I CANCER SCREENING AND PREVENTION ^226 ^241 ^306 ^386
Cancer is currently the second leading cause of death in women, after cardiovascular disease. Many treatments are available, but early detection significantly improves treatment outcomes and reduces mortality.
Because the obstetrician-gynecologist may be the only physician providing routine care, every obstetrician-gynecologist should be able to recommend immunizations against viruses known to cause cancer, routine cancer screenings for gynecologic cancers and nongynecologic cancers, and risk-reducing options for those women at high risk of cancer. The obstetrician-gynecologist should discuss both the benefits and limitations of screening tests with the patient. Evaluation of the risk of cancer includes assessment of high- risk behaviors and family history (see also the “Genetic Risk Assessment” section earlier in Part 3).The estimated number of women in the United States who would develop various malignancies and the number expected to die of these types of cancer in 2014 is shown in Table 3-5. Although breast cancer is the most frequent cancer in women, with approximately 232,670 new cases expected in 2014, the American Cancer Society reports that lung and bronchus cancer is the most common cause of cancer-related deaths in women in the United States, with approximately 72,330 deaths estimated in 2014.
According to currently available information, the most important factors in the development of cancer appear to be tobacco use, diet, infectious agents, alcohol consumption, and geographic location. The most well understood of these factors is tobacco use, which is thought to cause approximately 30% of cancer-related deaths in developed countries. Another major cause of cancer is the more complex factor of diet and nutrition, with 35% of cancer-related deaths associated with dietary practices. Recent research has identified clear associations between cancer risk and certain infectious agents, such as the association of some types of human papillomavirus with cervical, vulvar, vaginal, penile, anal, and
Table 3-5.
Estimated Number and Lifetime Risk of U.S. Women Who Will Develop or Die From Various Types of Cancer in 2014 ^Lifetime Lifetime
| Type of Cancer | Number of New Cases | Risk of Developing Cancer | Number of Deaths | Risk of Dying from Cancer |
| Breast | 232,670 | 1 in 8 | 40,000 | 1 in 36 |
| Lung and bronchus | 108,210 | 1 in 16 | 72,330 | 1 in 20 |
| Colorectal | 65,000 | 1 in 22 | 24,040 | 1 in 53 |
| Endometrial | 52,630 | 1 in 37 | 8,590 | 1 in 182 |
| Melanoma | 32,210 | 1 in 63 | 3,240 | 1 in 476 |
| Ovarian | 21,980 | 1 in 73 | 14,270 | 1 in 101 |
| Cervical | 12,360 | 1 in 152 | 4,020 | 1 in 435 |
Data from Siegel R, Ma J, Zou Z, Jemal A. Cancer Statistics, 2014. CA Cancer J Clin 2014;64:9-29 and American Cancer Society. Lifetime risk of developing or dying from cancer. Available at: http://www.cancer.org/cancer/cancerbasics/lifetime-probability-of-developing-or-dying- from-cancer. Retrieved January 14, 2014.
oropharyngeal cancer. In addition, striking associations exist between hepatitis viruses and liver cancer and between Epstein-Barr virus and nasopharyngeal cancer.
Current estimates suggest that at least 10% of cases of human cancer may be the result of infection, and it is expected that further research in this area will increase this estimate significantly. Most of the other proposed causes of cancer, including alcohol consumption, industrial by-products, food additives, and other constitutional and geographic factors, account for much smaller proportions of cancer-related deaths.Breast Cancer
Breast cancer is the most commonly diagnosed noncutaneous cancer in women in the United States, and the second leading cause of death from cancer in American women—second only to lung cancer (Table 3-5). The incidence of breast cancer increases with age. Breast cancer mortality can be effectively reduced through screening. Factors that increase the risk of breast cancer are outlined in Table 3-6, and the American College of Obstetricians and Gynecologists (the College) recommendations on individuals who warrant earlier or more frequent testing are available at www.acog.org/ About_ACOG/ACOG_Departments/Annual_Womens_Health_Care/High- Risk_Factors.
Table 3-6. Factors That Increase the Relative Risk of Breast Cancer in Women
| Relative Risk | Factor |
| >4.0 | Female Age (65+ years vs 30 years) Early menarche (55 years) No full-term pregnancies Never breastfed a child Recent oral contraceptive use Recent and long-term use of estrogen and progestin Obesity (postmenopausal) |
| Other factors | Personal history of endometrial or ovarian cancer Alcohol consumption Height (tall) High socioeconomic status Ashkenazi Jewish heritage |
Modified with permission from Hulka BS, Moorman PG. Breast cancer: hormones and other risk factors. Maturitas 2001;38:103-13; discussion 113-6. Copyright 2001, with permission from Elsevier.
