Chapter 5 Normal pregnancy
Antenatal care
Booking
Breastfeeding
Dating in pregnancy
Diagnosis of pregnancy
Minor symptoms of pregnancy
Physiological changes in pregnancy
Preparing for pregnancy
Puerperium
Routine blood tests in pregnancy Antenatal care
The main principles of antenatal care in uncomplicated pregnancies are to provide advice, education, reassurance and support.
It is also to address and treat the minor problems of pregnancy, to provide effective screening during the pregnancy and to identify major problems as they arise and to manage them. Booking appointmentRefer to Chapter 5.2, Booking. Antenatal information
• Information should be given in a form that is easy to understand and accessible to pregnant women including those with additional needs, such as physical, sensory or learning disabilities, and to pregnant women who do not speak or read English. Information can also be given in other forms such as audiovisual or touch screen technology; this should be supported by written information.
• Pregnant women should be offered information based on the current available evidence together with support to enable them to make informed decisions about their care. This information should include where they will be seen and who will undertake their care.
• At each antenatal appointment, healthcare professionals should offer consistent information and clear explanations, and should provide pregnant women with an opportunity to discuss issues and ask questions.
• Pregnant women should be offered opportunities to attend participant-led antenatal classes, including breastfeeding workshops.
• Pregnant women should be informed about the purpose of any test before it is performed. The healthcare professional should ensure the woman has understood this information and has sufficient time to make an informed decision.
The right of a woman to accept or decline a test should be made clear.• Information about antenatal screening should be provided in a setting where discussion can take place; this may be in a group setting or on a one-to-one basis. This should be done at or before the booking appointment. Provision and organization of care
Who?
• Midwife- and GP-led models of care should be offered to women with an uncomplicated pregnancy. Routine involvement of obstetricians in the care of women with an uncomplicated pregnancy at scheduled times does not appear to improve perinatal outcomes compared with involving obstetricians when complications arise.
• Antenatal care should be provided by a small group of healthcare professionals with whom the woman feels comfortable. There should be continuity of care throughout the antenatal period.
• A system of clear referral paths should be established so that pregnant women who require additional care are managed and treated by the appropriate specialist teams when problems are identified.
Where?
• Antenatal care should be readily and easily accessible to all pregnant women and should be sensitive to the needs of individual women and the local community.
• The environment in which antenatal appointments take place should enable women to discuss sensitive issues such as domestic violence, sexual abuse, psychiatric illness and recreational drug use. Documentation of care
• Structured maternity records should be used for antenatal care.
• Maternity services should have a system in place whereby women carry their own case notes.
• A standardized, national maternity record with an agreed minimum data set should be developed and used. This will help healthcare professionals to provide the recommended evidence-based care to pregnant women. Frequency of antenatal appointments
A schedule of antenatal appointments should be determined based upon the needs of the individual mothers. For a woman who is nulliparous with an uncomplicated pregnancy, a schedule of 10 appointments should be adequate.
For a woman who is parous with an uncomplicated pregnancy, a schedule of seven appointments should be adequate. Gestational age assessmentPregnant women should be offered an early ultrasound scan between 10 weeks 0 days and 13 weeks 6 days to determine gestational age and to detect multiple pregnancies. This will ensure consistency of gestational age assessment and reduce the incidence of induction of labour for prolonged pregnancy. Crown–rump length measurement should be used to determine gestational age. If the crown–rump length is above 84 mm, the gestational age should be estimated using head circumference. Lifestyle considerations
• Working during pregnancy should be discussed.
• Pregnant women should be informed of their maternity rights and benefits.
• Nutritional supplements
• Pregnant women (and those intending to become pregnant) should be informed that dietary supplementation with folic acid, before conception and throughout the first 12 weeks, reduces the risk of having a baby with a neural tube defect (for example, anencephaly or spina bifida). The recommended dose is 400 μg per day.
• Iron supplementation should not be offered routinely to all pregnant women. It does not benefit the mother’s or the baby’s health and may have unpleasant maternal side-effects.
• Prescribed medicines: see Chapter 8.12, Drugs in pregnancy
• Complementary therapies
• Pregnant women should be informed that few complementary therapies have been established as being safe and effective during pregnancy. Women should not assume that such therapies are safe and they should be used as little as possible during pregnancy.
• Exercise in pregnancy
• Pregnant women should be informed that beginning or continuing a moderate course of exercise during pregnancy is not associated with adverse outcomes.
• Pregnant women should be informed of the potential dangers of certain activities during pregnancy, for example contact sports, high-impact sports and vigorous racquet sports that may involve the risk of abdominal trauma, falls or excessive joint stress, and scuba diving, which may result in fetal birth defects and fetal decompression disease.
• Sexual intercourse in pregnancy is not known to be associated with any adverse outcomes.
• Alcohol consumption in pregnancy
• Pregnant women and women planning a pregnancy should be advised to avoid drinking alcohol in the first 3 months of pregnancy if possible because it may be associated with an increased risk of miscarriage.
• Excess alcohol can give rise to fetal alcohol syndrome.
• Fetal alcohol spectrum disorders are diagnosed in childhood and may present as attention disorders and inappropriate behaviour. The quantity of alcohol that causes these late problems is not known and hence avoidance is best.
• Smoking in pregnancy
• Pregnant women should be informed about the specific risks of smoking during pregnancy (such as the risk of having a baby with low birthweight and pre-term birth). The benefits of quitting at any stage should be emphasized.
• The direct effects of cannabis on the fetus are uncertain but may be harmful. Cannabis use is associated with smoking, which is known to be harmful; therefore, women should be discouraged from using cannabis during pregnancy.
• Pregnant women should be informed that long-haul air travel is associated with an increased risk of venous thrombosis. In the general population, wearing correctly fitted compression stockings is effective at reducing the risk. Minor ailments in pregnancy
• Women should be informed that most cases of nausea and vomiting in pregnancy will resolve spontaneously within 16–20 weeks and that nausea and vomiting are not usually associated with a poor pregnancy outcome. Information about all forms of self-help and non-pharmacological treatments should be made available for pregnant women who have nausea and vomiting.
• Women who present with symptoms of heartburn in pregnancy should be offered information regarding lifestyle and diet modification. Antacids may be offered to women whose heartburn remains troublesome despite lifestyle and diet modification.
• Women who present with constipation in pregnancy should be offered information regarding diet modification, such as bran or wheat fibre supplementation.
• Haemorrhoids: In the absence of evidence of the effectiveness of treatments for haemorrhoids in pregnancy, women should be offered information concerning diet modification. If clinical symptoms remain troublesome, standard haemorrhoid creams should be considered.
• Varicose veins are a common symptom of pregnancy that will not cause harm. Compression stockings can improve the symptoms but will not prevent varicose veins from emerging.
• An increase in vaginal discharge is a common physiological change that occurs during pregnancy. If it is associated with itch, soreness, offensive smell or pain on passing urine there may be an infective cause and investigation should be considered. A 1-week course of a topical imidazole is an effective treatment and should be considered for vaginal candidiasis infections in pregnant women. The effectiveness and safety of oral treatments for vaginal candidiasis in pregnancy are uncertain and these treatments should not be offered. Clinical examination of pregnant women
• Maternal weight and height should be measured and body mass index (BMI) calculated at the booking appointment (BMI = weight (kg)/height (m)2).
• Routine breast examination during antenatal care is not recommended for the promotion of postnatal breastfeeding.
• Routine antenatal pelvic examination does not accurately assess gestational age, nor does it accurately predict preterm birth or cephalopelvic disproportion. It is not recommended.
• Female genital mutilation: Pregnant women who have had female genital mutilation should be identified early in antenatal care through sensitive enquiry. Antenatal examination will then allow planning of intrapartum care.
• Healthcare professionals need to be alert to the symptoms or signs of domestic violence and women should be given the opportunity to disclose domestic violence in an environment in which they feel secure.
• In all communications (including initial referral) with maternity services, healthcare professionals should include information on any relevant history of mental disorder.
At a woman’s first contact with services in both the antenatal and the postnatal periods, healthcare professionals (including midwives, obstetricians, health visitors and GPs) should ask about past or present history of severe mental illness including schizophrenia, bipolar disorder or psychosis in the postnatal period. Severe depression, previous treatment by a psychiatrist/specialist mental health team, including inpatient care and a family history of perinatal mental illness should be known. After identifying a possible mental disorder in a woman during pregnancy or the postnatal period, further assessment should be considered, in consultation with colleagues if and when necessary. Screening for haematological conditionsAnaemia
• Pregnant women should be offered screening for anaemia. Screening should take place early in pregnancy (at the booking appointment) and at 28 weeks when other blood screening tests are being performed. This allows enough time for treatment if anaemia is detected.
• Haemoglobin levels outside the normal range for pregnancy (that is 11 g/100 mL at first contact and 10.5 g/100 mL at 28 weeks) should be investigated and iron supplementation considered if indicated.
Blood grouping and red cell alloantibodies
• Women should be offered testing for blood group and rhesus D status in early pregnancy.
• It is recommended that routine antenatal anti-D prophylaxis is offered to all non-sensitized pregnant women who are rhesus D negative.
• Women should be screened for atypical red cell alloantibodies in early pregnancy and again at 28 weeks, regardless of their rhesus D status.
• In some countries, if a pregnant woman is rhesus D negative, consideration is given to partner testing to determine whether the administration of anti-D prophylaxis is necessary.
Screening for haemoglobinopathies
• Screening for sickle cell diseases and thalassaemias should be offered to all women as early as possible in pregnancy (ideally by 10 weeks). The type of screening depends upon the prevalence and can be carried out in either primary or secondary care.
• Where prevalence of sickle cell disease is high (fetal prevalence above 1.5 cases per 10 000 pregnancies), laboratory screening (preferably high-performance liquid chromatography) should be offered to all pregnant women to identify carriers of sickle cell disease and/or thalassaemia.
• Where prevalence of sickle cell disease is low (fetal prevalence 1.5 cases per 10 000 pregnancies or below), all pregnant women should be offered screening for haemoglobinopathies using the Family Origin Questionnaire.
• If the Family Origin Questionnaire indicates a high risk of sickle cell disorders, laboratory screening (preferably high-performance liquid chromatography) should be offered.
• If the mean corpuscular haemoglobin is below 27 pg, laboratory screening (preferably high-performance liquid chromatography) should be offered.
• If the woman is identified as a carrier of a clinically significant haemoglobinopathy then the father of the baby should be offered counselling and appropriate screening carried out without delay.
Screening for fetal anomalies
• Ultrasound screening for fetal anomalies should be routinely offered, normally between 18 weeks 0 days and 20 weeks 6 days.
• Women should be informed of the limitations of routine ultrasound screening and that detection rates vary by the type of fetal anomaly, the woman’s BMI and the position of the unborn baby at the time of the scan.
• If an anomaly is detected during the anomaly scan pregnant women should be informed of the findings to enable them to make an informed choice of whether they wish to continue with the pregnancy or have a termination of pregnancy.
• Fetal echocardiography involving the four-chamber view of the fetal heart and outflow tracts is recommended as part of the routine anomaly scan.
• Routine screening for cardiac anomalies using nuchal translucency is not recommended.
• When routine ultrasound screening is performed to detect neural tube defects, alpha-fetoprotein testing is not required.
Screening for Down’s syndrome
• All pregnant women should be offered screening for Down’s syndrome. Women should understand that it is their choice to embark on screening for Down’s syndrome.
• The ‘combined test’ (nuchal translucency, beta-human chorionic gonadotrophin, pregnancy-associated plasma protein-A) should be offered to screen for Down’s syndrome between 11 weeks 0 days and 13 weeks 6 days.
• For women who book later in pregnancy, the most clinically and cost-effective serum screening test (triple or quadruple test) should be offered between 15 weeks 0 days and 20 weeks 0 days.
• When it is not possible to measure nuchal translucency, owing to fetal position or raised BMI, women should be offered serum screening (triple or quadruple test) between 15 weeks 0 days and 20 weeks 0 days.
• If a pregnant woman receives a screen positive result for Down’s syndrome, she should have rapid access to appropriate counselling by trained staff.
• The routine anomaly scan (at 18 weeks 0 days to 20 weeks 6 days) should not be routinely used for Down’s syndrome screening using soft markers.
• The presence of an isolated soft marker, with the exception of increased nuchal fold, on the routine anomaly scan should not be used to adjust the a priori risk for Down’s syndrome.
• The presence of an increased nuchal fold (6 mm or above) or two or more soft markers on the routine anomaly scan should prompt the offer of a referral to a fetal medicine specialist or an appropriate healthcare professional with a special interest in fetal medicine.
Screening for infections
• Asymptomatic bacteriuria: women should be offered routine screening for asymptomatic bacteriuria by midstream urine culture early in pregnancy. Identification and treatment of asymptomatic bacteriuria reduces the risk of pyelonephritis.
• Asymptomatic bacterial vaginosis: pregnant women should not be offered routine screening for bacterial vaginosis because the evidence suggests that the identification and treatment of asymptomatic bacterial vaginosis does not lower the risk of preterm birth and other adverse reproductive outcomes.
• Chlamydia trachomatis: at the booking appointment, healthcare professionals should inform pregnant women younger than 25 years about the high prevalence of chlamydia infection in their age group, and give details of their local National Chlamydia Screening Programme.
• Cytomegalovirus: the available evidence does not support routine cytomegalovirus screening in pregnant women and it should not be offered.
• Hepatitis B virus: serological screening for hepatitis B virus should be offered to pregnant women so that effective postnatal interventions can be offered to infected women to decrease the risk of mother-to-child transmission.
• Hepatitis C virus: pregnant women should not be offered routine screening for hepatitis C virus, because there is insufficient evidence to support its clinical and cost effectiveness.
• HIV: pregnant women should be offered screening for HIV infection early in antenatal care because appropriate antenatal interventions can reduce mother-to-child transmission of HIV infection.
• Rubella: rubella susceptibility screening should be offered early in antenatal care to identify women at risk of contracting rubella infection and to enable vaccination in the postnatal period for the protection of future pregnancies.
• Group B streptococcus: pregnant women should not be offered routine antenatal screening for group B streptococcus because evidence of its clinical and cost-effectiveness remains uncertain.
• Syphilis: screening for syphilis should be offered to all pregnant women at an early stage in antenatal care because treatment of syphilis is beneficial to the mother and baby.
• Toxoplasmosis: routine antenatal serological screening for toxoplasmosis should not be offered because the risks of screening may outweigh the potential benefits. Screening for clinical conditions
Gestational diabetes
• Screening for gestational diabetes using risk factors is recommended in a healthy population. At the booking appointment, the following risk factors for gestational diabetes should be determined:
• body mass index above 30 kg/m2
• previous macrosomic baby weighing 4.5 kg or above
• previous gestational diabetes (refer to Chapter 8.11, Diabetes in pregnancy (NICE clinical guideline 63, available from www.nice.org.uk/CG063)
• family history of diabetes (first-degree relative with diabetes)
• family origin with a high prevalence of diabetes.
• Women with any one of these risk factors should be offered testing for gestational diabetes.
• Screening for gestational diabetes using fasting plasma glucose, random blood glucose, glucose challenge test and urinalysis for glucose should not be undertaken.
Pre-eclampsia
• Blood pressure measurement and urinalysis for protein should be carried out at each antenatal visit to screen for pre-eclampsia.
• At the booking appointment, the following risk factors for pre-eclampsia should be determined:
• age 40 years or older
• nulliparity
• pregnancy interval of more than 10 years
• family history of pre-eclampsia
• previous history of pre-eclampsia
• body mass index 30 kg/m2 or above
• pre-existing vascular disease such as hypertension
• pre-existing renal disease
• multiple pregnancy.
• More frequent blood pressure measurements should be considered for pregnant women who have any of the above risk factors.
• The presence of significant hypertension and/or proteinuria should alert the healthcare professional to the need for increased surveillance.
• Hypertension in which there is a single diastolic blood pressure of 110 mmHg or two consecutive readings of 90 mmHg at least 4 hours apart and/or significant proteinuria (1+) should prompt increased surveillance.
• If the systolic blood pressure is above 160 mmHg on two consecutive readings at least 4 hours apart, treatment should be considered.
• All pregnant women should be made aware of the need to seek immediate advice from a healthcare professional if they experience symptoms of pre-eclampsia.
Preterm birth
• Routine screening for preterm labour should not be offered.
Placenta praevia
• Because most low-lying placentas detected at the routine anomaly scan will have resolved by the time the baby is born, only a woman whose placenta extends over the internal cervical os should be offered another transabdominal scan at 32 weeks. If the transabdominal scan is unclear, a transvaginal scan should be offered.
Fetal growth and wellbeing
• Symphysis–fundal height should be measured and recorded at each antenatal appointment from 24 weeks.
• Ultrasound estimation of fetal size for suspected large for gestational age unborn babies is of limited value in a low-risk population.
• Routine Doppler ultrasound should not be used in low-risk pregnancies.
• Fetal presentation should be assessed by abdominal palpation at 36 weeks or later, when presentation is likely to influence the plans for the birth. Routine assessment of presentation by abdominal palpation should not be offered before 36 weeks because it is not always accurate and may be uncomfortable. Suspected fetal malpresentation should be confirmed by an ultrasound assessment.
