Bloodstream Infections and Catheter-Related Bloodstream Infections
Bloodstream Infections
GENERAL PRINCIPLES
• Bloodstream infections (BSIs) are a major cause of morbidity and mortality despite available antimicrobials and supportive care.
• Community-acquired BSI is defined by positive blood cultures obtained in the outpatient setting or a rising incidence of acute bacterial endocarditis (ABE) and health care-associated endocarditis (related to IV catheters and invasive procedures).
• Enterococcus species cause 5%-10% of cases of subacute bacterial endocarditis (SBE).
• Bacteremia from distant foci of infection or dental procedures are frequent seeding events.
• Streptococcus gallolyticus (former S. bovis) bacteremia and endocarditis are associated with lower gastrointestinal tract disease, including neoplasms. Groups B and G streptococcal endocarditis may also be associated with large intestinal pathology.
• Gram-negative and fungal IEs occur infrequently and are usually associated with injection drug use or prosthetic heart valves.
• Early prosthetic valve endocarditis (PVE) (within the first year of surgery) commonly occurs in the first 2 months and is typically caused by S. aureus, coagulase-negative staphylococci, gram-negative bacilli, and Candida spp. Late-onset PVE is caused by the same organisms seen in NVIE.
• Coagulase-negative staphylococci (e.g., Staphylococcus epidermidis) primarily occur in patients with prosthetic heart valves, although NVIE is increasing, particularly in healthcare settings. Staphylococcus Iugdunensis is associated with a high rate of perivalvular extension and metastatic spread, resembling S. aureus clinically.
• HACEK is an acronym for a group of fastidious, slow-growing, gram-negative bacteria (H aemophilus, A ggregatibacter, C ardiobacterium, E ikenella, and K ingella species) that account for 5%-10% of community-acquired cases of IE.
Risk Factors
Acquired structural heart disease (e.g., degenerative valve disease, rheumatic heart disease), congenital disease (e.g., bicuspid aortic valve, ventricular septal defect), injection drug use, prosthetic heart valves, intravascular devices, chronic hemodialysis, and a prior history of endocarditis are predisposing factors for endocarditis.
DIAGNOSIS
The modified Duke criteria (Tables 14-5 and 14-6) incorporate microbiologic, pathologic, echocardiographic, and clinical findings and are widely used but should not replace clinical judgment.
TABLE 14-5
MODIFIED DUKE CRITERIA FOR THE DIAGNOSIS OF INFECTIVE ENDOCARDITIS11
Major Criteria
Positive Blood Cultures
1. Two separate blood cultures with viridans group streptococci, Streptococcus gallolyticus (formerly bovis), Staphylococcus aureus, HACEK group, or community-acquired enterococci, in the absence of a primary focus of infection.
2. Persistently positive blood cultures: At least two blood cultures drawn more than 12 h apart OR all of three or a majority of four separate blood cultures, drawn 1 h apart.
3. Single positive blood culture for Coxiella burnetii or antiphase 1 IgG antibody titer ≥E800.
Evidence of Endocardial Involvement
Positive echocardiogram for IE, such as:
1. Oscillating intracardiac mass on a valve or supporting structure, in the path of regurgitant jets, or on implanted material in the absence of another anatomic explanation
2. Abscess
3. New partial dehiscence of a prosthetic valve
4. New valvular regurgitation (change in preexisting murmur not sufficient)
Minor Criteria
1. Predisposing heart condition or IV drug use
2. Fever ≥38°C (100.4°F)
3. Vascular phenomena: Arterial emboli, septic pulmonary infarcts, mycotic aneurysm, intracranial or conjunctival hemorrhage, Janeway lesions
4. Immunologic phenomena: Glomerulonephritis, Osler nodes, Roth spots, rheumatoid factor
5. Microbiologic evidence: Positive blood culture but not meeting major criteria OR serologic evidence of infection with an organism consistent with IE
HACEK, Haemophilus, Aggregatibacter, Cardiobacterium, Eikenella, Kingella; IE, infective endocarditis.
