General Principles
BACKGROUND
Cancer is one of the leading causes of mortality both worldwide and in the US, accounting for approximately 608,000 deaths in the US in 2020.1 The most common malignancies in the US are lung cancer, prostate cancer, breast cancer, and colon cancer (Table 22-1).
Cancer death rates have declined by an estimated 29% over the past 3 decades owing to better uptake of screening strategies, advances in drug development, and the availability of better supportive care. Improved understanding of the molecular pathways operative in cancer cells and their complex interactions with the immune system and the tumor microenvironment has also led to the development of targeted agents, immunotherapies, and personalized treatment approaches associated with significant clinical benefit.TABLE 22-1
| ESTIMATED NEW CANCER CASES AND RATES OF DEATH FOR MOST COMMON CANCER DIAGNOSES IN THE US FOR 2020 | ||||
| Sites | New Cases Both Sexes | Male | Female | Deaths Total |
| Lung | 228,820 | 116,300 | 112,520 | 135,720 |
| Prostate | 191,930 | 191,930 | — | 33,330 |
| Breast | 279,100 | 2,620 | 276,480 | 42,690 |
| Colon/rectal | 147,950 | 78,300 | 69,650 | 53,200 |
Risk Factors
• Tobacco use is the most common cause of cancer and is associated with lung, head and neck, esophageal, gastric, pancreatic, kidney, and bladder cancers.