• Auscultation of the fetal heart may confirm that the fetus is alive but is unlikely to have any predictive value and routine listening is therefore not recommended. However, when requested by the mother, auscultation of the fetal heart may provide reassurance.
• The evidence does not support the routine use of antenatal electronic fetal heart rate monitoring (cardiotocography) for fetal assessment in women with an uncomplicated pregnancy and therefore it should not be offered.
• The evidence does not support the routine use of ultrasound scanning after 24 weeks of gestation and therefore it should not be offered.

Fig. 5.1.1 Antenatal care in the second trimester.
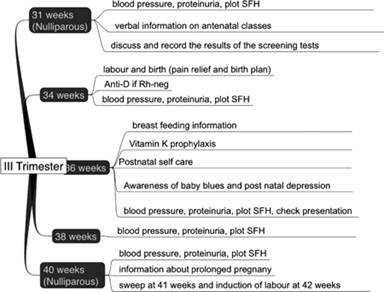
Fig 5.1.2 Antenatal care in the third trimester. Antenatal appointments
The schedule above, which has been determined by the purpose of each appointment, presents the recommended number of antenatal care appointments for women who are healthy and whose pregnancies remain uncomplicated in the antenatal period: 10 appointments for nulliparous women and seven for parous women. These appointments follow the woman’s initial contact with a healthcare professional when she first presents with the pregnancy and from where she is referred into the maternity care system.
The timing of the visits and care at each visit is summarized in Figs 5.1.1 and 5.1.2. Further reading
NICE Guidance. Antenatal care: routine care for healthy pregnant women. Ref CG62.
Fortner KB (ed.). The John Hopkins manual of gynecology and obstetrics. Philadelphia: Wolters Kluwer 2008.
Steven G, Gabbe JRN, Leigh Simpson J (eds). Obstetrics normal and problem pregnancies. New York: Churchill Livingston 1996.
Booking
Antenatal care begins when the pregnancy is registered with the midwife or GP. The vast majority of the patients would have had an ultrasound scan from the early pregnancy unit before registering with their GP. This is followed by a booking visit with the community midwife and is probably the most important visit in planning care during the pregnancy.
The booking visit is defined as the initial meeting between the pregnant woman and a professional from the maternity services.
The booking appointment or booking visit is the first official check-up in pregnancy. The term booking comes from the days when women literally had to book themselves a hospital bed for labour! It may take place in the woman’s home, the GP’s surgery or at the hospital antenatal clinic and usually consists of an elaborate interview with the midwife using a computerized booking form.
The aim of the booking visit is
• to introduce a woman and partner to the maternity services
• to assess the physical, social, psychological and cultural needs of the woman and family to plan future care
• to give information that allows the woman to explore the available options for care and make informed choices
• to identify risk factors and deviations from normal. Timing of the booking visit
The National Institute for Health and Clinical Excellence (NICE) recommends that the booking appointment should take place ideally by 10 weeks of pregnancy so that the mother has the time to arrange any first trimester screening tests. The factors that affect the timing of the visit are mainly the hospital policies and the time of diagnosis of the pregnancy. Studies have shown that ethnic minority women and multigravid women who smoke usually book their pregnancies much later than primigravid Caucasian women. Management at the booking clinic
At the booking visit a detailed history is taken, risk factors identified and appropriate referrals arranged. The details of the history include previous menstrual history, including contraception, smear tests and obstetric history to identify previous high-risk pregnancies. A detailed medical, family, social and personal history with an aim to enumerate factors that might affect the current pregnancy is taken. The first menstrual period is confirmed and the estimated date of confinement is also confirmed or amended based on initial dating scans. Part 2 deals with the history and examination of a pregnant woman.
The visit involves examination and screening for disorders such as anaemia, haemoglobinopathies, Rhesus isoimmunization. Rubella status is checked. Screening for infections such as syphilis, hepatitis B and HIV, if recognized and treated early, makes a huge difference to the outcome. This visit also provides an ideal opportunity for the women to discuss any anxieties she may have and to provide information on maternity benefits and statutory rights (Fig. 5.2.1). Assessment of risk
Structured maternity records with check lists and computerized data collection systems ensure that important questions are asked and risk factors identified.
The aim of risk scoring in pregnancy is to permit the classification of women into different categories for which appropriate management strategies can be implemented. Other benefits include defining populations for epidemiological purposes, allocation of resources and aid in audit and teaching. The main scores are designed to predict those who are likely to have adverse outcomes, such as perinatal death, small for gestational age, preterm labour and delivery, and perinatal asphyxia. Risk scoring tends to give a simplistic and inflexible view with the danger of ‘ignoring’ low-risk women. Computerized scoring systems are not widely in use to predict the likelihood of an adverse outcome, as their use has not been associated with the reduction in adverse outcomes. They also carry a risk of introducing interventions and treatments that may be of unproven value. Lifestyle advice
The booking visit gives the opportunity to educate women regarding antenatal care, lifestyle and minor ailments. Information is given on dietary requirements, exercise during pregnancy, parent craft education programmes and antenatal classes. General advice on healthy eating, folic acid and avoidance of food that may cause infections, e.g. uncooked meat and toxoplasmosis, is reiterated.
Smoking and alcohol cessation advice should be offered as appropriate. Identifying domestic violence at this stage may help the health professional to introduce appropriate safety measures to mother and the baby. Tests performed during the booking visit
Routine tests
Dating and a nuchal scan
A first trimester ultrasound scan, for pregnancy dating and measurement of nuchal translucency is performed between 10 and 14 weeks. With the recent guidelines for antenatal screening, nuchal translucency measurements are combined with serum markers such as human chorionic gonadotrophin (HCG) and pregnancy associated plasma protein-A (PAPP-A) as a screening test for trisomy 21. This combined test increases the sensitivity of Downs’s syndrome screening to 80%, retaining the false-positive rate at 5%.
Haematological investigations
A full blood count and haemoglobin in early pregnancy help to identify those with anaemia, exclude haemoglobinopathy, and to compensate them with iron so that they can cope with the physiological dilutional anaemia which occurs in pregnancy. Many women from ethnic minorities have low booking haemoglobin and with increasing gestational age they become profoundly anaemic. Anaemic patients at booking should be investigated with assessment of ferritin, total iron binding capacity and serum B12.
Blood grouping and screening for antibodies at booking identifies women who are rhesus negative and those at risk of Rh isoimmunization. The incidence of Rh immunization has dramatically fallen over the last 30 years since the advent of anti-D. Despite screening for antibodies at 28 and 34 weeks and administration of anti-D prophylactically a small number of Rh-negative women still develop Rh antibodies. Screening for red cell antibodies should be repeated in all pregnant women and in every pregnancy as there may be other clinically significant antibodies as a consequence of previous pregnancy or blood transfusion. Antibody screening is performed to detect the presence of antibodies that may put the baby at risk of haemolytic disease.
Screening for the haemoglobinopathies
Most hospitals perform these tests routinely in all patients. Given the increasing incidence of mixed populations, routine testing for haemoglobinopathies may be justified.
Microbiological investigations
These include serum screening for evidence of immunity to rubella and screening for infections like hepatitis B or HIV. Rubella infection in early pregnancy can have serious consequences to the fetus. In an attempt to reduce the incidence of congenital rubella, vaccination for rubella was introduced. Despite vaccination, the data show that a minority of women will not be immune to rubella. And it is recommended that all women should be tested for rubella in pregnancy, and if negative postnatal vaccination is recommended.
HIV infection in the mother has implications for the mother and the fetus, and hence it is essential to test for HIV infection in pregnancy. Early recognition and treatment reduces the mother to child transmission of the HIV virus quite significantly.
Screening for hepatitis B is aimed to determine if the patient has been infected and if she is a potential risk of contracting infection to her partner or to healthcare professionals. Hepatitis B surface antibody is tested for initially and if positive, core antigen ‘e’ status is tested to determine the potential infectivity. Combination of active and passive immunization is undertaken in the neonate if the mother is found to be ‘e’ positive.
Screening for syphilis is performed as routine. Around 250 cases are detected annually in the UK. The rational is that early treatment of the disease can prevent congenital syphilis in neonates.
Screening for urinary tract infection
Urine dipstick is carried out to check for glucose, proteinuria, ketonuria, and nitrites. At the booking visit a urine specimen is sent for culture to detect and treat asymptomatic bacteriuria. Asymptomatic bacteriuria if present can lead to urinary tract infections in 15%. It also increases the risk of preterm labour. The urine dipstick is tested for glucose and protein, and if positive checking blood sugar and blood pressure and additional tests may be appropriate.

Fig. 5.2.1 Antenatal care in the first trimester in graphic presentation.
Specific tests
Specific risk-oriented tests may be done. For example, if there is a history of hypertension, a renal function test would be appropriate, and history of diabetes should prompt testing fasting blood sugar and Hb A1C. Arrangement of appropriate referrals
Based on the history, examination and results of investigations, an individualized care plan needs to be compiled. The vast majority will be low risk and continued midwifery care is appropriate. If a medical disorder is diagnosed, appropriate referral is made to optimize the management plan. Further reading
Fortner KB (ed.). The John Hopkins manual of gynecology and obstetrics, 3 edn. Philadelphia: Wolters Kluwer 2008.
Kupek E, Petrou S, Vause S, Maresh M. Clinical, provider and socio-demographic predictors of late initiation of antenatal care in England and Wales. Br J Obstet Gynaecol 2000;109:265–73.
Robson J, Boomla K, Savage W. Reducing delay in booking for antenatal care. J R Coll Gen Pract 1986;36:274–5.
Stenhouse EJ, Crossley JA, Aitken DA, et al. First-trimester combined ultrasound and biochemical screening for Down syndrome in routine clinical practice. Prenat Diagn 2004;24:774–80.
Steven G, Gabbe JRN, Joe Leigh Simpson (eds). Obstetrics normal and problem pregnancies, 3rd edn. New York: Churchill Livingston 1996.
Breastfeeding
Exclusive breastfeeding until around 6 months of age, followed by the introduction of solids with continued breastfeeding, is considered to be the optimal nutritional start for the newborn infant. It has important health benefits for both mother and baby. Breastfeeding is often accompanied by challenges, and mothers require considerable help and support from healthcare professionals. Anatomy of breast
Each breast is divided into 15–20 lobules by fibrous tissue septae that radiate from the centre (Fig. 5.3.1). Each lobe further subdivides into lobules and consists of fibrofatty stroma, alveoli, and ductules draining the alveoli. Each alveolus is lined by columnar epithelium, where milk secretion occurs. A network of myoepithelial cells surrounds the alveoli and the smaller ducts. Contraction of these cells squeezes the alveoli and ejects the milk into the ductules. Each lobe is drained by the lactiferous duct, formed by the union of increasingly larger ductules and ducts. Each lactiferous duct dilates to form ampulla before converging onto the nipple. Milk is stored in the ampulla before release and secreted outside through nipple pores. Physiology of lactation
For successful breastfeeding to ensue, breasts go through three stages: mammogenesis, lactogenesis, and galactopoiesis.
Mammogenesis
This takes place in two further stages: stage I around puberty and stage II during pregnancy, parturition and lactation. Normal breast tissue contains three types of lobules. Formation of type I lobules begins with puberty. Under the influence of oestrogen and progesterone they sprout new alveolar buds and evolve to more mature type 2 and 3 lobules. Further maturation does not occur until pregnancy. During pregnancy they reach their maximum branching capability and form secretory acini, which are the terminal outgrowths of the ducts. These matured lobules seen in pregnancy and lactation are called type 4 lobules. Early pregnancy is characterized by ductular proliferation and later pregnancy by secretory activity. All these processes continue during lactation, the predominant event being milk production.

Fig. 5.3.1 Structure of the breast. Reproduced from Breast cancer, the facts, Saunders and Jassal, 2009, with permission from Oxford University Press.
Lactogenesis
Lactogenesis takes place in two stages: secretory initiation and secretory activation. Secretory initiation begins during the second half of pregnancy and is mediated by high levels of circulating progesterone. During pregnancy only minimal amounts of milk are formed in the breast, despite high levels of lactogenic hormones, prolactin, and human placental lactogen (HPL).
This is due to the inhibitory effect of oestrogen and progesterone. After delivery there is rapid decline in both these hormones and prolactin begins its milk secretory activity. This stage is known as secretory activation and occurs in women between 3 and 7 days postpartum. Secretory activation is delayed in primipara, after Caesarean and stressful vaginal deliveries, retained placental fragments and diabetes.
Galactopoiesis
This is the process of maintenance of lactation. This is regulated by the interaction of various factors, the most important being emptying of the breast by the infant’s suckling. Hormones such as oxytocin, prolactin and feedback inhibitor of lactation (FIL) play their role.
Failure to empty breasts at regular intervals leads to an increase in intramammary pressure. First, this obstructs blood flow and the supply of stimulatory hormones and nutrients to the breast. Second, increased intramammary pressure disrupts the synthesis and secretion of milk components. Third, FIL is synthesized by mammary epithelial cells in response to increased intramammary pressure. This downregulates prolactin receptors and decreases milk supply. Milk production is also dependent on infant demand.
The suckling of the baby sends afferent impulses through the nerve endings in the nipple areola complex to the pituitary gland, resulting in increased secretion of prolactin and oxytocin. Prolactin acts on the alveoli and increases the production of milk proteins. This is known as the suckling reflex. Oxytocin acts on the myoepithelial cells aiding expulsion of milk into the ducts from the alveolar lumen and out through the nipple. At the same time the ducts expand rapidly to facilitate milk flow. This is termed the milk ejection reflex and is recognized by the mothers as the milk let down. The milk ejection reflex is inhibited by maternal anxiety. Maternal benefits of breastfeeding
Breastfeeding provides both short and long-term benefits to the mother. Oxytocin released as a result of suckling accelerates uterine involution. In a randomized controlled trial, mothers who initiated frequent feedings immediately after delivery of the placenta experienced less blood loss than those who initiated later. Weight loss after pregnancy is enhanced by prolonged breastfeeding. Prolonged breast-feeding confers contraceptive benefits. The conception risk during lactational amenorrhoea is only 1–2% if three criteria apply: (1) amenorrhoea, (2) full lactation, (3) less than 6 months postpartum. It has been suggested that breastfeeding enhances maternal–infant bonding. Long-term benefits of breastfeeding include a decreased risk of developing breast cancer and ovarian cancer. It remains unclear whether lactation reduces the risk of osteoporosis, and further studies are required. Infant benefits of breastfeeding
Human milk is the ideal nutrient for term infants as it confers numerous benefits with respect to nutrition, gastrointestinal function and protection against illnesses.
Breast milk is secreted at body temperature. It generally does not need storage and is produced as and when the baby requires it. This obviates the inconveniences of warming and cooling formula, storage of milk and sterilization of bottles. Breastfeeding reduces the risk of accidental scalding or burns. Suckling helps the development of muscular coordination of the jaw and teeth of infant.
Breast milk is produced in the correct amount and is therefore not wasted. It comprises fore milk and hind milk, which vary in their fat content. The foremilk has low fat content and does not satiate baby till adequate intake is made. Hind milk occurs after the initial release of milk and contains higher levels of fat, and it is necessary for weight gain. Hind milk also retards gastric motility and aids absorption of the majority of milk lactose. Formula milk has excesses or deficiencies in substances and is prone to accidental contamination.
Breastfeeding during the first 13 weeks of life confers protection against gastrointestinal illnesses that persists beyond the period of breastfeeding itself. The risk of hospitalization for diarrhoea is reduced in infants exclusively breastfed compared with infants who never breastfed. Breastfed infants have reduced incidence of respiratory illnesses, urinary tract infections, and otitis media.
Neonatal necrotizing enterocolitis (NEC) is a major cause of morbidity in preterm infants. Human milk is known to decrease colonization of the bowel by pathogenic bacteria, promotes growth of non-pathogenic flora and maturation of the intestinal barrier. In addition it contains anti-inflammatory agents such as interleukin-10 and immunoglobulins (Ig) such as IgG and IgA. As a result it reduces inflammation-mediated ischaemic bowel injury leading to NEC.
Breastfed infants have enhanced host defence mechanisms. This is because maternal antibodies are transferred through breast milk. Enteromammary and bronchomammary immune systems have a major role to play in the protective nature of breast milk. When the mother is exposed to pathogens via her respiratory or gastrointestinal tract, protective antibodies are synthesized in the breast and secreted in the milk. Thus the infant receives passive immunity to the continuing exposure of antigens.
In addition milk proteins like lactoferrin and lysozyme have antimicrobial activity. Human milk also contains neutrophils, lymphocytes, and macrophages, which contribute to cell-mediated immunity.
