Heart Failure General Principles
Definition
Heart failure (HF) is a clinical syndrome in which either structural or functional abnormalities of the heart impair its ability to fill with or eject blood, resulting in dyspnea, fatigue, and fluid retention.1,2 HF is a progressive disorder and is associated with high morbidity and mortality.
Classification
• HF may be due to abnormalities in myocardial contraction (systolic dysfunction), relaxation and filling (diastolic dysfunction), or both.
• Left ventricular (LV) ejection fraction (EF) is used to subdivide HF patients into groups for therapeutic and prognostic purposes.3 These groups are:
î EF ≤40%: HF with reduced EF (HFrEF)
î EF 41%-49%: HF with mildly reduced EF (HFmrEF)
î EF ≥50%: HF with preserved EF (HFpEF)
• EF with baseline ≤40%, a ≥10-point increase from baseline EF, and a second measurement of LVEF >40%: HF with improved EF (HFimpEF).
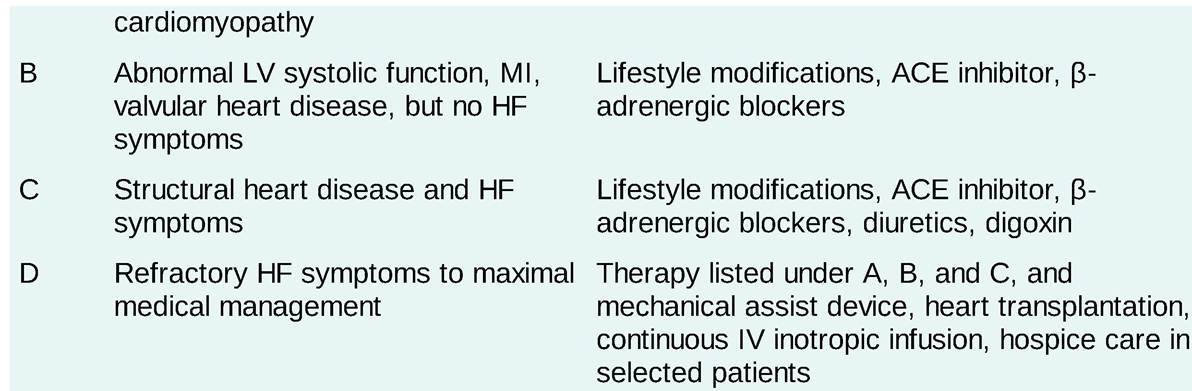
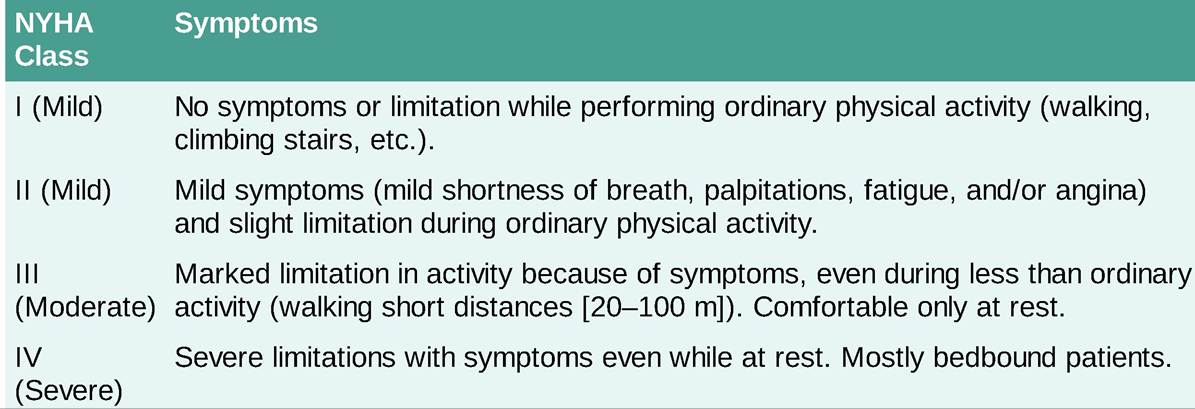
• HF is classified in terms of natural history by American College of Cardiology/American Heart Association (ACC/AHA) HF stage and in terms of symptom status by New York Heart Association (NYHA) Functional Class (Tables 5-1 and 5-2).
TABLE 5-1
AMERICAN COLLEGE OF CARDIOLOGY/AMERICAN HEART ASSOCIATION GUIDELINES OF EVALUATION AND MANAGEMENT OF CHRONIC HEART FAILURE IN ADULTS
![]()
![]()
ACE, angiotensin-converting enzyme; CAD, coronary artery disease; DM, diabetes mellitus; HF, heart failure; HTN, hypertension; LV, left ventricular; MI, myocardial infarction.
