Chapter 31 Endometriosis
This chapter deals primarily with APGO Educational Topic Area:
TOPIC 38 ENDOMETRIOSIS
Students should be able to discuss pathogenesis and common sites affected by endometriosis.
They should outline a basic approach to the diagnosis of endometriosis, using common symptoms and physical examination findings, and to the management of endometriosis.Clinical Case
A 32-year-old gravida 0 woman presents with symptoms of cyclic lower abdominal pain, dysmenorrhea, and inability to conceive after trying unprotected intercourse for the past year. Her partner has had semen analysis performed, and it is reported to be normal. The patient’s abdominal pain generally starts 1 to 2 days before her menses and lasts for the first day or so of menstrual flow. This pain has gradually worsened over the past 2 years and no longer is well controlled with nonsteroidal anti-inflammatory medications. The patient has recently begun experiencing deep-thrust dyspareunia. The patient’s periods have been regular with occasional episodes of midcycle spotting.
Endometriosis is the presence of endometrial glands and stroma in any extrauterine site and may be suspected based on history, symptoms, and physical examination as well as laboratory and imaging information. Like the endometrial tissue from which it is derived, endometrial implants and cysts respond to the hormonal fluctuations of the menstrual cycle. Laparotomy or laparoscopy may reveal lesions consistent with endometriosis, but, because lesions may be small, atypical, or caused by pathology other than endometriosis, only proven tissue biopsy diagnosis is diagnostic. Many women with endometriosis are asymptomatic, and diagnosis is discovered only when surgery is performed for other indications.
It is estimated that 7% to 10% of women in the general population have endometriosis. Pelvic endometriosis is present in 6% to 43% of women undergoing sterilization, 12% to 32% of women undergoing laparoscopy for pelvic pain, and 21% to 48% of women undergoing laparoscopy for infertility.
Endometriosis usually occurs in women of reproductive age and is less frequently found in postmenopausal women. Endometriosis occurs more often in women who have never had children.Some evidence suggests that endometriosis may have a genetic component. Women with first-degree relatives with endometriosis have nearly a 10-fold increased risk of developing endometriosis. The proposed mechanism of inheritance is polygenic and multifactorial.
 PATHOGENESIS
PATHOGENESIS
The exact mechanisms by which endometriosis develops are not clearly understood. Three major theories are commonly cited.
1. Direct implantation of endometrial cells, typically by means of retrograde menstruation: This mechanism is consistent with the occurrence of pelvic endometriosis and its predilection for the ovaries and pelvic peritoneum, as well as for sites such as an abdominal incision or episiotomy scar. (Many women experience some degree of retrograde menstruation without developing endometriosis.) Direct implantation is commonly referred to as the Sampson theory after the scientist whose experimental work showed the possibility of such a mechanism.
2. Vascular and lymphatic dissemination of endometrial cells (the Halban theory): Distant sites of endometriosis can be explained by this process (i.e., endometriosis in locations such as lymph nodes, the pleural cavity, and kidney).
3. Coelomic metaplasia of multipotential cells in the peritoneal cavity (the Meyer theory): Under certain conditions, these cells can develop into functional endometrial tissue. This could even occur in response to the irritation caused by retrograde menstruation. The early development of endometriosis in some adolescents before the onset of menstruation lends credence to this theory.
It is probable that more than one theory is necessary to explain the diverse nature and locations of endometriosis. Underlying all these possibilities is a yet undiscovered immunologic factor that would explain why some women develop endometriosis, whereas others with similar characteristics do not.