Breastfeeding provides long-term benefits to infants. Meta-analysis has shown a 32% reduction in obesity in patients who were breastfed for more than 9 months. Post-breastfeeding protection appears to increase with the duration of breastfeeding. Breast-fed compared with formula-fed infants appear to have a decreased risk of developing Type 1 and Type II diabetes mellitus. A systematic review has shown that breastfeeding is associated with increased mean total cholesterol and low-density lipoprotein levels in infancy but lower levels in adulthood/adult life. This along with reduction of obesity and diabetes may have long-term benefits for cardiovascular health. Breast milk being immunologically active is thought to reduce the incidence of allergic diseases such as atopic dermatitis, allergic rhinitis, and asthma. However, most of these studies are observational and further data are required. Combining data from the UK Childhood Cancer Study (UKCCS) with results from other published studies showed a small reduction in the odds ratios for leukaemia, Hodgkin’s disease, non-haematological cancers, and all childhood cancers combined, associated with ever having been breastfed. Several studies have suggested that breastfeeding improves cognitive development in childhood and adolescence. Economic benefits of breastfeeding
There are clear economic advantages to family and society as a whole. There is reduction in expenditure on formula as well as healthcare expenses. The cost savings from long-term benefits of breastfeeding such as reducing the incidence of chronic illnesses in children and adults and reduction in cancers in both mothers and children are substantial. Initiation and maintenance of breastfeeding
Breastfeeding should be started within the first hour after delivery. Skin-to-skin contact immediately after delivery helps to start breastfeeding off. Subsequent feedings should be on demand. Feeding on demand means that feedings are initiated in response to behavioural changes that indicate hunger (feeding cues). Examples of feeding cues are movement of the hands towards mouth, sucking on fists and fingers, fussiness, agitation and crying. ‘Rooming in’ means the baby stays with mother all the time. This increases the mother’s ability to understand and respond to feeding cues. Feeding the infant in response to early cues is optimal. Voluntary release of the nipple, relaxation of facial muscles and falling asleep signal satiety.
The average frequency of breastfeeding is 8–12 times per day in the first 1–2 weeks postpartum, which reduces to 7–9 times per day by 4 weeks. During the first postpartum week the duration between feeds should not be more than 4 hours. The average duration of feed on each breast is 10–15 minutes soon after birth and is dependent on efficiency of milk transfer. As efficiency improves, duration falls to 8–10 minutes by 4 weeks.
Breastfeeding mothers should have a balanced diet which is high in calories, protein, vitamins and minerals. There is an excess demand of at least 700 calories and 20 g of protein per day compared with the non-pregnant state. Daily requirements of calcium are increased by three times and vitamin A by one and a half times that of the non-pregnant state. An adequate fluid intake is important for successful breastfeeding. Latch-on
The baby’s gums should completely bypass the nipple and cover approximately 2.5 cm of the areola behind the nipple and this should form a tight seal (Fig. 5.3.2). The appearance of an adequate latch-on includes
• an angle of approximately 120 between the top and bottom lip
• the lower lip (and, to a lesser extent, the upper lip) turned outward against the breast
• the chin and nose in close proximity to the breast
• full cheeks
• the tongue extends over the lower dental ridge and is in visible contact with the breast if the lower lip is pulled away (Hopkinson and Schanler ‘Breast in the perinatal period’).
Colostrum is the first stage of breast milk that occurs during pregnancy and lasts for several days after the birth of the baby. It is either yellowish or creamy in colour. It is of higher density and lower volume than the milk that is produced later in breastfeeding. Colostrum is high in protein, fat-soluble vitamins, minerals and immunoglobulins. Colostrum may be scanty in amount but is very important for passive immunity. A good amount of milk production occurs by 3–5 days. Reliable indicators of sufficient intake are weight gain, clearance of meconium and increasing urine output. Normal infants lose about 5–7% of birth-weight by 5 days of age. They regain their birthweight by 1–2 weeks. Infants gain 15–40 g per day, once breastfeeding is established. Meconium is cleared by the third day and the majority of infants have four or more stools and at least six wet diapers per day. Any deviation from this should be brought to the attention of a healthcare professional.

Fig. 5.3.2 Correct ‘latch-on’. Baby-friendly hospital
The Baby-Friendly Hospital Initiative was launched by the World Health Organization (WHO) and the United Nations Children’s Fund in 1991 to improve breastfeeding rates. Hospitals can be designated baby-friendly if they comply with the following 10 steps:
• Have a written policy on breastfeeding that is communicated routinely to all staff.
• Train all healthcare staff in the skills needed to implement the policy.
• Inform all pregnant women of the benefits and management of breastfeeding.
• Help mothers start breastfeeding within 1 hour after birth.
• Show mothers how to breastfeed and maintain lactation, even if they are separated from their infants.
• Give newborns only breast milk, unless other feedings are medically indicated. Hospitals must pay a fair market price for formula and feeding supplies.
• Allow mothers and infants to remain together at all times.
• Encourage breastfeeding on demand.
• Provide no pacifiers or artificial teats to nursing infants.
• Foster the establishment of breastfeeding support groups and refer mothers to them.
A randomized controlled trial has shown that antenatal breastfeeding education and postnatal lactation support, as single interventions based in hospital, both significantly improve rates of exclusive breastfeeding up to 6 months after delivery. Postnatal support was marginally more effective than antenatal education. Hence ongoing post-partum support for patients in the form of house visits, telephone contacts with breastfeeding counsellors and peer support groups is very important in the maintenance of breastfeeding. Inadvertent promotion of artificial formula appears to reduce the number of women exclusively breastfeeding at all times. Problems encountered during breastfeeding
Engorgement
Breast engorgement is the painful overfilling of the breasts with milk. This is usually caused by an imbalance between milk supply and infant demand. National surveys have shown that painful breasts are the second most common reason for giving up breastfeeding in the first 2 weeks after birth in the UK. One factor contributing to such pain can be breast engorgement. Early engorgement coincides with Stage II lactogenesis and typically occurs 24–72 hours postpartum. In the majority of cases, once feeding is established this resolves spontaneously. Poor latch-on interferes with the infant’s ability to empty the breast and the consequent engorgement makes further latch-on difficult. Late engorgement occurs when there is inadequate emptying of the breasts due to disruption of the normal routine of breastfeeding for various reasons and the consequent accumulation of milk.
Frequent emptying of breasts is critical to prevent and treat engorgement. It is important to ensure satisfactory latch-on from the start. Breastfeeding should not be discontinued. Manual expression or breast pumps can be used if the baby is unwilling to nurse. A Cochrane database systematic review has shown that the anti-inflammatory agent serrapeptase and hand massage helps to relieve symptoms. Icepacks, cool compresses and simple analgesics are recommended for pain relief.
Galactocoeles/plugged ducts (non-infective mastitis)
A plugged duct is a sore, tender lump or knotty area in the breast. It occurs when a milk duct is not draining well and inflammation builds up. It is distinguished from mastitis by the absence of signs of systemic infection. Predisposing factors are mismatch between demand and supply and poor latching. Unrelieved plugged ducts may lead to galactocoeles, which are milk retention cysts. They are initially filled with milk and later replaced by thick, creamy or oily material. Galactocoeles can be visualized on ultrasound.
Management includes frequent emptying of breasts. Ensure that baby is properly latched on and well positioned in a way that the affected milk ducts are thoroughly drained with each feeding. Nurse as often as possible on the affected side to help drain the clogged duct. Gently massaging the lumpy area in a circular motion, starting behind the lump and working towards the nipple, can help loosen the plug. Apply warm compresses and/or stand in the shower with the spray directly on the sore area. This helps to unclog the duct. If the pain of a plugged duct or the lump does not go away within 2–3 days, appropriate advice should be sought. Galactocoeles that do not resolve are treated with needle aspiration.
Mastitis and breast abscess
Mastitis is an infection of the breast caused by bacteria. Staphylococcus aureus, streptococci and Escherichia coli are the common aetiological agents. Most studies agree that around 10% of all breastfeeding mothers are affected by mastitis. Left untreated, non-infectious mastitis can progress to infectious mastitis. This may be due to bacteria infecting the milk that remains in the breast tissue. Traumatized nipples are at risk of superficial infection that may lead to mastitis. Mastitis usually affects only one breast, causing it to become painful, red and swollen. It is associated with fever >38°C, myalgia, chills, malaise and flue-like symptoms.
Infectious mastitis requires prompt treatment to prevent more serious complications such as breast abscess. Antibiotic treatment should be started with flucloxacillin for 10–14 days. Alternatives such as cephalexin and amoxicillin are used if no response is seen in 24–48 hours. Breastfeeding should not be stopped and breasts should be emptied either manually or by pumps if the infant cannot relieve breast fullness. Supportive measures like bed rest and anti-inflammatory agents are helpful. Recurrent mastitis can result from inappropriate or incomplete antibiotic therapy or failure to resolve underlying problems in lactation management.
Breast abscess develops in 5–11% of women with mastitis and management is antibiotic therapy and drainage.
Nipple-related problems
Sore nipples are probably the most common difficulty mothers have when breastfeeding. Sore nipples can be due to nipple sensitivity, which is a normal phenomenon, or secondary to trauma. Nipple sensitivity peaks on approximately the fourth postpartum day and resolves by the seventh postpartum day. It typically subsides 30–60 seconds after suckling begins. It is due to enhanced lactational hormones like prolactin and oxytocin.
The commonest cause of trauma to nipples is poor latch-on techniques and ineffective sucking. The pain due to trauma in contrast to normal sensitivity persists throughout the nursing episode. Signs of poor latch-on include:
• contact between the upper and lower lip at the corners of the mouth;
• sunken cheeks;
• clicking sounds that correspond to breaking suction;
• tongue not visible below the nipple when the lower lip is pulled down;
• creased nipple following nursing (Hopkinson and Schanler ‘Breast in the perinatal period’).
Persistent painful latch-on should be brought to the attention of a lactation consultant. Traumatized nipples are at risk of infection predominantly by candida and staphylococci.
Sore nipples should be cleansed with clean water or saline and left to air dry after every nursing. Changing positions each time of nursing helps to avoid pressure on the same part of the nipple. Human milk has natural healing properties and emollients, and hence application of breast milk after feeding helps. Wearing a nipple shield during nursing will not relieve sore nipples. They actually can prolong soreness by making it hard for the baby to learn to nurse without the shield. Tight bras or clothes that are too tight and put pressure on the nipples should be avoided. Change Nursing pads should be changed often to avoid trapping in moisture. Application of emollients like lanolin helps to maintain moisture and facilitate healing. A combination of antibiotic (Muciprocin), antifungal (Miconazole) and a steroid is recommended if initial steps fail.
Bloody nipple discharge is seen in some women during the first few days postpartum. This is due to vascularization of the ducts during pregnancy and resolves spontaneously. Bloody milk during lactation is often detected when the infant’s stool is mixed with blood. The source of bleeding may be cracked nipples. A rare cause is intraductal papilloma and in the absence of an obvious source of bleeding this should be suspected and milk sent for cytological analysis. Contraindications to breast feeding
Few contraindications to breastfeeding exist. HIV and breastfeeding
The major mode of acquisition of HIV in children worldwide is through mother-to-child transmission. This happens antenatally, intrapartum and postpartum through breastfeeding. Breastfeeding alone accounts for 30–50% of mother-to-child transmission and doubles the rate of transmission. In developed countries breastfeeding is not advisable in women with HIV as the benefits of not breastfeeding outweigh the risks. The combination of antiretroviral therapy, elective Caesarean delivery, and avoidance of breastfeeding has reduced perinatal transmission to less than 2% in developed countries.
In the developing world, eliminating the risk of HIV transmission by stopping breastfeeding exposes children to different risks: increased exposure to other life-threatening infections, especially in the first year of life and malnutrition if replacement feeding is inadequate. In addition, formula may not be easily available, affordable or culturally acceptable. To date there are no proven strategies known to reduce the risk of HIV transmission during breastfeeding for those HIV-infected women who opt to breastfeed in developing countries. Breastfeeding with extended prophylaxis with antiretrovirals and vaccination of infants are currently the subject of research. The WHO recommends that women be counselled about the risk of HIV transmission through breastfeeding. When replacement feeding is affordable, feasible, acceptable, sustainable and safe, avoidance of all breastfeeding by HIV-infected mothers is recommended. When replacement feeding is not possible, then exclusive breastfeeding is recommended during the first months of life, with the time of stopping being determined by individual circumstances. Inborn errors of metabolism
Galactosaemia is an absolute contraindication for breast-feeding as infants are unable to metabolize galactose, a component of breast milk. As a result galactose accumulates in the blood with adverse consequences. Breastfeeding is not contraindicated with other inborn errors of metabolism such as phenylketonuria. Babies suffering from phenylketonuria may be breastfed while their phenylalanine levels are monitored. Drug abuse and other medications
Maternal drug abuse is a contraindication to breastfeeding. In the mother with an ongoing illicit drug abuse problem, drugs are secreted in breast milk. Hence the risks posed to the infant are substantial and outweigh the benefits of breastfeeding in most cases.
Most therapeutic drugs are compatible with breastfeeding. Administration of some drugs harms the infant whereas others have little effect. Toxicity to the infant can occur if the drug enters the milk in pharmacologically significant quantities. Some drugs like bromocriptine inhibit lactation. As a general rule anticancer drugs, certain anti-convulsants, ergot alkaloids, amiodarone, iodides and radiopharmaceuticals are avoided. Clinicians should consult reliable sources before prescribing drugs during breastfeeding.
In summary, exclusive breastfeeding is the ideal form of feeding infants for the first 6 months after birth as it confers invaluable benefits to mother and baby. It meets all the nutritional requirements for the infants in the first 6 months of life. The WHO advises that partial breastfeeding to be continued for at least 1 year or up to 2 years. Parental education and support is vital in initiation and maintenance of breastfeeding. It is not without its own challenges and healthcare professionals dealing with breastfeeding women should have the necessary knowledge and skills to advise and help mothers overcome these challenges. There are few contraindications to breastfeeding. Further reading
Breastfeeding and childhood cancer. Br J Cancer 2001;85:1685–94.
Harder T, Bergmann R, Kallischnigg G, Plagemann A. Duration of breastfeeding and risk of overweight: a meta-analysis. Am J Epidemiol 2005;162:397–403.
Hopkinson J, Schanler RJ. Breastfeeding in the perinatal period. Uptodate version 16.2: www.uptodate.com
Hopkinson J, Schanler RJ. Common problems of breastfeeding in the postpartum period. Uptodate version 16.2.
Hopkinson J, Schanler RJ. Physiology of lactation. Uptodate version 16.2.
Howard C, Howard F, Lawrence R, et al. Office prenatal formula advertising and its effect on breastfeeding patterns. Obstet Gynecol 2000;95:296–303.
Howie PW, Forsyth JS, Ogston SA, et al. Protective effect of breastfeeding against infection. BMJ 1990;300:11–15.
Millennium Cohort Study. Paediatrics 2007;119:e837–42.
Owen CG, Martin RM, Whincup PH, et al. Does breastfeeding influence risk of type 2 diabetes in later life? A quantitative analysis of published evidence. Am J Clin Nutr 2006;84:1043–54.
Owen CG, Whincup PH, Odoki, K, et al. Infant feeding and blood cholesterol: a study in adolescents and a systematic review. Paediatrics 2002;110:597–608.
Quigley MA, Kelly YJ, Sacker A. Breastfeeding and hospitalization for diarrhoeal and respiratory infection in the United Kingdom.
Schanler RJ. Infant benefits of breastfeeding. Uptodate version 16.2.
Schanler RJ. Maternal and economic benefits of breastfeeding. Uptodate version 16.2.
Sobhy SI, Mohame NA. The effect of early initiation of breastfeeding on the amount of vaginal loss during the fourth stage of labour. J Egypt Public Health Assoc 2004;79:1–12.
Su LL, Chong YS, Chan YH, et al. Antenatal education and postnatal support strategies for improving rates of exclusive breastfeeding: randomised controlled trial. BMJ 2007;335:596.
Ten steps to successful breastfeeding. www.unicef.org/newsline/tenstps.htm
Dating in pregnancy
Estimation of gestational age and the expected date of delivery are valuable to the expecting couple to arrange for the arrival, but also are important in the diagnosis of intrauterine growth restriction of the fetus and for management of high-risk pregnancy. Clinical dating
Estimation of gestational age by last menstrual period
Gestational age (GA) is about 280 days calculated from the first day of the last normal menstrual period (LMP). If the periods are regular, common practice is to calculate the expected date of delivery by Naegele’s formula. Without a history of regular, predictable, cyclic, spontaneous menses that suggest ovulatory cycles, accurate dating of pregnancy by history and physical examination is difficult. Unfortunately 30% of patients do not fulfil the criteria, making estimation of expected date of delivery (EDD) based on LMP unreliable1. If the interval of cycles is longer, the number of extra days is added to the EDD, and if shorter, the days are subtracted from the EDD. One-quarter of patients either don’t remember LMP or give it inaccurately. The last menstrual period is even more inaccurate if conception occurs during lactation amenorrhoea or immediately after stopping oral contraceptive pills. Estimation of EDD from last menstrual period becomes reliable if the patient remembers the date of fruitful coitus.
Estimation of GA by quickening
A crude estimate of the EDD can be derived if the woman remembers the exact date of quickening. Quickening appears in a multigravida at 16 weeks and in a primigravida at 18 weeks. Adding 24 weeks in a multigravida and 22 weeks in a primigravida from the date of quickening can estimate EDD. The reliability of EDD estimated in this way is highly inaccurate especially in primigravid mothers, as quickening is very subjective and varies with individual perception of fetal movements.