Adapted from Yancy CW, Jessup M, Bozkurt B, et al. 2017 ACC/AHA/HFSA focused update of the 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America.
Circulation. 2017;136(6):e137-e161. TABLE 5-2
NEW YORK HEART ASSOCIATION (NYHA) FUNCTIONAL CLASSIFICATION
![]()
Epidemiology
• In the United States, over 6.5 million adults over 20 years of age are living with HF and this number is expected to exceed 8 million by 2030.4
• Approximately 1 million new cases of HF are diagnosed each year.
• HF accounts for approximately 1 million hospitalizations per year.
• Estimated 1- and 5-year mortality rates are 22% and 42.3%, respectively.5
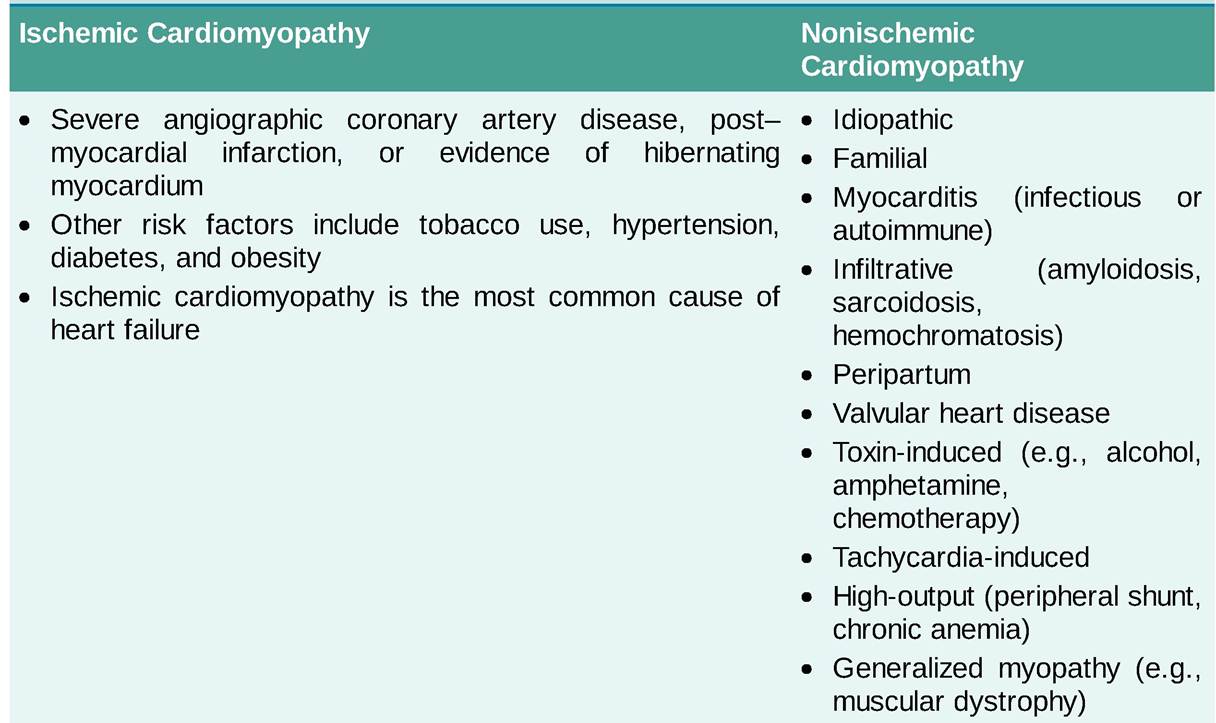
Etiology
See Table 5-3.
HEART FAILURE ETIOLOGY
![]()
Pathophysiology
• HF begins with an initial insult leading to myocardial injury.
• Regardless of etiology, the myocardial injury leads to a pathologic remodeling, which manifests as an increase in LV volume (dilatation) and/or mass (hypertrophy).