 PATHOLOGY
PATHOLOGY
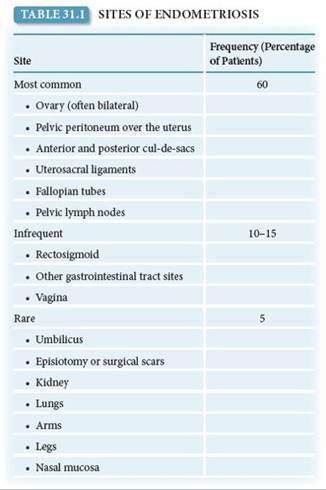
Endometriosis is most commonly found on the ovaries and is typically bilateral. Other common pelvic structures involved include the pouch of Douglas or posterior cul-de-sac (particularly the uterosacral ligaments and rectovaginal septum), the round ligament, the fallopian tubes, and the sigmoid colon (Fig. 31.1 and Table 31.1). On rare occasions, distant endometriosis is found in abdominal surgical scars, the umbilicus, and various organs outside the pelvic cavity, including the lungs, brain, and upper ureters.
The gross appearance of endometriosis varies considerably and includes the following forms:
• Small (1 mm), clear, or white lesions
• Small, dark red (“mulberry”), or brown (“powder burn”) lesions
• Cysts filled with dark red or brown hemosiderin-laden fluid (“chocolate” cysts)
• Dark red or blue “domes” that may reach 15 to 20 cm in size
Reactive fibrosis frequently surrounds these lesions, which gives a puckered appearance. More advanced disseminated disease causes further fibrosis and may result in dense adhesions.
SIGNS AND SYMPTOMS
Women with endometriosis demonstrate a wide variety of symptoms. The nature and severity of symptoms may not match either the location or extent of the disease. Women with grossly extensive endometriosis may have few symptoms, whereas those with minimal gross endometriosis may have severe pain. Endometriosis may also be asymptomatic. The pain associated with endometriosis is thought to depend more upon the depth of invasion of the implants rather than on the number or extent of the superficial implants. The classic symptoms of endometriosis include progressive dysmenorrhea and deep dyspareunia. Some patients experience chronic, unremitting pelvic discomfort along with dysmenorrhea and dyspareunia. Chronic pelvic pain may be related to the adhesions and pelvic scarring found in association with endometriosis.

FIGURE 31.1. Locations of endometrial implants.
Dysmenorrhea and Dyspareunia
Dysmenorrhea caused by endometriosis is not directly related to the amount of visible disease. In many women with endometriosis, the dysmenorrhea worsens over time. Endometriosis should be considered a possible etiology in patients who present with dysmenorrhea that does not respond to oral contraceptives or nonsteroidal anti-inflammatory drugs (NSAIDs). Dyspareunia is often associated with uterosacral or deep posterior cul-de-sac involvement with endometriosis. The dyspareunia is typically reported on deep penetration, although there is no correlation between dyspareunia and the extent of endometriosis.
Infertility
Infertility is more frequent in women with endometriosis, although a cause-and-effect relationship has not been established. With extensive disease, pelvic scarring and adhesions that distort pelvic anatomy may cause infertility secondary to tubal distortion, but the cause of infertility in women with minimal endometriosis is unclear. Prostaglandins and autoantibodies have been implicated, but these relationships remain unproven. In some cases, infertility may be the only complaint, and endometriosis is discovered at the time of laparoscopic evaluation as part of the infertility workup. The presence of endometriosis in asymptomatic infertility patients varies between 30% and 50%.
Other Symptoms
Other, less common symptoms of endometriosis include gastrointestinal (GI) symptoms, such as rectal bleeding and dyschezia (painful bowel movements), in patients with endometrial implants on the bowel and urinary symptoms such as hematuria in patients with endometrial implants on the bladder or ureters. Occasionally, patients may present with an acute abdominal emergency, which may be associated with the rupture or torsion of an endometrioma.
Other Signs
Pelvic examination may reveal the “classic” sign of uterosacral nodularity associated with endometriosis, but it is often absent even when substantial gross endometriosis is discovered at surgery. The uterus may be relatively fixed and retroflexed in the pelvis because of extensive adhesions. Ovarian endometriomas may be tender, palpable, and freely mobile in the pelvis, or adhered to the posterior leaf of the broad ligament, the lateral pelvic wall, or the posterior cul-de-sac (see Fig. 31.2).
