Eosinophilia
GENERAL PRINCIPLES
• Eosinophils are granulocytes that developed from bone marrow pluripotent progenitor cells.
• Eosinophil maturation is promoted by interleukins (IL-5, IL-3), and granulocyte-macrophage colonystimulating factor.
• Eosinophils are normally seen in peripheral tissue such as mucosal tissues in the gastrointestinal and respiratory tracts. They are recruited to sites of inflammation.
• Eosinophils can be involved in a variety of infectious, allergic, neoplastic, and idiopathic diseases.
Definition
• A value >500 eosinophils∕μL is defined as having eosinophilia.
• The extent of eosinophilia can be categorized as mild (500-1500 cells∕μL), moderate (1500-5000 cells∕μL), or severe (>5000 cells∕μL).
• The degree of eosinophilia is not a reliable predictor of eosinophil-mediated organ damage.
Classification
• Peripheral eosinophilia can be divided into primary, secondary, or idiopathic.
• Primary eosinophilia is seen with hematologic disorders where there may be a clonal expansion of eosinophils (chronic eosinophilic leukemia) or a clonal expansion of cells that stimulate eosinophil production (chronic myeloid or lymphocytic disorders).
• Secondary eosinophilia is also called reactive eosinophilia. It is a polyclonal expansion of eosinophils due to overproduction of IL-5. There are numerous causes such as parasites, allergic diseases, autoimmune disorders, toxins, medications, and endocrine disorders such as Addison disease.
• Idiopathic eosinophilia is considered when primary and secondary causes are excluded.
Hypereosinophilic syndrome
A proliferative disorder of eosinophils characterized by sustained eosinophilia >1500 cells∕μL for ≥1 month documented on two occasions with eosinophil-mediated damage to organs such as the heart, gastrointestinal tract, kidneys, brain, and lung.
All other causes of eosinophilia should be excluded to make the diagnosis.10• Hypereosinophilic syndrome (HES) occurs predominantly in men between the ages of 20 and 50 years and presents with insidious onset of fatigue, cough, and dyspnea.
• Approximately 10%-15% HES patients have myeloproliferative disorders. Myeloproliferative variants of HES are characterized by constitutive expression of FIP1L1/PDGFRA fusion protein and elevated serum vitamin B12 levels.
• Lymphocytic-variant HES (L-HES) accounts for 17%-26% HES patients. Unusual IL-5-producing T cells are found in L-HES.
• Cardiac disease is a major cause of morbidity and mortality in patients with HES. At presentation, patients typically are in the late thrombotic and fibrotic stages of eosinophil-mediated cardiac damage with signs of a restrictive cardiomyopathy and mitral regurgitation. An echocardiogram may detect intracardiac thrombi, endomyocardial fibrosis, or thickening of the posterior mitral valve leaflet. Neurologic manifestations range from peripheral neuropathy to stroke or encephalopathy. Bone marrow examination reveals increased eosinophil precursors.
• Acute eosinophilic leukemia is a rare myeloproliferative disorder that is distinguished from HES by several factors: an increased number of immature eosinophils in the blood and/or marrow, >10% blast forms in the marrow, and symptoms and signs compatible with an acute leukemia. Treatment is similar to other leukemias.
• Lymphoma. Eosinophilia can present in any T- or B-cell lymphoma. As many as 5% of patients with non-Hodgkin lymphoma and up to 15% of patients with Hodgkin lymphoma have modest peripheral blood eosinophilia. Eosinophilia in Hodgkin lymphoma has been correlated with IL-5 messenger RNA expression by Reed-Sternberg cells.
• Atheroembolic disease. Cholesterol embolization can lead to eosinophilia, eosinophiluria, renal dysfunction, livedo reticularis, purple toes, and increased erythrocyte sedimentation rate (ESR).
• Immunodeficiency. Hyper-IgE syndrome, autoimmune lymphoproliferative syndrome, and Omenn syndrome can present with recurrent infections, dermatitis, and eosinophilia.
Epidemiology
In industrialized nations, peripheral blood eosinophilia is most often due to atopic disease, whereas helminthic infections are the most common cause of eosinophilia in the rest of the world.
DIAGNOSIS
There are two approaches that are useful for evaluating eosinophilia, either by associated clinical context (Table 11-3) or by degree of eosinophilia (Table 11-4).