Modified from Li JS, Sexton DJ, Mick N, et al. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin Infect Dis. 2000;30(4):633-638, by permission of Oxford University Press.
TABLE 14-6
DEFINITION OF INFECTIVE ENDOCARDITIS (IE) BY MODIFIED DUKE CRITERIA11
Definite IE
Pathologic criteria:
Microorganism demonstrated by culture or histology of a vegetation or intracardiac abscess
OR
Confirmed histology showing active endocarditis
Clinical criteria:
Two major criteria OR
One major and three minor criteria OR
Five minor criteria
Possible IE
One major and one minor criteria OR
Three minor criteria
Rejected IE
Firm alternative diagnosis OR
Resolution of manifestations with therapy for ≤4 d OR
No pathological evidence at surgery or autopsy after antibiotic therapy ≤4 d
Modified from Li JS, Sexton DJ, Mick N, et al. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin Infect Dis. 2000;30(4):633-638, by permission of Oxford University Press.
Clinical Presentation
• Clinical presentation is variable, ranging from acute sepsis, commonly seen in ABE, to an indolent low-grade febrile illness, malaise, and anorexia in SBE.
• Fever and heart murmur are the two signature features.
• Local complications include valvular destruction, perivalvular extension, and heart failure.
• Embolic phenomena to microvascular sites (splinter hemorrhage, petechiae, Janeway lesions) or large vessels can occur. Metastatic infection can cause infarcts to organs such as the brain (stroke), kidneys, spleen, and lungs.
• Immune complex-mediated manifestations (nephritis, arthralgias, Osler nodes; or false positive serology of rheumatoid factor, syphilis) are more commonly seen in SBE.
• PVE must be considered in any patient with persistent bacteremia after heart valve surgery or new valve dehiscence with secondary hemolysis.
Diagnostic Testing
• The most reliable diagnostic criterion for IE and a major Duke criterion is persistent bacteremia in a compatible clinical setting. Three blood cultures should be taken from separate sites drawn 30 minutes apart before empiric antimicrobial therapy is initiated to maximize pathogen recovery. Blood cultures are negative in 10%-15% of patients, most commonly because of prior receipt of antibiotics.
• Echocardiography plays an important role in establishing the diagnosis of IE and determining the need for surgical intervention.
• Patients with IE and vegetations seen by transthoracic echocardiography (TTE) are at higher risk of embolism, heart failure, and valvular disruption. However, a negative TTE cannot rule out IE, having a sensitivity of 50%-60%.
• Transesophageal echocardiography has higher sensitivity (90%) and should be the first test in patients with prosthetic valves or complicated IE (i.e., perivalvular abscess). In every other situation, TTE should be performed first.12
• True culture-negative IE is rare and usually caused by fastidious pathogens that do not grow in standard blood culture media. These include Coxiella burnetii (Q fever), Bartonella, Brucella, Tropheryma whipplei (Whipple disease), Legionella, and fungi. Empiric therapy can be initiated despite negative cultures. Serological or molecular testing should be performed if blood cultures are negative and there are epidemiological clues for the pathogens above.
• 18F-Auorodeoxyglucose cardiac positron emission tomography plus CT may be useful in cases of suspected PVE. Its role in native valve IE remains to be determined.
TREATMENT
• IE often requires empiric antimicrobial treatment before culture results become available. Initial treatment for S. aureus should consist of vancomycin 15 mg/kg IV q12h. Infectious diseases consultation is advised to help define an antimicrobial regimen. Therapy should then be modified based on culture and susceptibility data.
For methicillin-sensitive isolates, oxacillin 2 g IV q4h is superior to vancomycin.• In selected cases of SBE where the patient is clinically stable, therapy can usually be delayed until culture data and susceptibilities are available.
