Disease-Modifying Antirheumatic Drugs
Immunomodulatory and immunosuppressive drugs, also known as disease-modifying antirheumatic drugs (DMARDs), include a number of pharmacologically diverse agents that exert anti-inflammatory or immunosuppressive effects.
They are characterized by a delayed onset of action and the potential for serious toxicity. Consequently, they should be prescribed with the guidance of a rheumatologist and in cooperative patients who are willing to comply with meticulous follow-up.Classification of DMARDs
• DMARDs are classified as synthetic and biologic DMARDs. Synthetic DMARDs are subclassified as conventional synthetic DMARDs (csDMARD) and targeted synthetic DMARDs (tsDMARDs). The latter category corresponds to small molecules targeting intracellular transduction pathways (Table 255). Biologic DMARDs are a novel class of medications that has revolutionized the treatment of rheumatologic conditions (Table 25-10). These selectively block important pathways in immunity that interfere with cytokine function, signal transduction or production, T cell costimulation, or B cell depletion.
TABLE 25-10
NOMENCLATURE
| Drug Suffix | Nomenclature |
| Mab | Monoclonal Ab |
| Cept | Soluble receptor |
| Xi | Chimeric |
| Zu | Humanized |
| U | Human |
| Pegol | Pegylated—decreased immunogenicity |
• Shared side effects:
î Inj ection site/infusion reaction
î Increased risk of infections (including reactivation of hepatitis B, hepatitis C, tuberculosis)
î Increased risk of malignancy
