Chapter 33 Disorders of the Breast
This chapter deals primarily with APGO Educational Topic Area:
TOPIC 40 DISORDERS OF THE BREAST
Students should be able to describe normal versus abnormal findings. They should outline a basic approach to patients with common breast complaints and breast cancer including evaluation and initial management.
Clinical Case
A 26-year-old patient presents with a 2- to 3-cm smooth, painless, freely movable mass in her left breast. She reports that the mass becomes somewhat tender but does not change during her menstrual cycle and has grown slowly over the past year. The patient initially found the mass during breast self-examination.
Diseases of the breast encompass a diverse spectrum of pathology, from benign breast disease to breast cancer. It is imperative that women’s health care providers understand the evaluation, treatment, and surveillance of breast-related complaints. Providers must ensure appropriate breast cancer screening for all patients, whether at high or low risk. In order to properly evaluate, treat, and follow breast-related complaints, a multidisciplinary approach is often necessary. Although referral to a specialist is sometimes necessary, the obstetrician–gynecologist is often the first person a woman consults for breast-related signs and symptoms.
 ANATOMY
ANATOMY
The adult female breast is actually a modified sebaceous gland, located within the superficial fascia of the chest wall (Fig. 33.1). Histologically, the breast is composed primarily of lobules or glands, milk ducts, connective tissue, and fat. The relative amounts of these tissue types vary considerably with age. In younger women, the breast consists predominantly of glandular tissue. With age, the glands involute and are replaced by fat, a process accelerated by menopause.
Differences in palpable consistency and in radiographic density between the glands and fat are key modifiers of breast cancer detection programs.Architecturally, the breast is organized into 12 to 20 lobes, with a disproportionate amount of the glandular or lobular tissue in the upper outer quadrants of each breast. This disproportionate distribution of glandular tissue accounts for why breast cancer most commonly arises in the upper outer quadrant. The lobules consist of clusters of secretory cells arranged in an alveolar pattern and surrounded by myoepithelial cells. These glands drain into a series of collecting milk ducts that course through the breast, ultimately coalescing into approximately 5 to 10 collecting ducts that lead to and drain at the nipple. Typically, cancer begins at these terminal duct–lobular units of the breast and follows the path of those ducts.
Congenital anomalies of the breast can include absence of the breast as well as accessory breast tissue located anywhere along the “milk lines,” which extend from the axilla to the groin in the fetus. Extra nipples (polythelia) are more common than true accessory breasts (polymastia).
The breast has a rich blood supply and lymphatic system, which support milk production and overall breast health. The blood supply comes from perforating branches of the internal mammary artery, the lateral thoracic artery, the thoracodorsal artery, the thoracoacromial artery, and various intercostal perforating arteries. The lymphatic vessels lead to several superficial and deep nodal chains throughout the trunk and neck, including those located in the axilla, deep to the pectoralis muscles, and caudal to the diaphragm (Fig. 33.2). The ipsilateral lymph node and, occasionally, the internal mammary nodes are the most common route of metastasis.
Breast tissue is very sensitive to hormonal changes, especially the glandular cells. The transition from the immature, pediatric breast to the mature, adult breast is orchestrated by the changes in circulating levels of estrogen and progesterone that accompany puberty.
Estrogen is primarily responsible for the growth of adipose tissue and lactiferous ducts. Conversely, progesterone stimulation leads to lobular growth and alveolar budding.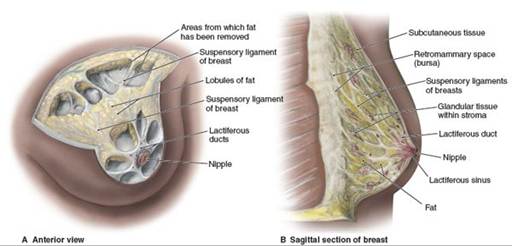
FIGURE 33.1. Anatomy of the breast. (From Agur A, Dalley AF. Grant’s Atlas of Anatomy. 12th ed. Baltimore, MD: Lippincott Williams & Wilkins: 2008:5.)