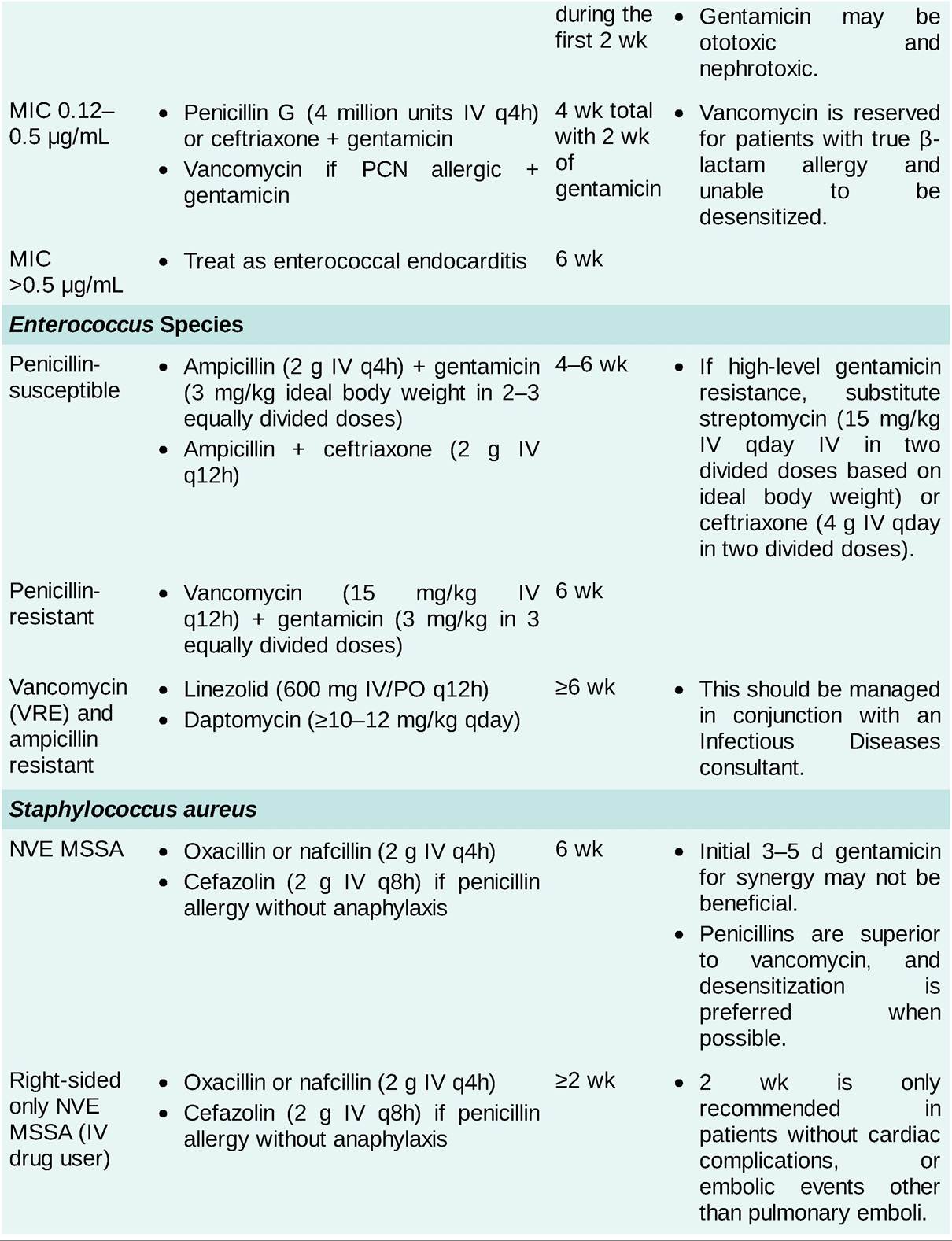
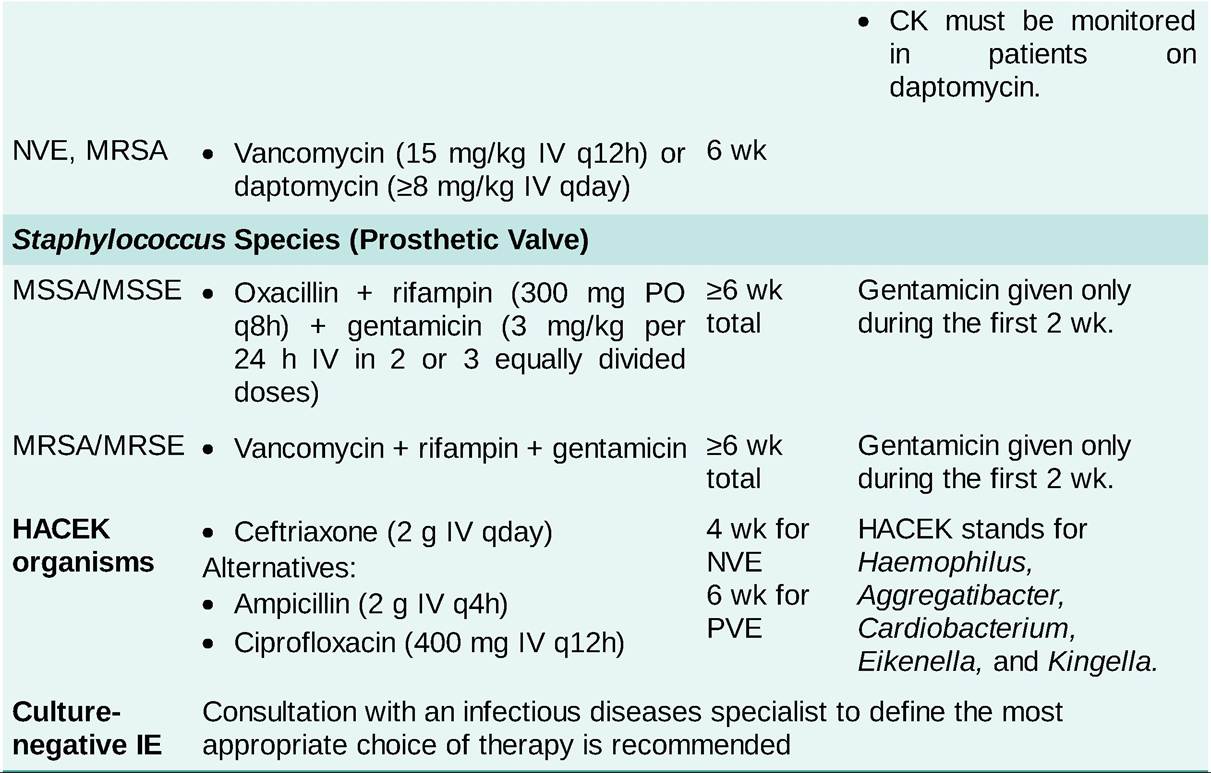
• Antibiotic therapy for specific organisms is described in Table 14-7.
TABLE 14-7
TREATMENT OF ENDOCARDITIS CAUSED BY SPECIFIC ORGANISMS12