DIFFERENTIAL DIAGNOSIS
Depending on the symptoms, the differential diagnosis will change. In patients with chronic abdominal pain, diagnoses such as chronic pelvic inflammatory disease, pelvic adhesions, GI dysfunction, and other etiologies of chronic pelvic pain should be considered. In patients with dysmenorrhea, both primary dysmenorrhea and secondary dysmenorrhea should be considered. In patients with dyspareunia, differential diagnoses include chronic pelvic inflammatory disease, ovarian cysts, and symptomatic uterine retroversion. Sudden abdominal pain may be caused by a ruptured endometrioma as well as by ectopic pregnancy, acute pelvic inflammatory disease, adnexal torsion, and rupture of a corpus luteum cyst or ovarian neoplasm.
 DIAGNOSIS
DIAGNOSIS
Endometriosis should be suspected in patients with the previously described symptoms. Many symptomatic women have normal findings on pelvic examination. The diagnosis of endometriosis can be suspected by direct visualization during laparoscopy or laparotomy and confirmed by tissue biopsy. Because endometriosis has various gross appearances, tissue biopsy and confirmation of endometrial glands and stroma are required for diagnosis. The presence of two or more of the following histologic features is used as the threshold criteria for the diagnosis by a pathologist:
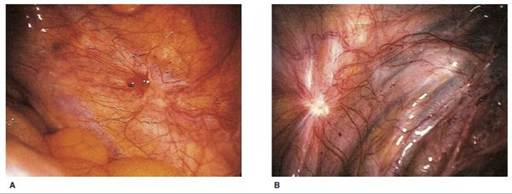


FIGURE 31.2.
Endometrial implants. (A) Clear lesion on the ovarian fossa; (B) white endometriotic deposit on the left uterosacral ligament; (C) “powder burn” lesion on the uterosacral ligaments; (D) right ovarian endometrioma; (E) chocolate cyst in an ovary containing other smaller fibrous-filled cavities. (From Overton C, Davis C, McMillan L, Shaw RW. An Atlas of Endometriosis. 3rd ed. London: Informa UK; 2007:3.2, 4.2, 5.3, 5.4, 9.55.)• Endometrial epithelium
• Endometrial glands
• Endometrial stroma
• Hemosiderin-laden macrophages
Because tissue confirmation of the diagnosis of endometriosis requires a surgical procedure, investigators have searched for a noninvasive alternative. Increased serum CA-125 levels have been correlated with moderate to severe endometriosis. However, because CA-125 levels may be elevated in many conditions (e.g., uterine fibroids, ovarian epithelial cancer, and pelvic inflammation) and nongynecologic sources (including cirrhosis and pancreatic and lung cancers) as well as in smokers, the clinical utility of using it as a diagnostic marker is limited.
Imaging
Imaging studies, such as ultrasonography, magnetic resonance imaging (MRI), and computed tomography, appear to be useful only in the presence of a pelvic or adnexal mass. Ultrasonography may be used to visualize ovarian endometriomas, which typically appear as cysts containing low-level, homogeneous internal echoes consistent with old blood. MRI may detect deeply infiltrating endometriosis that involves the uterosacral ligaments and the cul-de-sac but lacks sensitivity in detecting rectal involvement.
Classification
Once endometriosis is diagnosed, its extent and severity should be documented. The most widely accepted classification system has been established by the American Society for Reproductive Medicine (Fig. 31.3). Although this classification scheme has limitations, it provides a uniform system for recording findings and comparing the results of various therapies.
TREATMENT
Available therapies include expectant, hormonal, surgical, and combination medical-and-surgical treatment. The choice of treatment depends on the patient’s individual circumstances, which include 1) the presenting symptoms and their severity, 2) the location and severity of endometriosis, and 3) the desire for future childbearing. No treatment provides a permanent cure. Total abdominal hysterectomy with bilateral salpingo-oophorectomy is associated with a 10% risk of recurrent symptoms and a 4% risk of additional endometriosis. Reasonable goals for management of endometriosis include reduction in pelvic pain, minimizing surgical intervention, and preserving fertility.