EVALUATION OF BREAST SIGNS AND SYMPTOMS
A timely evaluation of the patient who presents with a breast complaint is important if for no other reason than to relieve patient anxiety. A systematic approach to evaluating a breast-related complaint will efficiently yield the proper diagnosis.
The two most common presenting complaints related to the breast are pain and concern about a mass. Gynecologists should be aware of the different etiologies of breast pain and be able to offer reassurance, follow-up, and potential treatment. One study has found that breast cancer was diagnosed in 6% of patients with breast complaints (most commonly a mass). Therefore, it is important that breast signs and symptoms be properly evaluated.

FIGURE 33.2. Lymphatic drainage of the breast. (From Agur A, Dalley AF. Grant’s Atlas of Anatomy. 12th ed. Baltimore, MD: Lippincott Williams & Wilkins; 2008:9.)
Patient History
The patient interview is considered the single most important step in the initial evaluation of any disease process. In the case of complaints related to the breast, questions that will aid in deciding the next step include the location of complaints, duration of symptoms, how a mass was first discovered, presence or absence of nipple discharge, any changes in size, and association with menstrual cycle. In addition, the clinician should ask about the presence of risk factors that would increase the likelihood of malignancy (Box 33.1).
Physical Examination
A complete breast examination should evaluate both breasts in a systematic fashion, both axillae and the entire chest wall. The best time to perform a breast examination is in the follicular phase of the menstrual cycle. If the initial examination fails to yield a dominant mass, the options (based on the patient’s risk factors) include either performing a repeat examination in 3 months or referral to a specialized breast care clinic.
Diagnostic Testing
After performing a complete history and physical examination, a number of modalities can be used to help locate and characterize a breast mass.
BOX 33.1 Risk Factors for Breast Cancer
• Age
• Personal history of breast cancer
• History of atypical hyperplasia (ductal or lobular) on past biopsies
• Inherited genetic mutations (BRCA1 and BRCA2)
• High breast tissue density
• First-degree relatives with breast or ovarian cancer diagnosed at an early age
• Early menarche (age < 12 years)
• Late cessation of menses (age > 55 years)
• No term pregnancies
• Late age at first live birth (>30 years)
• Never breastfed
• Recent and long-term oral contraceptive use
• Postmenopausal obesity
• Personal history of endometrial or ovarian cancer
• Alcohol consumption
• Height (tall)
• High socioeconomic status
• Ashkenazi Jewish heritage
Adapted from American College of Obstetricians and Gynecologists. Breast Cancer Screening, Practice Bulletin No. 122, Washington, DC: American College of Obstetricians and Gynecologists; August 2011.
Mammography
Mammography is an x-ray technique used to study the breast. Mammography is able to detect lesions approximately 2 years before they become palpable (Fig. 33.3).
Mammography can be done either as a screening or as a diagnostic test. During a screening mammogram, the patient stands or sits in front of the x-ray machine. Two smooth plastic plates are placed around the breast and subsequently compressed to allow for complete visualization of the tissue.
A standard four-image screening mammogram involves two craniocaudal and two mediolateral images. Images are formed either on standard radiographic film or by digital means (digital radiography). Digital radiographic techniques offer more possibilities of “postprocessing” of the image to enhance detection but are more expensive and not as widely available. No direct superiority has been proven for either technique, though digital mammogram may be preferred for women with more dense breast tissue. In each method, the images are evaluated for defects suspicious of cancer, microcalcifications, distortion of the normal architecture, and any discrete nonpalpable lesion. Lobular carcinoma is more difficult to detect with routine screening mammography.In collaboration with the National Cancer Institute (NCI) and the Food and Drug Administration (FDA), the American College of Radiology has standardized the reporting of mammographic results through a system known as the Breast Imaging Reporting and Data System (BI-RADS). This system helps clearly communicate the final assessment and recommendations to referring physicians (Table 33.1).