• Diet, obesity, inactivity, and alcohol abuse have been associated with increased risk of developing certain cancers.
• Chronic inflammatory states such as ulcerative colitis and infections including HIV, hepatitis, Epstein- Barr virus (EBV), human papillomavirus (HPV) and Helicobacter pylori are associated with
increased cancer risk.
• Numerous familial cancer syndromes have been described and have important implications for cancer risk and screening (Table 22-2).
• Prior exposure to cytotoxic chemotherapy or radiation therapy is associated with an increased risk of secondary cancers. For example, exposure to alkylating agents or topoisomerase II inhibitors increases the risk of treatment-related leukemia, and exposure to radiation therapy increases risk for cancers such as breast cancer, angiosarcoma, and osteosarcoma.
TABLE 22-2
LIST OF SELECTED FAMILIAL CANCER SYNDROMES WITH HIGH PENETRANCE
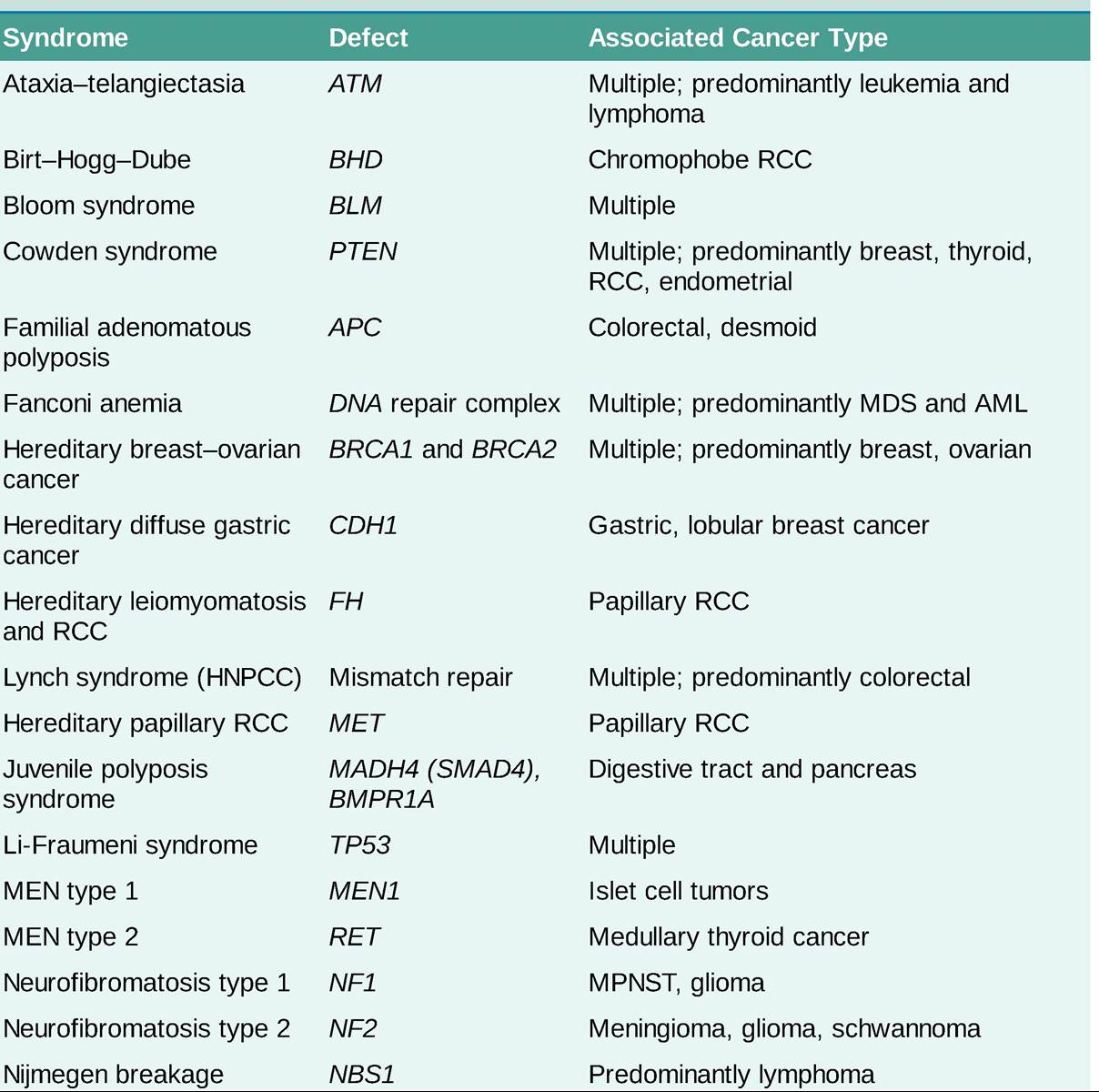
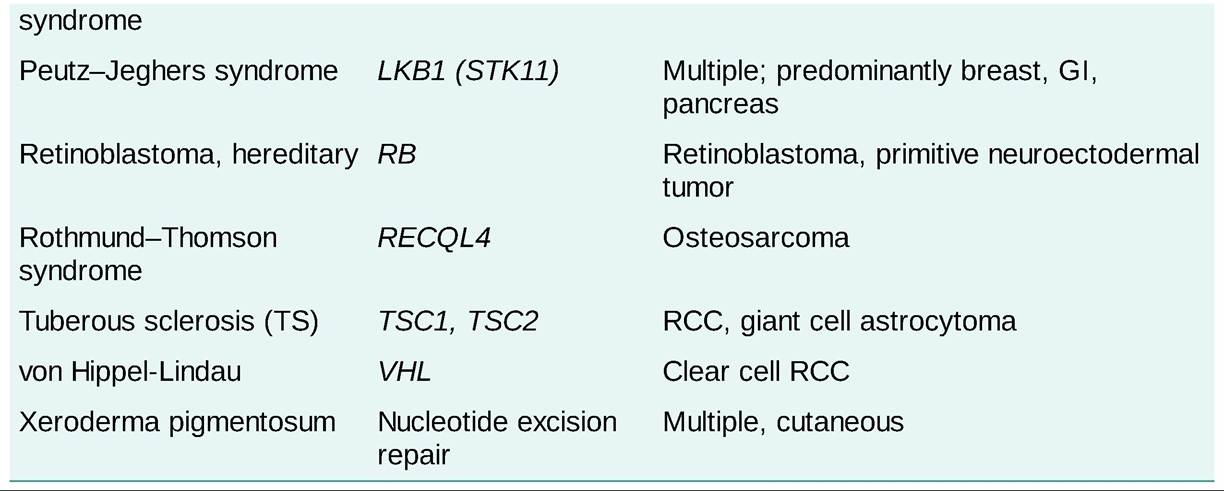
AML, acute myeloid leukemia; GI, gastrointestinal; HNPCC, hereditary nonpolyposis colorectal cancer; MDS, myelodysplastic syndrome; MEN, multiple endocrine neoplasia; MPNST, malignant peripheral nerve sheath tumor; RCC, renal cell carcinoma.
