Nephrolithiasis
GENERAL PRINCIPLES
Nephrolithiasis is more common in men than women by a 2:1 ratio, with a peak age at the third to fourth decade. There are certain medical conditions that predispose patients to kidney stones, including diabetes mellitus, hypertension, metabolic syndrome, distal renal tubular acidosis, gout, and ADPKD.
• Calcium-based stones are the most common type of kidney stones (80%). Among these, the most common type is mixed calcium oxalate and calcium phosphate followed by calcium oxalate alone, and then calcium phosphate alone. These stones are radiopaque. Calcium oxalate stones can be found in acidic or alkaline urine and can be dumbbell shaped or appear as paired pyramids (giving them an envelope appearance when viewed on end). Calcium phosphate stones can appear as elongated, blunt crystals and form in alkaline urine.
• Uric acid stones (10%) develop in conditions that promote an acidic urine, such as what is observed in patients with the metabolic syndrome. Hyperuricosuric states such as gout and myeloproliferative disorders are also associated with uric acid stones, though the predominant risk factor for their precipitation is an acidic environment. These stones are radiolucent, and the crystals can exhibit a variety of shapes, with needles and rhomboid forms being the most common.
• Struvite stones (10%) are also known as “triple phosphate” stones, with phosphate being present in its trivalent form and combining with three cations, ammonium, magnesium, and calcium. They are radiopaque and can extend to fill the renal pelvis, taking on a staghorn configuration. On microscopy, struvite crystals have a characteristic coffin-lid shape. They develop in alkaline urine associated with urea-splitting organisms (e.g., Proteus, Klebsiella, Serratia, Haemophilus, Pseudomonas) and are more commonly seen in patients with anatomic abnormalities (e.g., vesicoureteral reflux, obstruction of the pelviureteric junction, ureteral stricture).
• Cystine stones (as proteinuria, needs to be present for at least 3 months. Definitions for albuminuria are based on the urinary albumin-to- creatinine ratio as described earlier in the chapter. GFR, degree of albuminuria, etiology of CKD, and other risk factors should be considered together as these predict clinical outcomes and help in planning for renal replacement therapy.
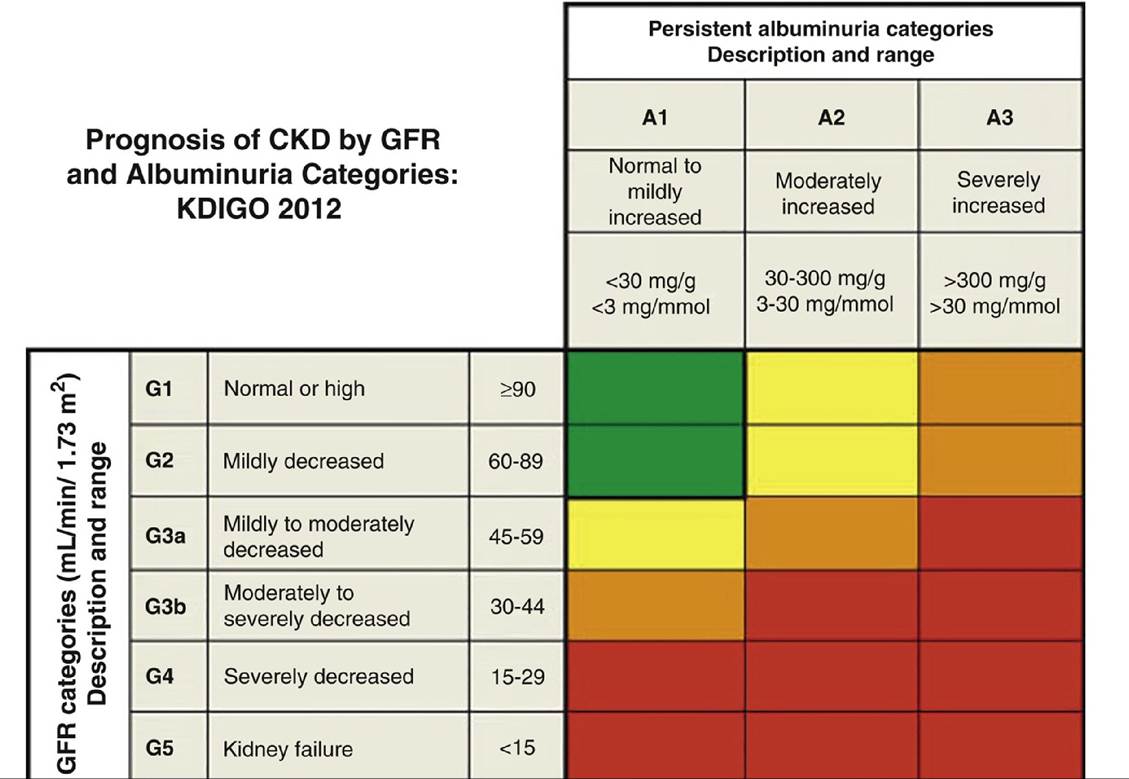
Figure 13-1 Stages of chronic kidney disease. CKD, chronic kidney disease; GFR, glomerular filtration rate.(Reprinted from Summary of recommendation statements. Kidney Int Suppl (2011). 2013;3(suppl):5-14. Copyright © 2013 International Society of Nephrology. With permission.)
