Evaluation of Thyroid Function1
GENERAL PRINCIPLES
The major hormone secreted by the thyroid is thyroxine (T4), which is converted by deiodinases in many tissues to the more potent triiodothyronine (T3).
Both are bound reversibly to plasma proteins, primarily thyroxine-binding globulin. Only the free (unbound) fraction enters cells and produces biologic effects. T4 secretion is stimulated by thyroid-stimulating hormone (TSH) from the pituitary gland. In turn, TSH secretion is inhibited by T4, forming a negative feedback loop that keeps free T4 levels within a narrow normal range. Diagnosis of thyroid disease is based on clinical findings, palpation of the thyroid, and measurement of plasma TSH and thyroid hormones.DIAGNOSIS
Clinical Presentation
Thyroid palpation determines the size and consistency of the thyroid and the presence of nodules, tenderness, or a thrill.
Diagnostic Testing
• Plasma TSH is the best initial test in most patients with suspected thyroid disease. TSH levels are elevated in very mild primary hypothyroidism and are suppressed in very mild hyperthyroidism. Thus, a normal plasma TSH level excludes nearly all causes of hyperthyroidism, as well as primary hypothyroidism. Because even slight changes in thyroid hormone levels affect TSH secretion, abnormal TSH levels are not specific for clinically important thyroid disease. Changes in plasma TSH lag behind changes in plasma T4, and TSH levels may be misleading when plasma T4 levels are changing rapidly, as during treatment of hyperthyroidism.
î TSH levels may be suppressed in severe nonthyroidal illness, in mild (or subclinical) hyperthyroidism, and during treatment with dopamine or high doses of glucocorticoids. In addition, TSH levels remain suppressed for 6-8 weeks after hyperthyroidism is corrected.
î Plasma TSH is mildly elevated (up to 20 #956;U#8725;mL) in some euthyroid patients recovering from nonthyroidal illnesses and in mild (or subclinical) hypothyroidism.
î TSH levels are usually within the reference range in secondary hypothyroidism and thus cannot be used to diagnose this rare form of hypothyroidism.
• Plasma-free T4 confirms the diagnosis and assesses the severity of hyperthyroidism when plasma TSH is low. It is also used to diagnose secondary hypothyroidism and adjust thyroxine therapy in patients
with pituitary disease. Most laboratories measure free T4 by immunoassay.
• Free T4 measured by equilibrium dialysis is the most reliable measure of unbound T4, but results are seldom rapidly available. It is needed only in rare cases in which the diagnosis is not clear from measurement of plasma TSH and free T4 by immunoassay.
• Effect of nonthyroidal illness on thyroid function tests: Many illnesses alter thyroid tests without causing true thyroid dysfunction (the nonthyroidal illness or euthyroid sick syndrome). These changes must be recognized to avoid mistaken diagnosis.
î Low T3 occurs in many illnesses, during starvation, and after trauma or surgery. Conversion of T4 to T3 is decreased, and plasma T3 levels are low. Plasma-free T4 and TSH levels are normal. This may be an adaptive response to illness, and thyroid hormone therapy is not beneficial.
î Low T4 occurs in severe illness. TSH levels decrease early in severe illness, sometimes to lt;0.1 #956;U#8725;mL. In prolonged illness, free T4 may also fall below normal. During recovery, TSH rises, sometimes to levels slightly above the normal range (rarely gt;20 #956;U#8725;mL).