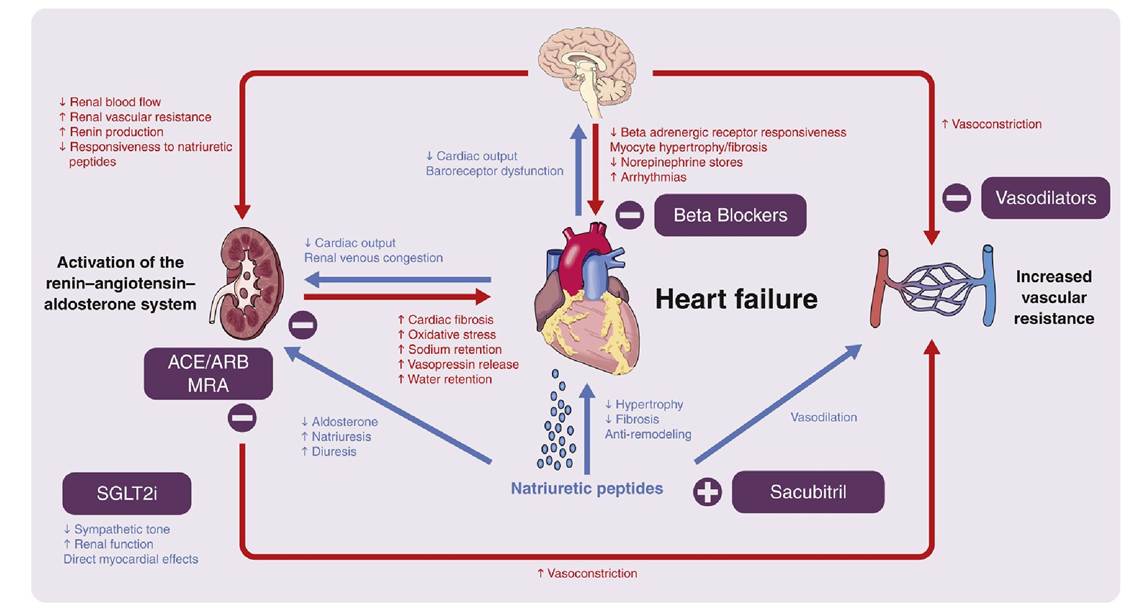
• Compensatory adaptations initially maintain cardiac output; specifically, there is activation of the renin-angiotensin-aldosterone system (RAAS) and vasopressin (antidiuretic hormone), which leads to increased sodium retention and peripheral vasoconstriction. The sympathetic nervous system is also activated (Figure 5-1), with increased levels of circulating catecholamines, resulting in increased myocardial contractility. Over time, these neurohormonal pathways result in direct cellular toxicity, fibrosis, arrhythmias, and pump failure.
![]()
Figure 5-1 Activation of the sympathetic nervous system,ACE, angiotensin-converting enzyme; ARB, angiotensin II receptor blocker; SGLT2i, sodium-glucose cotransporter 2 inhibitor.
Diagnosis
Clinical Presentation
History
• Afflicted patients most commonly present with the following symptoms:
î Dyspnea (on exertion and/or at rest)
î Fatigue
î Exercise intolerance
î Orthopnea, paroxysmal nocturnal dyspnea
° Bendopnea (dyspnea when leaning forward)
î Systemic or pulmonary venous congestion (lower extremity swelling or cough/wheezing)
° Presyncope, palpitations, and angina may also be present
• Other possible presentations include incidental detection of asymptomatic cardiomegaly or symptoms related to coexisting arrhythmia, conduction disturbance, thromboembolic complications, or sudden death.
• Clinical manifestations of HF vary depending on the severity and rapidity of cardiac decompensation, underlying etiology, age, and comorbidities of the patient.
• Extreme decompensation may present as cardiogenic shock (resulting from both low arterial and high venous pressures), characterized by hypoperfusion of vital organs, renal failure (decreased urine output), mental status changes (confusion and lethargy), or “shock liver” (elevated liver function tests).
Physical Examination
• The goal of the physical examination in HF is to estimate intracardiac pressures, cardiac output, and end-organ perfusion.
• Elevated right-sided pressures result in lower extremity edema, jugular venous distension (JVD), abdominojugular reflux, pleural and pericardial effusions, hepatic congestion, and ascites.
• JVD is the most specific and reliable physical examination indicator of right-sided volume overload and is representative of left-sided filling pressures except in cases of disproportionate right heart dysfunction (e.g., pulmonary hypertension, severe tricuspid regurgitation, and pericardial disease).
• JVD is best visualized with oblique light and the patient at 45 degrees. Venous pulsations are differentiated from carotid pulsation by their biphasic nature, respiratory variability, and compressibility.
• Abdominojugular reflux suggests an impaired ability of the right ventricle to handle augmented preload and may be due to constriction or pulmonary hypertension in addition to myocardial disease.
• Elevated left-sided pressures may result in pulmonary rales, but rales are absent in the majority of HF patients with elevated left-sided filling pressures.
• In the setting of systolic dysfunction, a third (S3) or fourth (S4) heart sound as well as the holosystolic murmurs of tricuspid or mitral regurgitation (MR) may be present; carotid upstrokes may also be diminished.