A diagnostic mammogram is done to supplement an abnormal screening mammogram or if a woman has a breast complaint and/or palpable mass. In women older than 40 years, mammography is often used as the first-line study in evaluating a patient presenting with a breast mass, even if not palpable on clinical breast examination (CBE). Spot compressions and magnified views are used to further localize any lesions, along with providing dimensions of the surrounding tissue (Fig. 33.4). The contralateral breast should also be imaged in cases of a clinically apparent mass. If possible, the lymph nodes are also imaged to search for unrecognized abnormalities.

FIGURE 33.3. Mammographic and clinical detection of a breast mass. With a presumed doubling time of 100 days, breast cancer may be detected by mammography significantly earlier than it can be identified clinically.
Micro calcif., microcalcification.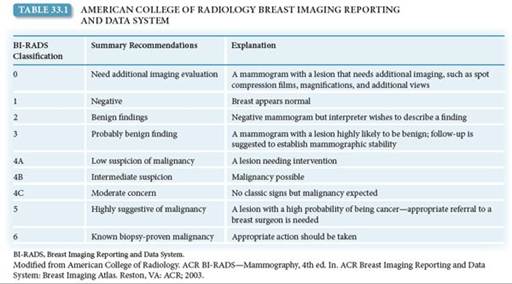
Ultrasonography
Ultrasonography has come to play an important role in the evaluation of breast lesions. It is useful in evaluating inconclusive mammographic findings, in evaluating the breasts of young women and others with dense tissue, allowing better differentiation between a solid and cystic mass, and in guiding tissue core-needle biopsies. An anechoic defect found on ultrasound is consistent with a simple cyst and can be drained for symptomatic relief. In women younger than 40 years (especially adolescents), ultrasonography is the most common initial modality to evaluate a breast mass.
Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) can be a useful adjunct to diagnostic mammography. The use of MRI for screening the general population is limited by the cost of the examination, lack of standard examination technique, and inability to detect microcalcifications. However, MRI is being used as an adjunct for early detection of breast cancer in women at very high risk, and it may also be used as part of post cancer breast diagnosis for further evaluation of breast involvement.
Fine-Needle Aspiration Biopsy
Fine-needle aspiration is useful in determining if a palpable lump is a simple cyst. The procedure is performed in the office with or without the aid of local anesthesia. The suspected mass is stabilized between two fingers of one hand and aspirated using a 22- to 24-gauge needle. Clear aspirated fluid does not need to undergo pathologic evaluation, and the patient may return for a CBE within 4 to 6 months if the mass disappears. If it reappears, the patient is managed with diagnostic mammography and ultrasonography. Bloody aspirated fluid should be evaluated cytologically, and the patient should undergo diagnostic mammography and ultrasonography.
Core-Needle Biopsy
In a core-needle biopsy, a large needle (14–16 gauge) is used to obtain samples from larger, solid breast masses. Three to six samples of tissue approximately 2 cm long are obtained and are evaluated for abnormal cells in relation to the surrounding breast tissue taken in the sample.

FIGURE 33.4. Bilateral film screen mammograms showing typical carcinoma in each breast, illustrating the importance of bilateral mammography in the workup of a clinically apparent mass. (Berek JS, Hacker NF. Practical Gynecologic Oncology. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2005:630.)
Diagnosis Algorithm
If a breast mass is found through a CBE, breast self-examination (BSE), or historically by a patient, the clinician must clearly document the finding and assign appropriate follow-up care. Figure 33.5 presents a practical algorithm for the evaluation and follow-up of a patient with a breast mass.
BENIGN BREAST DISEASE
Benign breast disease includes a large number of conditions that can significantly affect a woman’s quality of life. With accurate diagnosis, many benign breast conditions can be effectively treated with medications or other measures. Women presenting with a breast mass should also be evaluated for their risk of breast cancer.