TABLE 11-3
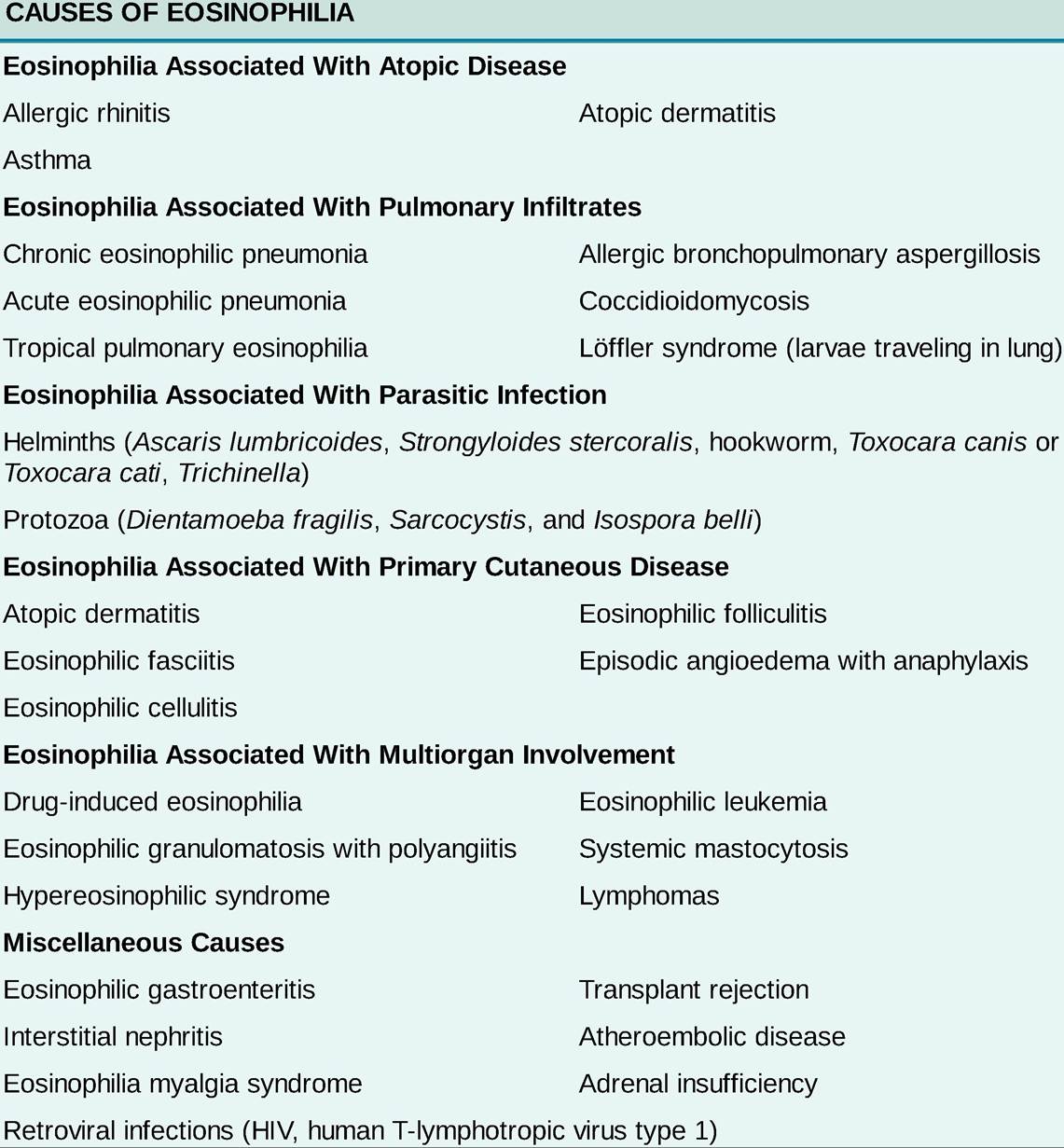
TABLE 11-4
CLASSIFICATION OF EOSINOPHILIA BASED ON THE PERIPHERAL BLOOD
EOSINOPHIL COUNT
Peripheral Blood Eosinophil Count (cells∕μL)
| 500-2000 | 2000-5000 | >5000 |
| Allergic rhinitis | Intrinsic asthma | Eosinophilia myalgia syndrome |
| Allergic asthma | Allergic bronchopulmonary aspergillosis | Hypereosinophilic syndrome |
| Food allergy | Helminthiasis | Episodic angioedema with eosinophilia |
| Urticaria | Drug reactions | EGPA |
| Addison disease | Vascular neoplasms | Leukemia |
| Pulmonary infiltrates with eosinophilia syndromes | Eosinophilic granulomatosis with polyangiitis (EGPA) | |
| Solid neoplasms | Eosinophilic fasciitis | |
| Nasal polyposis | HIV |
Clinical Presentation
HISTORY
• A history is important in narrowing the differential diagnosis of eosinophilia. It is important to determine if the patient has symptoms of atopic disease (rhinitis, wheezing, rash) or cancer (weight loss, fatigue, fever, night sweats) and to evaluate for other specific organ involvement such as lung, heart, or nerves.
Prior eosinophil count can help determine the duration and magnitude of eosinophilia.• A complete medication list, including over-the-counter supplements, and a full travel, occupational, and dietary history should be obtained.
• Any pet contact should be ascertained for possible exposure to toxocariasis.
PHYSICAL EXAMINATION
Physical examination should be guided by the history, with a special focus on the skin, upper and lower respiratory tracts, and cardiovascular and neurologic systems.