• Low cardiac output is suggested by a proportional pulse pressure (pulse pressure/diastolic blood pressure) ≤25%, diminished carotid upstroke, and cool extremities.
Diagnostic Testing
Laboratories
• Initial laboratory studies should include complete blood count, basic metabolic panel, magnesium, liver function tests, lipid profile, and thyroid function tests.
• B-type natriuretic peptide (BNP) and the biologically inactive cleavage product N-terminal prohormone BNP (NT-proBNP) are released by myocytes in response to stretch, volume overload, and increased filling pressures. Natriurietic peptides serve as a natural compensatory mechanism to enhance natriuresis.
î Elevated BNP/NT-proBNP is present in patients with asymptomatic LV dysfunction as well as symptomatic HF.
î BNP/NT-proBNP levels have been shown to correlate with HF severity and to predict survival.6 A serum BNP >400 pg/mL is consistent with HF; however, specificity is reduced in patients with renal dysfunction and levels may be low in the setting of obesity. A serum BNP level bgcolor=white>24/26 mg bid
97/103 mg bid | | IKf Channel Inhibitor | | |
| Ivabradine | 5 mg bid | 7.5 mg bid |
| Thiazide Diuretics | | |
| Hydrochlorothiazide | 25-50 mg daily | 25-50 mg daily |
| Metolazone | 2.5-5.0 mg daily or bid | 10-20 mg total daily |
| Loop Diuretics | | |
| Bumetanide | 0.5-1.0 mg daily or bid | 10 mg total daily (maximum) |
| Furosemide | 20-40 mg daily or bid | 400 mg total daily (maximum) |
| Torsemide | 10-20 mg daily or bid | 200 mg total daily (maximum) |
| Aldosterone Antagonists Eplerenone | 25 mg daily | 50 mg daily |
| Spironolactone β-Blockers | 12.5-25.0 mg daily | 25 mg daily |
| Bisoprolol | 1.25 mg daily | 10 mg daily |
| Carvedilol | 3.125 mg bid | 25-50 mg bid |
| Metoprolol succinate | 12.5-25.0 mg daily | 200 mg daily |
| Digoxin | 0.125-0.25 mg daily | 0.125-0.25 mg daily |
HydralazineZIsosorbide 37.5 mg/20 mg tid 75 mg/40 mg TID
Dinitrate
aValsartan and candesartan are the only U.S.
Food and Drug Administration-approved angiotensin II receptor blockers in the treatment of heart failure. î Typically, 2-3 months of therapy is required to observe significant effects on LV function, but reduction of cardiac arrhythmia and incidence of sudden cardiac death (SCD) may occur much earlier.13
î β-Blockers should be instituted at a low dose and titrated with careful attention to blood pressure and heart rate. Some patients experience volume retention and worsening HF symptoms that typically respond to transient increases in diuretic therapy.
î The survival benefit of β-blockers is proportional to the heart rate reduction and dosage achieved.
î Individual β-blockers have unique properties, and the beneficial effects of β-blockers are not a class effect. Therefore, one of the three β-blockers with proven benefit on mortality in large clinical trials should be used:
■ Carvedilol14,15
■ Metoprolol succinate16
■ Bisoprolol17
• Angiotensin receptor-neprilysin inhibitor. SacubitriiZvalsartan is a combination of the neprilysin inhibitor (sacubitril) and ARB (valsartan).
° Neprilysin is a neutral endopeptidase involved in the degradation of vasoactive peptides including the natriuretic peptides, bradykinin, and adrenomedullin. Inhibition of neprilysin increases the availability of these peptides, which exert favorable effects in HF.
î Sacubitril/valsartan was shown to be superior to enalapril in reducing death and rehospitalization among NYHA class II-IV patients with HFrEF who were stably tolerant of ACE inhibitor or ARB therapy.18
î Sacubitril/valsartan is approved for use in patients with HFrEF and NYHA class II-IV symptoms.
î Rates of angioedema are increased with sacubitril/valsartan compared with ACE inhibitors (0.5% vs. 0.2%) and require a 36-hour ACE inhibitor washout prior to initiation. Angioedema rates were comparatively higher in African-Americans (2.4% vs.
0.5%). • ACE inhibitors and ARBs target the compensatory RAAS activation and attenuate vasoconstriction, vital organ hypoperfusion, hyponatremia, hypokalemia, and fluid retention. These medications should be used as second-line therapy if patients cannot tolerate or afford ARNI.
