapped with warfarin therapy for at least 5 days and until a therapeutic INR due to warfarin is achieved.
#9632; INR monitoring during argatroban and warfarin coadministration may cause confusion; for an INR gt; 4, discontinue argatroban, remeasure the INR within 4-6 hours, and then restart the argatroban (and adjust the warfarin dose).
î Bivalirudin is a direct thrombin inhibitor with an indication for treatment of immunologic HIT in the setting of percutaneous coronary intervention in patients receiving ASA.
#9632; Bivalirudin has a half-life of 25 minutes in patients with normal renal function.
#9632; Bivalirudin requires reduction of the infusion rate in patients with renal insufficiency.
#9632; Bivalirudin dosing for HIT should start at a rate of 0.15-0.20 mg/kg/h IV with titration to a target aPTT 1.5-2.5 times baseline.24,90
#9632; aPTT monitoring during bivalirudin therapy should occur 2 hours after a dose change.
#9632; The interpretation of the INRs in patients receiving warfarin must consider the increased PT/INR caused by bivalirudin.
• Thrombolytic therapy
î In the life-threatening situation of an acute PE associated with shock or persistent hypotension from RV overload, rapid reperfusion treatment and cardiorespiratory support relieves the RV overload and prevents hemodynamic deterioration.
° Thrombolytic therapy (e.g., alteplase or recombinant tissue plasminogen activator [rtPA] as a 100mg IV infusion over 2 hours) is indicated for patients who have hemodynamically unstable (“massive”) PE who do not have a contraindication (e.g., a high risk of bleeding).91-93
î Patients receiving anticoagulation for acute PE who subsequently have a cardiac arrest from PE- associated RV failure or a suspected PE recurrence may benefit from thrombolytic therapy,92,93 such as a (non-FDA-approved) 50 mg IV bolus dose of rtPA91 or a (non-FDA-approved) tPA dose of 10 mg IV bolus followed by drip of 40 mg IV over 15-30 minutes.
î In patients who have high intermediate-risk/submassive PE, fibrinolytic therapy prevents hemodynamic decompensation but increases the risk of intracranial hemorrhage/stroke.91,94,95
î Thrombolytic therapy (administered either IV or by catheter-directed thrombolysis) for DVT increases the risk of hemorrhage and does not prevent postthrombotic syndrome, with the possible exception of patients who have massive iliofemoral DVT.96
• Duration of anticoagulation for DVT or PE
î An individual’s risk of recurrent VTE, risk of hemorrhage, risk of adverse outcomes, and preferences should determine the duration of anticoagulation.
î For treatment of provoked proximal DVT or provoked PE occurring in the setting of a surgical or nonsurgical (e.g., immobility, pregnancy) transient risk factor, 3 months of anticoagulation is sufficient because these events have low recurrence risk (#8804;2% per year).93
î For unprovoked PE, we recommend anticoagulation for gt;3 months in patients with low to moderate
risk of bleeding.81,93,97
î Patients with cancer and VTE should continue anticoagulation until cancer resolution or development of a contraindication.80,81
î For patients with a first VTE and an inherited hypercoagulable risk factor, consider an extended anticoagulation duration:
#9632; Heterozygous factor V Leiden or heterozygous prothrombin 20210A only modestly increases the odds of recurrence (relative risk, 1.6 and 1.4, respectively), so recommendation for anticoagulation duration should not change based on these.
#9632; Deficiency of protein S, protein C, or AT carries a high risk of recurrence; long-term anticoagulation is recommended.
#9632; APS or two inherited risk factors have a very high risk of recurrence, so indefinite anticoagulation is recommended.
î Patients with recurrent unprovoked VTE should receive long-term anticoagulation, unless a contraindication develops.81,97
î Long-term anticoagulation after an unprovoked VTE reduces the risk of recurrence but increases the risk hemorrhage in comparison to short-term anticoagulation.
#9632; The relative risk reduction of VTE depends on the secondary thromboprophylaxis: it is 32% with low-dose ASA.98,99 More effective therapies are: rivaroxaban 20 mg or 10 mg daily,100 apixaban 5 or 2.5 mg twice daily,101 dabigatran 150 mg twice daily,100,102 warfarin (target INR 2-3), or LMWH.
î Effective LMWHs for extended secondary prophylaxis include enoxaparin (1.5 mg/kg daily or 1 mg/kg twice daily) and dalteparin 150 IU#8725;kg daily.
• Nonpharmacologic therapies
î Leg elevation reduces edema associated with DVT.
î Ambulation is encouraged for patients with DVT, for improvement of pain and edema.
