Chapter 22 Cardiovascular and Respiratory Disorders
This chapter deals primarily with APGO Educational Topic Areas:
TOPIC 17 MEDICAL AND SURGICAL COMPLICATIONS OF PREGNANCY
TOPIC 18 PREECLAMPSIA–ECLAMPSIA
Students should be able to identify how pregnancy affects the natural history of various cardiovascular and respiratory disorders and how a preexisting cardiovascular, hypertensive, and respiratory disorder affects maternal and fetal health.
They should be able to outline a basic approach to evaluation and management of cardiovascular, hypertensive, and respiratory disorders in pregnancy. The student should be familiar with preeclampsia, a disorder unique to pregnancy including pathophysiology, the spectrum of presentation, initial evaluation, and management and complications.Clinical Case
You are seeing a new patient in your office, and the nurse records her sitting blood pressure at 150/90 and on repeat, 154/98. The urine dip was negative except for 1+ protein. The patient complains of having a mild headache earlier that morning that resolved after eating breakfast. She also complains of increased swelling in her legs and feet and says that her blood pressure yesterday at the drug store was 150/100. She is 26 weeks’ pregnant. Do you begin antihypertensive therapy? Do you need any further evaluation?
Maternal medical or surgical conditions can complicate the course of a pregnancy and can be affected by pregnancy. Physicians providing obstetric care must have a thorough understanding of the effect of pregnancy on the natural course of a disorder, the effect of the disorder on a pregnancy, and the change in management of the pregnancy and disorder caused by their coincidence.
 HYPERTENSIVE DISORDERS
HYPERTENSIVE DISORDERS
Hypertensive disorders occur in approximately 12% to 22% of pregnancies and cause substantial perinatal morbidity and mortality of both mother and fetus.
Hypertensive disease is directly responsible for approximately 20% of maternal deaths in the United States. The exact cause of hypertension in pregnancy remains unknown. CLASSIFICATION
CLASSIFICATION
Various classifications of hypertensive disorders in pregnancy have been proposed. Box 22.1 presents a commonly used classification. Because hypertensive disorders in pregnancy represent a spectrum of disease, classification systems should be used as a guide only.
Chronic Hypertension
Chronic hypertension is defined as hypertension present before pregnancy or before the 20th week of gestation or that persists longer than the postpartum period (i.e., 12 weeks after delivery). Criteria for chronic hypertension in pregnancy are as follows:
• Mild: Systolic pressure of 140–159 mm Hg or diastolic pressure of 90–109 mm Hg
• Severe: Systolic pressure of 160 mm Hg or greater or diastolic pressure of 110 mm Hg or greater
A major risk with chronic hypertension is the development of preeclampsia or eclampsia later in the pregnancy, which is relatively common and difficult to diagnose. Up to 30% of women with chronic hypertension or gestational hypertension (see below) can develop preeclampsia. The acute onset of proteinuria and gestational hypertension in women with chronic hypertension is suggestive of superimposed preeclampsia.
BOX 22.1 Hypertensive Disorders in Pregnancy
Gestational hypertension
Preeclampsia
Mild
Severe
Eclampsia
Chronic hypertension preceding pregnancy (any cause)
Chronic hypertension (any cause) with superimposed gestational hypertension
Superimposed preeclampsia
Superimposed eclampsia
Gestational Hypertension
Hypertension that develops for the first time after 20 weeks of gestation in the absence of proteinuria is termed gestational hypertension. Gestational hypertension develops in 5% to 10% of pregnancies, with a 30% incidence in multiple gestations, regardless of parity.
Maternal morbidity is directly related to the severity and duration of hypertension.Almost 50% of women with gestational hypertension go on to develop preeclampsia, and approximately 10% of eclamptic seizures occur before overt proteinuria develops. It is often difficult to distinguish between chronic hypertension, preeclampsia, and gestational hypertension when a patient is seen in the second half of pregnancy with an elevated blood pressure level. In such cases, it is always wise to assume that the findings represent preeclampsia and evaluate accordingly. Gestational hypertension is reclassified as transient hypertension if blood pressure returns to normal before 12 weeks postpartum or chronic hypertension if it persists.