• Screen all the patients for hepatitis B, hepatitis C, and tuberculosis before starting a biologic DMARD. Ideally, all patients should be up to date with vaccinations prior to initiation.
With the exception of rituximab, biologic DMARDs should be avoided in patients with active malignancy (Table 25-11).TABLE 25-11
BIOLOGIC DMARDS
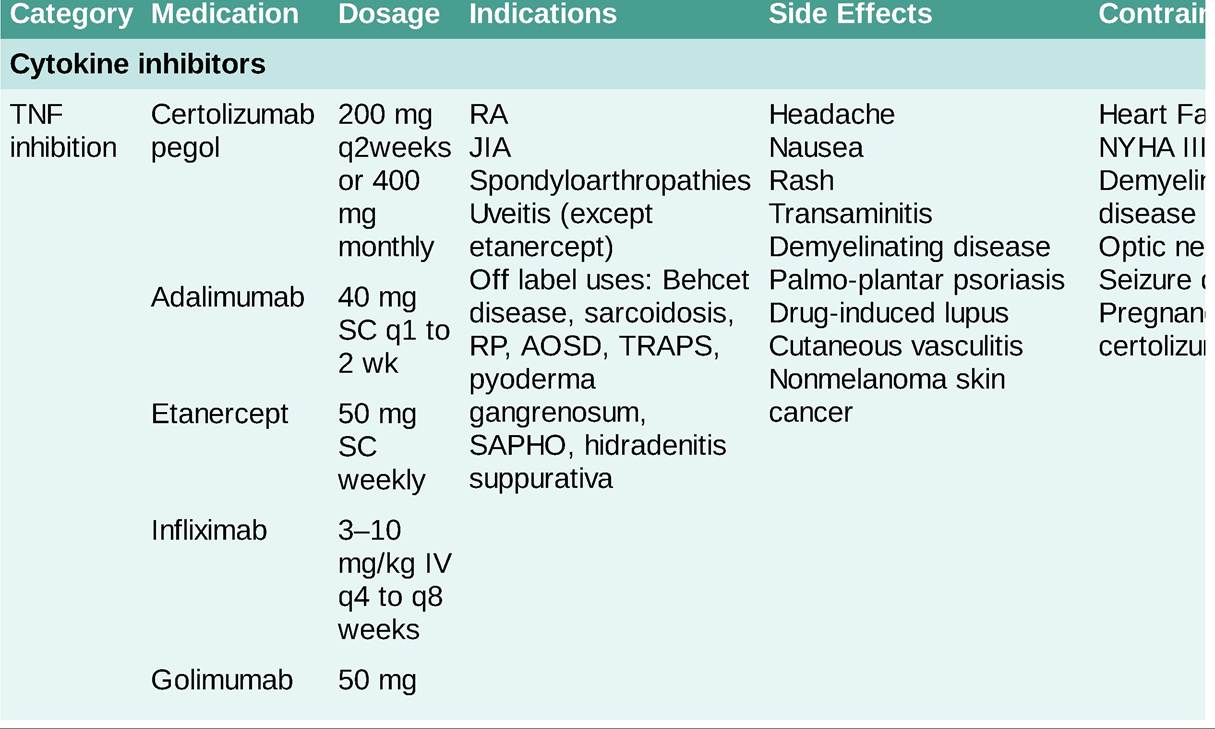
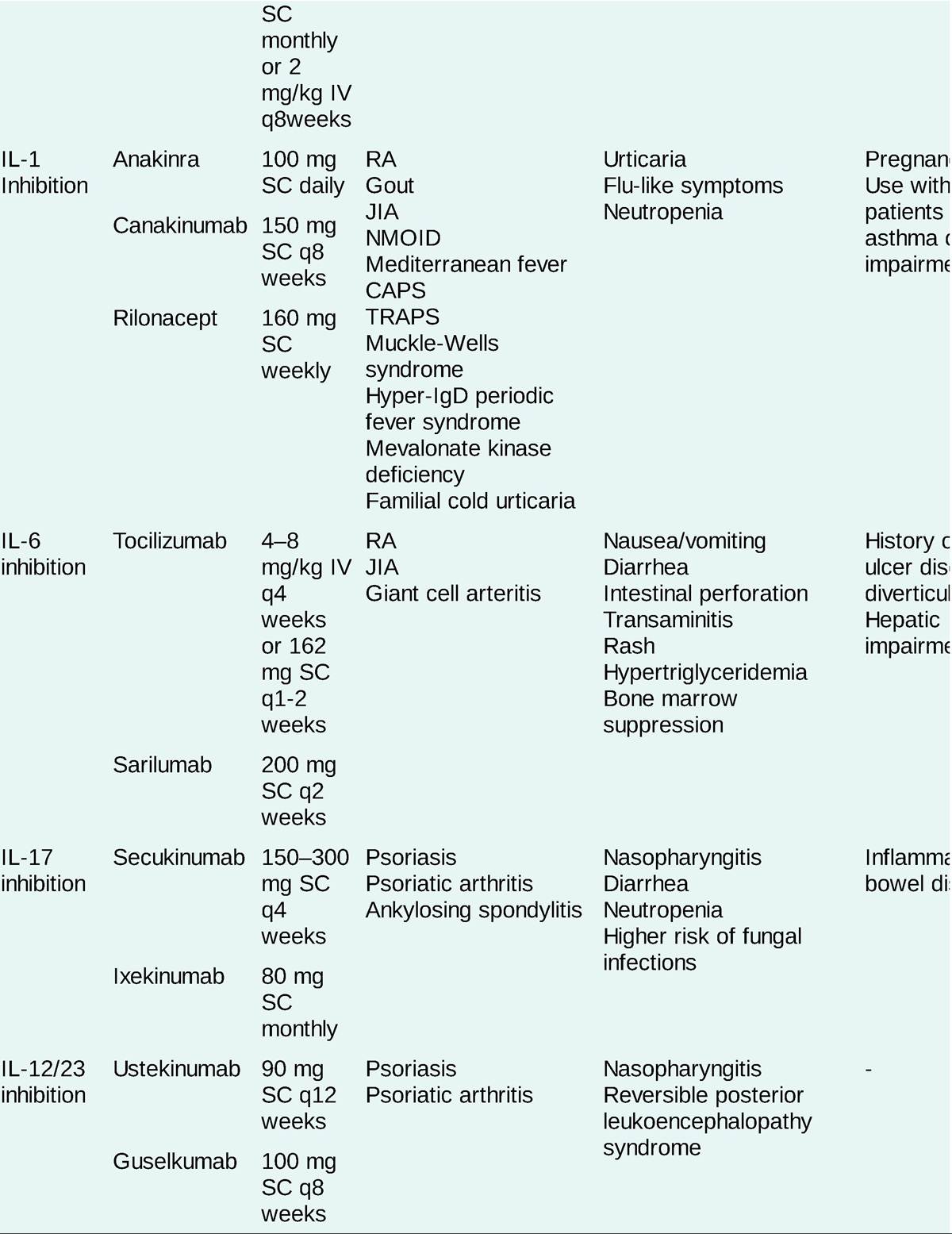
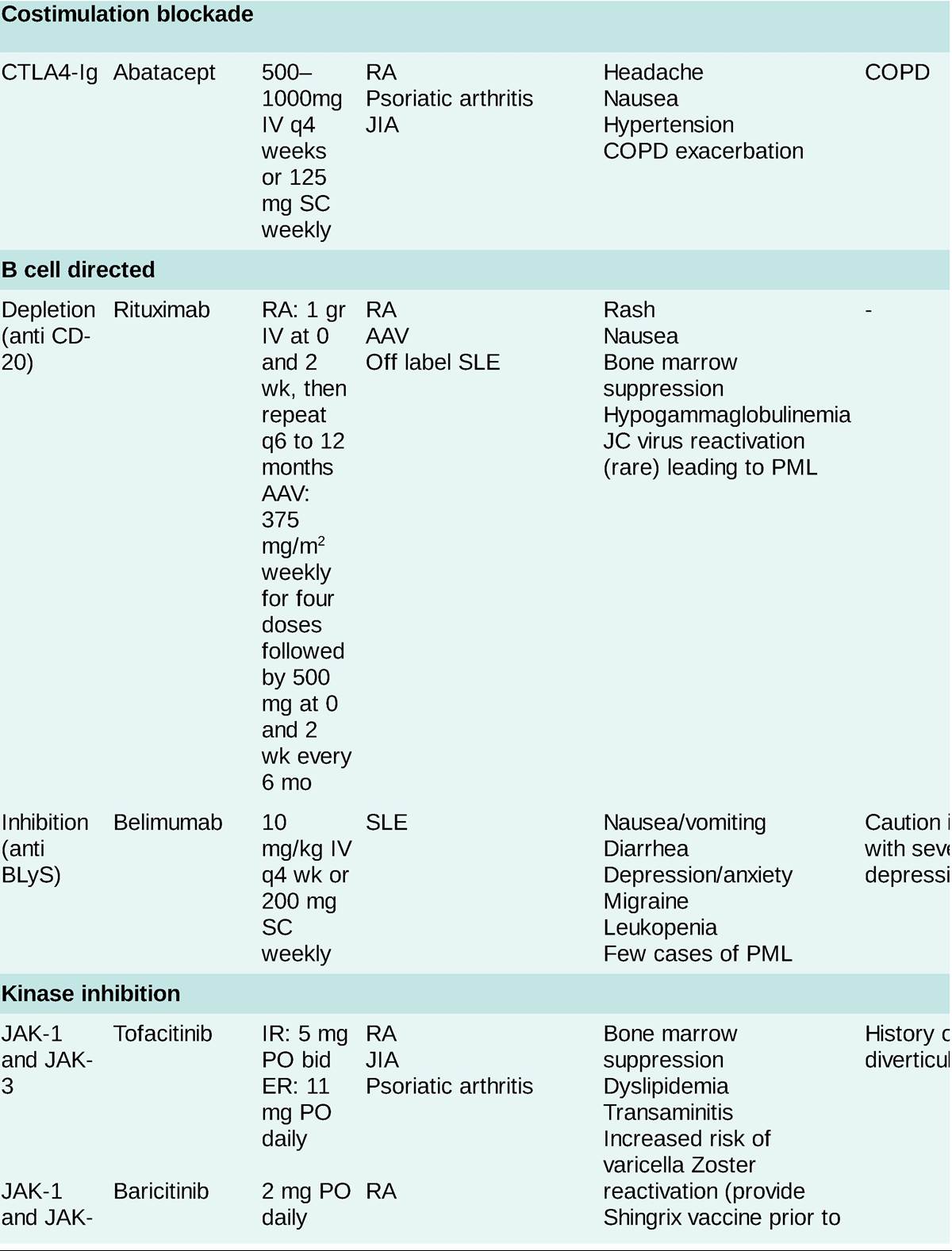
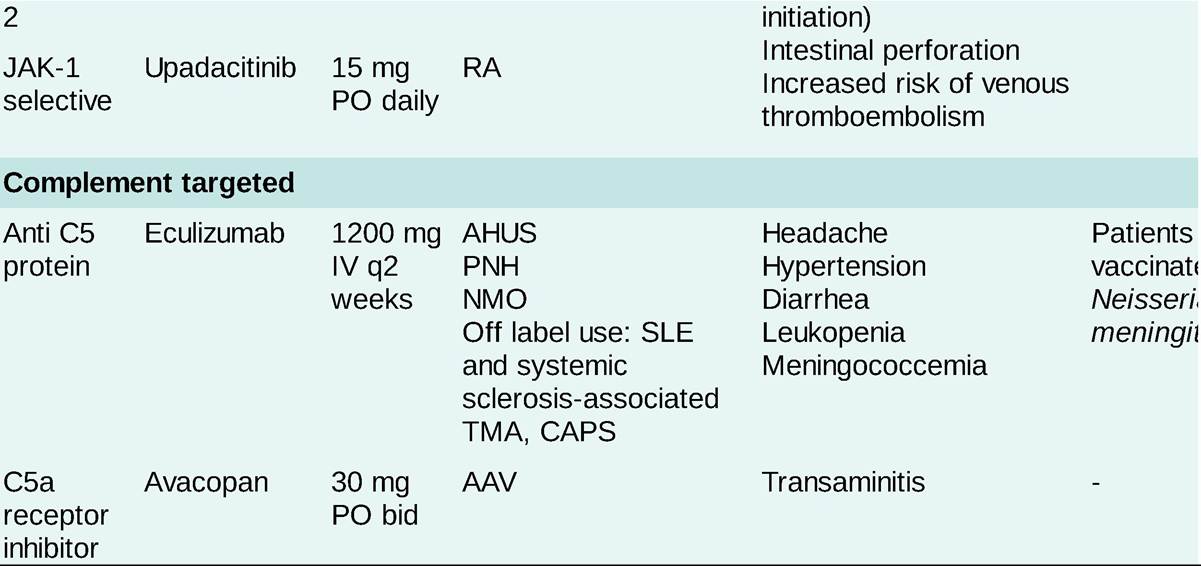
AAV, ANCA-associated vasculitis; AHUS, atypical hemolytic uremic syndrome; AOSD, adult-onset Still disease; COPD, chronic obstructive pulmonary disease; CAPS, catastrophic antiphospholipid syndrome; CAPS, cryopyrin-associated periodic syndromes; DM, dermatomyositis; ER, extended release; IR, immediate release; JIA, juvenile idiopathic arthritis; NMO, neuromyelitis optica; NMOID, neonatal-onset multisystem inflammatory disease; PML, progressive multifocal leukoencephalopathy; PNH, paroxysmal nocturnal hemoglobinuria; RA, rheumatoid arthritis; RP, relapsing polychondritis; SLE, systemic lupus erythematosus; TMA, thrombotic microangiopathy; TRAPS, TNF receptor-associated fever syndrome.
• Combinations of DMARDs can be used if the patient has a partial response to the initial agent. Methotrexate and leflunomide may have additive hepatotoxicity, and this combination should be used cautiously. Combination therapy with two biologic DMARDs is contraindicated because of increased infectious complications.