Estimation of GA by objective signs
Pelvic examination: the size of the uterus gives a rough guidance to the gestational age. At 12 weeks the uterus becomes an abdominal organ and at 24 weeks reaches the umbilicus. At 36 weeks the uterus reaches the xiphisternum and falls forwards because of lightening. Maternal obesity, observer experience, position of the uterus, amount of amniotic fluid, multiple gestation, uterine myomatosis and fetal growth disorders are variables that make assessment of gestation by uterine size unreliable.
In some patients EDD can be established by the date of the first positive pregnancy tests. It could be reliable if the pregnancy test was carried out on the fifth week of amenorrhoea. Clinical dating is inaccurate and if feasible all women should have an ultrasound in the first trimester to confirm dating.
Ultrasound estimation of GA
Sonographic measurements of fetal ultrasound parameters are the basis for accurate determination of gestational age and detection of fetal growth abnormalities. Selection of the most useful single biometric parameter depends on the timing and purpose of measurement and is influenced by specific limitations (Degani 2001).
First trimester
In the early first trimester, when no structures are visible within the gestational sac, GA may be estimated from the sac diameter. A common method is to measure the mean sac diameter (MSD) by calculating the mean of the three sac diameters. An alternative simpler method is to add 30 to the sac size in millimetres, to give GA in days. By the time the embryo becomes visible on ultrasound the sac diameter is no longer accurate in estimating gestational age. GA in the first trimester is usually calculated from the fetal crown–rump length (CRL) (Fig. 5.4.1). This is the longest demonstrable length of the embryo or fetus, excluding the limbs and the yolk sac. CRL measurement is used in embryos from 20 to 60 mm as the embryo loses the extreme flexion at the neck so that its greatest length becomes the CRL measurements (Goldstein 1991). The correlation between CRL and GA is excellent until approximately 12 weeks’ amenorrhea. The GA estimate has a 95% confidence interval of ±2–3 days before 11 weeks and 2–5 after 11 weeks.
Second trimester
Fetal biometry in the second trimester can yield acceptably accurate estimates of GA from 12 to approximately 22 weeks of amenorrhea. The best parameters are the biparietal diameter (BPD) and the head circumference (HC), which are virtually linearly related to GA. BPD measurements in the second trimester predict dates within a margin of ±7–11 days. BPD measurements before 20 weeks estimate GA by ±7 days. In cases where BPD may be altered because of head compression, head circumference has the advantage of being shape independent and can be used effectively as an alternative means of establishing gestational age. The femur length (FL) can also be used and is nearly as accurate as head measurements. The range of dates varies more with FL as gestation advances than with BPD. Racial differences in FL are significant, but differences in HC are not. GA estimates by the BPD or HC have a 95% confidence interval of ±8 days.
Third trimester
Fetal biometry in the third trimester is subject to much greater individual size variations than in the second trimester. Its accuracy for GA assignment is reduced considerably, and estimates may have confidence intervals of ±3 weeks. There is significant improvement in ultrasound estimation of EDD when two or more parameters were used, however the approach should be individualized excluding parameters that are suspected to be abnormal4.
When CRL measurement is not available, gestational age should not be changed unless the discrepancy between menstrual and second trimester ultrasound dating is 9 days or more, as this policy would result in the smallest proportion of incorrect adjustments. In the majority of cases, the gestational age of the fetus and the expected date of delivery will be established with a single ultrasound examination between 18 and 24 weeks if the results agree with clinical information. If there is more than a 1-week discrepancy between the clinical dating and the results of the ultrasound examination the ultrasound should be repeated 4 weeks later. If the second set of ultrasound measurements agrees with the first examination, the gestational age and the EDD become clearly established. If the second set of measurements deviate more than 1 week from the first set, abnormality in fetal growth should be suspected and the EDD determined by the first ultrasound examination should be used.

Fig. 5.4.1 Measurement of crown rump length for dating pregnancy. Reproduced from The Oxford handbook of obstetrics and gynaecology, Colins, Arulkumaran, Hayes, Jackson, and Impey, 2008, with permission from Oxford University Press.
Reliability of EDD
Good reliability
• Based on CRL in the first trimester is the most accurate.
• Women with adequate clinical information plus ultrasound examination between 16 and 24 weeks, indicating that the fetal measurements are in agreement with the clinical estimation of gestation.
• Women with inadequate or incomplete clinical information, but two ultrasound examinations between 16 and 24 weeks show linear fetal growth with the expected date of confinement.
Acceptable reliability
• Women who provide adequate clinical information and one confirming ultrasound examination obtained after 24 weeks of gestation.
• Women with inadequate or incomplete clinical information but two or more ultrasound examinations show adequate growth and similar expected date of confinement.
Poor reliability
Based on clinical history with none of those measurements listed above (Arias 1988). Further reading
Cunningham G (ed.). Williams obstetrics, 22nd edn. New York: McGraw-Hill 2005.
Arias F. Practical guide to high-risk pregnancy and delivery, 2nd edn. Bangalore: Harcourt Brace and Company Asia 1988.
Degani S. Fetal biometry: clinical, pathological, and technical considerations. Obstet Gynecol Surv 2001;56:159–67.
Deter RL, Rossavik IK, Cortissoz C, et al. Longitudinal studies of thigh circumference growth in normal fetuses. J Clin Ultrasound 1987;15:388–93.
Goldstein SR. Embryonic ultrasonographic measurements: crownrump length revisited. Am J Obstet Gynecol. 1991;165:497–501.
Diagnosis of pregnancy
The diagnosis of pregnancy usually begins when a woman presents with symptoms, and possibly a positive home urine pregnancy test. Most women receive confirmatory testing for human chorionic gonadotrophin (hCG) in urine or blood. There may be presumptive or diagnostic findings of pregnancy on examination. Ultrasound is often used, particularly in those cases in which there is a question about pregnancy viability or location. Signs and symptoms
First trimester
Cessation of menstruation
Cessation of menstruation in a healthy reproductive age woman who has been experiencing normal, regular cycles before is suggestive of pregnancy. There may be a variation in the length of the follicular phase and thus date of menstruation among women. Hence the probability of pregnancy increases 10 days after the missed period.
Uterine cyclical bleeding suggestive of menstruation may occur after conception. Such bleeding episodes can occur up to 12 weeks and usually correspond with the date of the expected period. This occurs until the decidual space is obliterated by the fusion of decidua vera with decidua capsularis and is known as the placental sign. Bleeding can also occur as a consequence of blastocyst implantation.
Morning sickness
Morning sickness occurs in 50% of women and is more common in first pregnancy. It appears following a missed period and persists until 16 weeks.
Frequency of micturition
Frequency of micturition is common between 8 and 12 weeks and is due to the pressure of the enlarging uterus on the bladder and congestion of the bladder mucosa.
Breast discomfort
Breast discomfort is evident as early as 6–8 weeks and more pronounced in primigravidae.
Fatigue
Fatigue is common in early pregnancy and usually less marked by 14 weeks. Objective signs of pregnancy
Breast changes
The anatomical changes in the breasts that accompany pregnancy are quite characteristic during the first pregnancy. These are less obvious in multiparas, whose breasts may secrete a small amount of colostrum for months after childbirth. There is vascular engorgement evidenced by the delicate veins visible under the skin. The nipple and the areola become more pigmented and Montgomery’s tubercles are prominent.
Skin changes
Increased pigmentation and changes in appearance of abdominal striae are common to, but not diagnostic of, pregnancy. They may be absent during pregnancy and may be seen in women taking oestrogen–progestin contraceptives.
Discolouration of the vagina
During pregnancy, the vaginal mucosa usually appears dark-bluish or purplish-red and congested, known as the Chadwick sign. There are increased pulsations felt though the lateral fornices from 8 weeks, known as Osiander’s sign.
Changes in cervical mucus
The level of sodium chloride in vaginal secretions in the presence of oestrogen causes fern-like patterns when dried on a slide. After approximately the twenty-first day in the presence of progesterone gives a beaded or cellular appearance. This beaded pattern is usually encountered during pregnancy. This concentration, and in turn the presence or absence of the fern pattern, is determined by the cervical glandular response to hormonal action. Thus, if copious thin mucus is present and if a fern pattern develops on drying, early pregnancy is unlikely.
Changes in the cervix
The cervix becomes soft as early as 6 weeks and is called ‘Goodell’s sign’. The softening is pronounced surrounding the external os, and on speculum examination the cervix has a bluish discoloration due to an increase in vascularity.
Changes in the uterus during pregnancy
During the first few weeks of pregnancy the uterus enlarges, mainly in the anteroposterior diameter. By 12 weeks, the body of the uterus is almost globular, and an average uterine diameter of 8 cm is attained. If there is a lateral implantation the uterus will be asymmetrically enlarged, known as Piskacek’s sign. At about 6–8 weeks’ menstrual age, on bimanual examination a firm cervix is felt, which contrasts with the softer body of the uterus. Because of the soft body of the uterus, on bimanual examination the abdominal and vaginal fingers seem to appose below the body of the uterus (Hegar’s sign). In inexperienced hands the soft uterus may be mistaken for an adnexal mass.
Changes in the cervix
The cervix undergoes increased softening as pregnancy advances. In primigravidas, the consistency of the cervical tissue that surrounds the external os is more similar to that of the lips of the mouth than to that of nasal cartilage, characteristic of the non-pregnant cervix. Other conditions, such as oestrogen–progestin contraceptives, may cause cervical softening. As pregnancy progresses, the cervical canal may become sufficiently patulous to admit the fingertip. Investigations
Hormonal tests of pregnancy
Presence of hCG in maternal plasma and its excretion in urine provides the basis for the endocrine test for pregnancy. hCG is produced by the syncitiotrophoblast and is a heterodimer, with the two units designated alpha and beta. Trophoblast cells produce hCG and increase exponentially from the day of implantation. The peak of hCG is at 60–70 days and the nadir is at approximately 14–16 weeks.
Immunoassay
Antibodies are developed with high specificity for the β-subunit of hCG. This specificity is the basis for detection of hCG in urine or blood. One commonly employed technique for detection and quantification of hCG is the sandwich-type immunoassay. This test uses a monoclonal antibody against the β-subunit, which is bound to a solidphase support. The bound antibody is then exposed to hCG in the serum or urine specimen. A second antibody is then added to ‘sandwich’ the bound hCG. In some assays, the second antibody is linked to an enzyme, such as alkaline phosphatase. When the test sample with hCG is added the second antibody is unbound exposing the enzyme and bringing a colour change that is proportional to the amount of the hCG present in the sample. The sensitivity for the laboratory detection of hCG in serum is as low as 1.0 mIU/mL using this technique. A false-positive hCG test occurs in women having circulating factors in their serum that may interact with the hCG antibody. The most common are heterophilic antibodies, which are human antibodies directed against animal-derived antigens used in immunoassays.
Home pregnancy tests
The immunometric/immunochromatographic method is used to detect hCG in urine. It is a rapid test and takes 2–5 minutes. Sensitivity ranges from 10 to 50 mIU/mL.
Quantitative laboratory test kits
Radioimmunoassay can be used to detect the hCG β-subunit 7–10 days after conception, even before the period is missed. Specific assays for the β-subunit are less likely to give false positives due to the binding of the β-subunit of LH.
Ultrasound
The use of transvaginal sonography has revolutionized imaging of early pregnancy and its growth and development. A gestational sac may be demonstrated by abdominal sonography after only 4–5 weeks’ menstrual age. By 35 days, all normal sacs should be visible, and after 6 weeks or when the crown–rump length (CRL) is 5 mm, a heartbeat should be detectable. Up to 12 weeks, the CRL is predictive of gestational age within 4 days. Second trimester
Perception of fetal movements or quickening
Primigravid women start feeling fetal movements between 20 and 22 weeks and multigravid women 2 weeks earlier.
Objective signs
A linear pigmented area stretching from the umbilicus to the symphysis pubis known as linea nigra may be seen. Pink and white striae may be visible to varying degrees.
Fundal height
The uterus progressively increases in size. The duration of pregnancy can be roughly estimated based on the height of the uterus in relation to different levels on the abdomen. The fundus reaches the level of the umbilicus at about 22 weeks and below the xiphisternum at 36 weeks.
Braxton–Hicks contractions
During pregnancy the uterus undergoes palpable but painless contractions at irregular intervals from the early stages of gestation. These contractions are referred to as Braxton–Hicks contractions. Close to term these contractions become more frequent, with the increase in intensity causing discomfort.
Table 5.5.1 Differential diagnosis of pregnancy

Palpation of fetal parts
Fetal parts can be distinctly palpated as early as 22–24 weeks of gestation.
Fetal heart sounds
The fetal heartbeat can be detected by auscultation with a standard non-amplified stethoscope by a mean of 17 weeks, and by 19 weeks in nearly all pregnancies in nonobese women. Because the fetus moves freely in amnionic fluid, the site on the maternal abdomen where fetal heart sounds can be heard best will vary. Instruments incorporating Doppler ultrasound are often used to easily detect fetal heart action.
Ultrasound
Ultrasound at this gestation allows prediction of gestational age with an accuracy of 2 weeks and rules out major structural anomalies. It can also be used for placental localization. Third trimester
Distension of the abdomen, more frequent and more pronounced fetal movements, return of frequency of micturition and lightening (falling forward of the uterus with the head sinking into the pelvis resulting in the relief of pressure exerted by the gravid uterus) are some of the subjective signs of pregnancy (Table 5.5.1).
Clear palpation of fetal parts and fetal movements are objective diagnostic signs of pregnancy in the last trimester.
Ultrasound can be used to confirm the diagnosis and also to rule out multiple pregnancies. Further reading
Arulkumaran S (ed.). Essentials of obstetrics. New Delhi: Jaypee Publishers 2004.
Cunningham G (ed.). Williams obstetrics. 22nd edn. New York: McGraw-Hill 2005.
Minor symptoms of pregnancy
Pregnancy is associated with considerable anatomical, physiological, biochemical, and immunological changes. These are adaptations for maintenance of pregnancy and preparation for delivery. However, these adaptations can give rise to minor symptoms of pregnancy. These symptoms may be trivial in some women but can cause considerable discomfort and distress in others. The adaptations of normal pregnancy can be misinterpreted as pathological and it can also unmask or worsen pre-existing disease. Hence our duty as healthcare professionals is to distinguish physiological from pathological and offer advice and reassurance. Nausea and vomiting
These are the most common symptoms of the first trimester. It occurs in 50–75% of women and is erroneously called morning sickness. The symptoms can occur anytime throughout the day. It is commonly seen in primigravidas, with a 25% recurrence rate in subsequent pregnancies. Symptoms usually commence between 6 and 8 weeks and last until 14–16 weeks. Morning sickness is believed to be due to high levels of pregnancy hormones secreted by the placenta, particularly human chorionic gonadotrophin (hCG) and oestrogen. The time of morning sickness coincides with the rapidly rising serum levels of hCG. hCG starts rising by 6–8 weeks, reaches its peak by 10–12 weeks, starts declining and reaches its nadir by 20 weeks. Owing to higher levels of hCG in women with multiple pregnancies and molar pregnancies, these symptoms tend to be exaggerated. Psychological factors may have a role to play through their direct action at the emetic centre in the midbrain.
Normally, morning sickness does not produce any impact on health or restrict the normal activities of the woman. Hyperemesis gravidarum is defined as vomiting sufficiently to produce weight loss, dehydration, ketonuria, and electrolyte and acid–base imbalances.
Treatment
The mother should be encouraged to eat small frequent feeds that are non-fatty, dry, and of high calorific value. One should avoid dehydration by adequate fluid intake between meals and not with meals. The smell of certain foods often precipitates or aggravates the symptoms and should be avoided. If simple measures fail anti-emetics like metoclopromide, cyclizine, or promethazine are used. Heartburn-induced vomiting should be treated with antacids. Women need to be hospitalized for intravenous rehydration should it be required. It is essential to exclude other causes of vomiting such as urinary tract infections, and thyroid and liver problems. A scan is carried out to rule out multiple pregnancies and hydatiform moles if the vomiting is severe. Morning sickness is self-limiting and should diminish by the end of the first trimester. Heartburn
Heartburn is caused by the reflux of gastric contents into the lower oesophagus. This occurs as a result of progesterone-mediated relaxation of lower oesophageal sphincter (LES) and the upward displacement and compression of the stomach by the uterus in the third trimester. The resulting reflux of acid gastric contents and bile irritates the LES and may also contribute to nausea and vomiting. The problem is aggravated by smoking and wearing tight clothing.