Screening
Breast cancer screening has traditionally included three elements: 1) breast imaging (primarily mammography), 2) clinical breast examination, and 3) patient self-screening (breast self-examination or breast self-awareness).
The College continues to endorse inclusion of all three strategies in breast cancer screening.Mammography
At present, mammography is the recommended screening method in most women to detect subclinical or occult breast cancer, the stage least likely to have spread to regional lymph nodes and beyond. Based on the incidence of breast cancer, the sojourn time for breast cancer growth, and the potential reduction in breast cancer mortality, the College recommends that women aged 40 years and older be offered screening mammography annually. Women should be educated on the predictive value of screening mammography and the potential for false-positive results and false-negative results. Women should be informed of the potential for additional imaging or biopsies that may be recommended based on screening results.
Digital mammography detects some cases of cancer that are not identified by film mammography, but overall detection is similar for many women. However, for women younger than 50 years or women who have dense breast tissue, overall detection is somewhat higher with digital mammography. Digital mammography may detect cases of breast carcinoma that are obscured or “hidden” by dense breast tissue or detect the low contrast of the tumor in comparison with the surrounding breast tissue. Dense breast tissue can mask tumors by lying directly above and below a tumor in a two-dimensional view. Image processing of digital data allows the degree of contrast in the image to be manipulated so that contrast can be increased in the dense areas of the breast with the lowest contrast.
The American College of Radiology’s Breast Imaging Reporting and Data System (also known as BI-RADS) classifies abnormalities identified by mammography with a standardized reporting system (see Bibliography). Mammography results are classified as Categories 0-6 based on likelihood of malignancy. A Category 3 result indicates a 0-2% chance of malignancy.
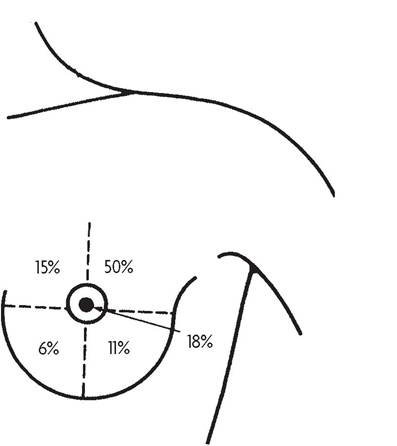
Fig.
3-2. Relative location of malignant lesions of the breast. (Reprinted with permission from DiSaia PJ, Creasman WT. Clinical gynecologic oncology. 6th ed. St. Louis [MO]: Elsevier/Mosby; Copyright 2002.)A Category 5 classification is used for findings with an approximate 95% or higher chance of malignancy. Findings that fall between these two categories are designated Category 4. The American College of Radiology has recommended an optional division of Category 4 into three subgroups to provide more concrete evaluation for treatment and outcome studies. Obstetrician-gynecologists who provide mammography services should be in compliance with the Mammography Quality Standards Act and its regulations (see also the “Compliance With Government Regulations” section in Part 1).
Clinical Breast Examination
The clinical breast examination involves visual assessment of skin changes and palpation. Malignant lesions of the breast are more common in the upper outer quarter (Fig. 3-2). For women aged 20-39 years, clinical breast examinations are recommended every 1-3 years. Clinical breast examination should be performed annually for women aged 40 years and older (see also the “Well-Woman Annual Health Assessment” section earlier in Part 3).
Patient Self-Screening
Breast self-examination is the performance of an examination of the breasts in a consistent, systematic way by the individual on a regular basis, typically monthly. Currently, there is an evolution away from teaching breast self-examination toward educating patients about the concept of breast self-awareness, which is defined as women’s awareness of the normal appearance and feel of their breasts. Breast self-awareness should be encouraged and can include breast self-examination. Women who desire to perform self-examination as a part of this breast self-awareness strategy may be instructed in the appropriate technique, although emphasis is not on examination techniques. Women should report any changes in their breasts to their health care providers.
Enhanced Screening
Women who are estimated to have a lifetime risk of breast cancer of 20% or greater, based on risk models that rely largely on family history (such as BRCAPRO, BODACEA, or Claus), but who are either untested or test negative for BRCA gene mutations, can be offered enhanced screening. For women who test positive for BRCA1 and BRCA2 mutations, enhanced screening should be recommended and risk-reduction methods discussed. Enhanced screening for these women includes twice-yearly clinical breast examinations, annual mammography, annual breast magnetic resonance imaging, and instruction in breast self-examination.