Preeclampsia
Preeclampsia is the development of hypertension with proteinuria after 20 weeks of gestation. Edema is typically present with the development of preeclampsia but is not useful as a diagnostic criterion insofar as some degree of edema is common in normal pregnancy. This condition can occur earlier in the presence of gestational trophoblastic disease (see Chapter 45). Risk factors for preeclampsia are summarized in Box 22.2. The criteria for the diagnosis of preeclampsia are:
• Blood pressure of ≥140 mm Hg systolic or ≥90 mm Hg diastolic that occurs after 20 weeks of gestation in a woman with previously normal blood pressure
BOX 22.2 Risk Factors for Preeclampsia
Nulliparity
Multifetal gestation
Maternal age 35 years or older
Preeclampsia in a previous pregnancy
Chronic hypertension
Pregestational diabetes
Vascular and connective tissue disorders
Nephropathy and other chronic renal disease
Antiphospholipid syndrome
Obesity
African American race
• Proteinuria, defined as urinary excretion of 0.3 g protein or higher in a 24-hour urine specimen
Severe preeclampsia is characterized by one or more of the following:
• Blood pressure ≥160 mm Hg systolic or ≥110 mm Hg diastolic on two occasions at least 6 hours apart while the patient is on bed rest
• Marked proteinuria (generally ≥5 g per 24-hour urine collection, or 3+ or more on two dipstick testing of random urine samples collected at least 4 hours apart)
• Oliguria effects: Plasma volume contraction or hemoconcentration may develop, with the risk of rapidonset hypovolemic shock, if hemorrhage occurs.
Plasma volume contraction is reflected in increased hematocrit values. Thrombocytopenia or disseminated intravascular coagulation may also develop from microangiopathic hemolytic anemia. Involvement of the liver may lead to hepatocellular dysfunction and further evolution of coagulopathy. Third spacing of fluid may be noted, because of increased blood pressure and decreased plasma oncotic pressure.• Renal effects: Decreased glomerular filtration rate (increasing serum creatinine) and proteinuria (urine protein levels >300 mg per 24 hours) develop secondary to vasospasm and atherosclerotic-like changes in the renal vessels (glomerular endotheliosis). Uric acid filtration is decreased; therefore, elevated maternal serum uric acid levels may be an indication of evolving disease.
• Neurologic effects: Hyperreflexia/hypersensitivity may develop. Other neurologic manifestations include head-ache, blurred vision, and scotomata. In severe cases, grand mal (eclamptic) seizures may develop.
• Pulmonary effects: Pulmonary edema may occur and can be related to decreased colloid oncotic pressure, pulmonary capillary leak, left heart failure, iatrogenic fluid overload, or a combination of these factors.
• Fetal effects: Decreased intermittent placental perfusion secondary to vasospasm is thought to be responsible for the increased incidence of IUGR (fetal effects if used in pregnancy.
Preeclampsia
The severity of the preeclampsia and the maturity of the fetus are the primary considerations in the management of preeclampsia. Care must be individualized, but there are well-accepted general guidelines.
Preeclampsia diagnosed at term and beyond is generally an indication for delivery. The mainstay of management for patients with mild preeclampsia who are being managed expectantly is rest and frequent monitoring of mother and fetus. Testing for suspected fetal growth restriction or oligohydramnios and twice-weekly NSTs, BPPs, or both is commonly employed and should be repeated as indicated, according to maternal condition.
Testing is recommended twice weekly for suspected IUGR or oligohydramnios. Ultrasound examination for fetal growth and amniotic fluid assessment is recommended every 3 weeks. Daily fetal movement assessment also may prove useful.Hospitalization is often initially recommended for women with new-onset preeclampsia. After maternal and fetal conditions are serially assessed, subsequent management may be continued in the hospital, at a day-care unit, or at home on the basis of the initial assessment.
Severe Preeclampsia
For the patient with worsening preterm preeclampsia or the patient who has severe preeclampsia, management is often best accomplished in a tertiary care setting. Daily laboratory tests and fetal surveillance may be indicated. Stabilization with magnesium sulfate, antihypertensive therapy (as indicated), monitoring for maternal and fetal well-being, and delivery by either induction or cesarean delivery are required.
For almost a century, magnesium sulfate has been used to prevent and to treat eclamptic convulsions. Other anticonvulsants, such as diazepam and phenytoin, are rarely used because they are not as efficacious as magnesium and because they have potential adverse effects on the fetus. Magnesium sulfate is administered by intramuscular or intravenous (IV) routes, although the latter is far more common. In 98% of cases, convulsions will be prevented. Therapeutic levels are 4 to 6 mg/dL, with toxic concentrations having predictable consequences (Table 22.2). Frequent evaluations of the patient’s patellar reflex and respirations are necessary to monitor for manifestations of rising serum magnesium concentrations. In addition, because magnesium sulfate is excreted solely from the kidney, careful attention for signs of magnesium toxicity is warranted in the setting of reduced urine output (1.0 mg/mL). In these situations, serum magnesium levels may be useful in adjusting the infusion rate and avoiding toxicity. Reversal of the effects of excessive magnesium concentrations is accomplished by the slow IV administration of 10% calcium gluconate, along with oxygen supplementation and cardiorespiratory support, if needed.

