Chapter 12 Reproduction
Ambiguous genitalia
Anatomy of female pelvis
Chronic pelvic pain
Contraception
Disorders of sex development
Donor insemination
Heavy menstrual bleeding
Dysmenorrhoea
Ectopic pregnancy
Embryo freezing
Emergency contraception
Endometriosis
Female infertility
Fertility in survivors of childhood malignancy
Imaging in reproductive medicine
Induction of ovulation
Intracytoplasmic sperm injection
Intrauterine devices
In vitro fertilization
In vitro oocyte maturation
Malformations of the genital tract
Male subfertility
Menopause and hormone replacement therapy
Menorrhagia
Menstrual cycle: physiology
Miscarriage: early
Oocyte donation
Oligomenorrhoea and amenorrhoea
Ovarian hyperstimulation syndrome
Paediatric and adolescent problems
Polycystic ovary syndrome
Preimplantation genetic diagnosis
Premature ovarian failure
Premenstrual syndrome
Psychosexual problems
Recurrent miscarriage
Termination of pregnancy Ambiguous genitalia
Definition
The genitalia are considered ambiguous when they are atypical in appearance and it is not possible to assign gender merely by inspection of the genitalia.
Incidence
About 1 in 4000 births. Aetiology
Normal sexual differentiation
Genetic sex is determined at the time of conception when the ovum is fertilized by a spermatozoa containing either X or Y chromosome. The developing gonad is indifferent until about 7 weeks of gestation and both sexes develop Müllerian and Wolffian ducts.
In a male fetus, the SRY (sex determining region of the Y chromosome) and testes-determining factors (TDFs) promote the differentiation of the gonad into testes. Ovarian development was considered to be a default position in the absence of the SRY gene, although recently ovarian-determining genes have been found.
Hormonal production by the developing testes determines phenotypic sex. The Sertoli cells produce anti-Müllerian hormone (AMH), which cause regression of the Müllerian duct. Around 8 weeks, the Leydig cells produce testosterone, which promotes the development of the Wolffian duct into the epididymis, seminal vesicles, and the vas deferens. Testosterone is converted by the enzyme 5-α-reductase to dihyrotestosterone (DHT), which causes the growth of the phallus, fusion of the urethral folds to create an opening at the tip of the penis, and fusion of labioscrotal folds to form the scrotum. Masculinization of the external genitalia is complete by 14 weeks and the penis, similar in size to the clitoris at 14 weeks, starts to grow from 20 weeks until birth.
In the female fetus, the absence of AMH causes the development of the Müllerian ducts into the Fallopian tubes, uterus, and upper portion of the vagina. In the absence of androgens, the urogenital sinus develops into the clitoris, labia, and the lower part of the vagina.
Pathophysiology of ambiguous genitalia
The older terminology for ambiguous genitalia included true hermaphroditism, pseudo-hermaphroditism, and intersex. These terminologies are generally unhelpful as a descriptor of the phenotypic abnormality and are considered pejorative by patient groups. Following international consensus, the terminology used for these conditions is disorders of sex differentiation (DSD).
The pathophysiology of the conditions that lead to ambiguous genitalia are essentially caused by overvirilization of an XX fetus (XX, DSD) or undervirilization of an XY fetus (XY, DSD).
As the development of the female external genitalia is essentially an autonomic process, genital ambiguity in a female fetus with normal ovaries can only happen when it is exposed to an environment where there is an excess of androgens. This can occur because of abnormalities in the fetal adrenal gland or placenta, or because of effects of exogenous androgens in the maternal circulation, which crosses the placenta.
The development of the male external genitalia is an active process and undervirilization of the external genitalia can cause genital ambiguity. This can be due to abnormalities in testicular development, failure to convert testosterone into dihyrotestosterone, which is the androgen responsible for virilization of the external genitalia (5-α-reductase deficiency), or abnormalities in the androgen receptor (androgen insensitivity syndrome (AIS)).
In some cases, testicular and ovarian tissue may be present in the same individual. This condition previously called true hermaphroditism is now termed ovo-testicular DSD.
The causes of ambiguous genitalia are listed in Table 12.1.1.