DIAGNOSIS
• Obtaining tissue is crucial for obtaining a definitive diagnosis, examining molecular features of the cancer, and planning treatment.
• Cytology specimens often consist of only a few malignant cells that are obtained either invasively through fine-needle aspiration (FNA), brushings (Pap smear or endoscopic), or aspiration of body fluids (blood, cerebrospinal fluid [CSF], pleural, pericardial, or peritoneal) or noninvasively through collection of fluids such as sputum and urine. Although these approaches are relatively less invasive compared to surgical biopsies, cytologic samples may be inadequate for molecular testing.
Furthermore, the absence of information about tissue architecture may prevent a final diagnosis in certain malignancies, such as lymphomas.• Histology specimens are obtained through core-needle biopsies, excisional biopsies, or surgical resection. These specimens are ideal for diagnosing most malignancies and provide sufficient tissue for molecular testing, although they are more invasive.
STAGING
• Once a tissue diagnosis is obtained, most cancer patients require additional imaging, procedures, and laboratory testing to determine the extent of disease and stage.
• Cancer stage provides an assessment of the extent of tumor dissemination, which is crucial for determining prognosis and treatment planning.
• The staging workup is cancer and patient specific and also varies by local and institutional patterns of practice. Organizations such as the American Society of Clinical Oncology, American Society of Hematology, National Comprehensive Cancer Network, and European Society of Medical Oncology review the available evidence and issue periodic recommendations to guide appropriate staging and management.
î Most solid malignancies are staged according to the tumor, lymph node, and metastasis (TNM) system with stages I to IV The T classification is based on the size and extent of local invasion. The N classification describes the extent of lymph node involvement and the M classification is based on the presence or absence of distant metastases.
° Most hematologic malignancies do not use TNM staging, but rather use disease-specific staging and risk criteria, which are frequently based on a combination of relevant clinical cytogenetic and molecular features.
î Performance status provides a quantitative measure of a patient's functional capacity and quality of life, with important implications for treatment planning (Table 22-3).
TABLE 22-3
| EASTERN COOPERATIVE ONCOLOGY GROUP (ECOG) AND KARNOFSKY SCORE | ||
| ECOG | Karnofsky Score Correlate | Description |
| 0 | 100 | Fully active, able to carry on all predisease performance without restriction. |
| 1 | 80-90 | Restricted in physically strenuous activity but ambulatory and able to carry out work of a light or sedentary nature (e.g., light housework, office work). |
| 2 | 60-70 | Ambulatory and capable of all self-care but unable to carry out any work activities. Up and about gt;50% of waking hours. |
| 3 | 40-50 | Capable of only limited self-care, confined to bed or chair gt;50% of waking hours. |
| 4 | 20-30 | Completely disabled. Cannot carry on any self-care. Totally confined to bed or chair. |
| 5 | 0 | Dead. |
Reprinted with permission from Oken MM, Creech RH, Tormey DC, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol. 1982;5(6):649-655.
TREATMENT
Surgical Therapy
• Surgical resection is often performed with curative intent, although select patients may benefit from palliative surgery performed to debulk large tumor masses (ovarian cancer), increase the efficacy of immunotherapy (renal cell carcinoma [RCC]), or relieve local symptoms (mastectomy in a patient with metastatic disease breast cancer).
• Surgery can facilitate staging and guide subsequent therapeutic decisions including the need for adjuvant treatment.