Treatment
Women are advised to wear loose-fitting clothes and avoid bending soon after meals. Lying in a propped up position and cessation of smoking also help to relieve heartburn. The mainstay of treatment is antacids like aluminium or magnesium hydroxides, magnesium trisilicate singly or in combination and alginate containing antacids (e.g. Gaviscon). These are given half hour after meals and at night. H2 receptor antagonists and proton pump inhibitors are safe in pregnancy and are reserved for intractable cases. Pica and ptyalism
Pregnant women experience cravings for strange foods and at times non-foods. This desire is sometimes triggered by underlying iron deficiency, the incidence of which is twice in women with pica than those without it. Not all women with pica have iron deficiency. Pregnant women may be distressed by excessive salivation known as ptyalism. Most cases are unexplained. Constipation and haemorrhoids
The reduced gut motility due to the smooth muscle relaxant effects of progesterone gives rise to constipation in pregnant women. This problem is further aggravated by iron supplementation and pressure from the enlarged uterus and presenting part late in pregnancy. In addition to the discomfort caused by the passage of hard faecal matter, bleeding and painful fissures may develop in the oedematous and hyperaemic rectal mucosa. Haemorrhoids are seen in 1 in 3 women in pregnancy. This may arise de novo or may represent exacerbation of pre-existing ones. This is a consequence of venous stasis in the perirectal plexus of veins, further aggravated by the increased intra-abdominal pressure caused by gravid uterus and straining at stools.
Treatment
High-fibre diet, plenty of fresh fruits and vegetables, and adequate intake of water are recommended. If laxatives are needed, bulk-forming laxatives (e.g. ispaghula husk) are preferred as they are not absorbed from the gastrointestinal tract and hence safe during pregnancy. Other alternatives are prune juice, milk of magnesia, lactulose, and senna. Haemorrhoids are best managed by avoidance of constipation, local anaesthetics, and analgesics. Haemorrhoids regress after pregnancy but may take several months. Surgery may be required in severe cases and is usually deferred until after pregnancy. Urinary problems
Women experience increased frequency of micturition in the first trimester and at term when the head engages. In the first trimester the uterus enlarges and presses on the bladder decreasing its capacity. This eases off by the twelfth to fourteenth week when the uterus becomes an abdominal organ. Near term, particularly in nulliparas in whom the presenting part often engages before the onset of labour, the entire bladder base is pushed forwards and upwards, reducing its capacity and impairing the venous and lymphatic drainage. The resulting bladder is small, oedematous and susceptible to infection. In addition, the increased urine production due to increased glomerular filtration rate and renal plasma blood flow leads to frequency. There is increased risk of urinary tract infections (UTIs) in pregnancy because of oedematous bladder, incomplete emptying, vesicoureteral reflux and pelvicalyceal dilatation. UTIs particularly cystitis can cause increased frequency of micturition and should be ruled out. Stress incontinence occurs in the latter part of pregnancy due to increased intra-abdominal pressure from the gravid uterus.
Treatment
Mothers should be advised to have a sensible fluid intake throughout the day, avoiding caffeine and alcohol. Restricting fluids before going to bed helps with nocturia. UTIs should be treated. Stress incontinence usually resolves in the postpartum period. Backache
About half of pregnant women experience low backache.
Previous back pain and obesity are risk factors. Back pain increases with the duration of gestation. A woman’s centre of gravity shifts from its prepregnancy position, where it passes through the knees, to the gravid situation, where it moves forward and is in front of the knees. Women compensate for this by an exaggerated lumbar lordosis, otherwise known as the ‘proud walk of pregnancy’. This causes strain on the vertebrae and lumbosacral joints and pressure on nerve roots, causing back pain. When it affects the sciatic nerve, it causes pain, tingling or numbness running down the buttocks, hips, and thighs, the condition being called sciatica. The relaxation effect caused by progesterone and relaxin in preparation for delivery sometimes can be excessive, resulting in undue separation of pubic bones, mobility of symphysis pubis and hip joints. This can cause back pain, pubic bone pain, and difficulty in walking and mobilization. This is called symphysis pubis diastasis. Other causes of back pain are due to muscular spasm and fibrositis from local strain injury and pregnancy-associated osteoporosis. Severe back pain not responding to conservative measures should not be attributed simply to pregnancy until a thorough orthopaedic examination has been conducted.
Treatment
Preventive measures include adopting a proper posture, having sufficient rest, avoiding lifting heavy objects, avoidance of high heels, using a back support with pillows while sitting and lying down on a firm mattress. Women should be advised to squat rather than bend over when reaching down. Muscular spasms and acute strain respond well to analgesics, anti-inflammatory agents, heat, and rest. Physiotherapy is found to be beneficial. In severe cases, a pregnancy brace girdle is used to lift the weight of the gravid uterus off the pelvis. Aches and pains of pregnancy
• Lower abdominal and groin pain: some women experience aching or sharp pain at the lower abdomen and groin. It maybe unilateral or bilateral. This typically appears between 16 and 20 weeks and continues till about the thirty-second week. This is due to the enlarging uterus pulling on round ligaments.
• Headaches: this complaint is common in early pregnancy and most cases decrease in severity or disappear in mid-pregnancy.
• Calf pain: this is due to muscle spasm and tends to occur at night. Venous stasis due to poor circulation can also give rise to calf pain.
• Treatment: simple analgesics and reassurance is all that is required in the absence of any other pathology. Avoidance of long periods of standing and ankle exercises to improve circulation help to relieve calf pain. Calf muscle spasm is relieved by straightening of legs and dorsiflexion of ankles. Before attributing the symptoms to pregnancy, other pathological causes that can give rise to similar symptoms should be ruled out. For instance, deep vein thrombosis in cases of calf pain, and pre-eclampsia in headaches occurring after 20 weeks should be ruled out. Carpal tunnel syndrome
Carpal tunnel syndrome occurs when the median nerve, which runs from the forearm to the hand, becomes pressed or squeezed at the wrist. It is otherwise known as median nerve neuropathy. The carpal tunnel is a narrow, rigid passageway under the flexor retinaculum of the hand housing the median nerve and tendons. The nerve gets compressed in the carpal tunnel secondary to oedema in pregnancy. The symptoms are vague ache or pain at the wrist, radiating to hand, forearm, or arm, tingling or numbness of the fingers, excluding little finger, inability to hold or grip objects, a sense of weakness and loss of sensation in the hand. The symptoms are worse early in the morning and gets better later during the day.
Treatment
The patients should be reassured that there is no underlying sinister pathology and that it will improve after delivery. Splinting the hand in dorsiflexion to relieve pressure on the median nerve helps relieve symptoms. Surgical intervention is rarely required in pregnancy, unless there is neurological deficit. Surgery involves making an incision on the carpal tunnel to release the nerve. Varicosities
The progressively enlarging gravid uterus causes compression of the pelvic veins and the inferior vena cava, leading to diminished venous drainage of the ileofemoral veins. As a result, there is enhanced venous pressure and exacerbation of pre-existing varicosities or the appearance of new ones. Other contributory factors are progesterone-mediated venous dilatation, congenital weakness of veins, familial tendency and prolonged standing. Varicosities are found in as high as 40% of pregnant women. They are more pronounced in the third trimester, but it has been reported as early as the first trimester. Varicosities may affect the lower limbs, vulva, abdominal wall and are also present as haemorrhoids. Varicose veins in the legs can be disfiguring and painful and secondary to phlebitis and thrombosis.
Mothers should avoid using tight-fitting elastic garters, panty girdles, and corsets that can obstruct venous return. The treatment involves periodic rest in the lateral decubitus position with elevation of legs and use of compression stockings. Exercises that improve leg circulation help to reduce venous stasis. If support stockings are to be used these should be put on while the patient is still horizontal, before getting out of bed, while the veins are relatively collapsed. Surgical correction is seldom advised, although rarely injection, ligation or stripping of the veins is necessary.
Abdominal wall varicosities rarely cause problems. Occasionally a varicocele of the round ligament can present as a groin swelling.
Vulval varicosities are seen rarely, except in pregnancy and tend to remit post partum. They may be small or large and may be seen around the introitus and extend into the vagina. They may become thrombosed, bleed, itch, and cause problems in delivery. The diagnosis is made on clinical grounds and biopsy is contraindicated as it can cause heavy bleeding. Episiotomy if required at delivery should be directed away from the varicosity. Vulvar varicosities may be aided by application of a foam rubber pad suspended across the vulva by a belt. Skin changes in pregnancy
Hyperpigmentation occurs in as high as 90% of pregnant women. It begins early on in pregnancy and is more pronounced in naturally hyperpigmented areas such as the areolae, perineum, umbilicus, and areas prone to friction such as inner thighs. This is due to increased melanocyte-stimulating hormone secreted by the intermediary lobe of the pituitary gland, leading to increased melanin deposition into the epidermal and dermal macrophages.
The linea nigra is the line that often forms when the abdominal linea alba darkens during pregnancy. Pigmentation of the face is referred to as the mask of pregnancy, chloasma or melasma. This is present in 50–70% of pregnant women in the second half of pregnancy. The usual distribution involves the forehead, cheeks, upper lip, and chin. This is exacerbated by ultraviolet rays and hence avoidance of sun exposure and use of sun screens are protective. Pigmentation usually regresses postpartum, but persists in one-third of affected women.
Cutaneous neavi darken and enlarge during pregnancy.
There is augmented cutaneous blood flow and oestrogen-induced changes in small blood vessels. As a result, vascular changes such as spider naevi and palmar erythema appear in pregnancy. Spider naevi occur on the face, upper trunk, and arms. Twenty-five per cent may persist. Palmar erythema is present in up to 75% of women and fades within 1 week after delivery.
Similarly, because of increased blood flow in the gum capillaries, gums bleed easily and are prone to gingivitis in pregnancy. Occasionally, some pregnant women will develop a localized swelling on the gum, known as a pregnancy epulis. Typically, this will occur in the second or third trimester, sometimes even appearing for the first time in the final month of the pregnancy. A pregnancy epulis will often bleed easily, and can appear very red and inflamed; however, they are generally not painful. They are also not cancerous and do not have the potential to become cancerous. Some women who have an epulis will have it removed during pregnancy, usually because of bleeding, for cosmetic reasons or because the diagnosis is uncertain. However, if left alone, the epulis will usually regress after childbirth.
Striae gravidarum (stretch marks, striae distensae) appear as red or pink-purple lines or bands on the abdomen, breasts, thighs, and buttocks. They occur due to breakage of subdermal collagen as a result of stretching in pregnancy. Risk factors for overstretching of the abdomen are macrosomia, obesity, family history and non-Caucasian ethnic origin. Striae gravidarum regress postpartum or persist as white, atrophic lines called striae albicantes.
Rashes are common in pregnancy and are not often serious. Other pregnancy-specific dermatoses such as PUPP (pruritic urticarial papules and plaques of pregnancy) should be ruled out. Most rashes will disappear after childbirth. Pruritis without either rash or cholestasis can be a feature in up to 20% of normal pregnancies. Liver function tests should be done in pregnant women with pruritis to exclude obstetric cholestasis.
Treatment
Most of the skin changes regress in the postpartum period and rarely require treatment. Apart from the cosmetic impairment, they have no implications on the pregnancy or fetus.
Numerous creams, emollients and oils (e.g. vitamin E cream, cocoa butter, aloe vera lotion, and olive oil) are used to prevent striae; however, there is no evidence that these treatments are effective. Limited evidence suggests that two topical treatments may help prevent striae. One contains Centella asiatica extract plus alpha-tocopherol and collagen elastin hydrolysates. The other treatment contains tocopherol, essential fatty acids, panthenol, hyaluronic acid, elastin, and menthol. However, the safety of these medications in pregnancy needs to be confirmed with further studies before these can be recommended. Postpartum treatment involves use of retinoic acid and laser, both of which are contraindicated with breastfeeding.
Pruritis is treated with topical agents such as calamine and systemic antihistamines. Topical or systemic steroids are rarely indicated. Palpitations
Palpitation is defined as unpleasant awareness of one’s own heartbeat. It is a symptom very common in pregnancy, usually occurring due to physiological changes in the cardiovascular system rather than any identifiable underlying heart disease. The exact mechanism still remains unknown.
It is important, however, to be aware that the incidence of arrhythmias due to underlying heart disease is significantly increased during pregnancy. Other causes of palpitations such as severe anaemia, hyperthyroidism, and beriberi should be excluded. In the absence of any significant pathology, reassurance is all that is required. Breathlessness
This is a common symptom experienced by pregnant mothers in the last trimester. There is a 40–50% increase in minute ventilation in pregnancy to accommodate for the additional oxygen demand. The expanding uterus pushes up the diaphragm reducing the lung capacity. These two factors are responsible for women experiencing breathlessness in pregnancy. Shortness of breath improves with engagement of the fetal head. Lying on the side helps to relieve breathlessness while sleeping. Insomnia
Women complain of inability to sleep in pregnancy. This is particularly pronounced in the third trimester. Discomfort due to the increased size of the abdomen, backache, heartburn, frequent urination in the night, anxiety, and the occurrence of vivid dreams are responsible for this.
Treatment
Women are advised to adopt comfortable sleeping positions. It is helpful to exercise during the day, try relaxation techniques, and take warm baths just prior to sleeping. Women rarely require sedatives and long-term use of sedatives is certainly not advised.
Braxton–Hicks contractions
These are painless tightenings of the uterus that the pregnant women experiences after the twentieth week. They become stronger and more frequent towards the end of pregnancy. They originate from the top of the uterus, radiate downwards, and fade after 30–60 seconds. Tiredness
Feeling fatigued or more tired is a pregnancy symptom that can start as early as the first week after conception. This feeling will generally ease off towards the second trimester but may return towards the end of pregnancy. Stress, exhaustion, depression, the common cold or flu, or other illnesses can also leave the woman feeling tired or fatigued. Vaginal discharge
Pregnant women commonly develop excessive vaginal discharge secondary to vaginal hyperaemia and oestrogen-mediated increased cervical glandular secretions. This is called leucorrhoea of pregnancy. The discharge is non-offensive, white in colour, clear, and mucoid. Bacterial vaginosis, candidiasis, and trichomoniasis are seen in 20–30% of pregnant women. This should be excluded in case of excessive vaginal discharge. References
Arulkumaran S. Minor symptoms of pregnancy. In: Arulkumaran S, Symonds IM, Fowlie A. (eds) Oxford handbook of obstetrics and gynaecology. Oxford: University Press 2004:57–63.
Cunningham FG et al. (eds) Prenatal care. In: Williams obstetrics. McGraw-Hill 2005:200–29.
Tamizian O, Arulkumaran S. Minor disorders of pregnancy. In: Arulkumaran S, et al. (eds) Essentials of obstetrics. New Delhi: Jaypee Brothers 2004:115–17.
Physiological changes in pregnancy
Many organs undergo physiological changes in Pregnancy. Understanding these changes is important to
• determine what is abnormal in pregnancy
• explain the multitude of symptoms described in normal pregnancy
• explain the altered reference ranges in pregnancy for a laboratory investigations and their subsequent interpretation
• explain that there are different responses to some emergencies and corrective measures in pregnancy.
All the changes are best explained as individual systems that adapt to the changing needs of pregnancy. Alimentary tract
• Most pregnant women experience an increase in appetite beginning early in the first trimester and persisting throughout pregnancy. In the absence of nausea and vomiting the increase in appetite gives 200 kcal, which is almost equal to the additional 300 kcal required per day.
• Ptyalism although uncommon occurs in women who have severe hyperemesis gravidarum.
• The tone and motility of the stomach decreases during pregnancy because of the smooth muscle relaxing effects of progesterone. A decrease in levels of motilin, a gut hormone that stimulates smooth muscle, has also been implicated. The decreased tone of the stomach contributes to the nausea of pregnancy.
• In the first and second trimester there is reduced gastric acid secretion, which decreases the symptoms of peptic ulcer disease. It increases significantly in the third trimester both during fasting and after histamine stimulation, which leads to symptoms like heart burn later on in pregnancy.
• The motility of the small bowel is reduced during pregnancy but the absorption of nutrients from the small bowel remains unchanged except for iron. The increase in iron absorption is due to the increasing demand rather than decreasing gastric motility.
• Constipation is a common problem occurring during pregnancy and is because of mechanical obstruction by the uterus, decreased motility of the bowel, and increased water absorption from the colon.
• Increase in portal venous pressure leads to the dilatation of porta systemic venous anastomosis, making haemorrhoids more common in pregnancy.
• The amount of blood supply to the liver remains unchanged, although there is a significant increase in the cardiac output. Serum albumin levels fall progressively during pregnancy. Serum cholesterol levels are increased twofold by the end of pregnancy. Fibrinogen levels rise 50% by the end of the second trimester. The levels of bilirubin, aspartate amino transferase, and alanine amino transferase fall in the third trimester. Respiratory tract system
• The configuration of the thoracic cage changes in pregnancy with an increase in the subcostal angle and transverse diameter of the chest.
• As pregnancy progresses the level of the diaphragm is pushed up. The elevation of the diaphragm decreases the residual volume. Since there is a reduction in the expiratory reserve volume and residual volume there is a decrease in the functional residual capacity.
• The oxygen consumption increases up to 29%, which leads to higher alveolar and arterial PO2 levels. This change is important as the increase in the CO2 gradient between fetus and mother facilitates transfer of CO2 from the fetus to the mother.
• The maternal arterial pH is maintained at normal levels because of increased renal excretion of bicarbonate. Hence the serum bicarbonate concentration is significantly below non-pregnant levels (Table 5.7.1). Urinary and renal system
Please refer to Table 5.7.2.
Anatomic changes
• The kidneys enlarge during pregnancy and the right kidney tends to enlarge more than the left. Dilatation of the ureters and renal pelvis begins by the second month of pregnancy and becomes maximal by the middle of the second trimester. The right ureter is more dilated than the left. Mechanical factors are the most important cause of this dilatation, although early onset of ureteral dilatation supports the hypothesis that smooth muscle relaxation caused by progesterone may play a role.