î ACE inhibitors
■ Multiple large clinical trials have clearly demonstrated that ACE inhibitors improve symptoms and survival in patients with LV systolic dysfunction.1
■ ACE inhibitors may also prevent the development of HF in patients with asymptomatic LV dysfunction and in those at high risk of developing structural heart disease or HF symptoms (e.g., patients with CAD, diabetes mellitus, hypertension).
■ No consensus exists on optimal dosing of ACE inhibitors in HF. Higher doses have been shown to reduce morbidity without improving overall survival.19
■ Most ACE inhibitors are excreted by the kidneys, necessitating careful dose titration in patients with renal insufficiency. ACE inhibitors should be used cautiously in the presence of renal dysfunction and use should be avoided in patients with bilateral renal artery stenosis. Renal function and potassium levels should be monitored with dose adjustment and periodically with chronic use.
■ A rise in serum creatinine up to 30% above baseline may be seen when initiating an ACE inhibitor and should not result in reflexive discontinuation of therapy.20
■ Additional adverse effects may include cough, rash, angioedema, dysgeusia, hyperkalemia, and leukopenia.
■ Oral potassium supplements, potassium salt substitutes, and potassium-sparing diuretics should be used with caution during treatment with an ACE inhibitor.
■ ACE inhibitors are contraindicated in pregnancy. Enalapril and captopril may be safely used by breastfeeding mothers.
î ARBs
■ ARBs reduce morbidity and mortality associated with HF in patients who are not receiving an ACE inhibitor21-23 and therefore should be instituted when ACE inhibitors are not tolerated.
■ In contrast to ACE inhibitors, ARBs do not increase bradykinin levels and therefore are not associated with cough.
■ Renal precautions and monitoring for ARB use are similar to ACE inhibitor use.
■ Use of ARBs is contraindicated in patients taking both ACE inhibitors and aldosterone antagonists due to a high risk for hyperkalemia.
■ ARBs are contraindicated in pregnancy and breastfeeding.
• MRAs attenuate aldosterone-mediated sodium retention, vascular reactivity, oxidant stress, inflammation, and fibrosis.
î MRAs are recommended for use in patients with NYHA class II-IV HF and acceptable renal function (serum creatinine is and HF hospitalizations when added to standard therapy in patients with HFrEF with or without diabetes.27,28 î Canagliflozin has been shown to decrease the composite outcome of cardiovascular mortality, nonfatal MI, or nonfatal stroke in patients with type 2 diabetes and elevated cardiovascular risk. Post-hoc analysis showed canagliflozin reduced cardiovascular mortality and HF hospitalizations across a range of subgroups.29
î Sotagliflozin is a dual SGLT1 and SGLT2 inhibitor that has been shown to reduce cardiovascular death and HF hospitalizations or urgent visits when initiated shortly before or after inpatient discharge in patients with HF and diabetes irrespective of EF.30
î Currently, the U.S. Food and Drug Administration (FDA) has approved dapagliflozin and empagliflozin for treatment of HFrEF independent of diabetes.
• Diuretic therapy in conjunction with restriction of dietary sodium and fluids often leads to clinical improvement in patients with symptomatic HF. Frequent assessment of the patient's weight and careful observation of fluid intake and output are essential during initiation and maintenance of therapy.
î Complications of therapy include hypokalemia, hyponatremia, hypomagnesemia, volume contraction alkalosis, intravascular volume depletion, and hypotension. Therefore, serum electrolytes, BUN, and creatinine levels should be monitored after institution of diuretic therapy.
î Hypokalemia may be life threatening in patients who are receiving digoxin or are predisposed to ventricular arrhythmias.
î Loop diuretics (furosemide, torsemide, bumetanide, ethacrynic acid) should be used in patients who require significant diuresis and in those with markedly decreased renal function.
■ Furosemide reduces preload acutely by causing direct venodilation when administered intravenously, making it useful for managing severe HF or acute pulmonary edema.
■ Use of loop diuretics may be complicated by hyperuricemia, hypocalcemia, ototoxicity, rash, and vasculitis. Furosemide, torsemide, and bumetanide are sulfa derivatives and may rarely cause drug reactions in sulfa-sensitive patients; ethacrynic acid can be used in such patients.
■ Dose equivalence of oral loop diuretics is approximately 50 mg ethacrynic acid = 40 mg furosemide = 20 mg torsemide = 1 mg bumetanide.
■ Torsemide and bumetanide have >80% oral bioavailability as compared to ~50% bioavailability of furosemide. In patients requiring increased dosage of furosemide, transition to torsemide or bumetanide should be considered.
î Thiazide diuretics (hydrochlorothiazide, chlorthalidone) can be used as initial agents in patients with normal renal function in whom only a mild diuresis is desired.