Congenital adrenal hyperplasia
Congenital adrenal hyperplasia (CAH) is the most common cause of virilization of a female fetus. It is most commonly due to 21 hydroxylase deficiency, an autosomal recessive disorder that leads to glucocorticoid and mineralocorticoid deficiency. This leads to excessive production of adrenocorticotropic hormone (ACTH), adrenal hyperplasia, accumulation of precursors prior to the enzymatic defect, and excess production of androgens due to diversion of the precursors along the androgen pathway.
This commonly presents as ambiguous genitalia in a female fetus, salt-losing crisis in male fetuses, or a general failure to thrive. In female fetuses, the clitoris is enlarged, the labia partially fused and rugose, and a common urogenital sinus is present instead of separate urethral and vaginal orifices. The internal genitalia are those of a normal female.
Androgen insensitivity syndrome
This syndrome is due to an abnormality of the androgen receptor. Despite the presence of normal levels of androgens, the phenotype is either female or ambiguous.
Complete AIS (CAIS) was previously known as testicular feminization syndrome. This terminology is considered offensive by patient groups and is no longer recommended. The typical presentation of CAIS is of primary amenorrhoea at puberty with normal breast development and pubertal growth spurt.
There is absence or scanty pubic and axillary hair, the vagina is often underdeveloped and the uterus and Fallopian tubes are absent.Table 12.1.1 Causes of ambiguous genitalia

CAIS can also present as bilateral inguinal hernias in female infants, which is otherwise a rare condition and should prompt investigation to exclude CAIS.
It should be noted that CAIS does not present as ambiguous genitalia, as the phenotype is of a normal female infant.
Partial androgen insensitivity syndrome (PAIS) encompasses a spectrum of conditions where there is partial response to androgens during development. It often presents as ambiguous genitalia with penoscrotal hypopadias, micropenis, and a bifid scrotum. In the most severe cases, it may present as isolated clitoromegaly only marginally varying from CAIS. In the mildest form, it may present as isolated hypospadias which may be severe.
5-α-reductase deficiency
This often presents with either ambiguous genitalia or phenotypically female infants who go on to develop significant virilization at puberty and in some cases to change of gender. The underlying cause is a defect in the enzyme 5-α-reductase, which coverts testosterone to the more potent DHT, which is required for virilization of the external genitalia. At puberty, virilization occurs under the influence of testosterone. The condition is inherited as an autosomal recessive trait and it is more common in some geographical areas such as the Dominican Republic.
The phallus is small and the urethral opening is situated in the perineum. The vagina is absent or inconspicuous and the testes are usually present in the inguinal region. Clinical approach
Diagnosis
History
• Maternal drug intake: progestogens cause virilization in a female fetus and cyproterone causes undervirilization in a male fetus.
• Maternal history of virilization during pregnancy: in placental aromatase deficiency, the fetal androgens which are not metabolized by the placenta cross into the maternal circulation and cause virilization.
• Family history: AIS is X linked, CAH-autosomal recessive. 5-α-reductase deficiency and 17 β-hydroxysteroid dehydrogenase deficiency is more common in consanguineous couples. Family history of neonatal deaths, problems at puberty and unexplained infertility may point to underlying syndromes.
Examination
• General examination of the infant should be carried out to exclude other morphological abnormalities that may point to a syndrome complex.
• Rarely, the mother may show signs of virilization suggesting either a functional tumour (adrenal/ovarian) or placental aromatase deficiency.
• Abnormal skin hyperpigmentation is suggestive of CAH as the increased production of ACTH stimulates melanocyte production.
• Assessment of the phallus requires care, as chordee is usually present resulting in the phallus appearing smaller than it actually is.
• The position of the urethral orifice should be ascertained, although this may be difficult to determine until the infant voids. This may be present either on the phallus or on the perineum, the position determines the degree of hypospadias.
• The colour and rugosity of the labioscrotal folds should be assessed: hyperpigmentation is suggestive of CAH and rugosity is suggestive of exposure to androgens.
The presence or absence of a vagina
• Palpation of the gonad requires practise and patience. With the thighs abducted, gentle palpation of the inguinal region starting above the inguinal ring towards the external genitalia is performed. The presence of a palpable gonad in this region indicates a male infant, as in cases of ambiguous genitalia in female infants, the ovaries are in their normal intra-abdominal position.
Investigations
The investigations to be undertaken in cases of ambiguous genitalia are listed in Table 12.1.2. As CAH is the most common cause of ambiguous genitalia, initial investigations should focus on excluding this condition. Simultaneous determination of sex chromosome status should be carried out using fluorescent in situ hybridization (FISH).
