Chapter 44 Cell Biology and Principles of Cancer Therapy
Students should be able to understand the fundamentals of cell biology and relate them to the behavior of malignant cells and their response to chemotherapy, radiation, and other novel approaches to cancer treatment.
Clinical Case
A 60-year-old patient has just completed her ovarian cancer debulking surgery and returns for postoperative care and consultation regarding chemotherapy. She has questions regarding the side effects of the treatment.
Treatment of cancers involving the breast and genital organs may involve surgery, chemotherapy, radiation therapy, or hormone therapy, used alone or in combination. The specific treatment plan depends on the type of cancer, the stage of the cancer, and the characteristics of the individual patient. Individualizing treatment is an important aspect of cancer therapy.
 CELL CYCLE AND CANCER THERAPY
CELL CYCLE AND CANCER THERAPY
Knowledge of the cell cycle is important in understanding cancer therapies. The ideal cancer treatment would be a drug that targets only cancer cells with no effect on healthy tissues. In order to optimally target only cancerous tissue, it is imperative to understand not only how normal cells function but also how cancer cells differ from normal cells.
Many treatments are based on the fact that cancer cells are constantly dividing, making them more vulnerable to agents that interfere with cell division.
The cell cycle consists of four phases in addition to a resting state (Fig. 44.1). During the G1 phase (postmitotic phase), RNA and protein synthesis, cell growth, and DNA repair take place. Once these processes are complete, the cell enters the S phase (synthesis phase), during which the DNA is completely replicated. The G2 phase is a period of additional synthesis of RNA, protein, and specialized DNA.
Cell division occurs during the M phase (mitosis). After mitosis, cells can again enter the G1 phase, or can “drop out” of the cell cycle and enter a resting phase (G0). Cells in G0 do not engage in the synthetic activities characteristic of the cell cycle and are not vulnerable to therapies aimed at actively growing and dividing cells. The growth fraction is the proportion of cells in a tumor that are actively involved in cell division (i.e., not in the G0 phase). The growth fraction of tumors decreases as they enlarge, because vascular supply and oxygen levels are decreased. Surgical removal of tumor tissue (cytoreductive debulking surgery) can result in G0 cells reentering the cell cycle, thereby making them more vulnerable to chemotherapy and radiation therapy.The generation time is the length of the cell cycle, from one M phase to the next M phase. For a given cell type, the lengths of the S and M phases are relatively constant, whereas G2 and, especially, G1 vary. The variable length of G1 can be explained by cells entering the resting phase (G0) for a period and then reentering the cycle. The length of G1 has a profound effect on the cell’s susceptibility to treatment.
Chemotherapeutic agents and radiation kill cancer cells by first-order kinetics. This means that each dose kills a constant fraction of tumor cells, instead of a constant number. The resulting clinical implication is that several intermittent doses are more likely to be curative than a single large dose.
 CHEMOTHERAPY
CHEMOTHERAPY
Chemotherapeutic agents can be 1) cell cycle (phase) nonspecific, which means that they can kill in all phases of the cell cycle and are useful in tumors with a low growth index, or 2) cell cycle (phase) specific, which means that they kill in a specific phase of the cell cycle and are most useful in tumors that have a large proportion of actively dividing cells.
FIGURE 44.1 illustrates common drugs and their sites of action within the cell cycle.
FIGURE 44.1. Actions of antineoplastic agents within the cell cycle.
Several classes of antineoplastic drugs are available (Table 44.1). Alkylating agents and alkylating-like agents bind and cross-link DNA, interfering with DNA replication and, ultimately, with RNA transcription. Dividing cells, especially those in the late G1 and S phases, are most sensitive to the effects of these drugs; however, these drugs are considered phase nonspecific (i.e., they are effective in all phases of the cell cycle). The major side effect of the alkylating agents is myelosuppression. The alkylating-like agents behave similarly and include the platinum-based agents cisplatin and carboplatin.
Antitumor antibiotics inhibit DNA-directed RNA synthesis and are also involved in the formation of free radicals, causing strand breakage. They are phase nonspecific. Their general side effects are similar to those of the alkylating agents; however, each drug has its own toxicity.