• The consequences of ureteral–calcyceal dilatation are an increased incidence of pyelonephritis among patients with asymptomatic bacteriuria, difficulty in interpreting urinary radiographs and in diagnosing urinary tract obstruction during pregnancy, and interference with studies of renal blood flow in glomerular filtration and tubular function.
Table 5.7.1 Respiratory changes in pregnancy

Table 5.7.2 Physiological changes of the renal system in pregnancy

Physiological changes
• Renal plasma flow (RPF) increases by 35–60% early in pregnancy and this increase is maintained until the late third trimester. Because the effective renal plasma flow increases up to 75% and the glomerular filtration (GFR) rate increases by 50%, the filtration fraction falls significantly. As a result of the increased GFR during pregnancy, serum urea and creatinine decrease and the blood urea nitrogen levels fall.
• Serum uric acid decreases in early pregnancy, reaching a nadir by 24 weeks. The serum uric acid levels start rising due to increased renal tubular reabsorption of urate during the third trimester and is elevated to a much higher extent in patients with pre-eclampsia. Because urate levels normally rise during late pregnancy, it is necessary to know a woman’s non-pregnant urate level before third trimester values can be used in the clinical setting.
• The plasma osmolality begins to decline as early as 2 weeks after conception and is mainly due to the reduction in serum concentration of sodium and associated anions. Sodium metabolism is delicately balanced in normal pregnancy to permit a net accumulation of 900–1000 mEq of sodium in the fetus.
• Glucose excretion increases in almost all pregnant women. In the non-pregnant state the glucose loss is usually not more than 100 mg but can increase up to 10 g in pregnancy. The cause for this increase in glucose excretion is said to be due to the increased filtered load being presented to the tubules as a result of an increase in GFR. Altered tubular reabsorptive capacity may also be involved. The increase in glucose excretion raises the chance of urinary tract infection and makes monitoring of urinary glucose unreliable in pregnancy. Cardiovascular system
Pregnancy causes marked and usually reversible changes in the cardiovascular system (Table 5.7.3). Characteristic haemodynamic changes include an increase in blood volume and cardiac output. With peripheral vasodilatation and a decrease in total vascular resistance the arterial blood pressure drops in the midtrimester.
Heart rate
Heart rate in pregnancy rises as a response to falling systemic vascular resistance. The rise is evident as early as 7 weeks and increases by up to 20% by the end of the third trimester. The rise in the heart rate leads to decreased diastolic filling and hence a decrease in the cardiac output and also a decrease in left atrial emptying, increasing the risk of pulmonary oedema.
Cardiac output
Cardiac output starts increasing as early as 5–6 weeks and increases by 30–50%. Initially there is an increase in stroke volume and later an increase in the heart rate. As pregnancy progresses, stroke volume decreases to near non-pregnant levels and the increase in heart rate is responsible for maintaining increased cardiac output. Haemodynamic measurements during labour demonstrate a rise in cardiac output of about 40% compared with late pregnancy levels.
Table 5.7.3 Cardiovascular changes in pregnancy

Peripheral vascular resistance
As pregnancy advances the peripheral vascular resistance varies to change blood flow patterns. The mechanisms for vasodilatation in pregnancy are not clear, but the increase in progesterone causing smooth muscle relaxation, circulating prostaglandins, and atrial natriuretic factor may act independently or collectively in an environment of increased heat production in the fetus and an enlarged uterus with low resistance. The reduction in resistance results in a progressive fall in systemic arterial blood pressure during the first 24 weeks of pregnancy. After 24 weeks, systolic and diastolic pressures gradually rise, returning to non-pregnant levels by term. The increase in the residual blood volume in the vasculature provides a reserve in blood volume that is not haemodynamically active. These changes protect against sudden changes in blood pressure, sudden decreases in venous return, blood loss, and higher oxygen and work load demands of pregnancy, labour, and delivery.
Heart
There is an increase in left ventricular dimensions and volume during pregnancy. Despite the increase in the left ventricular dimensions, most parameters of left ventricular function remain the same as in the non-pregnant state, preserving myocardial function during pregnancy. The cardiovascular status in pregnancy resembles that seen in response to physical training. The structural changes in the heart are consistent with the effects of chronic strain put upon the heart.
Central pressures
Central haemodynamic monitoring has shown a decrease in systemic vascular resistance and pulmonary vascular resistance and colloid oncotic pressure, pulmonary capillary wedge pressure, central venous pressure, or left ventricular/work index during normal pregnancy. The pulmonary capillary wedge pressure is maintained despite the increase in stroke volume because of a marked fall in systemic vascular resistance.
Table 5.7.4 Haematological changes in pregnancy

Haematological changes
Please refer to Table 5.7.4.
• In normal pregnancy, maternal plasma volume begins to increase at 10 weeks’ gestation and increases progressively until 30–34 weeks, after which it plateaus. The mean increase in plasma volume by 30–34 weeks is 50%, although higher increases may be found in normal pregnancies. At 34 weeks the plasma volume in a healthy pregnancy is about 3800 mL. The plasma volume will start to decline by 200–300 mL from 34 weeks, with a further drop at delivery. It will return to the non-pregnant value by 6–8 weeks postpartum. There are many reasons for increased blood volume during pregnancy. It protects the mother from the possibility of a haemorrhagic decompensation at the time of delivery. The increased plasma volume serves to dissipate fetal heat production and provide for increased excretion by glomerular filtration. The increased red blood cell mass is necessary to increase oxygen transport to meet the needs of the fetus.
• Erythrocyte mass also begins to increase at about 10 weeks. Without iron supplementation, the RBC mass increases about 18% by term. Women with dietary supplement of iron show a greater RBC mass increment, increasing about 400–450 mL or 30% by term. Because plasma volume increases by 50% and the average RBC mass increases by 18–30%, the haematocrit level drops during a normal pregnancy. This so-called physiological anaemia of pregnancy reaches its nadir at 30–34 weeks.
• The peripheral white blood cell count rises progressively during pregnancy. In the first trimester, the range is from 3000 to 15 000/mm3. During the second and third trimesters, the range is from 6000 to 16 000/mm3. In labour it may increase to 20 000–30 000/mm3, after which it gradually returns to non-pregnant levels by the end of the first week of puerperium. This causes a left shift with granulocytosis and more immature white cells.
• The platelet count gradually falls throughout pregnancy, although the counts remain within the normal range for non-pregnant subjects. The fall in platelet count could be either due to increased destruction in the periphery, which is supported by a shorter average platelet lifespan in pregnancy or due to haemodilution.
• Pregnancy is a procoagulable state with alteration in coagulation and fibrinolysis. Fibrinolytic activity decreases due to increase in plasminogen activator inhibitors. The levels of fibrinogen increase during pregnancy to 400–500 mg/dL. Bleeding time and clotting time remain unchanged during normal pregnancy. Endocrine and metabolic changes
Thyroid
• The normal pregnant women are euthyroid despite the alterations in thyroid function and laboratory values. However, pregnancy is a state of iodine deficiency due to inadequate intake and increased renal clearance. The change in thyroid function tests are due to an increase in oestrogen-mediated thyroid-binding globulin. Human chorionic gonadotrophin simulates the actions of thyroid-stimulating hormone (TSH). There is a decrease in the availability of iodide because of fetoplacental losses and increased renal clearance.
• TSH concentrations are decreased during the early weeks of gestation and then rise to prepregnancy levels by the end of the first trimester.
• The concentration of thyroid hormones, total T4, and total triiodothyronine rise sharply and then plateau. That is maintained until after delivery. Despite the increase in concentration of T4 and T3, the concentration of active hormones, free T4, and free T3 do not change in normal pregnancy. Determination of free T4 is the most reliable method of evaluating thyroid function in pregnancy.
• At physiological maternal blood levels, little if any transplacental passage of thyroid hormones T4 and T3 occurs. Maternal TSH does not cross the placenta, but the thyroid-stimulating immunoglobulins and TRH cross readily.
Adrenal glands
• The plasma concentration of corticosteroid-binding globulin increases because of oestrogen-induced increase in hepatic synthesis resulting in elevated plasma cortisol concentration. The cortisol concentrations show a twofold increase in the first trimester and a threefold increase in the third trimester.
• Marked elevation of maternal plasma concentration of deoxycorticosterone (DOC) is present by midgestation. Since the plasma DOC levels do not respond to adrenocorticotropic hormone (ACTH) stimulation or dexamethasone suppression the increase may be specifically arising from the fetoplacental unit.
• Dehydroepiandrosterone Sulphate levels decrease in pregnancy because of the marked rise in the metabolic clearance of this steroid.
Pancreas
During normal pregnancy an exaggerated starvation ketosis is observed with maternal hypoglycaemia and hypoinsulinaemia as a response to starvation. In response to feeding, hyperglycaemia hyperinsulinaemia, hypertriglyceridaemia, and reduced tissue sensitivity to insulin occur. The factors responsible for this diabetogenic effect are the hormones released by the placenta, mainly human placental lactogen (hPL). This hormone reduces the effectiveness of insulin by decreasing the sensitivity of peripheral tissues. Since hPL secretion is proportional to the total placental mass, the diabetogenic effect is higher in the later part of pregnancy.
Breast changes
Breast changes occur very early in pregnancy. Tenderness, tingling sensations, and a feeling of heaviness occur within 4 weeks of the last menstrual period. The breasts rapidly enlarge in the first 8 weeks, mainly because of vascular engorgement. Oestrogen stimulates ductal growth and progesterone stimulates alveolar growth.
Postural changes
The enlarging uterus shifts the centre of gravity quite anteriorly. This is compensated by progressive increased anterior convexity of the lumbar spine during pregnancy. This keeps the woman’s centre of gravity over the legs. This postural change unfortunately leads to low backache. The ligaments of the pubic symphysis and sacroiliac joints loosen during pregnancy secondary to the hormone relaxin. This mobility of the pelvic joints is to facilitate delivery, but it can lead to pelvic discomfort in late pregnancy. Relaxation of the joints coupled with the increase in lordosis and protuberant abdomen lead to unsteadiness of the gait. Further reading
Cunningham G (ed.). Williams obstetrics, 22nd edn. New York: McGraw-Hill;2005.
Fortner KB (ed.). The John Hopkins manual of gynecology and obstetrics, 3rd edn. Philadelphia: Wolters Kluwer 2008.
Steven G, Gabbe JRN, Leigh Simpson J (eds). Obstetrics normal and problem pregnancies, 3rd edn. New York: Churchill Livingston 1996.
Preparing for pregnancy
Preconception care and counselling are important, because they identify women who can benefit from interventions before pregnancy. Preconceptional screening and counselling offer an opportunity to identify and mitigate maternal risk factors before pregnancy begins. The preconception care can be incorporated into any visit to the GP for women of childbearing age. The chances of becoming pregnant and having a healthy pregnancy and baby are better if both partners are as fit and healthy as possible. The aim of the preconceptional clinic should be to provide a strategy to reduce or eliminate the pathological influences revealed by her family, medical, or obstetrical history, or by specific testing.
Counselling in a preconceptional clinic should begin with a thorough review of the medical, obstetrical, social, and family histories. Useful information is more likely to be obtained by asking specific questions regarding each aspect of the history. Commercially prepared questionnaires can be used in preconceptional clinics, but the answers should be reviewed with the patient to ensure appropriate follow-up. Review of an up-to-date history allows prospective parents to explore their concerns and questions. Reproductive history should include questions regarding infertility, abnormal pregnancy outcomes, including miscarriage, ectopic pregnancy, recurrent pregnancy loss, and preterm delivery, and complications such as pre-eclampsia and placental abruption. History suggestive of an incompetent cervix or uterine abnormality should warrant further investigations. Social assessment
A social and lifestyle history should be obtained to identify potentially risky behaviours and exposures that may compromise a good productive outcome.
Specialist referral for patients with disabilities who wish to become pregnant should be offered. Referral for maternity care to the same hospital where the disability care is carried out should be provided. Addresses of support groups such as Disability Pregnancy and Parenthood international (DPPi) is provided.
Victims of domestic violence should be identified before they conceive, as they’re more likely to be abused during pregnancy. Information about available community, social, and legal resources should be made available to women. They should have plans devised for dealing with the abusive partner.
Family history should include genetic risks that may help to incorporate carrier screening or prenatal diagnosis for genetic diseases.
Medical assessment should include an assessment of potential risks to the fetus and to the mother:
• diabetes or epilepsy
• heart or circulatory problems, such as high blood pressure or thrombosis
• hereditary conditions in the family, such as sickle cell anaemia, thalassaemia, cystic fibrosis, or muscular dystrophy
• gynaecological problems, such as endometriosis, polycystic ovary syndrome (PCOS), or previous ectopic pregnancy.
• genetic counselling should be discussed if either of the couple have an inherited condition.
After thorough assessment the following advice should be given to women attending the preconceptual clinic and appropriate follow-up arranged. Infectious disease screening
• Rubella screening should be carried out in all women planning for a pregnancy. Women not immune to rubella should be vaccinated at least 1 month prior to trying for a pregnancy.
• Universal screening of pregnant women for hepatitis B virus has been recommended by the CDC. Women with social or occupational risks of exposure to hepatitis B virus should be counselled and offered vaccination
• Cytomegalovirus screening should be offered preconceptually to women who work in neonatal ICUs, childcare facilities, or dialysis units.
• Testing for immunity against parvovirus B19 may be offered preconceptually to schoolteachers and childcare workers.
• Human immunodeficiency virus counselling and testing should be offered confidentially and voluntarily to all women.
• Toxoplasmosis is an infection caused by a parasite that can live in soil, raw meat, and cat faeces. Infection with toxoplasmosis during pregnancy can cause miscarriage, stillbirth, or damage to the baby’s eyes, ears, or brain. To reduce the risk of infection patients should avoid handling cat litter, wear gloves when gardening, and wash all soil off fruit and vegetables before consumption.
• Screening for the varicella antibody should be performed if a positive history cannot be obtained. The varicellazoster virus vaccine is now recommended for all nonimmune adults. Medicines and drugs
• Medications considered harmful to the fetus and with proven teratogenic risk should either be stopped or changed to safer alternatives preconceptually.
• If no alternatives are available the risk of congenital abnormalities should be discussed in detail with the couple and the benefit to risk ratio calculated.
• Any over-the-counter medications should be checked with the pharmacist to see whether these are safe to take while trying for a baby or when pregnant.
• Any herbal or alternative remedies or complementary therapies should be checked if they are safe to use during pregnancy, or while trying to get pregnant.
• Couples using recreational (illegal) drugs should be advised to stop all the drugs and appropriate referral arranged if required for methadone therapy. Information on street drugs and where to go for help and advice can be found on www.talktofrank.com. Sexual health
• Patients suspected to have sexually transmitted infections should be referred to GUM clinic for confidential advice. Some sexually transmitted infections can affect the chances of getting pregnant, and if not treated they can be passed to the baby during pregnancy or birth.
• Offer cervical screening tests if not done in the last 5 years.
• If the couples have a sexual problem they should be referred to a counsellor with expertise in that field. Stopping contraception
• Many women worry that some methods of contraception, such as the pill, injection, or IUD, will make it difficult to get pregnant when they stop using them. No method of contraception causes infertility.
• Patients should be warned that sometimes ovulation can be delayed or be irregular for a short time after stopping hormonal contraception. With implanon and depot medroxy progesterone injections menstruation and fertility take longer to return than after other methods of contraception. Eating healthily
Eating a variety of foods, with as much fresh food as possible, helps to ensure adequate intake of vitamins and minerals.
A healthy diet is made up of
• starchy foods, such as potatoes, sweet potatoes, bread, pasta, rice, and cereals
• at least five portions of fruit and vegetables a day (these can be fresh, dried, frozen, tinned, or juice)
• protein foods, such as meat, beans, chicken, eggs, pulses (e.g. lentils), and nuts (seek advice on foods to avoid)
• dairy foods, such as milk, yoghurt, and cheese (see ‘Foods to avoid’ for advice on cheese)
• fish (see ‘Foods to avoid’ for advice on fish). Folic acid
• All women planning a pregnancy should take a daily supplement of folic acid: 0.4 mg (400 μg) of folic acid should be taken from the time of stopping contraception or as soon as pregnancy is confirmed until week 12 of pregnancy.
• Folic acid prevents neural tube defects and if a previous pregnancy was affected by spina bifida, or either of the partners have a neural tube defect, or suffer from epilepsy a higher dose of folic acid should be taken.
• Patients should be advised to eat foods that contain folic acid, such as green leafy vegetables, breads, and cereals with folic acid added to them. Foods to avoid
Severe food poisoning during pregnancy can cause miscarriage, stillbirth, or damage to the developing baby. Pregnant women are advised to avoid foods that have a higher risk of causing food poisoning. The following foods can contain harmful bacteria:
• unpasteurized milk and cheese
• soft-cooked or raw eggs, for instance in homemade mayonnaise or mousse (check food labels to make sure eggs are pasteurized)
• soft cheeses with rind, such as Brie
• blue cheeses, such as Stilton
• undercooked meat, including pâte, or cold prepared meals, and cook–chill foods
• shellfish, such as mussels, prawns and clams.