Counselling
• Ambiguous genitalia constitutes one of the most distressing situations for parents because of the uncertainty regarding the most basic identity of their newborn child.
• It is advisable to avoid speculation regarding the gender. Instead, parents should be told that there is a problem identifying the gender and further investigations are required.
• Counselling of the parents should be performed by an experienced member of the team who will care for the child.
• Once the diagnosis has been established, a further discussion should occur with the parents regarding the long-term prognosis, including the need for hormonal treatment and impact on future fertility.
• The impact of prenatal exposure of androgens on the developing female brain may impact on future behaviour and gender identity.
• As many causes of ambiguous genitalia have an inherited basis, the parents should be informed regarding the inheritance pattern and counselled regarding the implication for other siblings and future pregnancies.
Management Management of CAH
• In the salt-losing form of CAH, presentation may be in the form of circulatory collapse or failure to thrive.
• Hyperkalaemia is one of the first signs, and serum electrolytes should be measured regularly.
• Replacement glucocorticoids and mineralocorticoids should be given.
• Hormonal therapy is required lifelong with additional higher doses required for surgical interventions.
• In fetuses at risk of developing CAH, CVS or amniocentesis may be considered with a view to commencing steroid therapy for affected females. Dexamethasone given prenatally suppresses the fetal hypothalamo-adrenal axis and prevents virilization in about 85% of cases. This treatment is controversial as the long-term effects of antenatal dexamethasone is unknown and should only be carried out in a specialist centre.
Assignment of gender of rearing
• Management of these children should be carried out by a multidisciplinary team that includes neonatologists, paediatric surgeons/urologists, endocrinologists and psychologists.
Table 12.1.2 Investigations in cases of ambiguous genitalia

• Factors influencing gender assignment include diagnosis, appearance of the genitalia, surgical options, need for hormonal therapy, fertility, parental wishes, and possibly cultural factors.
• More than 90% of 46,XX CAH and all cases of 46,XY CAIS reared as female identify with female gender. This supports the concept of raising even severely virilized female infants as female gender.
• The allocation of gender in 5-α-reductase deficiency and PAIS is more problematic. Around 60% of children with 5-α-reductase deficiency raised as girls will virilize at puberty and will have gender reassignment. About 25% of individuals with PAIS are dissatisfied with the gender of rearing whether male or female.
• Male infants with micropenis should be raised in the male gender. The severity of hypospadias is not necessarily a determining factor in gender assignment as it is often surgically correctable.
Surgery for ambiguous genitalia
• It has long been considered that children have a gender neutral identity until the age of 3 and that it is therefore necessary to assign gender by this age. Recently, this concept has been challenged as it is recognized that this is a gradual process.
• In cases of severe virilization of a female fetus, feminizing genital surgery was often carried out soon after birth. The aim was to restore the genitalia to a more ‘normal’ appearance allaying parental anxiety and confirming gender identity.
• Feminizing genitoplasty involves surgery to reduce the size of the clitoris, create or enlarge a vaginal orifice and reduce the size of the labia.
• Such surgery has come under the spotlight in recent years, particularly with adult patients claiming a feeling of ‘being mutilated’ following such surgery.
• There is growing evidence of the adverse impact of such surgery particularly on the clitoris and problems with sexual function in adulthood.
• Vaginoplasty procedures performed in children often require a revision procedure during adolescence because of stenosis.
• Clitoral surgery includes clitoredectomy (no longer recommended), clitoral recession (where the corpora are hitched under the symphysis; this can cause painful erections), and clitoral reduction (conserving the neurovascular bundle).
• The timing of such surgery is controversial and hotly debated in view of the potential adverse long-term outcomes.
• In cases of mild clitoromegaly, it is appropriate to avoid surgery.
• There are calls to defer such surgery until adolescence to enable the individual to play a major role in giving informed consent. This must be balanced against the potential psychological distress to both the individual and the parents from the uncorrected ambiguous genitalia.
• This type of surgery should only be performed in specialist centres with long-term follow up of outcomes.
• A historical difficulty in assessing the impact of such surgery has been that there has often been non-disclosure of the condition to the affected individual. It is currently recommended that full disclosure should be made so that individuals are able to access appropriate support and information.
Gonadectomy
Gonadectomy is often required when a 46,XY infant is assigned to a female gender of rearing. This is often required to prevent virilization at puberty. Dysgenetic gonads have a significant risk of malignancy and should be removed.