FIGURE 33.5. Workup of dominant, indeterminate, or suspicious breast mass. (Pruthi S. Detection and evaluation of a palpable breast mass. Mayo Clin Proc. 2001;76(6):641–647.)
Mastalgia
Mastalgia, or breast pain, can be divided into three categories: cyclic, noncyclic, and extramammary (nonbreast) pain. Cyclic mastalgia begins with the luteal phase of the menstrual cycle and resolves after the onset of menses. The pain is generally bilateral and often involves the upper outer quadrants of the breast. Noncyclic mastalgia is not associated with the menstrual cycle and includes such etiologies as tumors, mastitis, cysts, and a history of breast surgery. In some women, noncyclic mastalgia is idiopathic, and no cause is found. Noncyclic pain has also been associated with some medications, including hormonal medications; antidepressants, such as sertraline and amitriptyline; and antihypertensive drugs, in addition to others. If the onset of mastalgia is associated with the start of hormonal therapy, stopping or reducing the hormones may be beneficial. Extramammary pain can be caused by a number of conditions, such as chest wall trauma, rib fractures, shingles, and fibromyalgia. Treatment for musculoskeletal disorders includes anti-inflammatory drugs, but more serious causes of chest pain, such as angina, need to be ruled out.
Medical Therapy
The only medication approved by the FDA for treating mastalgia is danazol, but it has significant side effects. Other hormonal therapies that may decrease pain include bromocriptine and gonadotropin-releasing hormone agonists, but these drugs also have side effects that limit their widespread use. Lisuride maleate is a dopamine agonist that has shown pain-reducing effects, and it has fewer side effects than bromocriptine. Selective estrogen receptor modulators (SERMs), such as tamoxifen, also have a role in treating severe mastalgia, though this is an off-label use of the medications. These medications act as estrogen antagonists in the breast. Side effects of tamoxifen include an increased risk of endometrial hyperplasia and deep venous thrombosis as well as hot flushes and vaginal bleeding. One study concluded that side effects are reduced when the medication is given in smaller doses. Tamoxifen should be used only for cases of severe mastalgia that does not respond to other therapies. Raloxifen, also an SERM, has been shown to decrease the incidences of breast cancer in high-risk women. Unlike tamoxifen, it does not stimulate the endometrium. Hot flashes and increased risk of venous thrombosis are similar to tamoxifen.
Some women with cyclic mastalgia have reported a decrease in pain with oral contraceptives or the injectable contraceptive medroxyprogesterone acetate.
Other Therapies
Nonpharmacologic measures to help relieve breast pain include a properly fitting brassiere or a sports bra worn throughout the day or during exercise, weight reduction, and regular exercise. Although no studies have demonstrated the efficacy of these measures, they are worth recommending to patients and may help relieve pain. Some patients report decreased mastalgia with decreased caffeine and vitamin E supplements but definitive studies have mixed results on effectiveness.
Nipple Discharge
Nipple discharge is usually benign but may be an early sign of endocrine dysfunction or cancer. The color, consistency, and whether the discharge is bilateral or unilateral can yield important clues about its cause. A nonspontaneous, nonbloody, bilateral nipple discharge is usually attributed to fibrocystic changes of the breast or ductal ectasia, a condition characterized by dilation of the mammary ducts, periductal fibrosis, and inflammation. Ductal ectasia is seen in adolescent women as well as in perimenopausal women. Green, yellow, or brown sticky discharge can be due to ductal ectasia or fibrocystic changes of the breast. Milky discharge is common during childbearing, but it can also be associated with other endocrinologic abnormalities (hyperprolactinemia or hypothyroidism) and medications (oral contraceptives and tricyclic antidepressants). Purulent discharge may indicate an infectious etiology and may be due to mastitis or a breast abscess.