• Patients are usually asymptomatic until significant renal function is lost (late stage G4 and stage G5). However, complications including hypertension, anemia, and mineral bone disorders (renal osteodystrophy and secondary hyperparathyroidism) often develop during stage G3 and thus should be investigated and addressed before patients become symptomatic.
• In the setting of CKD, initiation of dialysis based solely on a target GFR has not shown a mortality benefit.43 Dialysis should be started before the worsening of the patient's metabolic or nutritional status.
Risk Factors
• Decreased renal perfusion can lead to a decline in GFR. This can occur with true volume depletion or diminished effective circulating volume (e.g., congestive heart failure, liver cirrhosis with ascites). NSAIDs can be particularly deleterious in this setting because they block renal autoregulatory mechanisms which preserve GFR. ACE inhibitors or ARBs also produce a reversible decrement in GFR through alterations in hemodynamics.
• Uncontrolled hypertension leads to hyperfiltration, which may lead to worsening proteinuria and further damage to the glomeruli.
• Albuminuria has also been identified as a risk factor for progression of renal disease.
A prognostic scale has been developed incorporating both the GFR and degree of albuminuria to predict thelikelihood to renal failure (see Figure 13-1).
• Nephrotoxic agents, such as iodinated contrast agents and aminoglycosides, should be avoided when possible. Careful attention to drug dosing is mandatory, frequently guided by the estimated GFR or CKD stage. Drug levels should be monitored where appropriate.
• Patients undergoing coronary angiography are at particular risk for worsening CKD. Contrast nephropathy and atheroembolic disease are potential complications of coronary angiography, and the risks and benefits of the procedure must be weighed with the patient before proceeding.
• UTI or obstruction should be considered in all patients with an unexplained drop in renal function.
• Worsening renal artery stenosis may also lead to a more rapid decline in GFR as well as sudden worsening of previously controlled hypertension.
• Renal vein thrombosis may occur as a complication of nephrotic syndrome and can exacerbate CKD. Hematuria and flank pain may be present.
• The APOL1 gene has been linked to a major health disparity in patients with African ancestry, with a cumulative lifetime risk of reaching ESRD approximately 7.5% compared to 2% in patients with European ancestry. The high-risk genotypes include homozygous G1/G1, homozygous G2/G2, and compound heterozygous G1/G2. African American patients with or without diabetes mellitus with two APOL1 risk alleles have a faster rate of CKD progression and increased likelihood of developing ESRD.44
• Other risk factors include high BMI, history of cardiovascular disease, and smoking.
TREATMENT
Treatment of CKD is focused on addressing the risk factors mentioned above: dietary modification, blood pressure control, adequate treatment of associated conditions, and ultimately, preparation for renal replacement therapy.
• Dietary recommendations
î Sodium restriction to with a GFR of ≥30 mL/min/1.73 m2.25
• Anemia
î A normocytic anemia is common in CKD and should be evaluated once the GFR falls below 60 mL/min/1.73.
° Alternate causes for an anemia should be sought in the appropriate setting and iron stores assessed.