■ Metolazone, unlike other oral thiazides, exerts its action at the proximal and distal tubule and may be useful in combination with a loop diuretic in patients with a low glomerular filtration rate.
î Potassium-sparing diuretics (amiloride, triamterene) do not exert a potent diuretic effect when used alone.
• Second-line therapies—In patients who have ongoing symptoms despite maximization of the four cornerstone medications mentioned above or have intolerance/contraindications preventing use of certain agents, additional therapies may provide benefit.
î Vasodilator therapy alters preload and afterload to improve cardiac output.
■ Hydralazine acts directly on arterial smooth muscle cells to produce vasodilation and reduce afterload. Reflex tachycardia and increased myocardial oxygen consumption may occur in the setting of hydralazine use, requiring cautious use in patients with ischemic heart disease.
■ Nitrates are predominantly venodilators and help relieve symptoms of congestion. They also reduce myocardial ischemia by decreasing ventricular filling pressures and by directly dilating coronary arteries. Nitrate therapy may precipitate hypotension, especially in patients who have low preload or are taking phosphodiesterase inhibitors.
■ A combination of hydralazine and isosorbide dinitrate (starting dose: 37.5/20 mg three times daily), when added to β-blockers and ACEi/ARB, was shown to reduce mortality in African- American patients.31
■ In the absence of ACEi/ARBs, MRAs, and β-blockers, the combination of nitrates and hydralazine improves survival in patients with HFrEF32 and should therefore be considered for use in HFrEF patients unable to tolerate RAAS blockade.
î Vericiguat is a soluble guanylate cyclase stimulator that increases cyclic guanosine monophosphate, leading to vasodilation and improved endothelial function.
■ Vericiguat was shown to reduce cardiovascular death and HF hospitalization in patients with HFrEF and worsening symptoms or recent decompensation.33 It is indicated for use in this population as an addition to background therapy with ACE/ARB/ARNI, MRAs, and β-blockers.
î Ivabradine is an inhibitor of the IKf channel involved in generating “pacemaker” currents in cardiac
tissue.
■ Ivabradine was shown to reduce HF hospitalization and HF death in outpatients with HFrEF and is indicated for the reduction of HF hospitalization in patients with EF is a synthetic analog of dopamine with predominantly β1- adrenoreceptor activity. It increases cardiac output, lowers cardiac filling pressures, and generally has a neutral effect on systemic blood pressure. Dobutamine tolerance has been described, and several studies have demonstrated increased mortality in patients treated with continuous dobutamine. Dobutamine has no significant role in the treatment of HF resulting from diastolic dysfunction or a high-output state.
TABLE 5-5
| INQTRQPiCZSYMPATHQMiMETiC AGENTSa |
| Drug | Dose | Mechanism | EffectsZSide Effects |
| Dopamine | 1-3 μg∕kg∕min | Dopaminergic receptors | Splanchnic vasodilation |
| | 2-8 μg∕kg∕min | β1-Receptor agonist | +Inotropic |
| | 7-10 μg∕kg∕min | α-Receptor agonist | ↑ SVR |
| Dobutamine | 2.5-15.0 μg∕kg∕min | β1- > β2- > α- receptor agonist | +Inotropic, t SVR, tachycardia |
| Epinephrine | 0.05-1 μg∕kg∕min; titrate to desired mean arterial | β1 > α1 | +Inotropic, ↑ |
| | pressure. May adjust dose every 10-15 min by 0.05-0.2 μg∕kg∕min to achieve desired blood pressure goal | Low doses = β High doses = α | SVR |
| Milrinoneb | 50-μg∕kg bolus IV over 10 min, 0.375-0.75 μg∕kg∕min | ↑ cAMP | +Inotropic, ł SVR |
cAMP, cyclic adenosine monophosphate; SVR, systemic vascular resistance; ↑, increased; r, decreased. aIncreased risk of atrial and ventricular tachyarrhythmias.
bNeeds dose adjustment for creatinine clearance.
î Phosphodiesterase inhibitors increase myocardial contractility and produce vasodilation by increasing intracellular cyclic adenosine monophosphate. Milrinone is indicated for treatment of refractory HF. Hypotension may develop in patients who receive vasodilator therapy or have intravascular volume contraction, or both. Milrinone may improve hemodynamics in patients who are treated concurrently with dobutamine or dopamine. Data suggest that in-hospital short-term milrinone administration in addition to standard medical therapy does not reduce the l ength of hospitalization or the 60-day mortality or rehospitalization rate when compared with placebo.41
• Oralinotropes
î Omecamtiv mecarbil binds cardiac myosin and directly augments cardiac sarcomere function. Use of omecamtiv mecarbil in addition to guideline medical therapy in patients with NYHA II-IV HF resulted in lower rates of the composite outcome of HF events or cardiovascular death.42 This agent is not yet FDA approved.