The timing of gonadectomy is discussed further in Section 12.5, Disorders of sex development. Further reading
Aaronson IA. The investigation and management of the infant with ambiguous genitalia: a surgeon’s perspective. Curr Probl Paediatr 2001;31:168–94.
Berra M, Liao LM, Creighton SM, Conway GS. Long-term health issues with women of XY karyotype. Maturitas 2010;65:172–78.
Hindmarsh PC. Management of a child with Congenital Adrenal Hyperplasia. Best Pract Res Clin Endocrin Res 2009;23:193–208.
Hughes IA, Deeb A. Androgen resistance. Best Pract Res Clin Endocrin Res 2006;20:577–98.
Lee PA, Houk CP, Ahmed SF, Hughes IA. Consensus Statement on the Management of Intersex Disorders. Paediatrics 2006; 118: e488–e500.
Merke DP, Bornstein SR. Congenital Adrenal Hyperplasia. Lancet 2005;365:2125–36.
Michala L, Creighton SM. The XY female. Best Pract Res Clin Obstet Gynaecol 2009; 1–10.
Rangecroft L 2003. Surgical management of ambiguous genitalia. Arch Dis Child; 88: 799–801.
Zucker KJ. Intersexuality and gender identity differentiation. J Paediatr Adolesc Gynecol 2002;15:3–13. Patient resources
Androgen Insensitivity Syndrome Support Group www.aissg.org Intersex Society of North America www.isna.org
Anatomy of female pelvis Introduction
A clear understanding of the anatomy of the female pelvis is essential for practising obstetricians and gynaecologists. Knowledge of specific anatomical relationships between the bony pelvis and its associated muscles and ligaments, blood vessels, lymphatics and pelvic viscera helps in the diagnosis as well as management of disorders affecting the female genital tract. Meticulous knowledge of normal anatomy as well as recognition of ‘distorted anatomy’ may help to avoid unintended damage to adjacent structures during pelvic surgery, such as ureteric damage, while ligating uterine arteries during a hysterectomy. Similarly, precise anatomical knowledge of pelvic vasculature may be life saving, as in ligation of internal iliac arteries during massive obstetric or gynaecological haemorrhage. The bony pelvis
The pelvis is formed of four bones: two hip bones laterally and in front and the sacrum and coccyx behind. The hip bones are fused iliac, ischial, and pubic bones. The ischium and pubis also meet below, in the centre of the inferior ramus, to form the obturator foramen. The arcuate line that extends from the sacral promontory to the pectineal line of the pubis divides the pelvis into bowl-shaped false and a circular true pelvis. The urogenital organs lie in the true pelvis.
A low midline incision allows a direct approach into the true pelvis. The bony landmarks for the pelvic surgeon are the anterior and posterior iliac spines, the iliac crests, the pubic tubercles, and the ischial tuberosities. Fig. 12.2.1 illustrates the parts of an articulated bony pelvis.
Cooper’s (pectineal) ligament overlies the pectineal line and offers a sure hold for sutures in prolapse repairs and urethral suspension procedures. The ischial spine is palpable transvaginally and provides attachment to the pelvic diaphragm and the sacrospinous ligament.
The sacroiliac joints are strong synovial joints and least prone to fractures. The pubic bones are the thinnest of the pelvic bones, are more prone to fractures, and their fragments may injure the adjacent bladder, urethra, and vagina. Diameters of the pelvic inlet, midcavity, and outlet influence the mechanism of human labour and these are given in Table 12.2.1.

Fig. 12.2.1 The bony pelvis.
Table 12.2.1 Diameters of the pelvic planes

Soft tissues of the pelvis
Muscles of the pelvis
The pelvic floor
The pelvic floor is composed of a funnel-shaped wide and thin fibromuscular tissue forming the inferior border of the abdominopelvic cavity. It separates the structures in the pelvis from the perineum and ischeorectal fossae and extends from midway of the symphysis pubis to the coccyx and from one lateral pelvic sidewall to the other. The primary muscles of the pelvic diaphragm are the levator ani and the coccygeus.