Other Imaging Techniques
Mammography has been the primary screening test for early breast cancer for more than five decades, but conventional mammography imaging continues to have limitations in sensitivity and specificity. Alternative breast imaging modalities that have been developed to improve cancer detection include ultrasonography, magnetic resonance imaging (MRI), and threedimensional digital breast tomosynthesis. These imaging tests may be indicated for women at increased risk of developing breast cancer, such as those with a BRCA1 or BRCA2 mutation, a strong family history of breast cancer or ovarian cancer, or prior chest radiation therapy. Women with dense breasts have a modestly increased risk of breast cancer and experience reduced sensitivity of mammography to detect breast cancer. However, current published evidence does not demonstrate meaningful outcome benefits (eg, reduction in breast cancer mortality) with supplemental tests (eg, ultrasonography and magnetic resonance imaging) to screening mammography or with alternative screening modalities (eg, breast tomosynthesis) in women with dense breasts who do not have additional risk factors. Thus, the American College of Obstetricians and Gynecologists does not recommend routine use of alternative or adjunctive tests in these cases. However, it recommends that health care providers comply with state laws that may require disclosure to women of their breast density as recorded in a mammogram report.
Ultrasonography is an established adjunct to mammography in the imaging evaluation. It is useful in evaluating inconclusive mammographic findings, in evaluating young patients and other women with dense breast tissue and other risk factors for breast cancer, in guiding tissue core-needle biopsy and other biopsy techniques, and in differentiating a cyst from a solid mass. It is not recommended as a screening modality for women at average risk of developing breast cancer. Ultrasonography may be an option for additional screening in women at high risk who are candidates for MRI screening but cannot receive MRI because of gadolinium contrast allergy, claustrophobia, or other barriers.
A three-dimensional modality used for breast cancer screening is MRI. Studies that use MRI for breast cancer screening indicate greater sensitivity but less specificity than mammography for detection of breast cancer in high-risk women. The American Cancer Society recommends annual screening using MRI in addition to mammography beginning at age 30 years for women at high risk of breast cancer (greater than 20-25% lifetime risk).
Digital breast tomosynthesis is another three-dimensional imaging technology that involves acquiring images of a stationary compressed breast at multiple angles during a short scan. The individual images are reconstructed into a series of thin high-resolution slices that can be displayed individually or in a dynamic cine mode. Digital breast tomosynthesis offers the potential to overcome one of the primary limitations of mammography, which is the inability to image overlapping dense normal breast tissue. This common clinical finding can reduce the accuracy of conventional mammography and digital mammography in distinguishing benign and malignant lesions. Digital breast tomosynthesis creates multiple projections that are imaged across a range of viewing angles to produce a series of section images. This procedure results in a reduction in the amount of superimposed breast tissue in each tomosynthesis section with presumed improved sensitivity for small tumors compared with mammography. Clinical data suggest that digital mammography with tomosynthesis produces a better image, improved accuracy, and lower recall rates compared with digital mammography alone. Further study will be necessary to confirm whether digital mammography with tomosynthesis is a cost-effective approach that is capable of replacing digital mammography alone as the first-line screening modality of choice for breast cancer screening.
Diagnostic Mammography
Mammography may be used as either a screening device or an adjunct in the diagnosis of a palpable mass. A palpable mass, in the presence of normal findings on mammography, requires further evaluation. Malignant lesions of the breast are more common in the upper outer quarter (Fig. 3-2). Normal diagnostic mammography alone is not always sufficient to rule out malignancy in a patient with a palpable breast mass. Ultrasonography may be useful to define a cystic lesion. If a cyst is aspirated and the fluid is clear (transparent and not bloody), there is no need for cytologic evaluation. If the cyst does not disappear after aspiration or recurs within 6 weeks, surgical follow-up should be considered. In adult women, a solid, dominant, persistent mass requires tissue diagnosis by core-needle biopsy or other biopsy techniques. Physical examination, imaging, and cytologic evaluations all contribute information but are not definitive (see also the “Cancer Diagnosis and Management” section in Part 4).