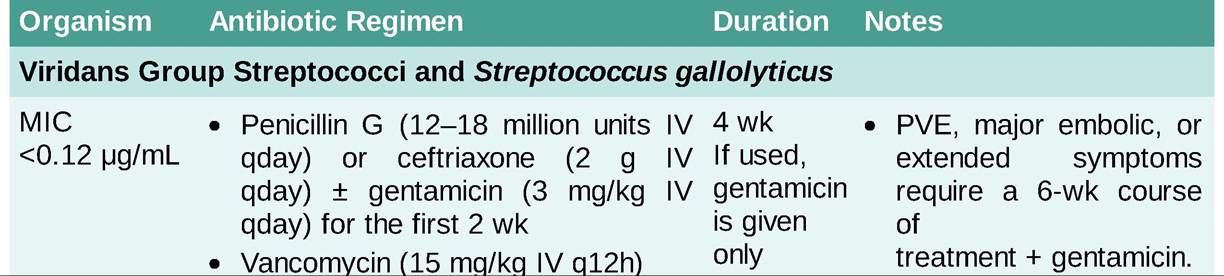
Baseline and weekly audiometry recommended for patients receiving aminoglycosides for >7 days. Monitor aminoglycoside and vancomycin levels. Goal vancomycin trough levels are 15-20 μg∕mL.