Antimetabolites are structural analogues of normal molecules necessary for cell function. They competitively interfere with the enzymes involved with normal synthesis of nucleic acids and, therefore, are most active during the S phase of cell division. They may cause bone marrow suppression or gastrointestinal (GI) mucositis when given in a bolus.
Plant (vinca) alkaloids interfere with the M phase of cell division by preventing the assembly of microtubules. They may cause bone marrow suppression or an anaphylactoid reaction.
Topoisomerase inhibitors result in cell death by inhibiting topoisomerase I (TOPO-I), an enzyme required for DNA replication. In a normally replicating cell, TOPO-I induces reversible single-strand breaks in the DNA. TOPO-I inhibitors combine with the DNA and TOPO-I and prevent repair of the breaks in the single strand of DNA, resulting in cellular death.
ENDOCRINE THERAPY
Hormonal agents are frequently used in gynecologic cancer treatment because these cancers contain estrogen, progesterone, and other endocrine receptors. These therapies are not specifically aimed at killing cancer cells but control disease via biochemical pathways. They are commonly used along with other therapies.
alt=Image>
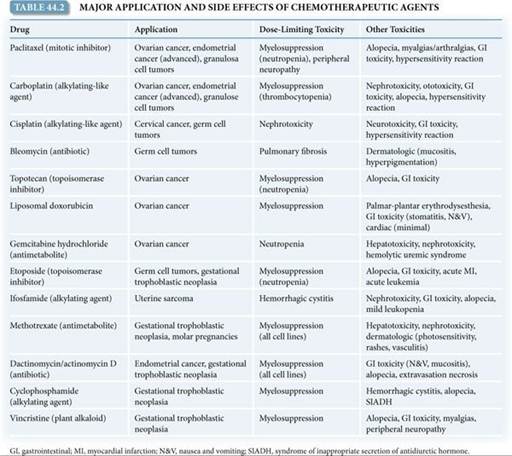
Toxicity of Chemotherapy
Antineoplastic drugs are toxic because they act on normal as well as cancer cells. Table 44.2 describes the major applications and side effects of antineoplastic agents. Rapidly dividing cell types of the erythroid, myeloid, and megakaryocytic lineages are most sensitive to damage by common neoplastic drugs. Anemia, granulocytopenia (neutropenia), and thrombocytopenia are predictable side effects. Patients with anemia will often experience incapacitating lethargy. Patients with neutropenia are at high risk for fatal sepsis, and those with sustained thrombocytopenia are at risk for spontaneous GI or acute intracranial hemorrhage. Prophylactic antibiotics are administered to patients with febrile neutropenia or in neutropenic patients to prevent serious infection. Platelet transfusions can be used to decrease the risk of hemorrhage.
Combination Chemotherapy
The use of single agents is limited by development of drug resistance and toxicity. Combination chemotherapy is used to counteract these limitations. Several strategies can be used to select drugs for combination chemotherapy. In sequential blockade, the drugs block sequential enzymes in a single biochemical pathway. In concurrent blockade, the drugs attack parallel biochemical pathways leading to the same end product. Complementary inhibition interferes with different steps in the synthesis of DNA, RNA, or protein.
The interactions between drugs used in combination are defined as synergistic (result in improved antitumor activity or decreased toxicity, compared with when each agent is used alone), additive (result in enhanced antitumor activity equal to the sum of the antitumor activities resulting from using the individual agents separately), or antagonistic (result in less antitumor activity than if each individual agent is used alone).
Drugs used in combinations should 1) be effective when used singly; 2) have different mechanisms of action; and 3) be additive or, preferably, synergistic in action.Chemotherapy Regimens
Chemotherapy is administered in various regimens. Adjuvant chemotherapy is usually a set course of combination chemotherapy that is given in a high dose to patients who have no evidence of residual cancer after radiotherapy or surgery. The purpose is to eliminate any residual cancer cells, typically with the intent to cure disease. Neoadjuvant chemotherapy aims to eradicate micrometastases or reduce inoperable disease to prepare patients for surgery and/or radiotherapy. Induction chemotherapy is usually a combination chemotherapy given in a high dose to cause a remission. Maintenance chemotherapy (consolidation chemotherapy) is a long-term and low-dose regimen that is given to a patient in remission to maintain the remission by inhibiting the growth of remaining cancer cells.