Risk Assessment and Reduction
The clinician should be knowledgeable regarding the indications and options for reducing the incidence of breast cancer, including prophylactic mastectomy and chemoprevention. A key factor to be considered is the woman’s risk of breast cancer. It is important that clinicians take a thorough history to assess the risk adequately. Researchers from the National Cancer Institute and the National Surgical Adjuvant Breast and Bowel Project have developed a computer-based tool to allow clinicians to project a woman’s individualized estimate of breast cancer risk. The Breast Cancer Risk Assessment Tool is a computer program that a woman and her health care provider can use to estimate her chances of developing breast cancer based on several established risk factors. The program is available at no charge in PC-compatible and Macintosh computer formats or online (see Resources).
Consideration should be given to tamoxifen or raloxifene chemopreventive therapy for women at high risk of developing breast cancer. Individualized risk assessment should be performed to determine whether a patient is a candidate for breast cancer risk reduction by chemoprevention unless she has ductal carcinoma in situ or lobular carcinoma in situ, in which case the benefit of chemoprevention already has been documented.
Cervical Cancer
The American Cancer Society estimates that there are more than 12,000 new cases of cervical cancer in the United States each year, with more than 4,000 deaths from the disease (Table 3-5). Estimates suggest that 50% of the women in whom cervical cancer is diagnosed never had cervical cytology testing, and another 10% have not been screened within the 5 years before diagnosis. Thus, approximately 60% of diagnoses of cervical cancer are a result of inadequate screening. Although rates of cervical cancer are decreasing in women born in the United States with access to screening, women who are immigrants to the United States, those lacking a regular source of health care, and the uninsured are at especially high risk.
Cervical cancer screening should begin at age 21 years. Women younger than 21 years should not be screened regardless of the age of sexual initiation or the presence of other behavior-related risk factors. Women aged 21-29 years should be tested with cervical cytology alone, and screening should be performed every 3 years. Co-testing with cytology and human papillomavirus (HPV) testing should not be performed in women younger than 30 years. For women aged 30-65 years, co-testing every 5 years is preferred, and screening with cytology alone every 3 years is acceptable. Annual screening should not be performed in women at average risk. Women who have received the HPV vaccine should be screened according to the same guidelines as women who have not been vaccinated.
Screening should be discontinued after age 65 years in women with evidence of adequate negative prior screening results and no history of cervical intraepithelial neoplasia (CIN) 2 or higher. Adequate negative prior screening results are defined as three consecutive negative cytology results or two consecutive negative co-test results within the previous 10 years, with the most recent test performed within the past 5 years. Women with a history of CIN 2, CIN 3, or adenocarcinoma in situ should continue to undergo routine age-based screening for 20 years after the initial posttreatment surveillance period, even if it requires that screening continue past age 65 years. In women who have had a total hysterectomy for benign indications and no history of CIN 2 or higher, routine cytology screening and HPV testing should be discontinued and not restarted for any reason. Women who have a history of cervical cancer, have human immunodeficiency virus (HIV) infection, are immunocompromised, or were exposed to diethylstilbestrol in utero may require more frequent cervical cytology screening and should not follow routine screening guidelines (see also the “Abnormal Cervical Cytology” section in Part 4).
Liquid-based and conventional methods of collecting samples for cervical cancer screening are acceptable. A cellular sample from the endocervical canal obtained with an endocervical brush and a scraping of the portio, to include the entire transformation zone, provides a reliable sample for cervical cancer screening. An endocervical brush should be used to obtain the endocervical cell sampling because it is more reliable in terms of identifying CIN, providing adequate cytology specimens, and limiting falsenegative test results than other tools for collection.
Certain measures can be taken to help ensure an adequate sample is obtained. Cells should be collected before the bimanual examination. Care should be taken to avoid contaminating the sample with lubricant. Ideally, the entire portio of the cervix should be visible when the sample is obtained. If a conventional Pap test is being done, the specimen should be transferred and fixed as quickly as possible in an effort to reduce air-drying artifact. Routine swabbing of the discharge from the cervix may result in cytologic samples of scant cellularity.
When conventional Pap tests are performed, a single slide (combining the endocervical sample and ectocervical sample) or two separate slides can be used. The most important consideration is rapid fixation. If liquidbased preparations are used, rapid immersion in liquid media is equally important.
