Preoperative Cardiac Evaluation
GENERAL PRINCIPLES
Perioperative cardiac complications are generally defined as cardiac death, MIs (both ST and non-ST elevation), CHF, and clinically significant rhythm disturbances.
DIAGNOSIS
Clinical Presentation
HISTORY
Patient factors and comorbid conditions that affect perioperative cardiac risk include the following:
• Clinical risk factors for coronary artery disease (CAD)
• Preexisting, stable CAD
• Unstable coronary syndromes
• Recent MI (defined as >7 but 70 years identified in several studies as a significant risk factor but not uniformly accepted as independent.11,12
PHYSICAL EXAMINATION
Specific attention should be paid to the following:
• Vital signs, in particular elevated BP. Systolic blood pressure (SBP) 110 mm Hg) is controversial. Though postposing elective surgery to allow adequate BP control in this setting seems reasonable, how long to wait after treatment implementation to proceed remains unclear. Evidence of de compensated CHF (elevated jugular venous pressure, rales, S3, edema).
• Murmurs suggestive of significant valvular lesions. According to the 2014 American Heart Association (AHA)ZAmerican College of Cardiology (ACC) Guideline for the Management of Patients with Valvular Heart Disease, the risk of noncardiac surgery is increased in all patients with significant valvular heart disease, although symptomatic aortic stenosis (AS) is thought to carry the greatest risk. The estimated rate of cardiac complications in patients with undiagnosed severe AS undergoing noncardiac surgery is 10%-30%. However, aortic valve replacement is also associated with considerable risk. Risk-benefit analysis appears to favor proceeding to intermediate-risk elective noncardiac surgery (see below) with appropriate intra- and postoperative hemodynamic monitoring (including intraoperative right heart catheter or transesophageal echocardiogram) as opposed to prophylactic aortic valve replacement in the context of asymptomatic severe disease.
The same recommendations (albeit with less supporting evidence) apply to asymptomatic severe mitral regurgitation, asymptomatic severe aortic regurgitation with normal ejection fraction, and asymptomatic severe mitral stenosis (assuming valve morphology is not amenable to percutaneous balloon mitral commissurotomy, which should otherwise be considered to optimize cardiac status prior to proceeding to surgery). Symptomatic severe valvular disease of any type should prompt preoperative cardiology consultation.Diagnostic Criteria
The 2014 ACCZAHA Guideline on Perioperative Cardiovascular Evaluation and Management of Patients Undergoing Noncardiac Surgery offers a stepwise approach to preoperative evaluation and risk stratification (Figure 1-1).
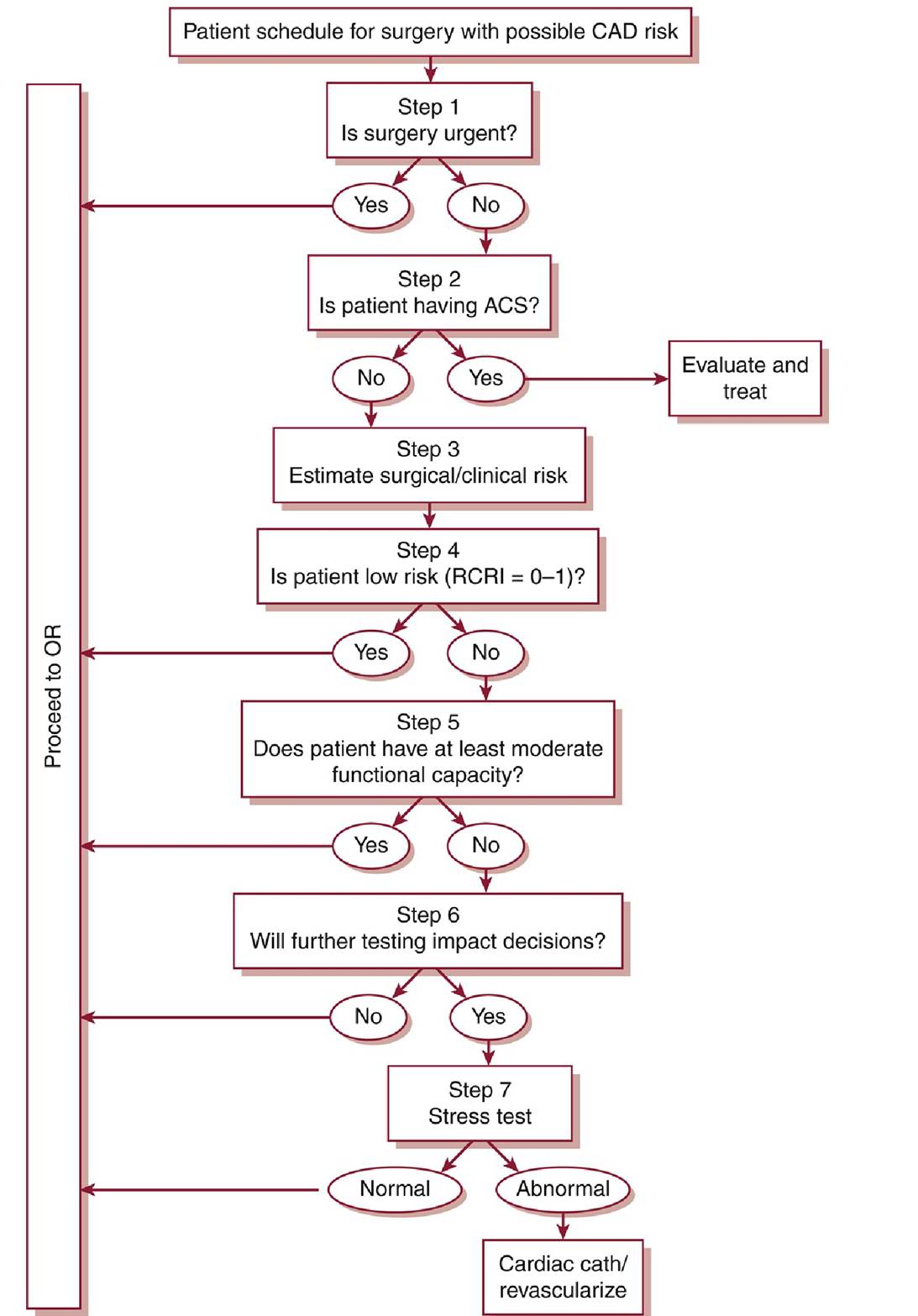