Foods containing substances that can cause harm to the unborn baby:
• vitamin A supplements (including cod liver oil)
• liver (including liver pâte) contains high levels of vitamin A, so limit this to no more than one portion a week
• fish such as swordfish, marlin and shark, which can contain high levels of mercury
• peanuts or foods containing peanuts, especially with a history of allergy. X-rays
Patients should not have an X-ray while trying for a pregnancy unless it is essential for health. Lifestyle issues
Exercise
• Both partners should be advised to continue exercise before planning for a pregnancy, and if not doing any exercise should be advised to start. The more active and fit the patient is the easier it is to cope with pregnancy.
• Walking and swimming are good ways to start getting fit, and a yoga or Pilates class can help with relaxation and muscle tone.
• Avoid exercise or sports where there is a risk of being hit in the abdomen, such as martial arts. Extra care should be taken during activities where there is a risk of falling or losing balance, such as cycling and horse riding.
Weight
• Being overweight or underweight can disrupt menstruation and reduce the chances of getting pregnant.
• Body mass index (BMI) more than 29 or less than 19 may make getting pregnant difficult.
• A BMI less than 18.5 is considered underweight, and a BMI above 25 is considered overweight. If you or your partner are concerned about your weight, talk to your doctor, nurse, or midwife.
Smoking
Stopping smoking may be the most important thing women can do for their health and the baby. Women who smoke during pregnancy have a greater risk of:
• miscarriage
• stillbirth
• giving birth too early (premature birth)
• complications during and after pregnancy and labour
• having low birthweight babies.
Babies who have low birthweight or are born prematurely are more likely to have health problems and are at higher risk of sudden infant death syndrome (SIDS, or cot death). See www.gosmokefree.nhs.uk for further information.
Alcohol
• Alcohol should be limited to one or two units per week and binge drinking should be avoided.
• Alcohol can damage sperm production. Partners should be advised to avoid drinking too.
• Drinks heavily and frequently during pregnancy, or regularly binge drinking (has five or more units of alcohol on any one occasion) can harm the baby’s development and health.
• Very heavy drinking can lead to fetal alcohol syndrome (FAS) and fetal alcohol spectrum disorder (FASD). These describe a range of symptoms that can be caused by alcohol in pregnancy, including damage to the facial features, brain, heart, and kidneys, and learning difficulties and behavioural problems in later life. See www.drinkaware.co.uk for further information Work environment
There are some occupations, such as working as a radiographer or working with chemicals, or exposure to substances in some surroundings, that may be harmful for pregnancy. Further information can be obtained from the Health and Safety Executive website at www.hse.gov.uk. Patient information and contacts
Disability Pregnancy and Parenthood international (DPPi), tel: 0800 018 4730, textphone: 0800 018 9949, www.dppi.org.uk Further reading
Cunningham G (ed.). Williams obstetrics, 22nd edn. New York: McGraw-Hill 2005.
Fortner KB (ed.). The John Hopkins manual of gynecology and obstetrics, 3rd edn. Philadelphia: Wolters Kluwer 2008.
FPA. Planning a pregnancy. FPA 2006.
Puerperium Definition
Puerperium is the period following childbirth during which the pelvic organs revert back to the prepregnant state both anatomically and physiologically. It lasts for 6 weeks after the delivery of the baby. Normal changes of the puerperium
Involution of the uterus, cervix, and vagina
The postpartum uterus, which weighs about 1 kg, returns to its prepregnant size of 80 g. Immediately after placental expulsion, the fundus of the contracted uterus is slightly below the umbilicus. By a process called involution it shrinks, and becomes a pelvic organ in 2 weeks and regains its prepregnant size in 6 weeks. The total number of muscle cells does not decrease appreciably; instead the individual cells decrease markedly in size. Simultaneous involution of the connective tissue framework also occurs. Endometrial regeneration is complete by the third week, except at the placental site. Complete extrusion of the placental site takes up to 6 weeks. If this process is defective, late puerperal haemorrhage may ensue.
The cervical opening readily admits two fingers for a few days after labour. By a process of gradual contraction the opening narrows, the cervix thickens, and the canal reforms. By 2–3 weeks into the puerperium the internal os is closed. The lower uterine segment over a course of a few weeks is converted into the uterine isthmus.
The vagina gradually diminishes in size, but rarely returns to nulliparous dimensions. Rugae reappear by the third week. The hymen is represented by small tags of tissue known as carunculae myrtiformis.
Lochia
Lochia is the vaginal discharge for the first 2–3 weeks during puerperium. It occurs because of the sloughing of the superficial layer of the decidua. The basal layer remains and new endometrium regenerates from it (Table 5.9.1).
Urinary tract
Puerperal diuresis occurs between the second and the fifth days. This is a reversal of the excessive extracellular water that accumulated during pregnancy. Because of the relative insensitivity to the raised intravesical pressure because of the nerve plexus trauma sustained during delivery, the bladder maybe over distended without the desire to pass urine. The paralysis effect of regional anaesthesia further compounds this. Stagnation of urine along with dilated ureters and renal pelvis predisposes to urinary tract infection (UTIs). Dilated ureters and renal pelvis return to normal size within 8 weeks.
Pelvic floor
Evidence of neuropathic injury of the pudendal nerve has been reported in up to half of the women following vaginal delivery. This leads to weakening of pelvic floor muscles and can result in incontinence of urine, faeces, or flatus and may contribute to development of prolapse later in life. Stress incontinence is known to affect one-third of women 3 months after normal delivery. Occult anal sphincter injury as identified by endoanal ultrasound is seen in one-third of primiparous women 6 weeks after normal delivery; 10–20% of women who had a normal delivery report symptoms of altered faecal incontinence 6 weeks after delivery. Both direct trauma and pudendal nerve injury causes altered faecal or flatus incontinence.
Table 5.9.1 Types of lochia

Recovery of pudendal nerve function was observed in two-thirds of women by 2 months postpartum with evidence of persistent neuropathy in the remainder. Postnatal pelvic floor exercises are very important and help women regain tone.
Blood
Blood volume returns to normal after the first week. Although the heart rate falls, stroke volume increases and overall cardiac output rises soon after delivery and remains elevated for at least 48 hours postpartum. The rise in cardiac output is due to the rise in stroke volume from venous return. Thus, early puerperium is a time that requires close surveillance in any woman at risk of cardiac compromise. By 2 weeks, these changes return to normal non-pregnant values.
The haemoglobin concentration and haematocrit level fluctuate moderately during the first few postpartum days. Haematocrit returns to normal by the end of first week. Considerably lower haemoglobin levels than the predelivery state indicate excessive blood loss at delivery. In response to the stress of labour there is marked leucocytosis in the puerperium. The platelet count falls soon after separation of the placenta, but secondary elevation occurs by 4–5 days. Puerperium is a hypercoagulable state due to increased platelet count, platelet adhesiveness, and fibrinogen levels. Women are at high risk of developing thromboembolism in the puerperium, and appropriate anticoagulant regimens should be instituted for those at risk.
Weight loss
Average weight loss in puerperium is 7–10 kg, 5–6 kg attributed to uterine evacuation and 2–3 kg due to diuresis.
Peritoneum and abdominal wall
The laxity of broad and round ligaments requires considerable time to recover. The abdominal wall remains soft and flabby as a result of the rupture of elastic fibres in the skin caused by prolonged distention of the abdomen by the pregnant uterus. A return to normal for these structures take several weeks. Exercise helps to regain abdominal tone.
Most striae fade to pale/white (striae albicantes) lines and shrink postpartum, although they do not disappear completely. Management of puerperium
Postnatal examination
At least for the first hour after delivery vital signs should be monitored every 15 minutes. Monitoring of the amount of vaginal bleeding and palpation of the fundal height and tone should be done to ensure that the uterus is well contracted.
In the postnatal ward women should be asked about general wellbeing, psychological wellbeing, adequacy of sleep and diet, pain control, excessive bleeding, bowel and bladder functions. Clinical examination should include monitoring of vital signs, involution of uterus, examination of perineum, and recording of colour and amount of lochia.
There may be a slight reactionary rise in temperature by 0.5° following delivery, which comes down to normal within 12 hours. The rate of involution is assessed by measuring the symphysiofundal height after emptying the bladder. The average rate of involution is 1 cm per day. The most common causes of delayed involution include full bladder, loaded rectum, uterine infection, retained products, fibroids, or broad ligament haematoma. Offensive lochia along with pyrexia and tender uterus suggest endometritis. Persistent red lochia along with subinvolution should alert the clinician to infection or retained products. Perineal examination is carried out daily to asses healing of episiotomy or tears and also to rule out vulval haematomas and infection. General care of the mother
The mother is encouraged to get good sleep and adequate rest. Rooming in with the baby improves breastfeeding and mother–baby bonding.
The mother can be ambulant a few hours after delivery. Early ambulation decreases the risk of thromboembolism, and bladder and bowel dysfunction. Women who have had regional analgesia should delay ambulation till the muscle power of the lower limbs returns to normal. For this reason and to avoid injury due to syncopal attacks, a trained attendant should be present at least at the first ambulation.
There are no dietary restrictions for women who have delivered vaginally. If the mother does not breastfeed, her dietary requirements are the same as for non-pregnant women. Breastfeeding mothers should have a balanced diet that is high in calories, protein, vitamins, and minerals. There is an excess demand of at least 700 calories and 20 g of protein per day compared with the non-pregnant state. Daily requirements of calcium are increased three times and vitamin A by one and a half times that of the non-pregnant state. An adequate amount of fluid intake is important for successful breastfeeding.
Women should be encouraged to start exercise to tone up the abdominal and pelvic floor muscles as soon as they are able to do so. These exercises should be continued for at least 3 months.
After pain
Oxytocin liberated in response to suckling causes strong uterine contractions and is felt by the patient as spasmodic pain. Simple analgesics and antispasmodics are required occasionally to relieve the pain.
Care of the bladder
Women should be encouraged to void soon after delivery. This may not be possible for women who have undergone regional analgesia: an indwelling catheter is desirable until the patient is adequately mobile. Overdistention of the bladder is quite common in the puerperium. The infusion of intravenous fluids during labour and sudden withdrawal of the antidiuretic effect of oxytocin can lead to rapid bladder filling. This along with inadequate bladder sensation due to neuropraxia and epidural analgesia result in overdistension. Difficult instrumental deliveries, painful genital lesions such as extensive episiotomies and lacerations cause pain and periurethral oedema and prevent bladder emptying. Other sources of pain, such as prolapsed haemorrhoids, abdominal wound pain, or even faecal impaction may all contribute to voiding difficulties. In general, after Caesarean section and difficult instrumental deliveries with extensive perineal repair, an indwelling catheter for 12–24 hours is recommended.
One should look for overdistended bladder during abdominal palpation. The bladder may be palpated as a cystic mass suprapubically, or the enlarged bladder may falsely elevate fundal height. If the women has not voided within 4–6 hours of delivery, her bladder is in danger of overdistention. She should be encouraged to void. Analgesics are administered to relieve pain. If these measures fail, an indwelling catheter should be left in situ for 24–48 hours or until bladder tone is regained.
The incidence of UTI in puerperium is 3–5%. The increased incidence of UTIs may be due to bladder stasis, voiding difficulties and catheterization in labour. UTIs should be monitored, and if present should be treated with antibiotics.
Care of the bowel
Constipation is common in pregnancy and remains so in the puerperium. Fear of defaecation due to pain of prolapsed haemorrhoids, anal fissure, and perineal injuries further exacerbate the problem. The mother should be encouraged to drink plenty of fluids, consume a high-fibre diet, and be ambulant. Non-responders to conservative measures should receive bulk-forming agents or laxatives. Prophylactic stool softeners should be given to women who had third- or fourth-degree repair to avoid straining at defaecation; 20–50% of women who had primary third-and fourth-degree repairs are known to suffer faecal or flatus incontinence. This has implications on their future pregnancy management and quality of life. Hence these women should routinely be followed up in the hospital at 6 weeks to detect these problems and institute appropriate management.
Perineal care
Perineal discomfort is the most common problem encountered postnatally, occurring in 42% of women after spontaneous vaginal delivery and persisting after the first 2 months in 8–10%. The figures following assisted vaginal deliveries are 84% and 30% respectively. Perineal pain is worse following instrumental delivery, episiotomy, or spontaneous tears. A warm sitz bath helps to relieve local pain and oedema. Topical cooling measures and local anaesthetic provide short-term relief. Non-steroidal anti-inflammatory drugs (e.g. diclofenac suppositories) are the mainstay of treatment.
Women should be advised of perineal hygiene and regular changing of sanitary pads. Perineal toilet should be carried out regularly with antiseptic solutions. Any evidence of infection should be aggressively treated with antibiotics. In case of episiotomy wound dehiscence, resuturing is contraindicated in the presence of infection, and healing by secondary intention should be allowed. Any local abscess or haematomas should be drained.
Postpartum blues
As many as half of women experience ‘postpartum blues’ in the puerperium. This is a passing state of heightened emotions and in itself is not an illness. Levels of oestrogen, progesterone, and cortisol fall dramatically within 48 hours after delivery. This sudden fall in hormones leads to an ‘emotional let down’ and is thought to play a role as this state classically peaks 3–5 days after delivery and can last up to 2 weeks. Other contributory factors are discomfort, fatigue, sleep deprivation during labour and puerperium, and anxiety over parenting capabilities.
These women cry easily, are irritable, and suffer from sleep disturbances. Postpartum blues usually do not interfere with a woman’s ability to care for her baby. Supportive therapy is all that is required. This condition should however be differentiated from a more serious postnatal depression.
Traumatic neuritis
This may present with foot drop, paraesthesia, sciatic pain, and muscle wasting in one or both limbs following delivery. The mechanism is thought to be herniation of lumbosacral discs at L4–5 due to exaggerated lithotomy position and instrumental delivery. Management entails bed rest, physiotherapy, and spinal/orthopaedic opinion with appropriate imaging. Peroneal neuritis may result from compression of the proneal nerve between the head of the fibula and the lithotomy pole, and presents as foot drop. Treatment is supportive with physiotherapy.
Diastasis of the symphysis pubis
Incidence is around 0.1% after spontaneous delivery. It maybe associated with a forceps delivery, a rapid second stage, or exaggerated flexion and abduction of maternal thighs such as in McRobert’s manoeuvre. The symptoms are of pain over the symphysis, which is exaggerated by weight bearing. The clinical signs are a waddling gait, tenderness over the joint, and occasionally a palpable interpubic gap. Management is supportive with bed rest, physiotherapy, analgesia, and anti-inflammatory drugs and a pelvic support brace.
Immunization
Anti-D gammaglobulin is administered within 72 hours to Rh-negative mothers bearing a Rh-positive baby. Rubella-susceptible women can be vaccinated postnatally. Pregnancy should be avoided until 1 month after vaccination. Breastfeeding should not be stopped.
Return of menstruation and ovulation
The time of return of menstruation and ovulation after delivery is variable and dependent on lactation. Menstruation returns by 6–8 weeks in non-lactating mothers; 70% of women with full or nearly full breastfeeding remain amenorrheic till 6 months. Ovulation is suppressed during the greater part of lactational amenorrhoea, except for the last 4 weeks when 30% of cycles are thought to be ovulatory. The conception risk during lactational amenorrhoea is only 1–2% if all three criteria, (1) amenorrhoea (2) full lactation (3) less than 6 months postpartum, continue to apply.
Contraception
Ovulation is found to return in non-lactating mothers as early as 3 weeks. Hence they should use appropriate contraception as early as possible. The choice of contraceptives available to non-lactating mothers is the same as any other woman. Contraceptive pills containing oestrogen are not prescribed during breastfeeding as they inhibit lactation. Instead, the progesterone-only pill is used. If an intrauterine device is preferred, the insertion is performed after 6 weeks, once involution is complete.
Resumption of intercourse
Women should resume intercourse as soon as they are physically and emotionally ready for it. It is preferable to postpone it until the third week when the lochia has ceased, the cervix has closed, and the uterus has become a pelvic organ. Dyspareunia is quite common in the postpartum period due to the hypo-oestrogenic effects of breastfeeding. Topical lubricants or vaginal oestrogen creams are recommended.
Time of discharge
NICE guidelines recommend that the length of stay in a maternity unit should be discussed between the woman and the healthcare professional, taking into account the health and wellbeing of the mother and the baby. After uncomplicated deliveries, woman can be discharged from the hospital as early as 6 hours.
Postnatal visit
Postnatal examination is carried out at the end of 6 weeks. The doctor should enquire about physical, emotional and social wellbeing and that of the infant. An abdominal and pelvic examination is performed to look for tone of abdominal and pelvic musculature, uterine involution, and healing of episiotomy and tears. Contraceptive advice should be given. Further reading
Arulkumaran S. Care in the puerperium. In: Arulkumaran S, Symonds IM, Fowlie A. (eds) Oxford handbook of obstetrics and gynaecology. Oxford: Oxford University Press 2004:365–72.
