Respiratory Failure
GENERAL PRINCIPLES
Definitions
• Hypoxemic (type 1) respiratory failure: Occurs when normal gas exchange is seriously impaired, causing hypoxemia (arterial oxygen tension [PaO2] and hypoxemia.
Pathophysiology
• Hypoxemic respiratory failure (type 1): Usually is the result of the lung's reduced ability to deliver oxygen across the alveolocapillary membrane. The severity of gas exchange impairment is determined by calculating the P(A-a) O2 gradient (A-a gradient) using the alveolar gas equation:
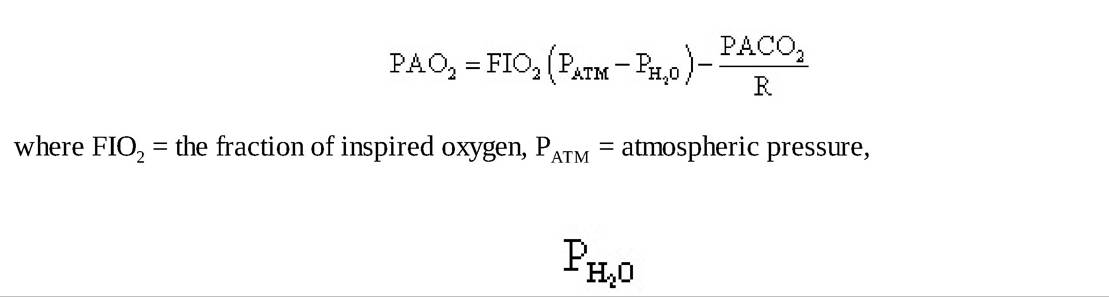
= water vapor pressure, and R = the respiratory quotient. Hypoxemia is caused by one of the following five mechanisms:
î Ventilation-perfusion (V/Q) mismatch: Occurs when perfusion does not compensate for a change in ventilation or vice versa (e.g., emphysema, pneumonia, pulmonary edema, pulmonary embolism). V/Q mismatch leads to an elevated A-a gradient. Administration of supplemental oxygen increases PaO2 (of note, supplemental oxygen paradoxically worsens V/Q mismatching in emphysema via reversing hypoxic vasoconstriction of pulmonary capillaries supplying poorly ventilated alveoli).
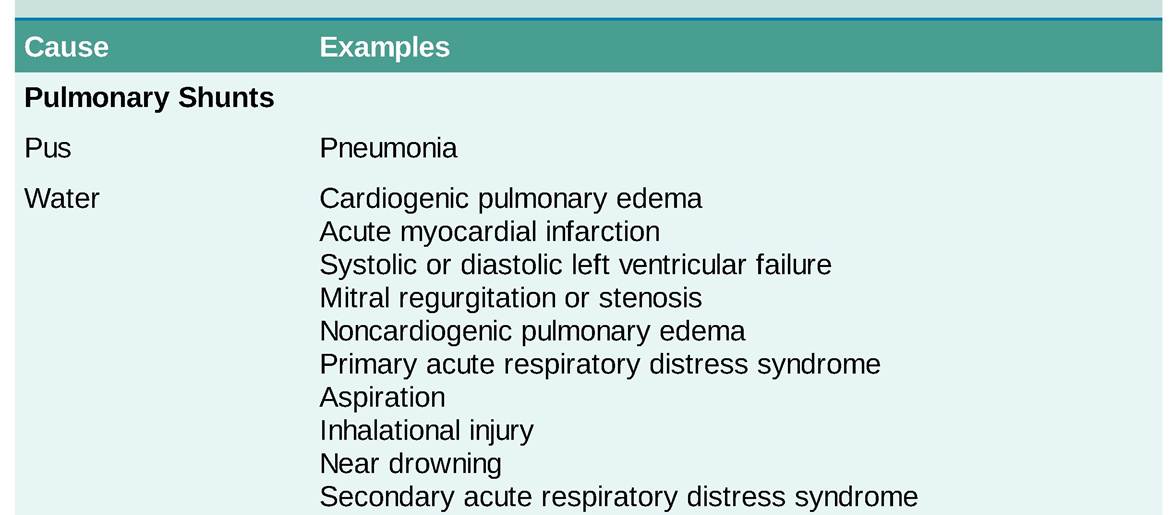
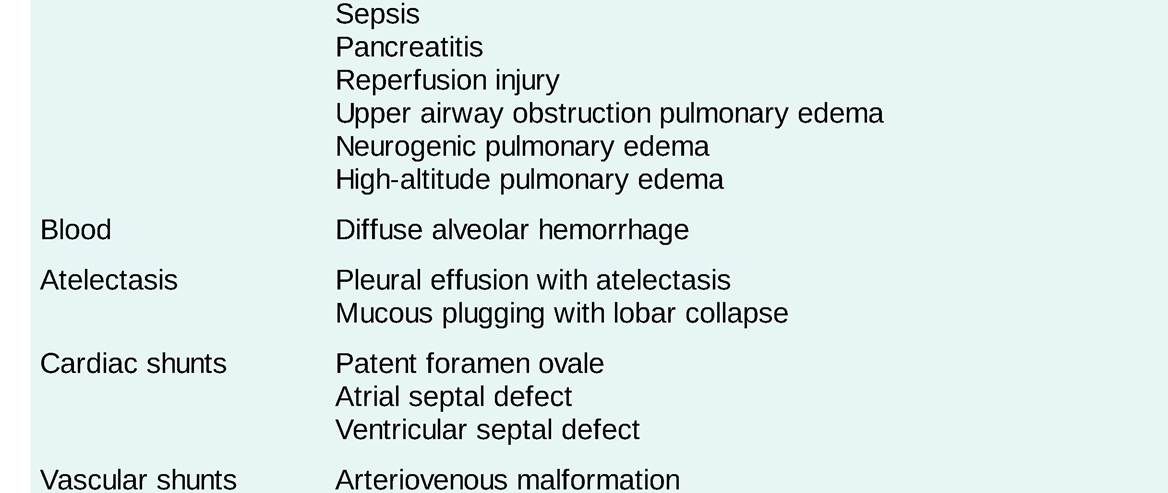
î Shunt: Occurs when mixed venous blood bypasses lung units and enters systemic arterial circulation without receiving oxygenation. Shunts can be congenital (e.g., intracardiac shunt) or acquired (atelectasis, hepatopulmonary syndrome). Shunt leads to an elevated A-a gradient. In pure shunt, administration of supplemental oxygen does not increase PaO2. See Table 8-1 for different causes of shunt.
TABLE 8-1
CAUSES OF SHUNT
î Diffusion abnormality: Occurs owing to abnormalities of the interstitium wherein the time it takes for gas equilibration is longer than the red blood cell transit time through the pulmonary capillaries (e.g., pulmonary fibrosis, pulmonary hypertension).