Figure 1-1 Cardiac evaluation algorithm for noncardiac surgery.ACS, acute coronary syndrome; CAD, coronary artery disease; OR, operating room; RCRI, Revised Cardiac Risk Index.(Modified from Fleisher LA, Fleischmann KE, Auerbach AD, et al. 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery: a report of the American College of CardiologyAmerican Heart Association Task Force on Practice Guidelines. Circulation. 2014;130(24):e278-e333.)
• Step 1: Establish the urgency of surgery. Many surgeries are unlikely to allow for a time-consuming evaluation.
• Step 2: Assess for active cardiac conditions (see “History,” above).
• Step 3: Determine the surgery-specific risk as follows:
î Low-risk surgeries (5% risk of adverse cardiac events).
• Step 4: Assess the patient's functional capacity.
Poor functional capacity (4 METs) include climbing one to two flights of stairs or walking a block at a brisk pace. Patients with a functional capacity of >4 METs without symptoms can proceed to surgery with relatively low risk.
• Step 5: Assess the patient's clinical risk factors.
î The number of risk factors combined with the surgery-specific risk (intermediate vs. vascular) determines further management. The following risk factors are adapted from the Revised Cardiac Risk Index (RCRI):16
■ Ischemic heart disease
■ History of TIA or CVA
■ History of CHF
■ Preoperative serum creatinine ≥2 mg/dL
■ Diabetes mellitus requiring insulin
î Patients with no clinical risk factors are at inherently low risk (more clinical risk factors are at high risk of adverse cardiac events, particularly when undergoing vascular surgery. In this population especially, stress testing may provide a better estimate of cardiovascular risk and may be considered if knowledge of this increased risk would change management.17 A positive stress test in a high-risk patient portends a substantially increased risk of a perioperative cardiac event, whereas a negative study suggests a lower risk than that predicted by clinical factors alone.11
Diagnostic Testing
• 12-Lead ECG. The value of a routine ECG is controversial. Per the 2014 ACC/AHA guidelines (level of evidence: B):
î ECG is “reasonable” in patients with known CAD, significant arrhythmia, peripheral arterial disease, cerebrovascular disease, or other significant structural heart disease prior to intermediaterisk surgery and above (class IIa);
î “May be considered” for asymptomatic patients without known coronary heart disease prior to intermediate- and high-risk surgery (class IIb);
î Is “not useful” for asymptomatic patients undergoing low-risk surgical procedures (class III).
• Resting echocardiogram. In general, the indications for preoperative echocardiographic evaluation are no different from those in the nonoperative setting. Murmurs found on physical examination suggestive of significant underlying valvular disease (see above) should be evaluated by echocardiogram. Assessment of left ventricular function should be considered when there is clinical concern for underlying undiagnosed CHF or if there is concern for deterioration since the last examination.