Endocrine therapy with selective estrogen receptor modulators (SERMs) acts in estrogen-sensitive breast tumors to block the interaction of estrogen with estrogen receptors (ERs). The therapeutic importance of cellular ERs has been well established in breast cancers. ER-positive tumors are responsive to endocrine therapy. Normally, estrogen enters cells and binds to ERs in the cytoplasm. The complex is translocated to the nucleus, where it binds to acceptor sites on chromosomes, resulting in activation of RNA and protein synthesis. SERMs act as competitive inhibitors of estrogen binding; the SERM–ER complex binds to chromosomes but does not activate cell metabolism. The subsequent decrease in cellular activity and cell division results in reduced tumor growth.
Additionally, SERMs are used to prevent cancer recurrence. The two SERMs most frequently prescribed in the United States are tamoxifen and raloxifene. Although relatively nontoxic, some SERMs increase the risk of endometrial cancer and uterine sarcomas as well as benign endometrial pathology.
Aromatase inhibitors (AIs), such as anastrozole and letrozole, which suppress intratumor and plasma estrogen levels, are being used in postmenopausal patients for the treatment of advanced breast cancer that has progressed beyond tamoxifen therapy. In addition, they are being used as an adjuvant therapy, often sequentially with tamoxifen, to prevent breast cancer recurrence. AIs have been associated with bone loss secondary to the induced hypoestrogenic state.
Progestational agents have been found to be useful in the treatment of early-stage endometrial cancer when surgery is either not feasible, unsafe, or not desired. Progestational therapy is also useful for some patients with recurrent disease. The most common progestational agents used are medroxyprogesterone and megestrol.
Research is ongoing to search for other hormonal agents effective for treatment or prevention of hormonally related neoplasms. Other agents that have demonstrated efficacy in cases of recurrent disease include goserelin (synthetic hormone) and arzoxifene (SERM).
RADIATION THERAPY
Ionizing radiation causes the production of free hydrogen ions and hydroxyl (•OH) radicals. With sufficient oxygen, hydrogen peroxide (H2O2) is formed, which disrupts the structure of DNA and, eventually, the cell’s ability to divide. As with chemotherapy, killing is by first-order kinetics. Because dividing cells are more sensitive to radiation damage and because not all cells in a given tumor are dividing at any one time, fractionated doses of radiation are more likely to be effective than a single dose. Providing multiple lower doses of radiation also reduces the deleterious effects on normal tissues.
The basis of fractionated dosage comes from the “four Rs” of radiobiology:
1. Repair of sublethal injury: When a dose is divided, the number of normal cells that survive is greater than if the dose were given at one time (higher total amounts of radiation can be tolerated in fractionated as opposed to single doses).
2. Repopulation: Reactivation of stem cells occurs when radiation is stopped; thus, regenerative capacity depends on the number of available stem cells.
3. Reoxygenation: Cells are more vulnerable to radiation damage with oxygen present; as tumor cells are killed, surviving tumor cells are brought into contact with capillaries, making them radiosensitive.
4. Redistribution in the cell cycle: Because tumor cells are in various phases of the cell cycle, fractionated doses make it more likely that a given cell is irradiated when it is most vulnerable.
The radiation absorbed dose (rad) has been used as a measure of the amount of energy absorbed per unit mass of tissue. A standard measure of absorbed dose is the Gray, which is defined as 1 J/kg; 1 Gray is equal to 100 rad. Radiation is delivered in two general ways: external irradiation (teletherapy) and local irradiation (brachytherapy). Teletherapy depends on the use of high-energy (>1 million eV) beams; it spares the skin and delivers less toxic radiation to the bone. Tolerance for external radiation depends on the vulnerability of surrounding normal tissues. Teletherapy is usually used to shrink tumors before localized radiation. Brachytherapy depends on the inverse square law: the dose of radiation at a given point is inversely proportional to the square of the distance from the radiation source. To put the radioactive material at the closest possible distance, brachytherapy uses encapsulated sources of ionizing radiation implanted directly into tissues (interstitial) or placed in natural body cavities (intracavitary). Intracavitary devices can be placed within the uterus, cervix, or vagina, and then loaded with radioactive sources in the form of either low-dose radiotherapy (cesium-137) or high-dose radiotherapy (iridium-192 and cobalt-60). This method protects health personnel from radiation exposure. A new method of treating early breast cancer involves high–dose rate brachytherapy inserted by a balloon catheter into the cavity created by lumpectomy. Interstitial implants use isotopes (iridium-192 and iodine-125) formulated as wires or seeds. These implants are usually temporary, but permanent seed implants are being investigated.