Fynes M, O’Herlihy C. The influence of mode of delivery on anal sphincter injury and faecal continence. Obstet Gynaecol 2001;3:120–25.
Groom KM, Paterson-Brown S. The influence of mode of delivery on anal sphincter injury and faecal continence. Obstet Gynaecol 2002;4:4–9.
Shetty J. Normal puerperium. In: Arulkumaran S, Sivanesaratnam V, Chatterjee, Kumar P. (eds) Essentials of obstetrics. New Delhi: Jaypee Brothers 2004: 373–77.
Cunningham FG, Leveno KJ, Bloom SL, et al. (eds). The puerperium. In: Williams obstetrics, McGraw-Hill 2005:695–710. Internet resources
Postnatal care: www.nice.org Patient resources
Postnatal care: www.nice.org
Routine blood tests in pregnancy
It is important to screen for certain illnesses in pregnancy, as these illnesses have adverse consequences on the mother and baby. By detecting and intervening at the right time, adverse outcomes can be reduced or prevented. This chapter focuses on the reasons for undertaking such blood tests and interventions available. A detailed discussion of individual conditions is beyond the scope of this chapter and the reader is advised to consult appropriate chapters of this textbook. Routine blood tests
• At booking: full blood count (FBC), blood group, presence of atypical antibodies, blood tests for syphilis, HIV, hepatitis B, immunity to chicken pox and rubella.
• 28 weeks: FBC, atypical antibodies
• 34 weeks: FBC, atypical antibodies. Special blood tests
• 8–10 weeks: haemoglobin electrophoresis
• 10–13 weeks: serum markers (PAPP-A, free β-human chorionic gonadotropin (hCG)) for first trimester Down’s syndrome screening
• 15–20 weeks: serum markers (α-fetoprotein (AFP), β-hCG, unconjugated oestradiol, inhibin) for second trimester down syndrome screening.
• 16-18 weeks: oral glucose tolerance test (OGTT) in women with previous history of gestational diabetes (GDM).
• 24-28 weeks: OGTT in women with risk factors for GDM. Anaemia
The incidence of anaemia in pregnancy varies from 10–30% in the developed world and 40–80% in the developing world. Anaemia in pregnancy is due to physiological haemodilution, increased demand, nutritional deficiency, and poor reserves. The lower limit of normal for haemoglobin in pregnancy is taken as 10.5 g/dL as opposed to 11.5 g/dL in a non-pregnant individual to account for physiological haemodilution. Iron deficiency anaemia is the commonest cause of anaemia in pregnancy followed by folate deficiency. If anaemia is detected in pregnancy, it should be investigated further by assessing other indices such as ferritin, total iron binding capacity (TIBC), serum and red cell folate, and serum B12 levels. Anaemia and pregnancy
Minor symptoms of pregnancy such as tiredness, lethargy, breathlessness, and palpitations are exacerbated due to iron deficiency anaemia. Iron deficiency adversely affects neuromuscular transmission because of the malfunction of iron-dependent tissue enzymes. Iron deficiency is associated with low birthweight, preterm delivery, and postpartum haemorrhage. There is increased incidence of childhood anaemia and impaired cognitive development in infants born to anaemic mothers. Low birthweight is in itself a risk factor for development of adult hypertension. Treatment
Correction of iron deficiency anaemia can be achieved by iron supplementation, either oral or parenteral. The maximum rise in haemoglobin achievable with oral or parenteral iron is 0.8 g/dL/week. Hence a woman presenting with anaemia late in pregnancy is treated with blood transfusion if rapid restoration of haemoglobin is indicated. Women with low haemoglobin presenting in labour should have their blood grouped and saved should blood be needed in case of postpartum haemorrhage. Megaloblastic anaemia is treated by high-dose folate or vitamin B12 injections. Blood grouping and screening for antibodies
Determining the blood group at booking makes it possible to identify women who are Rhesus negative and therefore at risk of Rhesus immunization. It also helps to identify other atypical antibodies acquired as a result of previous pregnancies or blood transfusions, quantify them, monitor their progress, and make appropriate management plans.
The current recommendation is to give universal Anti-D prophylaxis for pregnant women who are Rh D negative who have not already been sensitized. This is given at 28 weeks, 34 weeks, and after delivery. This is to prevent Rhesus alloimmunization and subsequent development of haemolytic disease of the newborn (HDN). Not all fetuses of sensitized mothers develop HDN. HDN can vary in severity from being detectable only in laboratory tests, through to stillbirth or birth of newborns with severe anaemia and jaundice leading to neonatal morbidity and death.
Since the implementation of post-delivery immunoprophylaxis using anti-D immunoglobulin (Ig) in the UK in 1969, deaths attributed to RhD alloimmunization have fallen from 46/100 000 births before 1969 to 1.6/100 000 in 1990.
A dose of 500 IU anti-D IgG is given at 28 and 34 weeks. After delivery, if the baby is found to be Rh negative, post-delivery prophylaxis is not indicated. Similarly, if the partner’s blood group is known to be Rhesus negative from the beginning and paternity is not in doubt antenatal prophylaxis is not indicated. Studies have shown that a dose of 500 IU is sufficient to cover a fetomaternal haemorrhage (FMH) of up to 4 mL at delivery. This is the case in more than 99% of deliveries. Further dosing is required if the amount of FMH is estimated to be more than 4 mL using quantification techniques. Anti-D is also indicated after sensitizing events such as termination of pregnancy at any gestation, miscarriages before 12 weeks managed surgically, spontaneous or threatened miscarriages after 12 weeks, recurrent episodes of threatened miscarriage, after external cephalic version, and antepartum haemorrhage. A dose of 250 IU should suffice before 20 weeks and 500 IU after 20 weeks. Routine prophylaxis should be carried on irrespective of recent administration of Anti-D after a sensitizing event.
Despite routine anti-D prophylaxis a small proportion of women develop anti-D antibodies. The most important cause is unrecognized transplacental bleeds late in pregnancy. The remainder appear to be due to inadequate prophylaxis, late prophylaxis, or no prophylaxis. Haemoglobin electrophoresis
Haemoglobin electrophoresis should be routinely performed in women of ethnic origin with a high incidence of haemoglobinopathies. These include women of Cypriot, Eastern Mediterranean, Middle Eastern, Indian and Southeast Asian origin, in whom the incidence of thalassaemia is greatest, and women of African or Afro-Caribbean origin, who are at risk of sickle cell disease. Persistent anaemia unresponsive to haematinics may be an indication for haemoglobin electrophoresis in any woman, irrespective of racial origin. Haemoglobinopathies and pregnancy
Both sickle cell disease and thalassaemias have an autosomal recessive pattern of inheritance.
Pregnancy in women with β-thalassaemia major is very rare as this condition is usually fatal in the first or second decade. Similarly α-thalassaemia major is incompatible with life. What we routinely encounter in antenatal clinics are those women with thalassaemia traits. These women have chronic anaemia.
There are significant fetal and maternal complications in pregnancies experienced by mothers with sickle cell disease. The increased metabolic demands, hypercoagulable state, and vascular stasis associated with pregnancy predispose to these complications. Fetal complications are due to compromised placental blood flow.
There is increased incidence of miscarriage, preterm labour, intrauterine growth restriction, and stillbirths. Anaemia, infection, pre-eclampsia, thromboembolic episodes and sickling crises are increased in mothers.
Management
If the mother is known to have sickle cell or thalassaemia trait, partner testing is done to establish the carrier status of the partner. If both parents are have traits the woman should be referred for prenatal diagnosis as there is a 25% chance that the fetus is affected. Parents may opt for further invasive testing or termination of pregnancy.
Women with thalassaemia traits need iron and folate supplementation throughout pregnancy, but should not be given parenteral iron. If anaemia does not respond to haematinics, blood transfusion may be required prior to delivery.
Women with sickle cell disease should be managed in an appropriate centre with multidisciplinary input from haematologists, obstetricians, anaesthetists, and paediatricians. Screening for gestational diabetes
GDM is defined as glucose intolerance of variable severity with onset or first identified during pregnancy. The incidence varies from 0.2–0.5% in white population to 3–6% in south Asian, Afro-Caribbean and Middle Eastern populations. GDM constitutes 90% of diabetes in pregnancy. GDM and pregnancy
GDM occurs usually in the latter half of pregnancy and hence has no effect on organogenesis. There is increased incidence of pre-eclampsia, polyhydramnios, preterm labour, and recurrent urinary tract infections and candidiasis with uncontrolled or poorly controlled GDM; 20–30% of women with GDM have macrosomic infants. This leads to the need for early induction of labour, prolonged labour, shoulder dystocia, increased incidence of operative deliveries, and postpartum haemorrhage. Poorly controlled diabetes can lead to sudden intrauterine deaths. In the neonatal period macrosomic infants are prone to hypoglycaemia, electrolyte imbalances, hyaline membrane disease, hyperviscosity syndromes, birth injuries and birth asphyxia. Women identified as having GDM are at 50% increased risk of developing non-insulin-dependent diabetes mellitus (NIDDM) within 10–15 years.
Although management of GDM is relatively clear-cut there exists lots of controversy in the screening methods used to detect GDM, the timing of screening, and the population to be screened. Studies have shown that selective screening misses 30% of cases of GDM, but universal screening is not cost-effective, especially in populations where there is low prevalence of GDM.
The National Institute of Clinical Excellence (NICE) recommends risk factor-based screening at booking using the OGTT. The risk factors are maternal obesity (BMI above 30 kg/m2), previous macrosomic baby weighing >4.5 kg, previous gestational diabetes, first-degree relative with diabetes, and south Asian, black Caribbean and Middle Eastern ethnic origins. The test is repeated at 16–18 weeks and 28 weeks if the previous tests are normal. If any new risk factors develop in the present pregnancy, such as persistent glycosuria, macrosomia, or polyhydramnios, the OGTT should be carried out at around 24–28 weeks. After delivery the OGTT is repeated at 6 weeks to identify those women with NIDDM.
Management
Identifying women with GDM is important as there is clear evidence that appropriate therapy can reduce both fetal and maternal morbidity. In a large randomized controlled trial, perinatal complications were 4% versus 1% and the incidence of macrosomia 21% versus 10% in the untreated and treated groups respectively. Treatment includes diet control, exercise, and use of insulin to achieve good blood sugar control. It is also possible that by diet control, regular exercises, and avoidance of obesity, these women can prevent or delay the later development of diabetes. Screening for Down’s syndrome
Down’s syndrome is associated with a spectrum of physical and mental handicaps, and some couples elect to terminate an affected pregnancy. Various tests are available for Down’s syndrome screening. An ideal screening test is one with maximum sensitivity and specificity. Parents may opt for further invasive tests to confirm diagnosis once they are found to be screen positive.
These invasive tests are not without complications, hence the need for a screening test with a low false-positive rate.
Studies have shown that levels of several fetoplacental products in the maternal circulation are strikingly altered in the presence of a Down’s syndrome fetus. Hence blood tests are carried out to measure these markers and give a risk scoring. The screening tests available are first trimester serum screening, measurement of nuchal translucency, second trimester serum screening, and anomaly scan. Combined testing utilizes both first trimester serum markers and nuchal translucency. Triple tests and quadruple tests utilize various serum markers of the second trimester. An integrated test is one in which a combination of first and second trimester screening is used to quantify the risk. A serum integrated test is one in which only first and second trimester serum markers are used in the absence of a scan (Table 5.10.1).
The National Screening Committee recommended that by April 2004 all women should be offered a screening method with a detection rate of 60% and FPR of presence of anti-HBs, anti-HBc, HBeAg, anti-HBe, specific IgG and IgM for hepatitis A and C. Highly infective carriers are HBeAg positive. The risk of transmission increases from 2–15% in HBeAg-negative carriers to 90% in HBeAg-positive carriers. Carrier mothers should be managed by hepatologists, and their liver function tests monitored to detect chronic active or chronic persistent hepatitis. Partner screening and appropriate counselling of family members is important. Healthcare professionals coming into contact with these mothers should take appropriate precautions during labour and delivery.
Infants born to HBsAg-positive mothers should be given hepatitis B Ig and full course of vaccination. This intervention is found to be protective against transmission in 90% of cases. Breastfeeding is not contraindicated in immunized babies.
Syphilis
Syphilis is a sexually transmitted illness caused by the spirochete Treponema pallidum. It has three stages: primary, secondary, and tertiary. Transplacental transmission can occur at any stage. Untreated maternal primary and secondary syphilis lead to symptomatic congenital syphilis in 50% of neonates. These figures are 40% for early latent syphilis and 10% for late latent syphilis. Infection in utero can lead to stillbirths, non-immune hydrops, early congenital syphilis and late congenital syphilis of the newborn. Congenital syphilis is a multisystem disorder with the involvement of skin, lymph nodes, liver, spleen, eye, bone, nerves, and heart.
Penicillin therapy in pregnancy is effective for treating maternal disease, preventing transmission to the fetus, and treating established fetal disease. Pregnant women with syphilis should be treated with the appropriate penicillin regimen according to their stage of disease. The risk of congenital infection can be reduced from 10–50% to 1–2% by maternal treatment with penicillin. Partners should be screened and treated. Patients should be screened and treated for other sexually transmitted diseases. There is no contraindication to breastfeeding.
HIV
The prevalence of HIV infection in pregnant women varies from 0.06–0.38% in the developed world to 10–15% in Africa. The National Screening Committee recommends universal screening for HIV. The aim is to increase the uptake of HIV testing to 90%. HIV and pregnancy
Pregnancy does not accelerate disease progression or reduce the CD4 lymphocyte count. There is increased incidence of miscarriage, preterm delivery, IUGR, and low birthweight. Women on highly active antiretroviral therapy (HAART) do not seem to have an increased incidence of congenital malformations. The major mode of acquisition of HIV in children worldwide is through mother-to-child transmission. This happens antenatally, intrapartum, and postpartum through breastfeeding. Breastfeeding alone accounts for 30–50% of mother-to-child transmission and doubles the rate of transmission. The rate of vertical transmission without prophylactic treatment varies from 15–20% in the developed world to 25–40% in Africa. Advantages of screening
Reduction of vertical transmission
The risk of perinatal transmission of 15–40% can be reduced to less than 2% with antiretroviral therapy (both antepartum and intrapartum), avoidance of labour and breastfeeding. A blanket policy of Caesarean section for all HIV-positive women is not appropriate. The viral load and CD4 count should be taken into consideration in deciding mode of delivery. It is recommended that breastfeeding should be avoided in HIV-infected women in the developed world, where there is easy access to alternatives. In the developing world the risk of stopping breastfeeding in the form of malnutrition and infections far outweighs the benefits of reducing transmission of HIV.
Appropriate medical management of the woman can be initiated
HIV-infected women should have multidisciplinary care involving an HIV specialist, obstetrician, and paediatrician. HAART in these women is known to reduce viral load, improve CD4 count, and reduce disease progression to AIDS. Women with high viral load and low CD4 count are at high risk of developing opportunistic infections. Such women receive prophylaxis for Pneumocystis pneumonia. Women with AIDS may make an informed decision about termination of pregnancy because of reduced life expectancy and increased risk of vertical transmission.
Partner screening and contact tracing
The antenatal period is a good time to offer partner testing and contact tracing in HIV-infected women. Studies have shown that about 30–40% of HIV-infected men and women are unaware of their HIV status.
Precautions for healthcare professionals
Healthcare professionals can take appropriate precautions to prevent risk of transmission to themselves once the HIV status is known. Post-exposure prophylaxis is available for healthcare professionals coming into accidental contact with the blood and body fluids of infected women. There should be clear departmental guidelines on the disposal and disinfection of instruments that have come into contact with infected mothers. Further reading
Crowther CA, Hiller JE, Moss JR, et al. Effect of treatment of gestational diabetes mellitus on pregnancy outcomes. N Engl J Med 2005;352:2477–86.
NICE. Diabetes in pregnancy. NICE clinical guideline 63, July 2008. www.nice.org.uk
Royal College of Obstetricians and Gynaecologists (RCOG). Chickenpox in pregnancy. Guideline No: 13, July 2001. Royal College of Obstetricians and Gynaecologists. www.rcog.org.uk
RCOG. Anti-D Immunoglobulin for Rh Prophylaxis. Guideline no. 22, May 2002. Royal College of Obstetricians and Gynaecologists. www.rcog.org.uk
RCOG. Management of HIV in pregnancy. Guideline no. 39, April 2004. Royal College of Obstetricians and Gynaecologists. www.rcog.org.uk
NICE. The use of routine antenatal anti-D prophylaxis for RhD-negative women. May 2002. www.nice.org.uk
Wald NJ, Rodeck C, Hackshaw AK, et al. First and second trimester antenatal screening for Down’s syndrome: the results of the Serum, Urine and Ultrasound Screening Study (SURRUS), Health Technology Assessments 2003: 7(11); www.hta.nhsweb.nhs.uk
Yankowitz J, Pastorek II JG. Maternal and fetal viral infections including listeriosis and toxoplasmosis. In: James DK, Steer PJ, Weiner CP, Gonik B. High risk pregnancy management options. W.B Saunders 1999: 525–58. Internet resources and patient information:
www.rcog.org.uk
www.nice.org.uk
www.screening.nhs.uk/an
www.arc-uk.org