• Noninvasive stress testing. The decision to pursue a stress evaluation should be guided by an assessment of preoperative risk as detailed above. For further details on stress testing, see Chapter 4, Ischemic Heart Disease.
SPECIAL CONSIDERATIONS
• Patients with drug-eluting coronary stents: See “Perioperative Anticoagulation and Antithrombotic Management.”
• Multiple studies have reported a correlation between delayed repair of hip fracture and increased morbidity and mortality.18,19 For urgent surgical procedures (i.e., those that should be done within 48 hours of diagnosis), the value of additional testing is typically outweighed by the risk of worsened short- and long-term outcomes incurred with surgical delay. Unnecessary preoperative cardiac testing may be an independent risk factor for postoperative complications in hip fracture patients.20 In such cases, it is advisable to optimize the patient's medical status and modifiable risk factors and then proceed to the operating room.
TREATMENT
Medications
• β-Blockers
° Multiple studies have provided support for perioperative β-blockade in patients with or at risk for CAD undergoing noncardiac surgeries. The most pronounced benefit has been observed in high-risk patients undergoing vascular surgery where β-blocker dose was titrated to heart rate control.17,21 However, a subsequent analysis has called into question the role of dose titration.22 Although reduction in perioperative cardiac events has been observed consistently, it warrants mentioning that few data support the effectiveness of perioperative β-blockade in reducing mortality.
î According to the 2014 ACC/AHA guidelines:
■ In patients with three or more RCRI risk factors (see above) or evidence of myocardial ischemia on preoperative stress testing, starting preoperative β-blockade is reasonable (level of evidence: B).
■ β-Blockade should not be started on the day of surgery, as it is at minimum ineffective level and may actually be harmful (level of evidence: B).
■ Patients already taking β-blockers should be continued on their medication (level of evidence: B).
• Statins
î Multiple trials have shown a decrease in perioperative cardiac events and/or mortality with statin use in patients undergoing vascular surgery. Moreover, a recent cohort study of statin therapy in patients undergoing intermediate-risk noncardiac, nonvascular surgery revealed a fivefold reduced risk of 30-day all-cause mortality along with a statistically significant reduction in the composite end point of 30-day all-cause mortality, atrial fibrillation (AF), and nonfatal MI.23
î Per the 2014 ACC/AHA guidelines:
■ Patients currently taking statins should be maintained on therapy (level of evidence: B).
■ Patients undergoing vascular surgery, and those with risk factors undergoing intermediate-risk surgery, may benefit from initiation of statin therapy perioperatively (level of evidence: B and C, respectively). Optimal dose, duration of therapy, and target low-density lipoprotein levels for perioperative risk reduction are unclear.
• Aspirin
For discussion, see “Perioperative Anticoagulation and Antithrombotic Management.”
Revascularization
• The best available data on preoperative revascularization come from the Coronary Artery Revascularization Prophylaxis (CARP) trial, a prospective study of patients scheduled to undergo vascular surgery.24 Patients with proven significant CAD were randomized to revascularization versus no revascularization. There was no difference between the groups in the occurrence of MI or death at 30 days or in mortality with long-term follow-up. Patients with three or more clinical risk factors and extensive ischemia on stress testing were evaluated in a separate small study.25 High event rates were seen in both study arms, and no benefit was seen with revascularization. Taken together, these studies suggest that the risk of adverse cardiac events is not altered by attempts at preoperative revascularization, even in high-risk populations.
Patients with left main disease, who appeared to have benefited from preoperative revascularization in a subset analysis of the CARP trial data, are a notable possible expectation.26• Based on these cumulative results, a strategy of routinely pursuing coronary revascularization as a method of decreasing perioperative cardiac risk cannot be recommended. However, careful screening of patients is still essential to identify those high-risk subsets who may obtain a survival benefit from revascularization independent of their need for noncardiac surgery.
Monitoring/Follow-Up
Postoperative Infarction and Surveillance
• Most events will occur within 48-72 hours of surgery, with the majority in the first 24 hours.27 Most are also clinically silent.28 Although overall 30-day mortality has been linked to postoperative troponin elevation, the cause of death is not predictable, and no specific course of therapy may be offered.29
• The 2014 ACC/AHA guidelines offer the following30:
î Routine postoperative ECGs and troponins are not recommended.
î The benefit of troponin measurements and ECGs in high cardiac risk patients is uncertain.
î Symptomatic infarctions should be addressed according to standard therapy of acute coronary syndromes (see Chapter 4, Ischemic Heart Disease). The major caveat is that bleeding risk with anticoagulants must be carefully considered.