Bloody, unilateral nipple discharge may be caused by an invasive ductal carcinoma, intraductal papilloma, or an intraductal carcinoma. Patients with nipple discharge of this type usually require ductography and ductal excision. Breast ductography is an imaging technique that can reveal the location of an intraductal lesion. A new technique that employs fiberoptic technology, fiberoptic ductoscopy, allows the direct visualization of the breast ducts as well as sampling of ductal cells. However, this modality is not widely available.
Breast Masses
The most worrisome finding for patients and clinicians is an unexplained breast mass. Some characteristics of breast masses that suggest malignancy include size greater than 2 cm, immobility, poorly defined margins, firmness, skin dimpling or color changes, retraction or change in the nipple (e.g., scaling), bloody nipple discharge, and ipsilateral lymphadenopathy. The growth rate of a tumor in the breast is thought to be constant from the time of its origin. It is estimated that it takes an average of 5 years for a tumor to reach palpable size.
Benign Breast Masses
A variety of benign breast masses are found on clinical or selfbreast examinations, screening mammograms or incidentally. Table 33.2 summarizes the three morphologic categories and their associated risk of developing invasive breast cancer.

Nonproliferative Lesions
Fibrocystic changes of the breast are a spectrum of features that can be observed in the normal breast. Lobules of the breast may dilate and form cysts of varying sizes. The cyst walls are lined by flattened atrophic epithelium or may be modified through apocrine metaplasia. If these cysts rupture, the resulting scarring and inflammation may lead to fibrotic changes, which make the breast feel firm. An increase in the number of glands with associated lobular growth is known as adenosis. In this case, the architecture of the lobule remains unchanged. In some lactating women, a palpable lactation adenoma may arise secondary to an exaggerated hormonal response.
Simple fibroadenomas are common tumors found in women in their late teens and early twenties. These masses are solid, round, rubbery, and mobile on examination. The tumors do have structural and glandular components in the mass. Although they do not have malignant potential, they can enlarge in pregnancy and cause discomfort.
Proliferative Lesions without Atypia
These lesions are commonly found on mammography and do not usually cause a palpable mass. Histologically, they represent proliferation of cells of the ductal or lobular epithelium. The cells themselves are normal, that is, nonmalignant.
In a normal breast, only myoepithelial cells and a single layer of luminal cells rest on the basement membrane. If there are more than two cell layers, the abnormality is known as epithelial hyperplasia. If there is increased fibrosis within the expanded lobule with distortion and compression of the epithelium, the lesion is termed sclerosing adenosis. A radial scar (or complex sclerosing lesion) is a nidus of tubules entrapped in a densely hyalinized stroma surrounded by radiating arms of epithelium. The lesion mimics an invasive carcinoma. Finally, papillomas are intraductal growths composed of abundant stroma and lined by both luminal and myoepithelial cells. Solitary intraductal papillomas are found in the major lactiferous ducts of women, typically between the ages of 30 and 50 years, and cause a serous or serosanguineous drainage.
Proliferative Lesions with Atypia
When malignant cells replace the normal epithelium lining the ducts or lobules, the lesion is known as a carcinoma in situ. The basement membrane remains intact, and, therefore, the cells cannot metastasize.
There are two major types of carcinoma in situ: lobular carcinoma in situ (LCIS) and ductal carcinoma in situ (DCIS). LCIS is characterized by obliteration of the lumina of the glandular acini by a uniform population of small, atypical cells. In DCIS, the ducts are filled with atypical epithelial cells. Women with DCIS are at increased risk for developing invasive cancer or a recurrence of the DCIS lesion. For these reasons, DCIS should be evaluated with core-needle biopsy followed by surgical biopsy or excision. Management of LCIS and its related condition, atypical lobular hyperplasia, consists of excisional biopsy. Following treatment of both LCIS and DCIS, preventive therapy with SERMs such as tamoxifen has been shown to reduce the risk of invasive breast cancer in these patients.
