Nutrient Requirements General Principles
Energy
Ģ Total daily energy expenditure (TEE) is composed of resting energy expenditure (normally ~70% of TEE), the thermic effect of food (normally ~10% of TEE), and energy expenditure of physical activity (normally ~20% of TEE).
Ģ Use of predictive equations can provide a reasonable estimate of daily energy requirements that should be modified based on the factors that affect the patient's metabolic rate.
Ģ Malnutrition and hypocaloric feeding may decrease resting energy expenditure to 15%-20% below expected for actual body size, whereas metabolic stressors, such as inflammatory diseases or trauma, often increase energy requirements by ~30%-50%.
Ģ The Harris-Benedict equation provides a reasonable estimate of resting energy expenditure (in kilocalories [kcal] per day) in healthy adults. It takes into account the effects of body size and lean tissue mass (which are influenced by gender and age) on energy requirements and can be used to estimate total daily energy needs in hospitalized patients (where W is the weight in kilograms, H the height in centimeters, and A is the age in years).1
Ņ Men = 66 + (13.7 ? W) + (5 ? H) - (6.8 ? A) Ņ Women = 665 + (9.6 ? W) + (1.8 ? H) - (4.7 ? A)
Ģ Energy requirements per kilogram of body weight are inversely related to body mass index (BMI) (Table 2-1). The lower range within each category should be considered in insulin-resistant, critically ill patients unless they are depleted in body fat.
TABLE 2-1
ESTIMATED ENERGY REQUIREMENTS FOR HOSPITALIZED PATIENTS BASED ON BODY MASS INDEX


Note: These values are recommended for critically ill patients and all obese patients; add 20% of total calories in estimating energy requirements in non-critically ill patients.
Ģ Ideal body weight can be estimated based on height
Ņ For men: 106 + 6 lb for each inch over 5 ft
Ņ For women, 100 + 5 lb for each inch over 5 ft
Protein
Ģ Protein intake of 0.8 g/kg/d meets the requirements of 97% of the adult population.
Ģ Protein requirements are affected by several factors, including the amount of nonprotein calories provided, overall energy requirements, protein quality, baseline nutritional status, and the presence of inflammation and metabolic stressors (Table 2-2).
TABLE 2-2
RECOMMENDED DAILY PROTEIN INTAKE
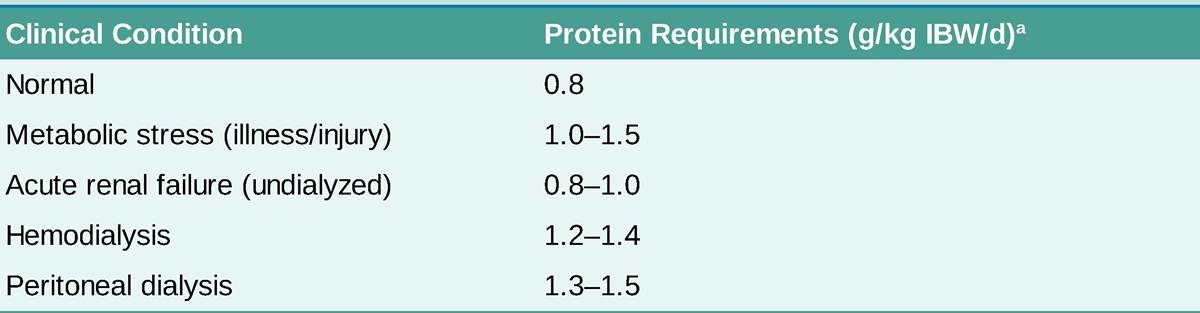
IBW, ideal body weight.
aAdditional protein intake may be needed to compensate for excess protein loss in specific patient populations such as those with burn injury, open wounds, and protein-losing enteropathy or nephropathy. Lower protein intake may be necessary in patients with chronic renal insufficiency who are not treated by dialysis and certain patients with hepatic encephalopathy.
Ģ Inadequate amounts of any essential amino acid results in inefficient utilization.
