Cystitis
• Uncomplicated cystitis is defined as infection of the bladder or lower urinary tract in otherwise healthy, nonpregnant women.
• Complicated cystitis is defined as infection in patients with anatomic abnormalities, obstruction, immunosuppression, pregnancy, indwelling catheters, or unusual pathogens.
• Recurrent cystitis can occur in women, either due to reinfection or recurrence.31
DIAGNOSIS
Clinical Presentation
• Lower UTI is diagnosed based on history of dysuria, urgency, frequency, or suprapubic pain associated with pyuria and bacteriuria on urinalysis and urine culture. Fever is more likely if there is pyelonephritis.
• Dysuria without pyuria in sexually active patients warrants consideration of sexually transmitted infection (see Chapter 16, Sexually Transmitted Infections, Human Immunodeficiency Virus, and Acquired Immunodeficiency Syndrome).
Diagnostic Testing
• Acute uncomplicated cystitis in women. Many women are treated empirically without a urine culture. A pretreatment urine culture is recommended for patients at risk for antimicrobial resistance, or for patients at risk for more serious infection such as those with underlying urological abnormalities or immunosuppression.
• Sterile pyuria. Prior antimicrobials may result in negative urine cultures. Differential diagnosis includes chronic interstitial nephritis, interstitial cystitis, or infection with atypical organisms including Chlamydia trachomatis, Ureaplasma urealyticum, N. gonorrhoeae, or rarely, M. tuberculosis. Specific cultures of the endocervix for sexually transmitted infections should be performed.
TREATMENT
• See Tables 14-11 and 14-12.
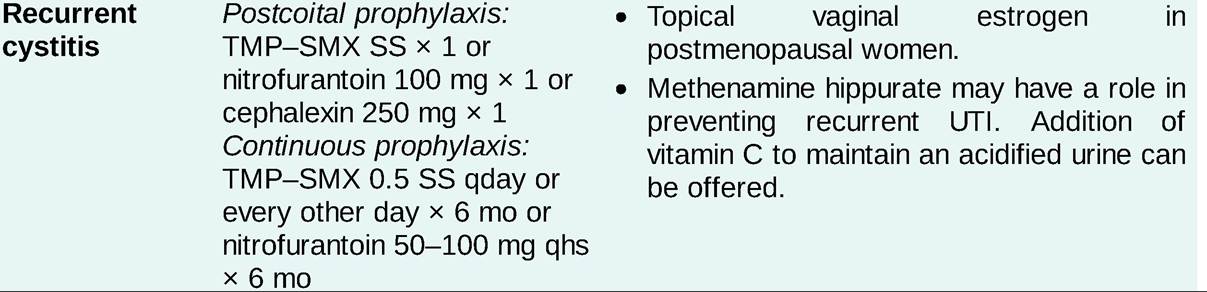
TABLE 14-11
EMPIRIC THERAPY FOR URINARY TRACT INFECTIONS31
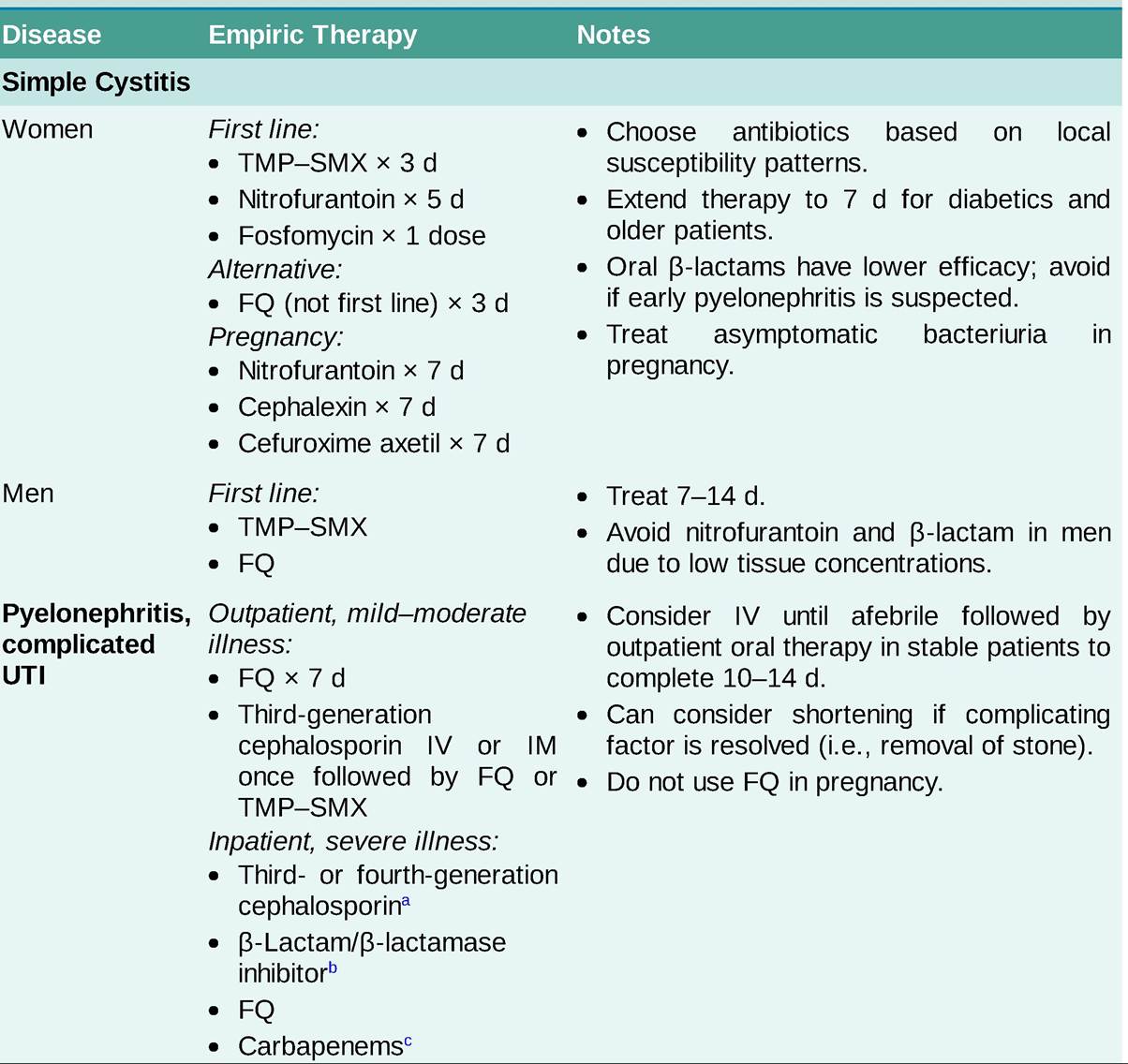
DS, double strength; FQ, fluoroquinolone; GU, genitourinary; SS, single strength; TMP, trimethoprim; TMP-SMX, trimethoprimsulfamethoxazole; UTI, urinary tract infection.
aThird- or fourth-generation cephalosporins include ceftriaxone 1-2 g IV qday (third-generation) or cefepime 1 g IV q8h (fourthgeneration).
bβ-Lactam∕β-lactamase inhibitors: PiperacillinZtazobactam 3.75-4.5 g IV q6h.
cCarbapenems: Meropenem 1 g IV q8h.