Endometrial Cancer
Endometrial cancer is the most common gynecologic malignancy. The American Cancer Society estimates that there are more than 52,000 new cases diagnosed in the United States each year (Table 3-5). The most common cause is an excess of endogenous or exogenous estrogen unopposed by progestin that leads to endometrial hyperplasia followed by cancer. This cause allows for prevention and early detection of the most common and most indolent form of endometrial cancer (type I or estrogen dependent). Type I endometrial cancer typically has a good prognosis. The more lethal variety of endometrial cancer, type II, accounts for approximately 10% of cases. There is no clear epidemiologic profile for type II endometrial cancer. Modifiable risk factors for type II endometrial cancer include obesity, cigarette smoking, postmenopausal unopposed estrogen therapy, and high cumulative doses of tamoxifen. Carcinosarcoma of the endometrium is the most aggressive form of endometrial cancer.
Routine screening of asymptomatic women for endometrial cancer and its precursors is not cost-effective. Obtaining a family history may alert the gynecologist to women at increased risk of genetically linked cancers, such as Lynch syndrome (also known as hereditary nonpolyposis colorectal cancer), in which young age at presentation of colon cancer is important. The most common manifestation of Lynch syndrome in women is endometrial cancer. Women with a history or evidence of abnormal vaginal bleeding are at increased risk of endometrial cancer and should be evaluated. It is important to identify women at risk in order to provide them with appropriate evaluation, prophylactic surgery, and counseling.
Ovarian Cancer
Ovarian cancer is the leading cause of death from gynecologic pelvic malignancies. More women die from ovarian cancer than from cervical cancer and endometrial cancer combined (Table 3-5). Currently, there are no techniques that have proved to be effective in the routine screening of asymptomatic low-risk women for ovarian cancer. The use of transvaginal ultrasonography and tumor markers (such as CA 125) as potential screening strategies has been evaluated. These methods, however, have proved to be ineffective for screening low-risk asymptomatic women because their sensitivity, specificity, positive predictive value, and negative predictive value all have been modest at best. It appears that the best way to detect early ovarian cancer is for the patient and her clinician to have a high index of suspicion for the diagnosis in the symptomatic woman. This strategy requires education of physicians and patients about the symptoms commonly associated with ovarian cancer. Factors that are most significantly associated with ovarian cancer, if they occur more than 12 days per month and for less than 1 year, are pelvic or abdominal pain, increase in abdominal size or bloating, and difficulty eating or feeling full.
Inherited susceptibility to ovarian cancer has the greatest effect of all ovarian cancer risk factors. Women with the highest risk of ovarian carcinoma are those with hereditary breast and ovarian cancer syndrome, followed by women with Lynch syndrome. Suggestive family histories of hereditary cancer risk include cancer occurring at young ages; cancer in first-degree relatives; cancer in multiple generations; bilateral, metachronous, or synchronous cancer in one individual; and clustering of cancer on one side of the family. Evaluating a patient’s risk of a hereditary cancer syndrome should be a routine part of obstetric and gynecologic practice. Initial screening should involve asking specific questions about personal and family history of breast cancer and ovarian cancer as well as cancer types associated with Lynch syndrome. A hereditary cancer risk assessment is conducted by a health care provider with expertise in cancer genetics and includes gathering of family history information, risk assessment, education, and counseling. This assessment may include genetic testing if desired, after appropriate counseling and consent is obtained. Genetic testing can clarify ovarian carcinoma risk as well as risk of cancer to other organs. More information on genetic risk assessment can be found in the “Genetic Risk Assessment” section earlier in Part 3.
Women with an increased risk of ovarian carcinoma secondary to hereditary breast and ovarian cancer syndrome or Lynch syndrome are at risk of cancer in other organs and qualify for more intensive surveillance or prevention measures. Women with hereditary breast and ovarian cancer syndrome should be offered surveillance for breast cancer with breast magnetic resonance imaging in addition to mammography and should be counseled about the option of prophylactic mastectomy. Women with Lynch syndrome should have annual colonoscopies with removal of any polyps. Ovarian cancer risk should not be addressed in isolation without consideration of other cancer risks.