Ģ Illness increases the efflux of amino acids from skeletal muscle; however, increasing protein intake to >1.2 g/kg/d of prehospitalization body weight in critically ill patients may not reduce the loss of lean body mass.2
Essential Fatty Acids
Ģ Humans lack the desaturase enzyme needed to produce the ω-3 and ω-6 fatty acids. Therefore, linoleic acid should constitute at least 2% and linolenic acid at least 0.5% of the daily caloric intake to prevent deficiency.
Ģ The plasma pattern of increased triene-to-tetraene ratio (>0.4) can be used to detect essential fatty acid deficiency.
Carbohydrate
Certain tissues, such as bone marrow, erythrocytes, leukocytes, renal medulla, eye tissues, and peripheral nerves, cannot metabolize fatty acids and require glucose (~40 g/d) as a fuel. Endogenous protein and glycerol from lipid stores can undergo gluconeogenesis to supply glucose-requiring organs.
Major Minerals
Major minerals such as sodium, potassium, and chloride are important for ionic equilibrium, water balance, and normal cell function.
Micronutrients (Trace Elements and Vitamins)
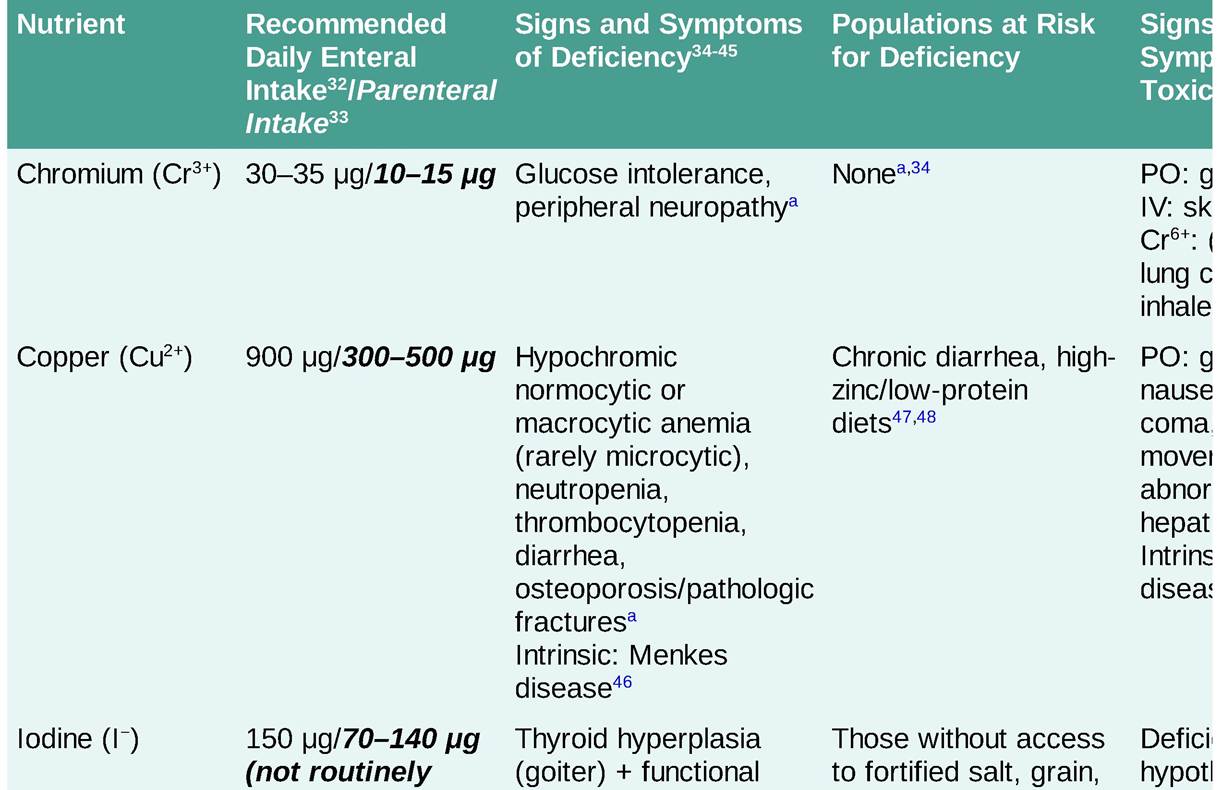
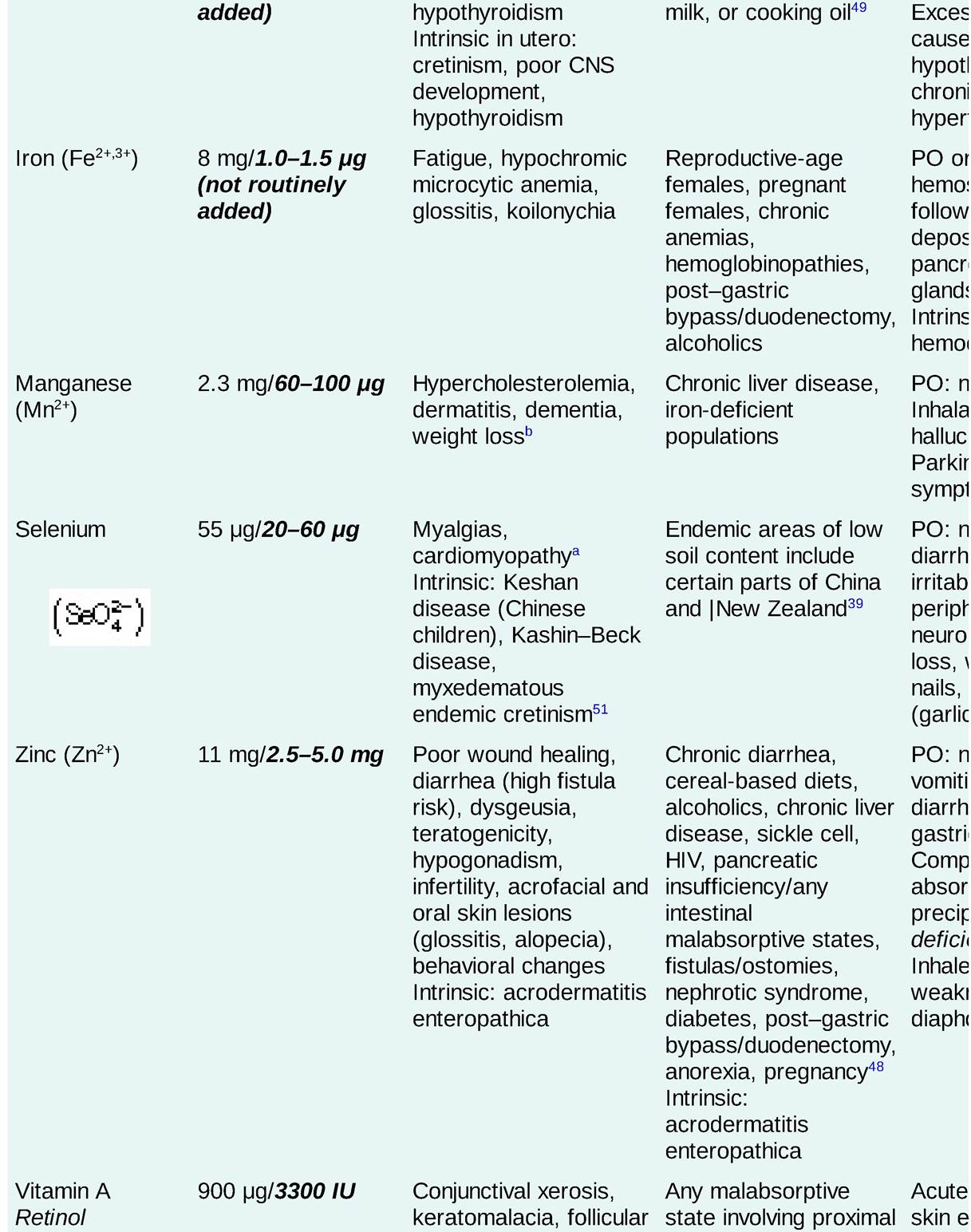
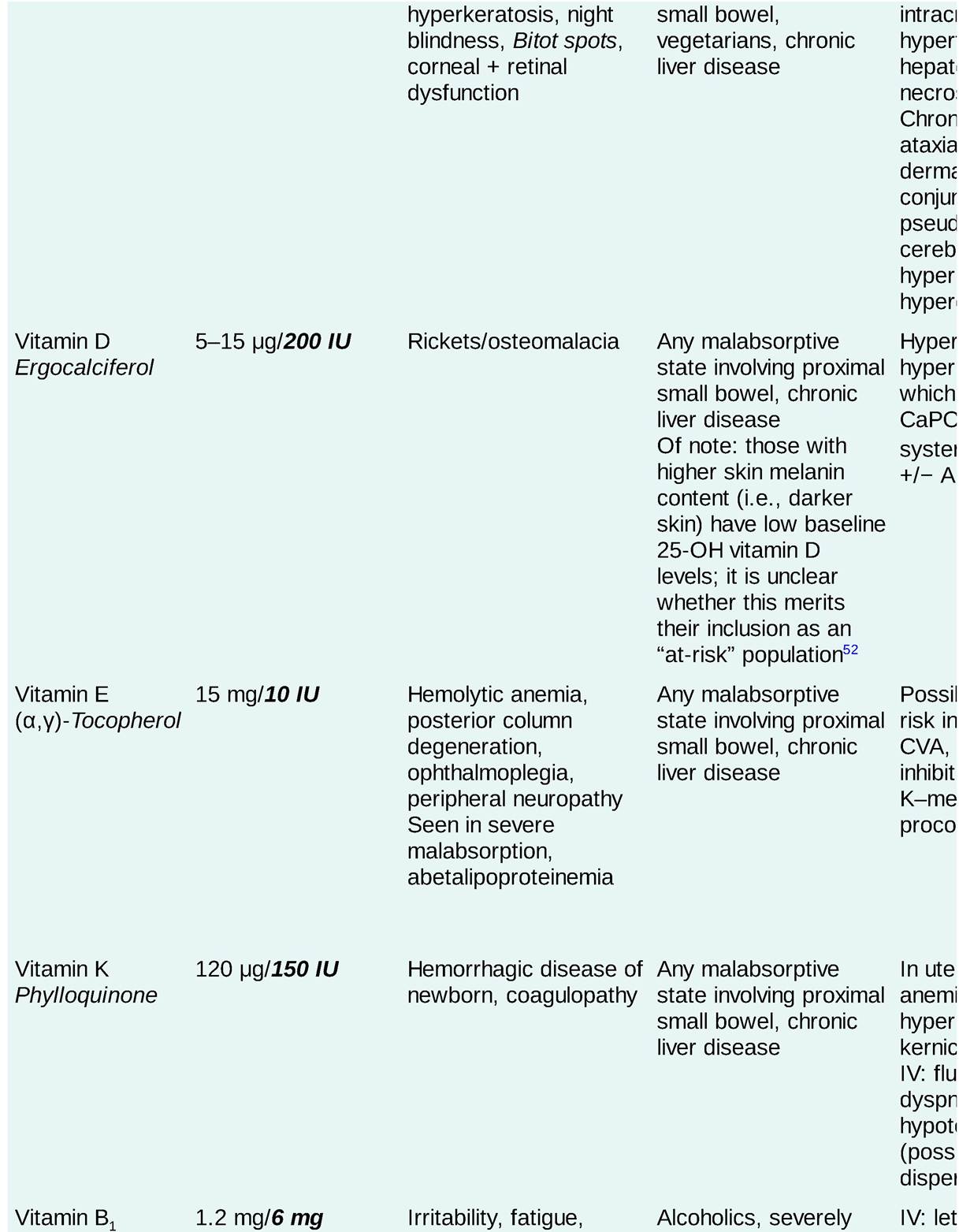
Trace elements and vitamins are essential constituents of enzyme complexes. The recommended dietary intake for trace elements, fat-soluble vitamins, and water-soluble vitamins is set at two standard deviations above the estimated mean as to meet the needs of 97% of the healthy population.
See Table 2-3 for specifics regarding the assessment of micronutrient nutritional states as well as signs and symptoms of micronutrient deficiency and toxicity.