Diffusion abnormalities lead to an elevated A-a gradient. Administration of supplemental oxygen increases PaO2.î Hypoventilation: Occurs owing to a decrease in minute ventilation that results in an increase in PaCO2 (see the causes of hypercapnia under “Hypercapnic respiratory failure [type 2]”) and displacement of oxygen. The A-a gradient is normal. Primary treatment is directed at correcting the cause of hypoventilation. Administration of supplemental oxygen increases PaO2.
î Low inspired oxygen: Occurs owing to a low partial pressure of inspired oxygen (e.g., high-altitude travel). A-a gradient is normal. Administration of supplemental oxygen increases PaO2.
• Hypercapnic respiratory failure (type 2): Primarily occurs owing to ventilatory failure, resulting in an elevated PaCO2 >45 mm Hg:
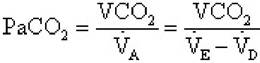
where CO2 = CO2 production, Va = alveolar ventilation, Ve = expired total ventilation, and Vd = dead space ventilation. The cause of hypercapnia is generally failure of one of the following components of the respiratory system:
î Disorders of the central nervous system: An impaired respiratory drive causes a decreased respiratory rate (“won't breathe”); e.g., opiate overdose, central apnea/hypoventilation, metabolic alkalosis, central nervous system (CNS) infection.
î Disorders of anterior horn cells, peripheral nervous system, or muscles: Neuromuscular failure or muscle weakness causes decreased tidal volume (“can't breathe”); e.g., Guillain-Barre syndrome, myasthenia gravis, amyotrophic lateral sclerosis, muscular dystrophies, myopathies.
î Disorders of the thoracic cavity: Anatomic abnormality causes decreased tidal volume; e.g., kyphoscoliosis, morbid obesity, pleural effusions, abdominal distention, diaphragmatic injury.
° Disorders of the airway or lung parenchyma: Lung pathology causes increased dead space; e.g., asthma, chronic obstructive pulmonary disease (COPD), severe ARDS.
î Hypermetabolic states can cause increased CO2 production and lead to hypercapnia; e.g., sepsis, seizure, thyrotoxicosis, serotonin syndrome.