The levator ani muscles forms the bulk of the pelvic diaphragm and has three parts named after their origin and insertion: pubococcygeus, iliococcygeus, and ischiococcygeus. It arises from the tendinous arch extending from the posterior aspect of the body of pubis, arcuate line (or the ‘white line’) on the obturator fascia, to ischial spine. The coccygeus is a triangular muscle that occupies the area between the ischial spine and the coccyx.
The paired levator ani muscles act as a single muscle. It is pierced in the midline by urethra, vagina, and anal canal, and, hence plays an important role in the control of urination, in parturition, and in maintaining faecal continence. Fig. 12.2.2 illustrates the muscular attachments of the pelvic floor.
Urogenital diaphragm
The urogenital diaphragm is a strong muscular membrane that lies external and inferior to the pelvic diaphragm. It occupies the area between the pubis symphysis and ischial tuberosities anteriorly and has two layers that enclose the deep transverse perineal and sphincter urethrae muscles. These muscles surrounds both the vagina and the urethra. The urogenital diaphragm reinforces the pelvic diaphragm and provides support to the urethra and maintains the urethrovesical junction.
Perineal body or the central perineal tendon
The perineal body is a pyramidal shaped fibromuscular tissue located in the midline between the anus and the vagina, forming a ‘hub’ for supporting the pelvic viscera. The superior border of the perineal body represents the point of insertion of rectovaginal (Denonvilliers’) fascia, which extends to the underside of the peritoneum covering the Pouch of Douglas, separating the ano-rectum from the urogenital compartment. The perineal body represents the point of fusion between the free posterior edge of the urogenital diaphragm and the posterior apex of the urogenital hiatus. Virtually every muscle of the perineum (superficial and deep transverse perinei, bulbocavernosus, levator ani, external anal sphincter, striated urethral sphincter) and fascia (perineal membrane, Denonvilliers’, Colles’, and endopelvic) are attached to the perineal body. At its core are abundant elastin smooth muscle fibres which are richly innervated, which suggests that it may have a dynamic role in supporting the genital tract. Fig 12.2.3 illustrates the perineal body.

Fig 12.2.2 The muscles of the pelvic floor (‘pelvic diaphragm’).
The perineal body is also an important part of the pelvic floor as it supports the lower vagina, and its weakness predisposes to defects such as rectocele and enterocele.
The endopelvic fascia and ligaments form a system of connective tissue interlaced with elastin, smooth muscle cells, fibroblasts, and vascular structures. It lies immediately beneath the peritoneum and is a single continuous unit with various thickenings or condensations in specific areas. Over the viscera, it merges with the visceral fascia and is very thin. This allows for displacements and changes in volume of the uterus, bladder, and rectum. Anteriorly, laterally, and posteriorly the endopelvic fascia gets condensed and thickened to form strong ligaments that support the pelvic visera. The urinary bladder and urethra are attached to the pelvic walls by pubovesical and pubourethral ligaments and the uterus by the pubocervical ligaments, lateral sacral (Cardinal), and uterosacral ligaments, respectively, to the bony pelvis. Blood supply in the pelvis
Ovarian artery
The ovarian arteries arise from the anteriolateral aspect of the aorta just below the renal vessels and run downwards in the retroperitoneal space. The right ovarian artery crosses the anterior surface on vena cava, the lower part of the ‘abdominal’ ureter on the right side and then runs lateral to the ureter. It then enters the pelvis via the infundibulopelvic ligament. The left artery crosses the ureter almost immediately after its origin at just below the left renal artery and then runs in the retroperineal space, crossing the bifurcation of the common iliac artery at the pelvic brim to enter the infundibulopelvic ligament.
Fig 12.2.3 External genitalia and the perineal body.

The blood supply to the ovary and lateral aspects of the fallopian tubes is derived from the numerous small branches of the ovarian artery as it passes through the mesovarium. The ovarian artery ends by anastomosing with the tubal branch of the uterine artery in the mesovarium.
Common iliac artery
The aorta bifurcates at the level of the fourth lumbar vertebra into two common iliac arteries, each being approximately 5 cm long until dividing into the external and internal iliac arteries.
The internal iliacs, or hypogastric arteries, are approximately 3–4 cm in length and are responsible for supplying structures of the pelvis. Throughout their course they are in close proximity to the ureters and divide into a larger anterior and a small posterior branches. The posterior division has three branches: the iliolumbar, lateral sacral, and superior gluteal arteries and provides blood supply to the lumbosacral and gluteal region.