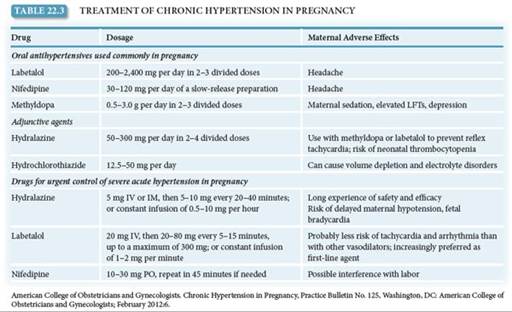
Antihypertensive therapy is initiated if, on repeated measurements, the systolic blood pressure is >160 mm Hg or diastolic blood pressure exceeds 105 to 110 mm Hg. Hydralazine is often the initial antihypertensive medication of choice, given in 5- to 10-mg increments IV until an acceptable blood pressure response is obtained. A 10- to 15-minute response time is usual. The goal of such therapy is to reduce the diastolic pressure to the 90- to 100-mm Hg range. Further reduction of the blood pressure may impair uterine blood flow to rates that are dangerous to the fetus. Labetalol is another agent used to manage severe hypertension (Table 22.3).
Once anticonvulsant and antihypertensive therapies are established in patients with severe preeclampsia or eclampsia, attention is directed toward delivery. Induction of labor is often attempted, although cesarean delivery may be needed either if induction is unsuccessful or not possible or if the maternal or fetal status is worsening. At delivery, blood loss must be closely monitored, because patients with preeclampsia or eclampsia have significantly reduced intravascular volumes and may not tolerate increased blood loss. After delivery, patients remain in the labor and delivery or antepartum high-risk area for 24 hours (longer if the clinical situation warrants) for close observation of their clinical progress and further administration of magnesium sulfate to prevent postpartum eclamptic seizures. Approximately 25% of eclamptic seizures occur before labor, 50% occur during labor, and 25% occur in the first 24 hours after delivery. Usually, the vasospastic process begins to reverse itself in the first 24 to 48 hours after delivery, as manifested by a brisk diuresis.
Eclampsia
The eclamptic seizure is life-threatening for the mother and fetus. Maternal risks include musculoskeletal injury (including biting the tongue), hypoxia, and aspiration. Maternal therapy consists of inserting a padded tongue blade, restraining gently as needed, providing oxygen, assuring maintenance of an adequate airway, and gaining IV access. Eclamptic seizures are usually self-limited, so medical therapy should be directed at the initiation of magnesium therapy (4–6 g slowly, IV) to prevent further seizures. If a patient receiving magnesium sulfate experiences a seizure, additional magnesium sulfate (usually 2 g slowly) can be given and a blood level obtained. Other anticonvulsant therapy with diazepam or similar drugs is generally not warranted.
Transient uterine hyperactivity for up to 15 minutes is associated with fetal heart rate changes, including bradycardia or compensatory tachycardia, decreased variability, and late decelerations. These are self-limited and are not dangerous to the fetus unless they continue for 20 minutes or more. Delivery during this time imposes unnecessary risk for mother and fetus and should be avoided. Arterial blood gases are often obtained, any metabolic disturbance should be corrected, and a Foley catheter should be placed to monitor urinary output. If the maternal blood pressure is high, if maternal urinary output is low, or if there is evidence of cardiac disturbance, consideration of a central venous catheter and, perhaps, continuous electrocardiogram monitoring is appropriate. Delivery is indicated once the mother is stabilized.
HELLP Syndrome
Patients with HELLP syndrome are often multiparous and have blood pressure recordings lower than those of many preeclamptic patients. Liver dysfunction may manifest as RUQ pain and is all too commonly misdiagnosed as gallbladder disease or indigestion. Major morbidity and mortality with unrecognized HELLP make accurate diagnosis imperative. The first symptoms are often vague, including nausea and emesis and a nonspecific viral-like syndrome. Treatment of these gravely ill patients is best done in a high-risk obstetric center and consists of cardiovascular stabilization, correction of coagulation abnormalities, and delivery. Platelet transfusion before or after delivery is indicated if the platelet count is of those with other cardiac conditions that traditionally have been less commonly seen in pregnancy. Because pregnancy is itself associated with an increase in cardiac output of 40%, the risks to mother and fetus are often profound for women with preexisting cardiac disease. Ideally, cardiac patients should have preconceptional care directed at maximizing cardiac function. They should also be counseled about the risks their particular heart disease poses in pregnancy.