• Surgical resection of isolated or oligometastatic sites in select patients may improve survival. Some examples include solitary brain metastases, pulmonary metastases in sarcoma, and liver metastases in colorectal cancer.
Radiation Therapy
• Commonly used forms of radiation include external-beam photons, electrons, and protons.
• Brachytherapy is an alternative delivery method, where radioactive sources are placed close to or in
contact with the target tissue. Brachytherapy sources can be temporary or permanent.
• Radioactive therapy can also be administered systemically (oral iodine-131 in thyroid cancer, injection of yttrium-90 microspheres into liver vasculature in hepatocellular cancer, and intravenous radium-223 for prostate cancer with skeletal metastases).
• Radiation therapy planning is designed to optimize precision doses of radiation to a tumor while minimizing radiation to surrounding tissues.
• Curative intent radiotherapy is used in several settings.
î Neoadjuvant: Preoperative therapy intended to reduce both the extent of surgery and the risk of local relapse. Radiation in this setting is commonly administered in combination with chemotherapy.
î Adjuvant: Postoperative therapy intended to reduce the risk of local relapse.
î Definitive: High dose with curative intent.
î Concurrent chemoradiation: Chemotherapy combined with definitive radiation is associated with increased efficacy but also increased toxicity compared to chemotherapy or radiation alone.
• Palliative radiotherapy is used to reduce cancer-related symptoms, such as bone pain, bleeding, and neurologic symptoms.
• The total dose of radiation administered is usually divided over multiple days (fractionated), which allows normal tissue to repair and increases the probability of delivering radiation to tumor cells in a radiosensitive phase of the cell cycle. Radiation treatments are typically delivered on conventional fractionation, hypofractionation, hyperfractionation, or accelerated fractionation schedules, as detailed below.
î Conventional fractionation consists of daily fractions typically of 1.8-2.0 Gy, 5 days per week.
î Hypofractionation consists of delivering radiation divided into larger doses, with treatment once a day or less often.
î Hyperfractionation refers to delivering radiation in smaller doses per fraction, with treatments more than once per day.
Additional Local Therapies
Local ablative therapy with modalities such as lasers, cryoablation, microwave, radiofrequency, and high intensity-focused ultrasound is increasingly used in cancer patients for pain palliation, for attempting local disease control or in treating oligometastatic disease in certain types of cancer.
Chemotherapy
• Cytotoxic chemotherapy targets all dividing cells and has a broad spectrum of toxicities, which can be life-threatening.
• In patients with resectable disease, chemotherapy may be used before (neoadjuvant) or following surgery (adjuvant).
• Chemotherapy is typically given in cycles of 1-4 weeks. In most regimens, IV treatment is given on the first few days of the cycle, with no further treatment until the next cycle. In other regimens, treatments are administered weekly for 2-3 weeks, with 1 week off between cycles.
• Curative intent chemotherapy often includes neoadjuvant, adjuvant, and chemoradiation regimens in solid tumors. Chemotherapy alone or in combination with immunotherapy or stem cell transplantation may be curative in many lymphomas, leukemias, and germ cell tumors (GCTs).
• Palliative chemotherapy is used in advanced solid tumors and relapsed hematologic malignancies, with a focus on prolonging survival and improving the quality of life.
• Most agents have a narrow therapeutic index and dosing is based on weight (mg/kg) or body surface area (mg/m2), with close attention to renal, hepatic, and bone marrow function.
Targeted Therapy
• The use of molecularly targeted agents has led to improved outcomes in many cancer-types.
• The most common classes of drugs are monoclonal antibodies and receptor tyrosine kinase inhibitors (TKIs). Monoclonal antibodies (mAbs) are administered IV and by standard nomenclature have names that end with the stem -mab. Substems indicate the source and target of the antibody. The most common source substems in oncology include -xi- indicating a chimeric antibody (cetuximab), -zu- indicating humanized antibody (bevacizumab), and -u- indicating fully human antibodies (ipilimumab). The most common target substems include -ci- indicating circulatory system (bevacizumab), -tu- indicating tumor (cetuximab), and -li- indicating immune system modulating (ipilimumab).