î Fitted below-the-knee graduated compression stockings can reduce swelling after DVT, but do not prevent DVT recurrence, and the reduction of postthrombotic syndrome is controversial.103
î Inferior vena cava (IVC) filters can be placed for acute VTEs when there are absolute contraindications to anticoagulation (e.g., bleeding). When transient contraindications resolve, patients should undergo full-dose anticoagulation.
î Prophylactic IVC filters in patients with acute VTE reduce the short-term risk of nonfatal PE, but they do not decrease mortality, and they increase DVT recurrence.104
#9632; If IVC filters are used, temporary/retrievable IVC filters should be used, and they should be removed when no longer indicated.
Surgical Management
SURGICAL EMBOLECTOMY
• Surgical embolectomy has a role in patients who have massive/high-risk PE and a contraindication to thrombolytic therapy or a failure to respond to thrombolytic therapy. Depending on center expertise, catheter-based interventions should be considered as a potential alternative option to surgical embolectomy.98
• Patients who have a right heart thrombus that straddles the interatrial septum via a patent foramen ovale/atrial septal defect should be considered for surgical embolectomy.105
• Embolectomy for free-floating right heart thrombus remains controversial.106
SPECIAL CONSIDERATIONS
Anticoagulant Bridging
• Perioperative management of anticoagulation requires coordination with the surgical service (see Perioperative Medicine in Chapter 1) to address timing of interventions and therapeutic changes with the aim of VTE and bleeding prevention.
• Invasive procedures usually require discontinuation of anticoagulation.
î For patients receiving warfarin, stop the warfarin therapy 4-5 days before the invasive procedure.
î BRIDGE study showed that in patients with atrial fibrillation who had warfarin treatment interrupted for an elective procedure, forgoing bridging anticoagulation was noninferior to perioperative bridging with LMWH for the prevention of arterial thromboembolism and decreased the risk of major bleeding.107
î In situations where a clinician aims to minimize the patient's time off therapeutic anticoagulation (such as mechanical valve or APS), initiate parenteral anticoagulation (IV UFH or LMWH) when the INR becomes subtherapeutic, stop the parenteral anticoagulation 6-12 hours before the procedure, and resume anticoagulation as soon as hemostasis and bleeding risk reach an acceptable level, typically within 24 hours.108
î PAUSE regimen (including holding the DOAC 1 day before a low-bleeding-risk procedure and 2 days before a high-bleeding-risk procedure) is recommended for patients with AF on DOACs that requires interruption of anticoagulation.109
• Studies are needed to address the risks and benefits of anticoagulation for isolated subsegmental PE.
• Upper extremity acute DVT should receive standard-duration (e.g., 3 months) anticoagulation.110 DVT associated with a functioning central venous catheter does not require catheter removal, but anticoagulation should continue as long as the catheter remains in place.
• Isolated calf acute DVT without symptoms or risk factors for extension may undergo serial imaging in 1-2 weeks instead of anticoagulation. Otherwise, treat with 6-12 weeks of anticoagulation.111
• Supe rficial ve in thrombophle bitis (SVT)
î Small SVTs (lt;5 cm in length) and SVT associated with IV infusion therapy do not require anticoagulation; treatment consists of oral NSAIDs and warm compresses.
î Treatment of extensive SVT (e.g., gt;5 cm in length) with fondaparinux (2.5 mg SC daily for 45 days)68 or rivaroxaban 10 mg daily112 decreases the incidence of SVT recurrence, SVT extension, and VTE but increases the risk of bleeding.113
î Recurrent SVT may be treated with anticoagulation or vein stripping.113
• Chronic PE occurs in 2%-4% of patients with PE,114 and patients with this disorder should undergo evaluation for chronic thromboembolic pulmonary hypertension (CTEPH). Additionally, patients who have PH associated with acute PE should undergo evaluation for resolution of PH. Continued PH should lead to further testing (e.g., V/Q scan). Those diagnosed with CTEPH should undergo extended- duration anticoagulation, consideration of riociguat therapy,115 and evaluation for possible pulmonary thromboendarterectomy.
Complications
• Bleeding is the major complication of anticoagulation.
î Patients taking anticoagulants have a major bleeding rate of 1%-3% per year.
î Concomitant use of antiplatelet agents increases the risk of bleeding. Major bleeding in patients taking antiplatelet agents can be treated with DDAVP (Desmopressin) 0.3-0.4 #956;g#8725;kg IV
î Major bleeding after an acute VTE often leads to the discontinuation of anticoagulation and consideration of a temporary or permanent IVC filter. If the bleeding risk is resolved, the anticoagulant should be resumed and any temporary IVC filter can be retrieved.
• Warfarin-associated INR elevation in asymptomatic patients
î For an asymptomatic minor INR elevation (INR lt; 5), hold or reduce the warfarin dose until the INR returns to a safe range, and then resume warfarin at a reduced dose.