TABLE 2-3
TRACE MINERALS, FAT-SOLUBLE VITAMINS, AND WATER-SOLUBLE VITAMINS: RECOMMENDED DAILY INTAKE, DEFICIENCY, AT-RISK POPULATIONS, TOXICITY, AND STATUS EVALUATION
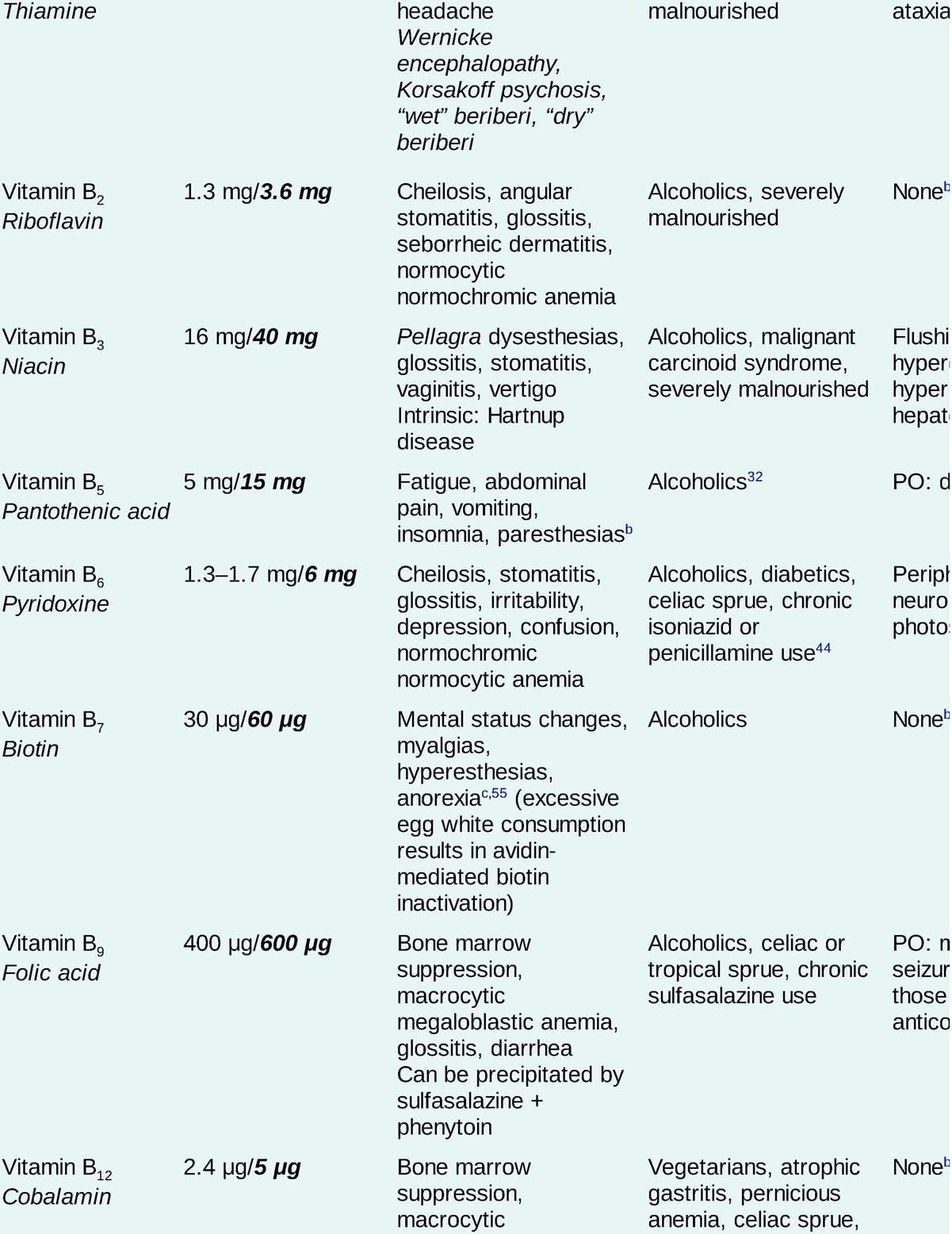
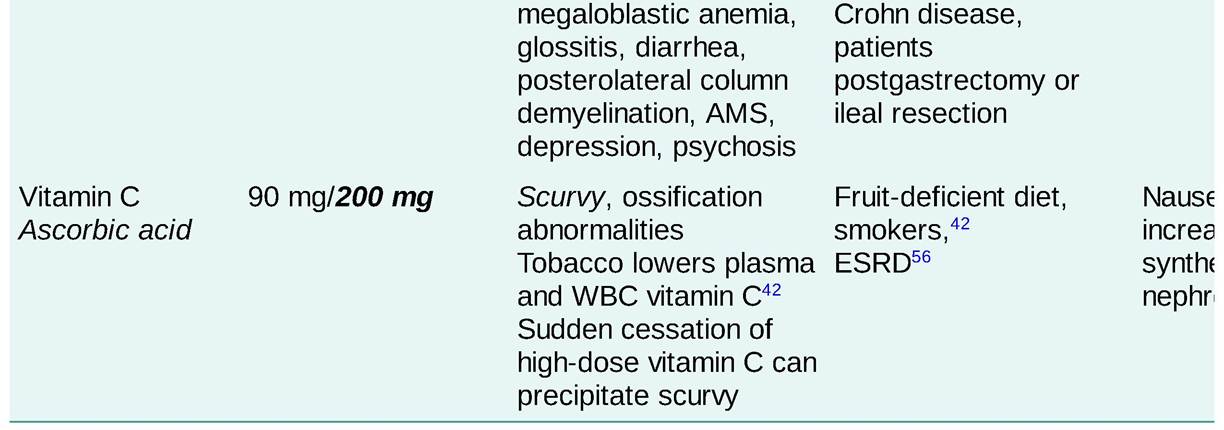
AKI, acute kidney injury; AMS, altered mental status; CNS, central nervous system; CVA, cerebrovascular accident; ESRD, endŁstage renal disease; IOM, Institute of Medicine; GI, gastrointestinal; HDL, high-density lipoprotein (cholesterol); RBC, red blood cell; TIBC, total iron bonding capacity; TPN, total parenteral nutrition; TSH, thyroid-stimulating hormone; WBC, white blood cell. Subscript: b, blood; c, calculated; p, plasma; s, serum; u, urine.
aOnly reported in patients on long-term TPN.
bNever demonstrated in humans.
cOnly able to induce under experimental conditions and/or only been able to induce in animals.
SPECIAL CONSIDERATIONS
Ģ Both the amount and location of prior gut resection influence nutrient needs.
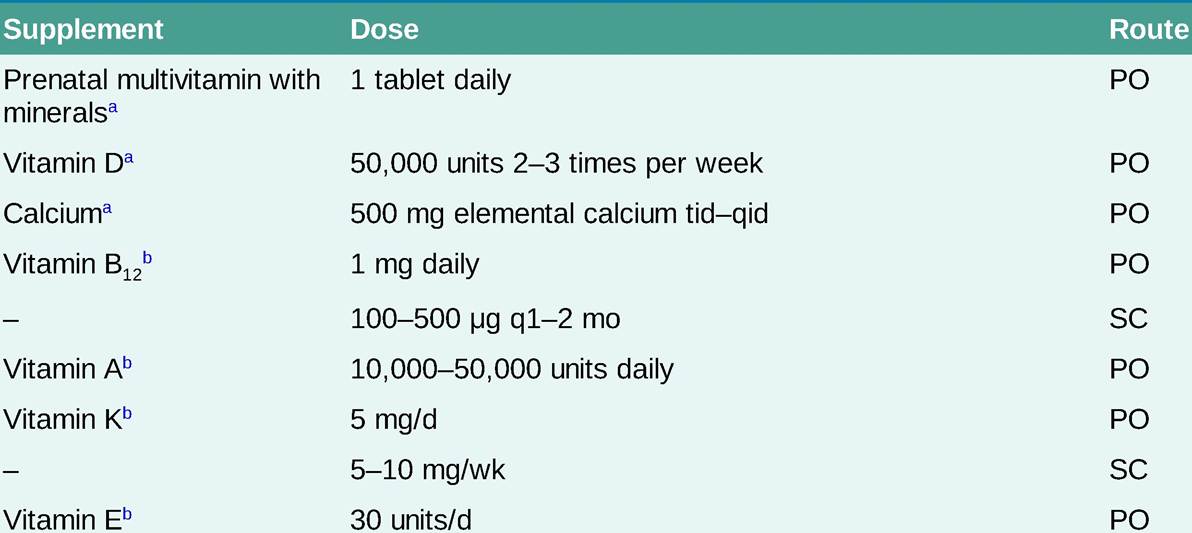
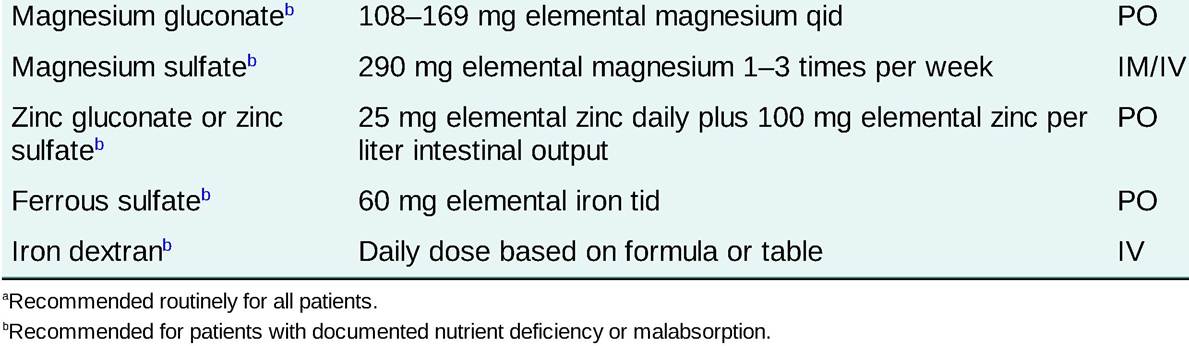