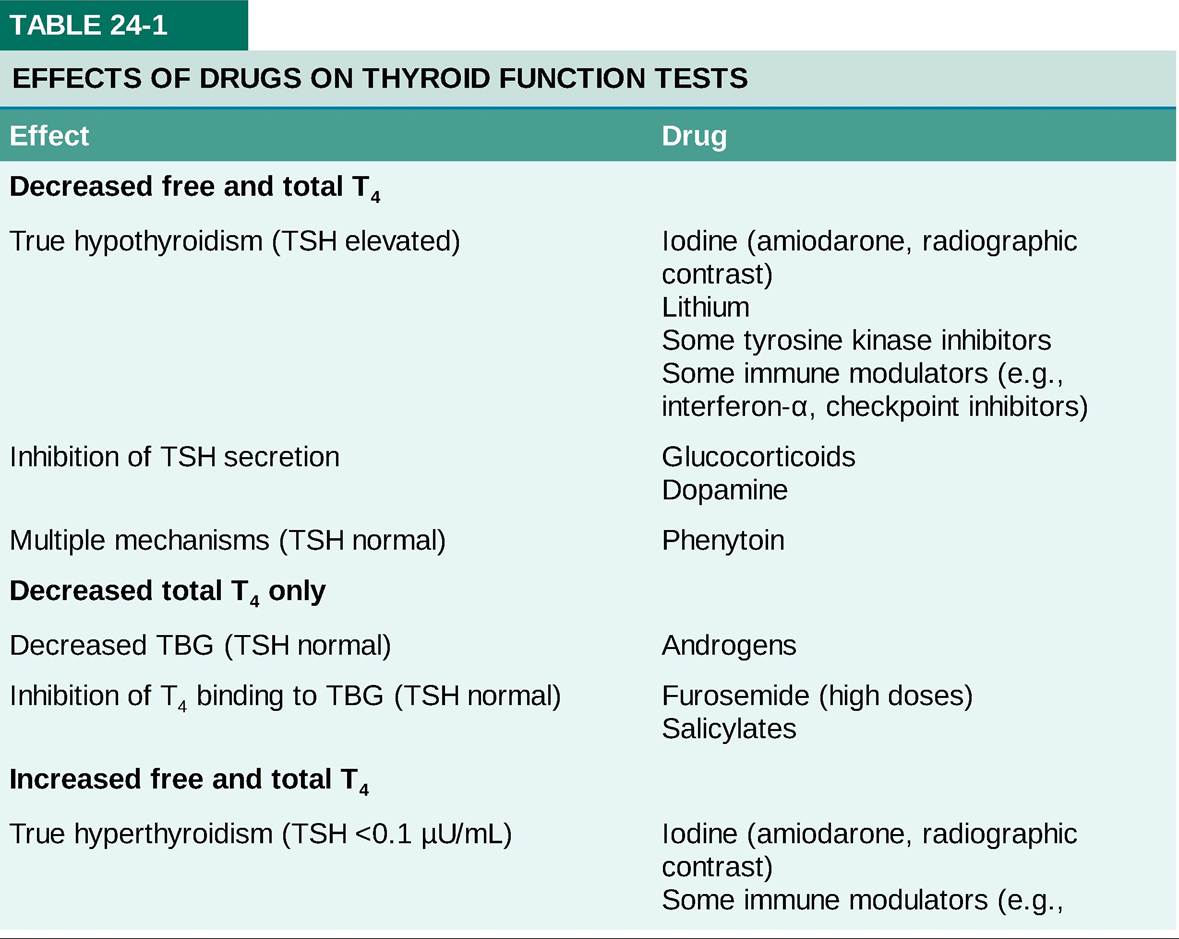
î Some drugs affect thyroid function tests (see Table 24-1). Iodine-containing drugs (amiodarone and radiographic contrast media) and immune modulators may cause hyperthyroidism or hypothyroidism in susceptible patients. In general, plasma TSH levels are a reliable guide to whether true hyperthyroidism or hypothyroidism is present.
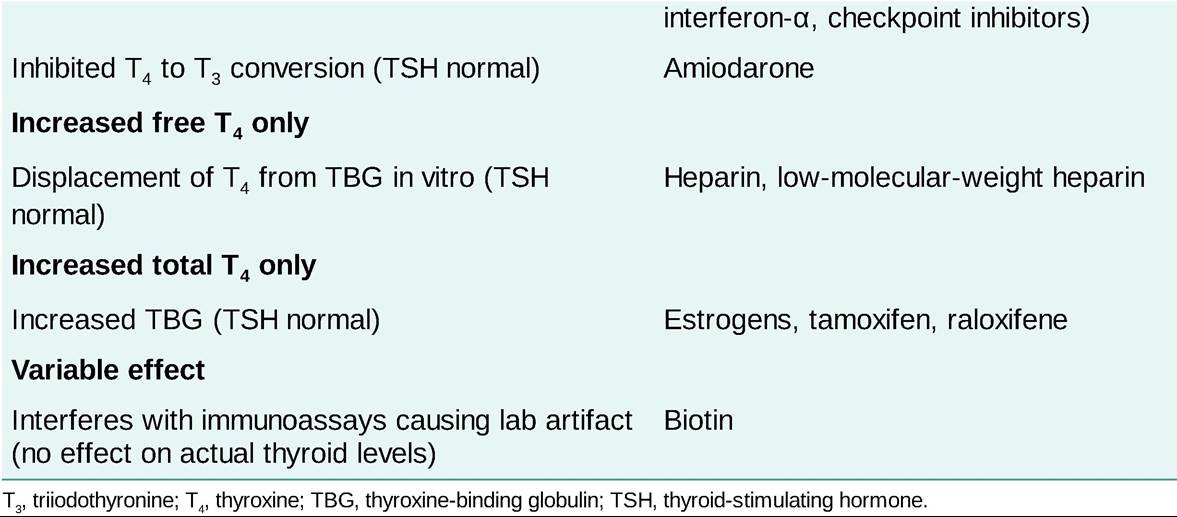
î Biotin, commonly taken as an over-the-counter supplement, can interfere with immunoassays for TSH, free T4, and/or free T3 at high concentrations. It has a short half-life and should be held for 12 days before laboratory testing.