• TKIs are administered orally and have names that end with -ib.
• Most monoclonal antibodies are used in combination with chemotherapy or radiation, whereas TKIs are commonly used as single agents or in combination with other TKIs.
• Toxicities of targeted therapies are unique to each agent, although specific classes of drugs can be associated with characteristic side effects.
î Inhibitors of the epidermal growth factor receptor (EGFR) frequently cause an acne-like rash on the face and upper chest, which can be severe. Treatment is typically with topical corticosteroids or oral tetracyclines (minocycline, doxycycline).
î Inhibitors of human epidermal growth factor receptor 2 (HER2) are associated with a reversible decline in cardiac systolic function, which should be monitored closely.
° Inhibitors of angiogenesis are associated with endothelial toxicity, leading to hypertension, proteinuria, delayed wound healing, cardiac toxicity, bleeding, thromboembolism, and gastrointestinal (GI) perforation or fistula. All antiangiogenics should be held in the perioperative period due to impaired wound healing.
Immunotherapy
Under normal physiological conditions, the innate and adaptive immune system perform surveillance for and elimination of cancer cells within the body. In addition, the immune system maintains self-tolerance via checkpoint molecules to prevent autoimmunity and limit collateral inflammatory damage to normal tissues during response to infections. However, tumor cells may co-opt this pathway to escape T cell- induced antitumor activity.
• Programmed cell death 1 (PD-1) is one such immune checkpoint and is a receptor expressed primarily on the surface of activated T cells. Binding of PD-1 to one of its ligands, PD-L1 or PD-L2, inhibits the cytotoxic T cell response. PD-1 and PD-L1 interactions may be blocked by monoclonal antibodies against PD-1 (nivolumab, pembrolizumab) or PD-L1 (atezolizumab, durvalumab, avelumab). These immune checkpoint inhibitors (ICIs) have been approved for the treatment of numerous solid and hematologic malignancies. In addition, PD-L1 expression by immunohistochemistry (IHC) has been associated with response to anti-PD-1 or PD-L1 antibodies in some, but not all cancers.
• Chimeric antigen receptor T cells (CAR-Ts) are genetically engineered T cells with specialized receptors which target antigens expressed on tumor cells, such as CD19 or BCMA, to promote an anticancer immune response. Currently, five CAR-Ts have been approved by the Food and Drug Administration (FDA) in the US for certain hematologic malignancies, with many more in clinical development for both solid and hematologic malignancies.
• Other modalities of immunotherapy include engineered, antibody-based bispecific T cell-engaging therapies such as blinatumomab (CD3 ? CD19), which engage T cells and cancer cells to promote an anticancer immune response.
Response to Therapy
Objective assessment of changes in tumor burden is crucial for planning cancer treatment and evaluating treatment efficacy. Criteria such as the Response Evaluation Criteria in Solid Tumors (RECIST) are commonly used for this purpose (Table 22-4). Whereas response assessments for hematologic malignancies often use disease-specific criteria such as Lugano classification and Deauville five-point scale for lymphoma, International Working Group (IWG) Criteria for leukemia, International Myeloma Working Group (IMWG) Criteria for multiple myeloma, and others.
SUMMARY OF SELECTED RESPONSE EVALUATION CRITERIA IN SOLID TUMORS (RECIST) 1.1 CRITERIA
| Measurable lesions | Tumor: gt;10 mm in longest diameter (LD) on axial CT or MRI Lymph node: gt;15 mm in short axis on CT |
| Method | Sum of longest diameter (SLD) of the lesions in axial plane. Up to five target lesions (two per organ). |
Response
| Complete response (CR) | Disappearance of all non-nodal target lesions. All target lymph nodes must be lt;10 mm in short axis. |
| Partial response (PR) | At least 30% decrease in the SLD of target lesions, with baseline sum of diameters as reference. |
| Progressive disease (PD) | New lesions or SLD increased by #8805;20%. |
| Stable disease (SD) | Neither PR nor PD. |