The larger anterior division has parietal and visceral branches. The three parietal branches are the obturator and the terminal branches, internal pudendal, and inferior gluteal arteries. The six visceral branches include the umbilical, middle vesical, inferior vesical, middle rectal, uterine, and vaginal arteries. The superior vesical artery usually arises from the umbilical artery.
Uterine artery
The uterine artery is a branch of the anterior division of the internal iliac artery and runs medially towards the isthmus of the uterus. Approximately 2 cm lateral to the endocervix, it crosses above the ureter and reaches the lateral wall of the uterus. The ascending branch of the uterine artery courses in the broad ligament, with a tortuous route and ends by anastomosing with the ovarian artery in the mesovarium.
Throughout its tortuous course in the parametrium, the uterine artery gives off numerous branches that unite with arcuate arteries from the opposite side. Arcuate arteries develop radial branches that supply the myometrium, which give rise to basilar arteries that supply the basalis layer of the endometrium. The basilar arteries give rise to the spiral arteries that supply the functional layer of the endometrium. The descending branch of the uterine artery branches to both the cervix and the vagina. In each case, the vessels enter the organ laterally and anastomose freely with vessels from the opposite side.
Surgical management of postpartum haemorrhage includes ligation of the anterior division of internal iliac artery. Owing to extensive collateral circulation, this occlusion does not cause hypoxia of the pelvic viscera but reduces haemorrhage by decreasing the arterial pulse pressure. Fig. 12.2.4 illustrates the blood supply to the pelvis.
Vaginal artery
The vaginal artery may arise either from the anterior trunk of the internal iliac or from the uterine artery. It supplies blood to the vagina, bladder, and rectum. There are extensive anastomoses with the vaginal branches of the uterine artery to form the ‘azygos plexus’ of arteries of the cervix and vagina.
Internal pudendal artery
This artery is the terminal branch of the internal iliac artery and supplies branches to the rectum, labia, clitoris, and perineum.
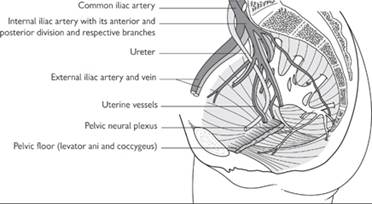
Fig. 12.2.4 Blood vessels of the pelvis. Veins
The veins of the female pelvis and perineum are thin walled with few valves. The venous drainage of the pelvis begins in small sinusoids that drain to numerous venous plexuses within or immediately adjoining the pelvic organs and follow the course of the arterial supply.
The venous drainage of the ovaries is an exception. The left ovarian vein empties into the left renal vein, whereas the right ovarian vein directly drains into the inferior vena cava. Nerve supply
The pelvis is richly innervated by both autonomic and somatic nervous systems.
Autonomic nerves
The sympathetic supply is derived from the lower part of lumber sympathetic chain and the aortic plexus which continues downwards over the bifurcation of the aorta to form the hypogastric plexus. This divides into right and left pelvic plexuses, which lie lateral to the rectum and are subdivided into anterior innervations for the bladder and urethra and posterior innervations for the uterus, cervix, vagina, sigmoid colon, and rectum.
Parasympathetic nerves
The parasympathetic nerves enter the pelvis through second, third and fourth sacral nerves. The pre-ganglionic fibres are distributed through the pelvis plexus and the parasympathetic ganglia are situated close or in the walls of the viscera. All the internal pelvic organs are supplied by the pelvic plexus. However, the ovaries and fallopian tubes are supplied directly by nerves from the pre aortic plexus travelling along the ovarian vessels.
Somatic nerves
The lumbosacral plexus and its branches provides motor and sensory innervations to the lower abdominal wall, the pelvic and the urogenital diaphragms, the perineum, hip, and lower extremity Lymphatic drainage
Lymph nodes are arranged along the blood vessels. The structures supplied by the aorta, i.e. ovary, fallopian tubes, upper ureter, and uterine fundus drain directly to lateral aortic group of nodes.
The lymph drainage of most other structures within the pelvis is via more distant groups of lymph nodes associated with iliac vessels (i.e. internal iliac and common iliac nodes). Anatomy of the female reproductive tract
External genitalia
External genital organs in females include the mons pubis, clitoris, urinary meatus, labia majora, labia minora, vestibule, Bartholin’s glands, and periurethral glands. These are often collectively referred as the ‘female perineum’.