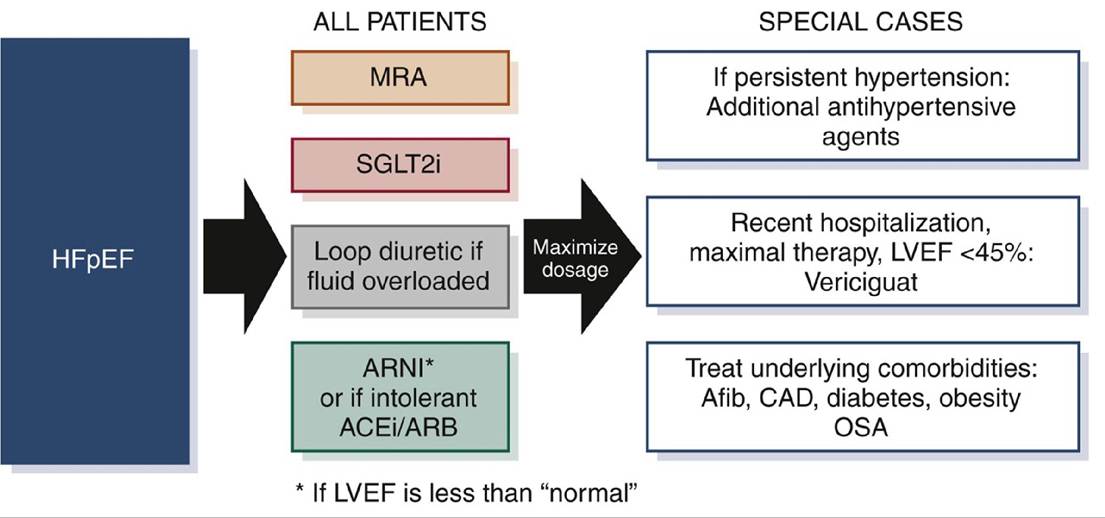
Chronic Medical Therapy With Preserved Ejection Fraction (Figure 5-3)
![]()
Figure 5-3 Chronic medical therapies for heart failure with preserved ejection fraction (HFpEF).ACEi, angiotensin-converting enzyme inhibitor; Afib, atrial fibrillation; ARB, angiotensin II receptor blocker; ARNI, angiotensin receptor-neprilysin inhibitor; CAD, coronary artery disease; LVEF, left ventricular ejection fraction; OSA, obstructive sleep apnea; SGLT2i, sodium-glucose cotransporter 2 inhibitor.
• No pharmacotherapy has been definitively shown to improve mortality in HFpEF.
î The use of ACE inhibitors, ARBs, spironolactone, and β-blockers is reasonable and may be associated with a small reduction in HF hospitalization rates.
î Sacubitril/valsartan did not reduce cardiovascular mortality or HF hospitalizations compared to valsartan in patients with HFpEF and EF >45%. However, sacubitril/valsartan did have a beneficial effect in patients who had less than normal LVEF. Therefore, FDA has approved sacubitril/valsartan for use in all patients with HFpEF, with benefit most likely in patients with less than normal LV systolic function.43,44
î Spironolactone reduced HF hospitalization in patients with HFpEF in a large randomized trial, but mortality was not reduced.45
o SGLT2 inhibitors have the most extensive data for improved outcomes in HFpEF. Empagliflozin reduced the composite outcome of HF hospitalizations and cardiac death in patients with HFpEF, independent of diabetes, driven by decrease in HF hospitalizations.46 In a prespecified, pooled analysis from two placebo-controlled trials of type 2 diabetics with HF, sotagliflozin reduced cardiovascular death and HF hospitalizations or urgent visits, irrespective of EF.30,47 SGLT2 inhibitors should be considered in all patients with HFpEF.
• Control of blood pressure, treatment of atrial fibrillation (AF), and treatment of coronary disease through pharmacotherapy and/or revascularization in accordance with practice guidelines is recommended.