BREAST CANCER
Breast cancer is the second most common malignancy in women, ranking only behind skin cancer. In addition, it is the second leading cause of cancer-related death in women. According to the American Cancer Society (ACS), an estimated 226,870 women would be diagnosed with and 39,510 women would die of breast cancer in 2012. The steady increase in the incidence of breast cancer can be attributed to the increased use of mammography screening, which has enabled the detection of smaller invasive lesions and the earlier diagnosis of in situ lesions. Advances in treatment have also helped maintain the downward trend in overall breast cancer mortality.
Nevertheless, breast cancer is a serious health concern in the United States. It is estimated that the United States spends approximately $8.1 billion annually on treating breast cancer. The lifetime risk of developing breast cancer in the United States is approximately 12.1% (1 in 8), while the lifetime risk of dying from breast cancer is 3.6% (1 in 28). The age-adjusted death rate was 24.0 per 100,000 women per year.
Risk Factors
Numerous studies have documented factors that increase the relative risk of breast cancer (see Box 33.1).
Age and Race
Age is the single largest risk factor for developing breast cancer. The majority of breast cancer cases occur in women over the age of 50 years. Stratified studies relate risk with age (by decades) and show that the risk of developing breast cancer increases as a woman gets older. For example, a woman has a 1.4% chance of being diagnosed with breast cancer between ages of 40 and 49 years, compared with 3.7% between ages of 60 and 69 years. When stratified by race, white women are more likely to be diagnosed with breast cancer compared with age-matched women of Latin, Asian, and African American descent.
Family History and Genetics
Women who have first-degree relatives (parent, sibling, and offspring) with breast cancer have a higher risk than the general population. If a woman younger than 40 years is diagnosed with breast cancer, evaluating for genetic mutations that predispose individuals to cancer is reasonable. The two most commonly discussed genetic mutations linked to breast cancer are the BRCA1 and BRCA2 gene mutations.
BRCA1 is a gene located on the 17q21 chromosome. This mutation is associated with nearly half of the early-onset breast cancers and approximately 90% of hereditary ovarian cancers. BRCA2 is a gene located on the 13q12–13 chromosome. This mutation has a lower incidence of early-onset breast cancers (35%) and much lower risk of ovarian cancer, compared with BRCA1.
Reproductive and Menstrual History
In general, women who have an early age of menstrual onset (before the age of 12 years) and transition through menopause after the age of 55 years are at increased risk for breast cancer. Delayed childbearing and nulliparity also increase the chance of breast cancer.
Radiation Exposure
Breast tissue of young women (along with the bone marrow and infant thyroid) is highly susceptible to the cancer-causing effects of ionizing radiation. Women who have received a sufficiently large dose of radiation (radiation therapy to treat Hodgkin disease or an enlarged thymus gland) are at risk for radiation-induced breast cancer. The relationship between dose of radiation and risk of cancer is directly linear, although the threshold is unclear. Thus far, epidemiologic studies have not detected a significant increase in cancer risk below a cumulative dose of about 20 cGy. To put this dose into perspective, a typical mammogram results in a breast tissue dose of about 0.3 cGy. The time needed for a radiation-induced lesion to develop is about 5 to 10 years from exposure.
Breast Changes
It is believed that women with dense breast tissue are at increased risk for breast cancer. In addition, histologic biopsies finding atypical hyperplasia or lobular carcinoma in situ greatly increase the risk of breast cancer.
Other Factors
Being overweight after menopause has been linked to an increased risk of breast cancer. A possible mechanism in this relationship is that the increased peripheral conversion of androstenedione to estrone stimulates breast cancer development. Lack of exercise throughout life is linked to the increased risk of breast cancer through the associated risk of obesity.
Women who consume 2 to 4 alcoholic drinks per week have a 30% greater risk of dying from breast cancer than women who never drink. The exact mechanism of action is unclear, but researchers speculate that alcohol consumption stimulates the growth and progression of breast cancer by inducing angiogenesis and increasing the expression of vascular endothelial growth factor.