î For an asymptomatic moderate INR elevation 5 #8804; INR lt;10 in an asymptomatic patient, hold one or more warfarin doses. Oral vitamin K1 is not needed for the INR to decline.116
î For an asymptomatic severe INR elevation (INR #8805; 10), hold warfarin, consider checking for a spurious INR result, and consider treatment with vitamin K (e.g., oral vitamin K1 2 mg).117
• Bleeding with warfarin
î For patients who have warfarin-associated bleeding and an elevated INR, give vitamin K replacement PO or IV IV vitamin K carries the risk of anaphylactoid reactions, so the oral route is preferred unless more rapid INR correction is necessary. With adequate replacement therapy, the INR will fall within 12 hours and normalize in 24-48 hours. Treat serious hemorrhage with IV vitamin K (10 mg) by slow infusion (over 30 minutes) and with IV 4-factor PCC (e.g., Kcentra 35 units of Factor IX/kg body weight [up to 3500 units]).118 When 4-factor PCC is not available, use three-factor PCC and/or FFP (two or three units) Because of the long half-life of warfarin (approximately 36 hours), repeat the vitamin K treatment (e.g., oral vitamin K) every 8-12 hours to prevent INR rebound.
î Although expensive and potentially thrombotic,119 rFVIIa may stop life-threatening warfarin- associated (elevated INR) bleeding.
• Bleeding with UFH, LMWH, and pentasaccharide
î Discontinuation usually sufficiently restores normal hemostasis.
î With moderate to severe bleeding, FFP may reduce bleeding.
î For patients receiving UFH who develop major bleeding, heparin can be completely reversed by infusion of protamine sulfate in situations where the potential benefits outweigh the risks (e.g., intracranial bleed, epidural hematoma, retinal bleed).
î Approximately 1 mg of protamine sulfate IV neutralizes 100 units of heparin, up to a maximum dose of 250 mg. The dose can be given as a loading dose of 25-50 mg by slow IV injection over 10 minutes, with the rest of the dose over 12 hours.
î For major bleeding associated with LMWH, protamine sulfate neutralizes only approximately 60% of LMWH.120 Protamine does not reverse pentasaccharide (e.g., fondaparinux).
î For patients with serious bleeding on fondaparinux, aPCC (20 IU/kg)121 or andexanet alfa (see below) may be used.
• Bleeding with direct oral anticoagulants (DOACs)
î Reversal of dabigatran: Idarucizumab (5 g IV) is a monoclonal antibody that binds to dabigatran with gt;350-fold affinity compared to thrombin and neutralizes its activity in minutes.122 Because the majority of dabigatran remains unbound in plasma, hemodialysis can also decrease dabigatran concentration.
î Reversal of factor Xa inhibitors: Andexanet alfa (coagulation factor Xa inactivated-zhzo) is a recombinant, modified human factor Xa decoy protein that binds and inactivates factor Xa inhibitors; it also inhibits tissue factor pathway inhibitor (TFPI), thus increasing tissue factor-associated thrombin generation.123 Dosing includes a 400-800 mg bolus at 30 mg/min followed by followed by 4-8 mg/min for up to 120 min. Four-factor PCC (e.g., Kcentra 35 units of Factor IX/kg body weight [up to 3500 units]) can reverse bleeding from DOACs.124
• Warfarin-induced skin necrosis, associated with rapid depletion of protein C, may rarely occur (incidence lt;0.1%) during initiation of warfarin therapy.
î Necrosis occurs most often in areas with a high percentage of adipose tissue, such as breast tissue, flank, hips, and thighs, and it can be life-threatening.
î Therapeutic anticoagulation with an immediate-acting anticoagulant (e.g., UFH, LMWH) and/or avoiding “loading doses” of warfarin prevents warfarin-induced skin necrosis.
Monitoring/Follow-Up
• For a suspicious clinical presentation, testing for intrinsic hypercoagulable risk factors should wait until the patient is in stable health and off anticoagulation therapy for at least 2 weeks (e.g., at the end of a standard course of treatment) to avoid false-positive results for nongenetic testing.
î Although uncommon, if reasons exist to screen for hypercoagulable risk factors around the time of diagnosis, collect blood for factor V Leiden and prothrombin gene mutations and LA.
î If done, blood collection for protein C, protein S, and AT activity and antigen level testing should occur while patients are not on anticoagulation and should be avoided in the setting of acute VTE. If testing occurs near the time of the acute VTE, normal protein C, protein S, and AT tests rule out congenital deficiencies, and abnormally low results require confirmation through repeat testing (or screening first-degree relatives).
î Although testing for PE in patients with DVT and testing for DVT in patients with PE will produce many positive findings, such testing rarely affects therapy.
• Outpatient therapy is appropriate for most DVTs and for low-risk PEs.125