TABLE 14-12
DOSING EXAMPLES FOR URINARY TRACT INFECTIONS
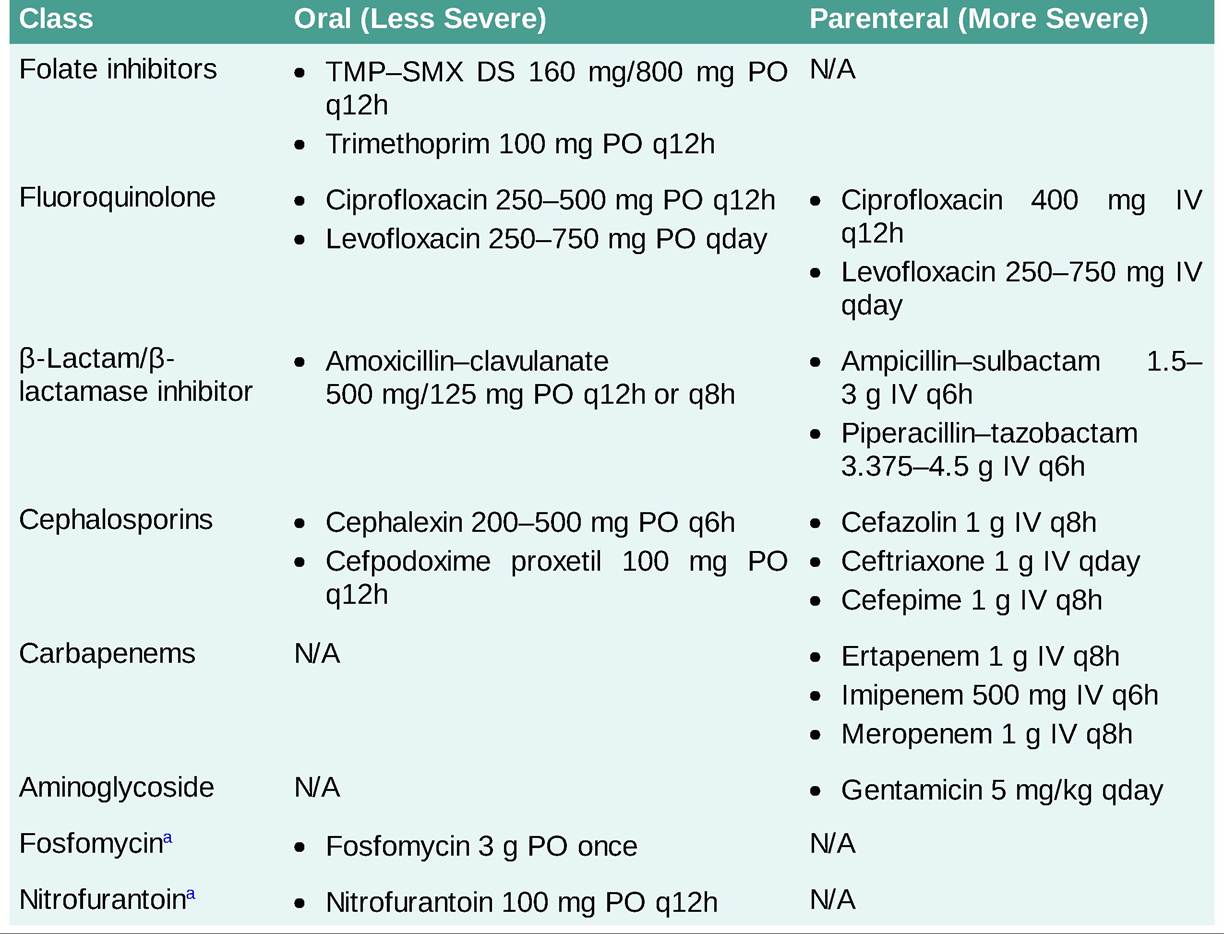
DS, double strength; N/A, not applicable; TMP-SMX, trimethoprim-sulfamethoxazole. aUncomplicated cystitis.
• Posttreatment urine culture is unnecessary unless symptoms do not improve within 48 hours. Foreign bodies including stents and catheters should ideally be removed if feasible.
• Recurrent cystitis in women is usually due to reinfection (with a different organism). Risk factors include frequency of intercourse and spermicide use in young women and urologic abnormalities such as incontinence and cystocele in older women. Relapses (with the original infecting organism) that occur within 2 weeks of cessation of therapy should be treated similar to the original episode of cystitis.
• Prophylaxis may be considered for patients with frequent reinfection using continuous or postcoital antibiotics. Estrogen therapy in postmenopausal women may also have a role in prevention; cranberry products have not been shown to help.