Given the limitations of current ovarian cancer screening approaches, women at high risk of ovarian cancer (women with BRCA1 or BRCA2 mutations) should be offered risk-reducing salpingo-oophorectomy by age 40 years or after the conclusion of childbearing. Risk-reducing salpingo- oophorectomy for these women should include careful inspection of the peritoneal cavity, pelvic washings, removal of the fallopian tubes, and ligation of the ovarian vessels at the pelvic brim. If hysterectomy is not performed, care must be taken to completely remove the fallopian tubes to the level of the cornu. Complete, serial sectioning of the ovaries and fallopian tubes is necessary, with microscopic examination for occult cancer. Carriers of the BRCA1 and BRCA2 mutations who undergo salpingo-oophorectomy achieve an 80-90% ovarian cancer risk reduction, as well as an approximate 50-60% decrease in breast cancer risk if surgery is performed before menopause. There are no established guidelines for age of risk-reducing surgery in women with Lynch syndrome mutations. In women with Lynch syndrome, the average age of ovarian cancer diagnosis is 42 years and the average age of endometrial cancer diagnosis is 50 years. Thus, it is also reasonable to consider prophylactic surgery in women aged 35-40 years with Lynch syndrome if childbearing is no longer desired.
Colon Cancer
Colon cancer causes nearly as many deaths among women as all gynecologic pelvic malignancies combined (Table 3-5). In most cases, it is preceded by adenomatous polyps. The College recommends colorectal cancer screening with colonoscopy every 10 years beginning at age 50 years for average-risk women and at age 45 years for African American women. The College supports stopping routine screening at age 75 years. An earlier starting age for screening is recommended in African American women because of increased incidence and earlier age of onset of colorectal cancer in this population. The College’s recommendations on individuals who warrant earlier or more frequent testing are available at www.acog.org/About_ACOG/ ACOG_Departments/Annual_Womens_Health_Care/High-Risk_Factors.
The advantages and limitations of other appropriate colorectal cancer screening methods also should be discussed so that women may choose to be tested by whichever method they are most likely to accept and complete. Annual testing of stool for blood using methods with high sensitivity can aid in early detection. High-sensitivity guaiac fecal occult blood testing and fecal immunochemical testing require two or three samples of stool collected by the patient at home and returned for analysis. A single stool sample for fecal occult blood testing or fecal immunochemical testing obtained by digital rectal examination is not adequate for the detection of colorectal cancer. Other acceptable screening methods include flexible sigmoidoscopy every 5 years, computed tomography colonography every 5 years, and fecal DNA testing (interval undetermined). However, the U.S. Preventive Services Task Force currently considers computed tomography colonography and fecal DNA testing to be evolving technologies with insufficient evidence of benefits or risks to make a recommendation. In addition, there currently is no fecal DNA test approved by the U.S. Food and Drug Administration. Abnormalities found with any screening method other than colonoscopy necessitate referral for diagnostic colonoscopy.
Lung Cancer
Lung cancer is the leading cause of death from malignancy for women, estimated to account for 72,330 deaths—surpassing breast cancer—in 2014. Available screening techniques are not cost-effective and have not been shown to reduce mortality from lung cancer in the general population. Accordingly, routine lung cancer screening is not recommended for women at average risk. However, the National Cancer Institute recommends consideration of lung cancer screening with low-dose helical computed tomography for patients aged 55-74 years who have at least a 30-pack- year smoking history and who currently smoke or have quit within the past 15 years. The U.S. Preventive Services Task Force has issued similar guidance that extends the age range for screening to 80 years. The only effective way to reduce mortality is to promote smoking cessation. Health care providers can make a major contribution to the long-term health of women who smoke by identifying all women who smoke and counseling them to stop (see also the “Substance Use and Abuse” section later in Part 3). A smoking-cessation plan—coupled with the use of pharmacotherapy aids when indicated—as well as proper follow-up care can help women quit smoking and avoid relapse. Legislative and voluntary measures to reduce the risk of secondary exposure to smoke also are important current efforts to reduce the incidence of lung cancer. In June 2009, the Family Smoking Prevention and Tobacco Control Act was passed. This Act provides the U.S. Food and Drug Administration with some power to regulate the tobacco industry, including a ban on most flavored cigarettes and more stringent requirements for labeling.
Bibliography
ACR BI-RADSβ-mammography: assessment categories. In: ACR breast imaging reporting and data system, breast imaging atlas. 5th ed. Reston (VA): American College of Radiology; 2014. p. 135-8.
Breast cancer screening. Practice Bulletin No. 122. American College of Obstetricians and Gynecologists. Obstet Gynecol 2011;118:372-82. [PubMed] [Obstetrics & Gynecology]
Centers for Disease Control and Prevention. Cervical cancer. Available at: http:// www.cdc.gov/cancer/cervical. Retrieved July 26, 2013.
Chemoprevention of breast cancer: recommendations and rationale. U.S. Preventive Services Task Force. Ann Intern Med 2002;137:56-8. [PubMed] [Full Text]
DiSaia PJ, Creasman WT. Clinical gynecologic oncology. 6th ed. St. Louis (MO): Elsevier/Mosby; 2002.