Breast Cancer Risk Assessment Tool: The Gail Model
The NCI has developed a computer-based tool to allow clinicians to estimate a woman’s risk of developing invasive breast cancer over the next 5 years and in their lifetime (up to age 90 years). The tool is based on a mathematical model of breast cancer risk calculation called the Gail model. Seven risk factors are used in the calculations: a history of LCIS or DCIS, age, age at onset of menstruation, age at the time of the first live birth, number of first-degree relatives with breast cancer, history of breast biopsy, and race/ethnicity. The usefulness of the Gail model is limited in patients with second-degree relatives with breast cancer (e.g., paternal transmission) and is falsely increased in patients with multiple breast biopsies. A family history of breast cancer is the strongest predictor of risk among the factors used in the model.
Women at high risk, defined as a 5-year risk of 1.7% or more, can be referred for possible prophylactic therapy. Current prophylactic options include chemoprevention with the SERMs tamoxifen and raloxifene and prophylactic mastectomy. Because all of the options are associated with significant side effects, individualized risk assessment should be performed to determine whether a patient is a candidate for breast cancer risk reduction and, if so, which option is best.
Histologic Types of Breast Cancer
Malignant tumors of the breast may arise from any of the major components of the breast. The American Joint Committee on Cancer (AJCC) classifies most breast malignancies into one of three histologic categories according to their corresponding cells of origin: ductal, lobular, and nipple. About 70% to 80% of breast cancers are invasive ductal carcinomas. These are most common among women in their fifties and have a tendency to spread to regional lymph nodes. Invasive lobular carcinomas comprise 5% to 15% of breast cancers. This type is often multifocal and bilateral. Table 33.3 summarizes the differences between the two processes. Paget disease of the nipple presents as a superficial skin lesion similar to eczema.
Breast Cancer Staging
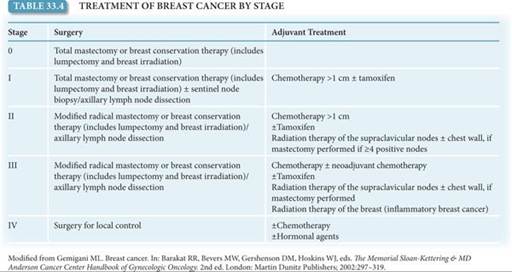
The AJCC stages breast malignancies according to the TNM system that describes characteristics of the primary tumor, involvement of regional lymph nodes, and distant metastasis. Surgical stage helps determine the appropriate types of therapy (Table 33.4).

In addition to stage, receptor status is another important indicator of breast cancer prognosis. Expression of estrogen or progesterone receptors positively affects prognosis. The Her2/ neu (or c-erb-B2) is an oncogene encoding a membrane-bound growth factor receptor. Overexpression confers a poor prognosis and is noted in 20% to 30% of invasive ductal cancers.
Breast Cancer Treatment
Breast cancer poses both a local regional risk (i.e., to the breast and regional lymph nodes) and a systemic risk.
Surgical Therapy
The surgical treatment is lumpectomy (breast conservation therapy) or mastectomy. Both procedures are aimed at achieving local control. Mastectomy is removal of all breast tissue and the nipple areolar complex with preservation of the pectoralis muscles. A modified radical mastectomy also includes removal of the axillary lymph nodes. Radiation therapy is used in conjunction with mastectomy for later stages of breast cancer and to accompany lumpectomy and partial mastectomy for early stages of breast cancer. Radiation is an essential component of lumpectomy. The combination of lumpectomy and radiation yields outcomes that are equal to those of radical mastectomy.
Breast reconstruction should be an option for all women who desire it. Reconstruction can be achieved by several methods, including the insertion of a saline implant under the pectoral muscle or by using a rectus muscle to replace the lost tissue. To prepare for a saline implant, a tissue expander is placed beneath the muscle. Saline is injected into the expander over a period of weeks to months until the space is large enough to accommodate the implant. Breast reconstruction can take place immediately after surgery or it can be delayed for several months. Radiation therapy can be given if breast reconstruction has taken place.