Patients with a reduced length of functional small bowel may require additional vitamins and minerals if they are not receiving parenteral nutrition. Table 2-4 provides guidelines for supplementation in these patients.TABLE 2-4
GUIDELINES FOR VITAMIN AND MINERAL SUPPLEMENTATION IN PATIENTS WITH SEVERE MALABSORPTION
Ģ Ileal inflammation, resection, inflammatory bowel disease (IBD), and bypass (ileojejunal bypass) can cause B12 deficiency and bile salt loss. Diarrhea in this setting may be improved with oral cholestyramine.
Ģ Proximal gut resection (stomach or duodenum) via partial gastrectomy, Billroth I and II, duodenal switch/biliopancreatic diversion, Roux-en-Y gastric bypass, pancreaticoduodenectomy (Whipple), and sleeve gastrectomy may impair absorption of divalent cations such as iron, calcium, and copper. Copper deficiency is extremely common in post-gastric bypass patients who do not receive routine supplementation.3
Ģ Patients with excessive gastrointestinal (GI) tract losses require additional fluids and electrolytes. An assessment of fluid losses due to diarrhea, ostomy output, and fistula volume should be made to help determine fluid requirements. Intestinal mineral losses may be calculated by multiplying the volume of fluid loss by the fluid electrolyte concentration (Table 2-5).
TABLE 2-5
| ELECTROLYTE CONCENTRATIONS IN GASTROINTESTINAL FLUIDS | ||||
| Location | Na (mEq/L) | K (mEq/L) | Cl (mEq/L) | HCO3 (mEq/L) |
| Stomach | 65 | 10 | 100 | - |
| Bile | 150 | 4 | 100 | 35 |
| Pancreas | 150 | 7 | 80 | 75 |
| Duodenum | 90 | 15 | 90 | 15 |
| Mid-small bowel | 140 | 6 | 100 | 20 |
| Terminal ileum | 140 | 8 | 60 | 70 |
| Rectum | 40 | 90 | 15 | 30 |
Ģ Hyperammonemic encephalopathy is an uncommon but serious complication of Roux-en-Y gastric bypass with an estimated mortality rate of 50%.4 Laboratory hallmarks include elevated ammonia, elevated plasma glutamate, hypoalbuminemia, nutritional and essential amino acid deficiencies, and low zinc.5 It does not appear to resolve with replacement of trace elements. Some reports suggest improvement with total parental nutrition after several months; however, data remain limited.6