Chronic Lymphocytic Leukemia
Epidemiology and Etiology
Chronic lymphocytic leukemia (CLL) is the most common leukemia in the US, with an estimated 21,040 new cases in 2020 and a median age at diagnosis of 72 years.1
Pathology
CLL is typically positive for the B cell antigens CD19, CD20 (dim), and CD23, as well as aberrant expression of the T cell antigen, CD5.
CLL is typically negative for cyclin D1 and CD10.Staging
The traditional classification of CLL is based on the Rai and Binet staging systems (Table 22-8). Molecular and cytogenetic markers have become increasingly useful for prognostication, including high- risk markers: del(17p) or TP53, del(11q) or unmutated IGHV; and the low-risk markers: del(13q), trisomy 12 or mutated IGHV.37
TABLE 22-8
CHRONIC LYMPHOCYTIC LEUKEMIA CLINICAL STAGING
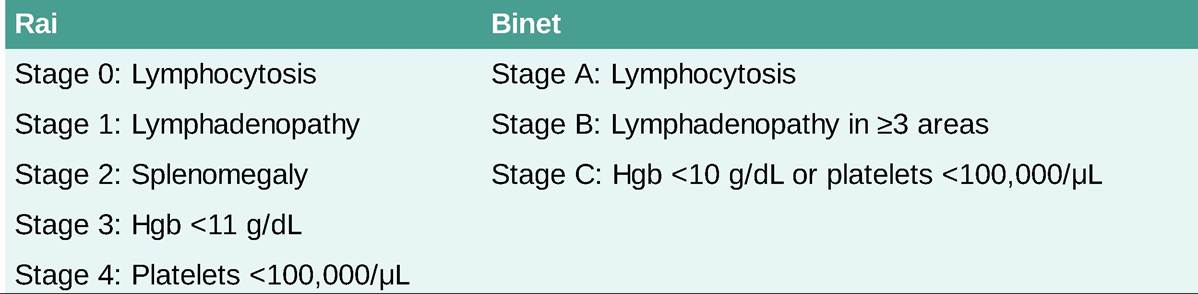
Hgb, hemoglobin.
Clinical Presentation
Most patients are diagnosed while asymptomatic, often presenting with lymphocytosis on routine laboratory evaluation. When present, symptoms may include fatigue, weight loss, lymphadenopathy, symptoms of anemia or thrombocytopenia, and infections. Patients may also present with an autoimmune hemolytic anemia, immune thrombocytopenia, or Richter transformation of CLL to a more aggressive diffuse large B cell lymphoma.
Diagnostic Testing
The diagnosis of CLL requires a peripheral blood absolute lymphocyte count of gt;5 ? 109#8725;L and characteristic cell surface markers on peripheral blood flow cytometry. Patients should also have peripheral blood FISH for prognostic markers.
TREATMENT
Many patients do not require treatment at the time of initial diagnosis. The indication for treatment is based on the presence of active disease, defined by the International Workshop on CLL by at least one of the following: progressive marrow failure, massive or symptomatic splenomegaly (gt;6 cm below costal margin), lymphadenopathy (gt;10 cm in longest diameter), progressive lymphocytosis (gt;50% increase in 2 months or doubling time of lt;6 months), autoimmune hemolytic anemia or thrombocytopenia that is poorly responsive to standard therapy, and/or the presence of constitutional symptoms.37 Chemotherapeutic options traditionally include alkylating agents (chlorambucil, cyclophosphamide, bendamustine), purine analogues (fludarabine), and anti-CD20 monoclonal antibodies such as rituximab, ofatumumab, or obinutuzumab. Oral targeted agents have shown significant efficacy in CLL and are particularly effective in patients with high-risk cytogenetics, such as 17p and 11q deletions, leading to a significant shift from chemotherapy-based regimens to molecularly targeted agents in the treatment of CLL, including ibrutinib or acalibrutinib (BTK inhibitors), idelalisib (PI3K inhibitor), and venetoclax.37