Expectant Management
Patients can be treated expectantly (i.e., without either medical or surgical therapy) in some selected cases, including patients with limited disease whose symptoms are minimal or nonexistent and those who are attempting to become pregnant. Because endometriosis responds to estrogen and progesterone, older patients with mild symptoms may opt to wait until the natural decrease in levels of these hormones that occurs with menopause.
Medical Therapy
Because the glands and stroma of endometriosis respond to both exogenous and endogenous hormones, suppression of endometriosis is based on a medication’s potential ability to induce atrophy of the endometrial tissue. This treatment approach is optimal for patients who are currently symptomatic, have documented endometriosis beyond minimal disease, and who desire pregnancy in the future. The patient should be aware that recurrence after the completion of medical therapy is common and that medical therapy does not affect adhesions and fibrosis caused by the endometriosis. Medical therapy may often be instituted empirically without a definitive surgical diagnosis of endometriosis, if the patient’s symptoms are consistent with the disease and appropriate, thorough physical examination and workup have been performed to rule out other causes of pain, including gynecological, GI, and urologic causes.
Oral Contraceptives
Because of their ease of administration and relatively low level of side effects, combined oral contraceptives used in conjunction with NSAIDs are often the first line of treatment for pain associated with endometriosis. Oral contraceptive therapy induces a decidual reaction in the functioning endometriotic tissue. Continuous therapy, in which the oral contraceptive regimen is taken continuously without the 7 days of inactive pills that induce withdrawal bleeding, can also be prescribed to prevent secondary dysmenorrhea.
Progesterone therapy, in the form of subcutaneous depot medroxyprogesterone acetate (DMPA) or implants, suppresses gonadotropin release and, in turn, ovarian steroidogenesis; it also directly affects the uterine endometrium and endometrial implants. DMPA has been associated with an increased risk of bone mineral loss, although bone mineral density returned to pretreatment levels 12 months after treatment (see Chapter 26). Daily oral medroxyprogesterone is an option for women who are trying to become pregnant insofar as it does not offer a reliable contraceptive effect.
Other Pharmacologic Agents
Danazol is a medication that suppresses both luteinizing hormone (LH) and follicle-stimulating hormone (FSH) midcycle surges. In the absence of LH and FSH stimulation, the ovary no longer produces estrogen, which induces amenorrhea and endometrial atrophy. Side effects of danazol, which occur in a minority of patients, are related to its hypoestrogenic and androgenic properties and include acne, spotting and bleeding, hot flushes, oily skin, growth of facial hair, decreased libido, atrophic vaginitis, and deepening of the voice. Some of these side effects do not resolve with the discontinuation of therapy. Lipoprotein metabolism is also altered; serum high-density lipoprotein levels increase significantly while low-density lipoprotein levels decrease.
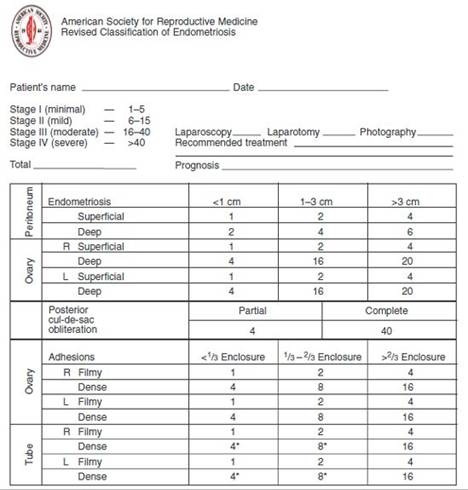
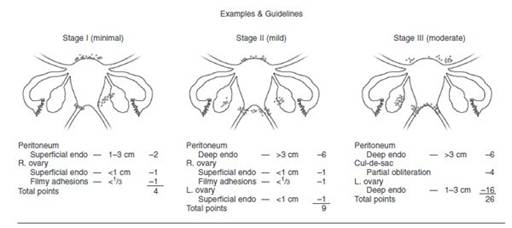

FIGURE 31.3. Revised American Society for Reproductive Medicine classification of endometriosis. (Reprinted from American Society for Reproductive Medicine. Revised American Society for Reproductive Medicine classification of endometriosis: 1996. Fertility and Sterility; 1997:67(5):817–821, with permission from the American Society for Reproductive Medicine.)