Digital breast tomosynthesis. Technology Assessment in Obstetrics and Gynecology No. 9. American College of Obstetricians and Gynecologists. Obstet Gynecol 2013; 121:1415-7. [PubMed] [Obstetrics & Gynecology]
Elective and risk-reducing salpingo-oophorectomy. ACOG Practice Bulletin No. 89. American College of Obstetricians and Gynecologists. Obstet Gynecol 2008; 111:231-41. [PubMed] [Obstetrics & Gynecology]
Freeman HP, Wingrove BK. Excess cervical cancer mortality: a marker for low access to health care in poor communities. NIH Pub. No. 05-5282. Rockville (MD): National Cancer Institute, Center to Reduce Cancer Health Disparities; 2005. Available at: http://crchd.cancer.gov/attachments/excess-cervcanmort.pdf. Retrieved July 26, 2013.
Hereditary breast and ovarian cancer syndrome. ACOG Practice Bulletin No. 103. American College of Obstetricians and Gynecologists and Society of Gynecologic Oncologists. Obstet Gynecol 2009;113:957-66. [PubMed] [Obstetrics & Gynecology] Hulka BS, Moorman PG. Breast cancer: hormones and other risk factors. Maturitas 2001;38:103-13; discussion 113-6. [PubMed] [Full Text]
Induced abortion and breast cancer risk. ACOG Committee Opinion No. 434. American College of Obstetricians and Gynecologists. Obstet Gynecol 2009; 113:1417-8. [PubMed] [Obstetrics & Gynecology]
Levin B, Lieberman DA, McFarland B, Andrews KS, Brooks D, Bond J, et al. Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guideline from the American Cancer Society, the U.S. Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. Gastroenterology 2008;134:1570-95. [PubMed]
Lifetime risk of developing or dying from cancer. Available at: http://www.cancer. org/cancer/cancerbasics/lifetime-probability-of-developing-or-dying-from-cancer. Retrieved January 14, 2014.
Management of endometrial cancer. ACOG Practice Bulletin No. 65. American College of Obstetricians and Gynecologists. Obstet Gynecol 2005;106:413-25. [PubMed] [Obstetrics & Gynecology]
Moyer VA. Screening for lung cancer: U.S. Preventive Services Task Force recommendation statement. U.S. Preventive Services Task Force. Ann Intern Med 2014;160:330-8. [PubMed] [Full Text]
National Cancer Institute. Lung cancer screening (PDQ®). Bethesda (MD): NCI; 2013. Available at: http://www.cancer.gov/cancertopics/pdq/screening/lung/ HealthProfessional. Retrieved September 26, 2013.
Saslow D, Boetes C, Burke W, Harms S, Leach MO, Lehman CD, et al. American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. American Cancer Society Breast Cancer Advisory Group [published erratum appears in CA Cancer J Clin 2007;57:185]. CA Cancer J Clin 2007;57:75-89. [PubMed]
Schiffman M, Wentzensen N. From human papillomavirus to cervical cancer. Obstet Gynecol 2010;116:177-85. [PubMed] [Obstetrics & Gynecology]
Schiller JS, Lucas JW, Ward BW, Peregoy JA. Summary health statistics for U.S. adults: National Health Interview Survey, 2010. Vital Health Stat 10 2012;(252):1- 207. [PubMed]
Screening for cervical cancer. Practice Bulletin No. 131. American College of Obstetricians and Gynecologists. Obstet Gynecol 2012;120:1222-38. [PubMed] [Obstetrics & Gynecology]
Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin 2014;64: 9-29. [PubMed]
Smith RA, Manassaram-Baptiste D, Brooks D, Cokkinides V, Doroshenk M, Saslow D, et al. Cancer screening in the United States, 2014: a review of current American Cancer Society guidelines and current issues in cancer screening. CA Cancer J Clin 2014;64:30-51. [PubMed]
Spence AR, Goggin P, Franco EL. Process of care failures in invasive cervical cancer: systematic review and meta-analysis. Prev Med 2007;45:93-106. [PubMed]
The role of the obstetrician-gynecologist in the early detection of epithelial ovarian cancer. Committee Opinion No. 477. American College of Obstetricians and Gynecologists. Obstet Gynecol 2011;117:742-6. [PubMed] [Obstetrics & Gynecology] Warner E, Messersmith H, Causer P, Eisen A, Shumak R, Plewes D. Systematic review: using magnetic resonance imaging to screen women at high risk for breast cancer. Ann Intern Med 2008;148:671-9. [PubMed] [Full Text]
Resources
Agrawal S, Bhupinderjit A, Bhutani MS, Boardman L, Nguyen C, Romero Y, et al. Colorectal cancer in African Americans. Committee of Minority Affairs and Cultural Diversity, American College of Gastroenterology [published erratum appears in Am J Gastroenterol 2005;100:1432]. Am J Gastroenterol 2005;100:515-23; discussion 514. [PubMed]
American College of Obstetricians and Gynecologists. Annual women's health care: high risk factors. Available at: http://www.acog.org/About_ACOG/ACOG_ Departments/Annual_Womens_Health_Care/High-Risk_Factors. Retrieved October 1, 2013.