Antiarrhythmic Therapy
• Suppression of asymptomatic ventricular premature beats or nonsustained ventricular tachycardia (NSVT) using antiarrhythmic drugs in patients with HF does not improve survival and may increase mortality as a result of the proarrhythmic effects of the drugs.48
• For patients with AF as a suspected cause of new-onset HF, a rhythm control strategy should be pursued. For patients with preexisting HF who develop AF, despite evidence suggesting improved symptom status in patients treated with rhythm control, the use of antiarrhythmic drug therapy for the maintenance of sinus rhythm has not been shown to improve mortality.49
• Agents recommended for the maintenance of sinus rhythm in HF with reduced LVEF include dofetilide and amiodarone. Sotalol may also be considered in patients with mildly depressed LVEF. These agents require close monitoring of the QT interval. In patients with severe LV systolic dysfunction and HF, dronedarone should not be used.50
• Catheter ablation for AF in patients with HF as compared with medical therapy was associated with a lower rate of mortality in one randomized trial, but guideline consensus for use has not been formalized.51
Anticoagulant and Antiplatelet Therapy
• Although patients with HF are at relatively greater risk for thromboembolic events, the absolute risk is modest, and routine anticoagulation is not recommended in HF patients in the absence of AF, prior thromboembolism, or a cardioembolic source.
• In patients with AF, use of the CHADS2 or CHA2DS2-VASc risk score is recommended for determining when to use anticoagulant therapies.
• The direct oral anticoagulants dabigatran, rivaroxaban, and apixaban have been shown to be effective in HF patients with nonvalvular AF.
• There are insufficient data to support the routine use of aspirin in patients with HF who do not have coronary disease or atherosclerosis.
Nonpharmacologic Therapies for Heart Failure
• Coronary revascularization reduces ischemia and may improve systolic function in patients with CAD and HF.
• Surgical or percutaneous revascularization is recommended in HF patients with angina and suitable anatomy (class I recommendation) and may be considered in patients without angina who have suitable anatomy, whether in the presence of viable myocardium (class IIa recommendation) or nonviable myocardium (class IIb recommendation).1
• In a large, randomized trial of HF patients with CAD and LVEF 40% of the time).
î Factors most strongly favoring response to CRT include female sex, QRS duration ≥150 ms, LBBB, body mass index 1 year with good functional capacity. ICD therapy should not be used in end-stage HF patients who are not candidates for transplantation or durable mechanical circulatory support (MCS).
• CardioMEMS™ is an implantable hemodynamic monitoring system delivered into the pulmonary artery that can be used to monitor a patient's ambulatory pulmonary artery pressures and allow clinicians to adjust medications accordingly. It has been shown to reduce hospitalization in patients with NYHA class III HF, irrespective of LVEF.57
Surgical Management
• Surgical or nonsurgical replacement or repair of the mitral valve in the setting of a reduced LVEF and severe MR is discussed elsewhere (see Chapter 6, Pericardial and Valvular Heart Disease).
î In select patients who are on maximally tolerated medical therapy with symptomatic moderate to severe MR, Mitraclip™ resulted in lower mortality and HF hospitalizations.58
• Left ventricular assist devices (LVADs) are surgically implanted pumps that draw blood from the left ventricle, energize flow through a motor unit, and deliver the energized blood to the aorta, resulting in augmented cardiac output and lower intracardiac filling pressures. These devices may be temporary (CentriMag, percutaneous LVADs) or durable (HeartWare, HeartMate II, HeartMate III). Due to clinical inferiority, HeartWare and HeartMate II are no longer manufactured. HeartMate 3 is the only durable LVAD commercially available in the United States.
î Temporary MCS is indicated for patients with severe HF after cardiac surgery or individuals with intractable cardiogenic shock after acute MI.
° Durable MCS is indicated as a “bridge to transplantation” for patients awaiting heart transplantation or as “destination” therapy for select patients ineligible for transplant with refractory end-stage HF and HF-related life expectancy with therapy of Sleep apnea has a prevalence rate as high as 50% in the HF population. Treatment of obstructive sleep apnea with nocturnal positive airway pressure improves symptoms and EF.63 However, treatment of central sleep apnea with adaptive servo-ventilation in patients with HFrEF was associated with increased mortality.64
• Dialysis or ultrafiltration may be beneficial in patients with severe HF and renal dysfunction who cannot respond adequately to fluid and sodium restriction and diuretics.65 Ultrafiltration is not superior to a scaled diuretic regimen in patients with acute HF and cardiorenal syndrome and is associated with higher rate of adverse events.66 Other mechanical methods of fluid removal such as therapeutic thoracentesis and paracentesis may provide temporary symptomatic relief of dyspnea. Care must be taken to avoid rapid fluid removal and hypotension.
• End-of-life considerations should be strongly considered in patients with advanced HF who are refractory to therapy. Discussions regarding the disease course, treatment options, survival, functional status, and advance directives should be addressed early in the treatment of the patient with HF. For those with end-stage disease (stage D, NYHA class IV) with multiple hospitalizations and severe decline in their functional status and quality of life, hospice and palliative care is recommended.67