New strategies are being developed for radiation therapy. For example, intraoperative therapy is being used for previously irradiated patients with recurrent disease who would require unacceptably high dosages of external radiation.
Complications
Complications associated with radiation therapy can be acute or late (chronic). Acute reactions affect rapidly dividing tissues, such as epithelia (skin, GI mucosa, bone marrow, and reproductive cells). Manifestations are cessation of mitotic activity, cellular swelling, tissue edema, and tissue necrosis. Early problems associated with irradiation of gynecologic cancers include enteritis; acute cystitis; vulvitis; proctosigmoiditis; topical skin desquamation; and, occasionally, bone marrow depression. Chronic complications occur months to years after completion of radiation therapy. These include obliteration of small blood vessels or thickening of the vessel wall, fibrosis, and reductions in epithelial and parenchymal cell populations. Chronic proctitis, hemorrhagic cystitis, formation of ureterovaginal or vesicovaginal fistula, rectal or sigmoid stenosis, and bowel obstructions as well as GI fistulae may result.
NOVEL CHEMOTHERAPEUTIC AGENTS
The next horizon for cancer treatment is molecularly targeted agents, cancer vaccines, and gene therapy. Several drugs are currently available that target specific molecules or proteins in cancer cells. For example, trastuzumab is a DNA-derived monoclonal antibody to the human epidermal growth factor receptor 2 protein (HER-2). Treatment with trastuzumab is currently indicated in patients with metastatic breast cancer whose tumors overexpress HER-2. Some ovarian, cervical, and endometrial tumors express the HER-2/neu receptor; therefore, investigation is currently ongoing regarding the usefulness of this agent in gynecologic tumors. Additionally, bevacizumab is a monoclonal antibody designed to target the vascular endothelial growth factor protein and inhibit angiogenesis in tumors. It is currently under investigation for the possible treatment of a variety of tumors, including epithelial ovarian cancer.
Tumor vaccines are also currently being investigated for the treatment of ovarian cancer. The underlying principle behind these therapeutic vaccines is to inoculate the patient with a modified cancer cell line in an attempt to stimulate the patient’s immune system to recognize and eliminate the tumor. Inactivated virus strains have also been studied as a vector for the vaccines in hopes of creating higher immunogenicity. Currently, the response to this type of therapy has been modest, but studies are ongoing.
Because a large proportion of gynecologic cancers result from the loss of genetic function through DNA mutations, investigational therapies have also focused on genetic manipulation of the tumors, or gene therapy. For instance, because half of ovarian cancers exhibit deleterious mutations in the p53 gene, research has focused on delivering a normal p53 gene product to the tumor using a variety of viral vectors. The hope is that the wild-type gene product would then be expressed by the tumor, and the growth would then be inhibited. So far, response has been minimal, but investigation continues.
The potential benefits of these novel therapeutic concepts are manifold, whether considered as primary or adjunct therapy. Work in this area is in the experimental stage, but the goal of eliminating cancer cells with minimal toxicity remains the goal of cancer therapeutics.
Clinical Follow-Up
As the physician, you explain the toxic effects of chemotherapy to the patient including a change in her blood cell counts causing her increased risk of infection, changes in her kidney functioning, loss of hair, changes in hearing, and gastrointestinal symptoms as well as aches and pains. She is now prepared to undergo chemotherapy with a better understanding of what she might expect.
thePoint Visit http://thepoint.lww.com/activate for an interactive USMLE-style question bank and more!