American College of Obstetricians and Gynecologists. Cancer of the cervix. Patient Education Pamphlet AP163. Washington, DC: American College of Obstetricians and Gynecologists; 2013.
American College of Obstetricians and Gynecologists. Cancer of the ovary. Patient Education Pamphlet AP096. Washington, DC: American College of Obstetricians and Gynecologists; 2011.
American College of Obstetricians and Gynecologists. Cancer of the uterus. ACOG Patient Education Pamphlet AP097. Washington, DC: American College of Obstetricians and Gynecologists; 2008.
American College of Obstetricians and Gynecologists. Cervical cancer prevention in low-resources settings. College Statement of Policy 79. Washington, DC: American College of Obstetricians and Gynecologists; 2011.
American College of Obstetricians and Gynecologists. Cervical cancer screening. Patient Education Pamphlet AP085. Washington, DC: American College of Obstetricians and Gynecologists; 2013.
American College of Obstetricians and Gynecologists. It's time to quit smoking. Patient Education Pamphlet AP065. Washington, DC: American College of Obstetricians and Gynecologists; 2012.
American College of Obstetricians and Gynecologists. Reducing your risk of cancer. Patient Education Pamphlet AP007. Washington, DC: American College of Obstetricians and Gynecologists; 2013.
American College of Obstetricians and Gynecologists. Smoking and women's health. In: Special issues in women's health. Washington, DC: ACOG; 2005. p. 151-67.
Aromatase inhibitors in gynecologic practice. ACOG Committee Opinion No. 412. American College of Obstetricians and Gynecologists. Obstet Gynecol 2008; 112:405-7. [PubMed] [Obstetrics & Gynecology]
Genetics and Public Policy Center. Johns Hopkins University. Available at: http:// www.dnapolicy.org. Retrieved April 10, 2014.
Moyer VA. Screening for cervical cancer: U.S. Preventive Services Task Force recommendation statement. U.S. Preventive Services Task Force [published erratum appears in Ann Intern Med 2013;158:852]. Ann Intern Med 2012;156:880-91, W312. [PubMed] [Full Text]
National Cancer Institute. Breast cancer risk assessment tool. Available at: http:// www.cancer.gov/bcrisktool/. Retrieved September 20, 2013.
Sarfaty M. How to increase colorectal cancer screening rates in practice: a primary care clinician's evidence-based toolbox and guide. Atlanta (GA): American Cancer Society; 2008. Available at: http://www.cancer.org/acs/groups/content/documents/ document/acspc-024588.pdf. Retrieved July 26, 2013.
Saslow D, Solomon D, Lawson HW, Killackey M, Kulasingam SL, Cain J, et al. American Cancer Society, American Society for Colposcopy and Cervical Pathology, and American Society for Clinical Pathology screening guidelines for the prevention and early detection of cervical cancer. ACS-ASCCP-ASCP Cervical Cancer Guideline Committee. CA Cancer J Clin 2012;62:147-72. [PubMed] [Full Text]
Screening for breast cancer: U.S. Preventive Services Task Force recommendation statement. US Preventive Services Task Force [published errata appear in Ann Intern Med 2010;152:688. Ann Intern Med 2010;152:199-200]. Ann Intern Med 2009;151:716-26, W-236. [PubMed] [Full Text]
Screening for colorectal cancer: U.S. Preventive Services Task Force recommendation statement. U.S. Preventive Services Task Force. Ann Intern Med 2008;149:627-37. [PubMed] [Full Text]
Screening for ovarian cancer: recommendation statement. U.S. Preventive Services Task Force. Ann Fam Med 2004;2:260-2. [PubMed] [Full Text]