If the transferrin saturation is ≤30% and there is no evidence of iron overload (ferritin (IHD) typically runs for 3-4 hours per session and is performed three times weekly. Outpatient, in-center hemodialysis for ESRD generally uses this modality, although variations are available for patients undergoing home treatments.• Continuous renal replacement therapy (CRRT) can be used in specialized circumstances, particularly when the patient's hemodynamic status would not tolerate the rapid fluid shifts of IHD. Although less efficient (with slower blood flow) and with slower UF rates, CRRT can achieve equivalent clearances of both solute and fluid compared to IHD due to its continuous, 24-hour nature. The slower blood flows may necessitate anticoagulation (with either systemic heparin or regional citrate) to prevent the filter from clotting. Continuous modalities require specialized nursing and an intensive care setting.
î There are various modalities of CRRT, including continuous venovenous hemodiafiltration (CVVHDF) and continuous venovenous hemodialysis (CVVHD). None of these modalities have been shown to be superior to the others.
î In CVVHDF, blood is slowly pumped counter-currently to a dialysis solution (allowing for diffusive clearance), and a replacement fluid (an isotonic physiologic solution devoid of uremic toxins and other waste products) is infused into the circuit to balance most of the ultrafiltrate (convective clearance). CVVHD does not utilize a replacement fluid and thus convective clearance is not performed.
• Sustained low-efficiency dialysis uses intermediate treatment lengths (8-12 hours), allowing for adequate clearances, while patients can spend a significant portion of the day off the machine to allow for non-bedside testing, procedures, and physical therapy.
• Prescription and adequacy
î IHD typically runs for 3-4 hours and can ultrafilter 3-4 L safely in hemodynamically stable patients. In the chronic setting, IHD is generally performed three times weekly, although the longer interdialytic interval on the weekend has been associated with a heightened mortality risk.51 In the acute setting, the appropriate interval is not clearly defined, although a three times weekly schedule is likely adequate and remains common practice.
î Adequacy is assessed by calculating BUN clearance, which serves as a surrogate marker of the “uremic factors.” The urea reduction ratio can be calculated by the following:

î A reduction rate of ≥65% is considered adequate in the chronic setting.52 An adequacy target is less well defined for AKI. Intensive daily hemodialysis was not shown to be superior to standard three times weekly treatments.53
î Clearance is measured differently in CRRT in which dialytic therapy spans over 24 hours, effectively providing an extracorporeal “GFR.” Drug dosing needs to be adjusted accordingly; an estimate of this clearance can be calculated by the sum of the dialysis fluid, replacement fluid, and net UF rates converted into milliliters per minute. For most circumstances, this approximates a clearance of 20-50 mL/min.
î With CRRT, the net UF rate can be adjusted as needed, according to the patient's hemodynamic status. Electrolyte levels (particularly calcium and phosphorus) should be monitored very carefully to ensure they remain within the desired ranges. Ionized calcium levels are especially important to follow when regional citrate anticoagulation is being used.
î Phosphate, which is predominantly intracellular, is generally poorly removed by IHD; however, in CRRT, there is continuous efflux of this anion, and significant hypophosphatemia can occur.
Complications
• Nontunneled catheters are typically placed in the internal jugular or femoral vein and carry the same risks as other central venous catheters (infection, bleeding, pneumothorax). They are almost exclusively used in the inpatient setting and are typically used for up to 1-2 weeks. Tunneled catheters have lower rates of infection and can be used for 6 months while a more definitive access is maturing (AV fistula or graft).
î Fevers and rigors, particularly during dialysis, should prompt a search for an infectious cause, and empiric antibiotic coverage for staphylococci and gram-negative bacteria should be administered.
î The catheter should then be replaced after a period of defervescence and sterilization of the blood (at least 48 hours). Documented bacteremia should be treated with antibiotics for at least several weeks.
• Thrombosis of an AV fistula or graft can frequently be recanalized by thrombolysis or thrombectomy. Stenotic regions can be evaluated by a fistulogram, and treatment may encompass angioplasty or stent deployment.
• Intradialytic hypotension is most commonly due to intravascular volume depletion from rapid UF. Antihypertensive medications may also contribute. Infectious causes should be considered in the appropriate setting. Acute treatment of hypotension includes infusion of normal saline (as 200-mL boluses) and reduction of the UF rate.
• Dialysis disequilibrium is an uncommon syndrome that may occur in severely uremic patients undergoing their first several treatments. Rapid toxin clearance is thought to result in cerebral edema by osmolar shifts and can present as nausea, emesis, headache, confusion, or seizures. Occurrence can be prevented or ameliorated by initiating patients on dialysis with slower blood flow rates, slower dialysate flow rates, and shorter treatments.