CK, creatinine kinase; IE, infective endocarditis; MIC, minimum inhibitory concentration; MRSA, methicillin-resistant Staphylococcus aureus; MRSE, methicillin-resistant Staphylococcus epidermidis; MSSA, methicillin-sensitive Staphylococcus aureus; MSSE, methicillin-sensitive Staphylococcus epidermidis; NVE, native valve endocarditis; PCN, penicillin; PVE, prosthetic valve endocarditis; VRE, vancomycin-resistant Enterococcus.
• Standard care consists of targeted IV antimicrobials for 4-6 weeks, starting from the day that source control and blood culture clearance are achieved.12
• PVE requires aggressive combination of antimicrobials for at least 6 weeks or longer and surgery because of the increased risk for treatment failure and relapse. Initial empiric therapy pending culture data include the addition of rifampin and gentamicin to improve biofilm penetration.
• Transition to oral therapy can be considered in selected patients after an initial IV course but additional trials are needed to validate this approach in other clinical settings.
• Response to antimicrobial therapy
î Clinical improvement is frequently seen within 3-10 days of initiating therapy.
î Blood cultures should be obtained daily until clearance of bacteremia has been documented.
î Persistent or recurrent fever usually represents extensive cardiac infection but also may be due to septic emboli, drug hypersensitivity, or subsequent nosocomial infection.
Surgical Management
• Indications for surgery in patients with NVIE include persistent vegetation after systemic embolization; mobile vegetations ≥10 mm; ≥1 embolic event in the first 2 weeks of treatment or increase in the size of the vegetation despite antimicrobial therapy; refractory heart failure and aortic or mitral regurgitation with ventricular failure; heart block, annular or aortic abscess, fistula, or perforation; infection with fungi or other highly resistant organisms; and persistent bacteremia or fever lasting >5-7 days, provided that other sites of infection and fever have been excluded.
• For PVE, besides the indications listed above, valve dehiscence, intracardiac fistula, severe prosthetic valve dysfunction resulting in heart failure, and relapsing PVE also warrant surgery.12
SPECIAL CONSIDERATIONS
American Heart Association recommendations for prophylaxis for IE are outlined in Table 14-8.
TABLE 14-8
ENDOCARDITIS PROPHYLAXIS13
I. Endocarditis prophylaxis is recommended for the following cardiac conditions: prosthetic valves; previous endocarditis; unrepaired cyanotic congenital heart disease or repaired congenital heart disease with prosthetic material during the first 6 mo after procedure, or with residual defects at or adjacent to the site of the prosthetic device; and cardiac valvulopathy in transplant recipients.
II. Regimens for dental, oral, or respiratory tract procedures (including dental extractions, periodontal or endodontic procedures, professional teeth cleaning, bronchoscopy with biopsy, rigid bronchoscopy, surgery on respiratory mucosa, and tonsillectomy):
| Standard prophylaxis | Amoxicillin 2 g PO 1 h before procedure |
| Unable to take PO | Ampicillin 2 g IM or IV, or cefazolin or ceftriaxone 1 g IM or IV within 30 min before procedure |
| Penicillin-allergic patient | Clindamycin 600 mg PO, or cephalexin 2 g PO, or clarithromycin or azithromycin 500 mg PO 1 h before procedure |
| Penicillin allergic and unable to take PO | Clindamycin 600 mg IV, or cefazolin or ceftriaxone 1 g IV within 30 min before procedure |
III. Gastrointestinal and genitourinary procedures do not require routine use of prophylaxis. High-risk patients infected or colonized with enterococci should receive amoxicillin, ampicillin, or vancomycin to eradicate the organism before urinary tract manipulation.
IV. Prophylaxis is recommended for procedures on infected skin, skin structures, or musculoskeletal tissue ONLY for patients with cardiac conditions outlined above. An antistaphylococcal penicillin or cephalosporin should be used.