Classification of Heart Diseases in Pregnancy
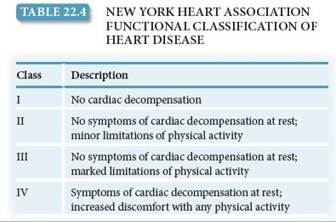
The classification of heart disease by the New York Heart Association is useful to evaluate all types of cardiac patients with respect to pregnancy (Table 22.4). It is a functional classification and is independent of the type of heart disease. Patients with septal defects, patent ductus arteriosus, and mild mitral and aortic valvular disorders often are in classes I or II and tend to do well throughout pregnancy. Primary pulmonary hypertension, uncorrected tetralogy of Fallot, Eisenmenger syndrome, Marfan syndrome with significant aortic root dilation, dilated cardiomyopathy, and certain other conditions are associated with a much worse prognosis (frequently death) through the course of pregnancy. For this reason, patients with such disorders are strongly advised not to become pregnant.
Management
General management of the pregnant cardiac patient consists of avoiding conditions that add additional stress to the workload of the heart beyond that already imposed by pregnancy, including prevention and/or correction of anemia, prompt recognition and treatment of any infections, a decrease in physical activity and strenuous work, and proper weight gain. Adequate rest is essential. For patients with class I or II heart disease, increased rest at home is advised; and in cases of higher class levels, hospitalization and treatment of cardiac failure may be required. Coordinated management between the obstetrician, cardiologist, and anesthesiologist is especially important for patients with significant cardiac dysfunction.
The fetuses of patients with functionally significant cardiac disease are at increased risk for low birth weight and prematurity. A patient with congenital heart disease is 1% to 5% more likely to have a fetus with congenital heart disease than is someone without this condition; antepartum fetal cardiac assessment using ultrasound is recommended.
The antepartum management of pregnant cardiac patients includes serial evaluation of maternal cardiac status as well as fetal well-being and growth. Anticoagulation, antibiotic prophylaxis for subacute bacterial endocarditis, invasive cardiac monitoring, and even surgical correction of certain cardiac lesions during pregnancy can all be accomplished if necessary. The intrapartum and postpartum management of pregnant cardiac patients includes consideration of the increased stress of delivery and postpartum physiologic adjustment. Labor in the lateral position to facilitate cardiac function is often desirable. Every attempt is made to facilitate vaginal delivery because of the increased cardiac stress of cesarean section. Because cardiac output increases by 40% to 50% during the second stage of labor, shortening this stage by the use of forceps or vacuum extractor is often advisable. Epidural anesthesia to reduce the stress of labor is also recommended, although fluid shifts induced by sympathetic nervous system blockade must be watched for. Even with patients who are stable at the time of delivery, cardiac output increases in the postpartum period because of the additional 500 mL added to the maternal blood volume as the uterus contracts. Indeed, most obstetric patients who die with cardiac disease do so following delivery.
Rheumatic Heart Disease
Rheumatic heart disease remains a common cardiac disease in pregnancy. As the severity of the associated valvular lesion increases, the risk of thromboembolic disease, subacute bacterial endocarditis, cardiac failure, and pulmonary edema increases. A high rate of fetal loss also occurs in women with rheumatic heart disease. Approximately 90% of these patients have mitral stenosis, whose associated mechanical obstruction worsens as cardiac output increases during pregnancy. Women with mitral stenosis associated with atrial fibrillation have an especially high risk of developing congestive heart failure.
Cardiac Arrhythmias
Maternal cardiac arrhythmias are occasionally encountered during pregnancy. Paroxysmal atrial tachycardia is the most commonly encountered maternal arrhythmia and is usually associated with overly strenuous exercise. Underlying cardiac disease such as mitral stenosis should be suspected when atrial fibrillation and flutter are encountered.
Peripartum Cardiomyopathy
Peripartum cardiomyopathy is an unusual but especially severe cardiac condition identified in the last month of pregnancy or the first 6 months following delivery. It is difficult to distinguish from other cardiomyopathies (e.g., myocarditis) except for its association with pregnancy. In many cases, no apparent cause can be determined. Treatment is generally unchanged from cardiac failure unassociated with pregnancy, except that the use of ACE inhibitors is avoided if the patient is pregnant. Management includes bed rest, digoxin, diuretics, and, in some cases, anticoagulation. The mortality rate is high and is related to cardiac size 6 to 12 months later. If cardiac size returns to normal, prognosis is improved, although it remains guarded. Sterilization counseling is warranted for patients with persistent cardiomyopathy.