LABORATORIES
• Initial laboratory evaluations generally include complete blood count (CBC) with differential and eosinophil count, liver function tests, serum chemistries and creatinine, serum vitamin B12 level, troponin, markers of inflammation (e.g., ESR and/or C-reactive protein [CRP]), and urinalysis. Further diagnostic studies are based on clinical presentations and initial findings. Mild eosinophilia associated with symptoms of rhinitis or asthma is indicative of underlying atopic disease, which can be confirmed by skin testing.
• Depending on the travel history, stool examination for ova and parasites should be done on three separate occasions. Because only small numbers of helminths may pass in the stool and because tissue- or blood-dwelling helminths will not be found in the stool, serologic tests for antiparasite antibodies should also be sent. Such tests are available for strongyloidiasis, toxocariasis, and trichinellosis.
• Diagnosis at the time of presentation with Loffler syndrome can be made by detection of Ascaris larvae in respiratory secretions or gastric aspirates but not stool.
• Peripheral blood smear and flow cytometry of lymphocyte subpopulations can aid in the diagnosis of hematologic malignancy. Bone marrow biopsy for pathologic, cytogenetic, and molecular testing on bone marrow and/or peripheral blood (e.g., for FIP1L1/PDGFRA mutation) may be required. Serum vitamin B12 level may be elevated in myeloproliferative neoplasms and autoimmune lymphoproliferative syndrome.
• Evaluation for idiopathic HES should also consist of troponin measurement, echocardiogram, and ECG.
• Immunoglobulin levels are helpful if concerned for an immunodeficiency. Elevated immunoglobulin levels can be found in L-HES.
• A tryptase level is necessary if mastocytosis is considered as a cause of eosinophilia.
IMAGING
CXR or CT findings may also help to narrow the differential diagnosis.
• Peripheral infiltrates with central clearing are indicative of chronic eosinophilic pneumonia.
• Diffuse infiltrates in an interstitial, alveolar, or mixed pattern may be seen in acute eosinophilic pneumonia as well as drug-induced eosinophilia with pulmonary involvement.
• Transient infiltrates may be seen in Loffler syndrome, EGPA, or allergic bronchopulmonary aspergillosis (ABPA).
• Central bronchiectasis is a major criterion in the diagnosis of ABPA.
• A diffuse miliary or nodular pattern, consolidation, or cavitation may be found in cases of tropical pulmonary eosinophilia.
• A CT of the sinuses, nerve conduction studies, and testing for p-ANCA may be helpful in the diagnosis of eosinophilic granulomatosis with polyangiitis (EGPA).
DIAGNOSTIC PROCEDURES
• If no other cause of pulmonary infiltrates has been identified, a bronchoscopy may be necessary for analysis of bronchoalveolar lavage (BAL) fluid and lung tissue. The presence of eosinophils in BAL fluid or sputum with eosinophilic infiltration of the parenchyma is most typical of acute or chronic eosinophilic pneumonia.
• Skin biopsy will aid in diagnosing the cutaneous eosinophilic diseases and EGPA.
TREATMENT
• Mild eosinophilia with no evidence of end-organ damage may not need treatment.
• Oral steroids are indicated when there is evidence of organ involvement. However, strongyloidiasis must be excluded before administration of steroids to prevent hyperinfection syndrome.
• When a drug reaction is suspected, discontinuation of the drug is both diagnostic and therapeutic.
Other treatment options depend on the exact cause of eosinophilia because, with the exception of HES, eosinophilia is a manifestation of an underlying disease.• HES: Patients with marked eosinophilia with no organ involvement may have a benign course. In contrast, those with organ involvement and FIP1L1∕PDGFRA-associated disease may have an extremely aggressive course without treatment.
o Monitoring and early initiation of high-dose glucocorticoids should be pursued in all patients except those who have the FIP1L1/PDGFRA fusion gene.
î Patients with the FIP1L1/PDGFRA fusion mutation should be started on imatinib mesylate (Gleevec), a tyrosine kinase inhibitor. Treatment should be initiated promptly in these patients to prevent progression of cardiac disease and other end-organ damage. Imatinib has been shown to induce disease remission and halt progression.11
î Hydroxyurea has been the most frequently used effective second-line agent and/or steroid-sparing agent for HES. Interferon-α2b in combination with glucocorticoids has been used to treat L-HES. Hematopoietic cell transplantation may be considered in refractory HES.
î Mepolizumab, a humanized anti-IL-5 antibody, has shown corticosteroid-sparing effects in FIP1L1∕PDGFRA-negative, corticosteroid-responsive subjects with HES.12
î Alemtuzumab, an anti-CD52 antibody (CD52 is expressed on the surface of eosinophils), has been shown to be effective in treatment for patients with refractory idiopathic HES.13
• Primary eosinophilia disorders should be followed by a specialist; any cases of unresolved or unexplained eosinophilia warrant evaluation by an allergist/immunologist.