Comparable symptom relief can be achieved with fewer effects using gonadotropin-releasing hormone (GnRH) agonists. GnRH agonists downregulate the pituitary gland and cause marked suppression of LH and FSH. However, the side effects are less severe than those of danazol, because androgenic side effects are eliminated. However, the hypoestrogenic effect produced by GnRH agonists may cause hot flushes and night sweats and a slight increase in the risk of bone density loss. If a patient develops side effects while taking a GnRH agonist, if the therapy is required for longer than 6 months, or if repeated treatments are required, add-back therapy consisting of low-dose combination oral contraceptives, low-dose hormone therapy, or medroxyprogesterone should be considered. Norethindrone acetate 5 mg has been extensively studied and is also approved for this use by the Food and Drug Administration. Add-back therapy is often started with GnRH agonist therapy because it does not affect the drug’s control of pelvic pain and mitigate the vasomotor and bone density side effects. Aromatase inhibitor therapy is also emerging as an alternative for the pain associated with endometriosis and may be considered for some patients.
Surgical Therapy
The surgical management of endometriosis can be classified as either conservative or extirpative.
Conservative Surgery
Conservative surgery includes excision, cauterization, or ablation (by laser or electrocoagulation) of visible endometriotic lesions; normalization of anatomy; and preservation of the uterus and other reproductive organs to allow for a possible future pregnancy. Conservative surgery is often undertaken at the time of the initial laparoscopy performed for pain or infertility. If extensive disease is found, conservative surgery involves lysis of adhesions; removal of active endometriotic lesions; and, possibly, reconstruction of reproductive organs. Success rates of conservative surgery appear to correlate with the severity of the disease at the time of surgery as well as with the skill of the surgeon. Medical therapy can be instituted before surgery to reduce the amount of endometriosis and after surgery to facilitate healing and prevent recurrence. Pregnancy rates following electrical energy or argon laser range from 34% to 75%. Pregnancy rates after carbon dioxide laser vaporization range from 25% to 100% for stage 2 disease, from 19% to 66% for stage 3 disease, and from 25% to 50% for stage 4 disease.
Extirpative Surgery
Extirpative surgery for endometriosis is reserved only for cases in which the disease is so extensive that conservative medical or surgical therapy is not feasible, or when the patient has completed her family and wishes definitive therapy. Definitive surgery includes total abdominal hysterectomy, bilateral salpingo-oophorectomy, lysis of adhesions, and removal of endometriotic implants. One or both ovaries may be spared if they are uninvolved, and the endometriosis can be resected completely. Approximately one third of women treated conservatively will have recurrent endometriosis and require additional surgery within 5 years. Ovarian conservation at the time of hysterectomy carries an increased risk of recurrent endometriosis requiring additional surgery. After bilateral oophorectomy, estrogen therapy may be initiated immediately, with little risk of reactivating residual disease.
Clinical Follow-Up
This patient’s history is typical for endometriosis, and the patient was offered empiric treatment with an oral contraceptive, a gonadotropin-releasing hormone agonist, or diagnostic laparoscopy. Because of the patient’s desire to achieve pregnancy in the shortest amount of time, she elected to undergo laparoscopic evaluation, which documented mild to moderate pelvic endometriosis with tubal scarring.
thePoint Visit http://thepoint.lww.com/activate for an interactive USMLE-style question bank and more!