Medical Therapy
Adjuvant (systemic) therapy is used in the treatment of all stages of breast cancer, regardless of lymph node status. Adjuvant therapy includes chemotherapeutic drugs that kill cancer cells and hormonal therapies such as tamoxifen that act as estrogen antagonists. Tamoxifen or raloxifen are used to treat women with estrogen receptor–positive breast cancer. It can be used in conjunction with chemotherapy. It is also given as a 5-year course of preventive treatment following surgery. Aromatase inhibitors (AIs) prevent the production of estrogen in postmenopausal women. AIs are used to extend survival in women with metastatic cancer, as primary adjuvant therapy, and in conjunction with tamoxifen to prevent cancer recurrence.
Another drug used to treat breast cancer is trastuzumab. It acts on membrane-bound protein produced by Her2/neu. If a patient’s cancer is found to overexpress the Her2/neu protein, trastuzumab can be given as adjuvant therapy. Trastuzumab is associated with significant side effects, including heart failure, respiratory problems, and life-threatening allergic reactions.
Follow-Up
Obstetrician–gynecologists are in the unique position of providing care for women who have been treated for breast cancer. For some women, the continuation of care spans many years. Once the initial treatment has been completed, the obstetrician–gynecologist often takes on the role of screening and surveillance. For the first 2 years, follow-up appointments occur every 3 to 6 months and then annually after that. Annual mammography and physical examinations should continue indefinitely. Most breast cancer recurrences will occur within 5 years of primary therapy.
 SCREENING GUIDELINES
SCREENING GUIDELINES
For the general population, breast cancer surveillance involves a combination of CBEs and radiographic imaging. In 2009, the U.S. Preventative Service Task Force (USPSTF) found insufficient evidence for teaching BSEs. The American College of Obstetricians and Gynecologists (College) supports the practice of BSE only in high-risk patients and for breast self-awareness in low-risk patients. The value of CBE in detecting breast cancer has also been studied. Pooled data from multiple studies support the use and effectiveness of CBE. Multiple reviews have supported the combination of CBE and mammography for breast cancer screening for women ages 50 to 69 years. The College supports the recommendations of the ACS, which calls for CBEs every 1–3 years for women ages 20 to 39 years and annually thereafter. In 2009, USPSTF concluded that the current evidence is insufficient to assess the additional benefits and harms of CBE beyond screening mammography in women of 40 years or older.
The value of mammography increases with age. The USPSTF found sufficient evidence to demonstrate that mammogram screening every 1 to 3 years significantly reduced mortality from breast cancer. Controversy exists over screening intervals in younger women, in whom the incidence of breast cancer remains low. The College currently recommends that mammography be performed annually after the age of 40 years, whereas the USPSTF recommends that the decision to start regular, biennial screening mammography before age 50 years should be an individual one and take patient context into account, including the patient’s values regarding specific benefits and harms. The USPSTF concluded that the current evidence is insufficient to assess the additional benefits and harms of screening mammography in women 75 years or older, though many patients and practitioners continue to recommend the practice.
These screening standards do not apply to women with inherited genetic mutations placing them at increased risk for developing breast cancer. In this population, breast cancer occurs at a younger age and is missed by screening mammography nearly 50% of the time. Current recommendations for BRCA carriers include monthly BSEs beginning at the age of 18 to 20 years, annual CBEs, and screening mammograms beginning after age 25 years (or 5–10 years before the age of diagnosis in the affected relative). MRI is recommended as a supplement to mammography, not a replacement.
Clinical Follow-Up
This patient’s history and findings are consistent with fibrocystic change. Physical examination suggested a cystic mass, and aspiration with a small-gauge needle yields a quantity of straw-colored fluid and resolution of the mass. Follow-up 1 month later fails to find any recurrence.
thePoint Visit http://thepoint.lww.com/activate for an interactive USMLE-style question bank and more!