RESPIRATORY DISORDERS
Asthma
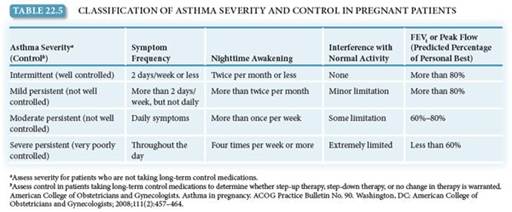
Asthma is a restrictive airway disease that is encountered in approximately 4% to 8% of pregnant patients. The effects of pregnancy on asthma are variable—in general, about one third of patients worsen, one third improve, and the remaining one third are unchanged. Women with mild or moderate asthma usually have excellent maternal and fetal outcomes (Table 22.5). However, suboptimal control of asthma during pregnancy may be associated with increased maternal or fetal risk. Decreased FEV1 (forced expiratory volume in the first second of expiration) is associated with increased risk of low birth weight and prematurity.
Pregnant patients with asthma, even those with mild or well-controlled disease, should be monitored with peak expiratory flow rate or FEV1 testing as well as by close symptom observation. Routine evaluation of pulmonary function in pregnant women with persistent asthma is recommended. Serial ultrasound examinations and antenatal fetal testing should be considered for women who have moderate or severe asthma during pregnancy beginning at 32 weeks of gestation or for women recovering from a severe asthma exacerbation.
Management
The ultimate goal of asthma therapy in pregnancy is maintaining adequate oxygenation of the fetus by preventing hypoxic episodes in the mother. Inhaled corticosteroid therapy, particularly budesonide, is the first-line controller treatment for persistent asthma during pregnancy. Inhaled albuterol is the recommended rescue therapy. In the stepcare therapeutic approach, the number and dosage of medications are increased with increasing asthma severity. Once control of symptoms is achieved, a “step-down” approach is usually implemented in the nonpregnant patient. In pregnant patients, it may be prudent to postpone a reduction in a therapy that is effectively controlling a patient’s asthma until after the birth. Patients should be instructed to identify and control or avoid factors, such as allergens and irritants, particularly tobacco smoke.
Management of a severely asthmatic pregnant patient is similar to that of a nonpregnant patient. Evaluation consists of measurement of pulmonary function and arterial blood gases. Treatment may include administration of supplemental oxygen, treatment with nebulized β-agonists, corticosteroids (oral or IV), or intubation. Women who are currently receiving or recently have taken systemic corticosteroids should receive IV administration of corticosteroids during labor and for 24 hours after delivery to prevent adrenal crisis.
INFLUENZA
Respiratory infection caused by influenza virus A (including the H1N1 strain) or B in pregnancy can be serious, with increased susceptibility to pneumonia and higher rates of hospitalization for pregnant women compared with nonpregnant women. In addition, pregnancy has been associated with higher mortality rates with serious influenza respiratory illness, including during the recent 2009 pandemic. Symptoms of influenza infection include dry cough, fever, and systemic symptoms such as myalgias. Diagnosis can be confirmed using rapid flu assays. Treatment includes supportive care and antiviral therapy. There is no firm evidence that influenza virus causes congenital malformations; risk to the fetus is primarily that associated with maternal hypoxia and systemic inflammatory effects of maternal infection (preterm labor and exposure to hyperthermia with high maternal fever).
Women who will be pregnant during the influenza season (October through May in the United States) should be vaccinated with a current (based on predictions of prevalent strains for the season in the community) influenza vaccine at any time during the pregnancy. There are no contraindications to the inactivated influenza vaccine in pregnancy and vaccination prevents clinical illness in 70% to 90% of adults. Chemoprophylaxis with antiviral therapy should also be offered to pregnant women who are in close contact with an infected person.
Clinical Follow-Up
This patient may have chronic hypertension or may be developing preeclampsia. Since she is a new patient, you obtain a careful history and perform a physical examination. She has no history of chronic hypertension and no other chronic medical disorders. Because of the risk of adverse outcome for mother and fetus if the diagnosis is preeclampsia, you plan to evaluate her further. You send her to Labor and Delivery for laboratory tests, maternal blood pressure monitoring, and fetal evaluation with ultrasonography and fetal heart rate monitoring.
thePoint Visit http://thepoint.lww.com/activate for an interactive USMLE-style question bank and more!