The internal genital organs are located in the true pelvis and include the vagina, cervix, uterus, fallopian tubes, ovaries, and surrounding supporting structures.
The perineum is a diamond shape area bounded anteriorly by lower margin of symphysis pubis, posteriorly by the tip of coccyx, and laterally by the ischial tuberosities and sacrotuberous ligaments. An imaginary line joining the ischial tuberosities divides this area into an anterior urogenital triangle and a posterior anal triangle.
The urogenital triangle contains the vulva and the urethral opening, and the anal triangle includes lower end on anal canal. The external anal sphincter surrounds the anal canal and the ischeorectal fossae are on either side of the anal canal. Posteriorly, the anococcygeal body lies between the anus and the tip of the coccyx and consists of thick fibromuscular tissue supporting the rectum and lower part of the anal canal.
The vulva refers to an area that extends anteriorly from the mons pubis to the rectum, posteriorly and is bounded by genitocrural folds laterally. The entire vulval area is covered by keratinized, stratified squamous epithelium.
Mons pubis: this is a triangular eminence directly anterior and superior to the symphysis pubis. It becomes hairy after puberty.
Labia majora: these are a pair of longitudinal cutaneous folds of fibroadipose tissue measuring 7–8 cm in length and 2–3 cm in width. They extend from the mons pubis anteriorly and fuse in the midline between the vagina and the anus at the posterior fourchette. The skin of the outer convex surface of the labia majora is pigmented and covered with hair follicles. The inner surface is devoid of hair follicles but is rich in sebaceous glands. Histologically, the labia majora have both sweat and sebaceous glands.
Labia minora: these are a pair of small red cutaneous folds situated between the labia majora and the vaginal orifice. Anteriorly, they separate at the clitoris to form superiorly the prepuce and inferiorly the frenulum of the clitoris. Posteriorly, they merge at the posterior fourchette. Histologically, they are composed of dense connective, elastic, and erectile tissues. The skin is rich in sebaceous glands, but it has no hair follicles or sweat glands.
Clitoris: it is a short, cylindrical, erectile organ at the superior portion of the vestibule measuring approximately 1.5–2 cm in length and 1 cm in width. The base of the clitoris consists of two crura, attached to the periosteum of the symphysis pubis. The body has two cylindrical corpora cavernosa composed of thin-walled, vascular channels that function as erectile tissue. The distal one-third of the clitoris is the glans, richly supplied by nerve endings
Hymen: this is a thin usually perforated fibrous tissue covered by stratified squamous epithelial membrane present at the entrance of the vagina.
The vestibule is the cleft between the labia minora extending from the clitoris to the posterior fourchette. The urethral meatus, vaginal orifice, and ducts of the Bartholin’s glands open into the vestibule.
Urethra: This is immediately anterior to the vaginal orifice and about 2 cm beneath the clitoris. The female urethra measures 3.5–5 cm in length. The proximal two-thirds of the urethra is composed of stratified transitional epithelium, whereas the distal one-third is stratified squamous epithelium. Internal genitalia
Vagina
The vagina is a thin-walled, distensible, fibromuscular tube that extends posterosuperiorly from the vestibule to the uterus. The vagina is attached at a higher point posteriorly than anteriorly; therefore, the posterior wall is 9 cm and the anterior is 7 cm long. The potential space of the vagina is larger in the middle and upper thirds. The walls of the vagina are normally in apposition except superiorly at the vault, where they are separated by the cervix. The vault of the vagina is divided into four fornices: posterior (deepest), anterior, and two lateral.
The axis of the upper vagina lies fairly close to the horizontal plane when a woman is standing, with the upper portion of the vagina curving toward the hollow of the sacrum. In most women an angle of at least 90° is formed between the axis of the vagina and the axis of the uterus.
Vagina supports: the vagina is held in position by the surrounding endopelvic fascia and ligaments. The lower third of the vagina is in close relationship with the urogenital and pelvic diaphragms. The middle third of the vagina is supported by the levator ani muscles and the lower portion of the cardinal ligaments. The upper third is supported by the upper portions of the cardinal ligaments and the parametrium.
Histologically the vagina is composed of four distinct layers.
• The vagina is lined by stratified, non-keratinized squamous epithelium that is firmly attached to the underlying muscle. The epithelium is thick and rich in glycogen, which increases in the post-ovulatory phase of the menstrual cycle. There are no glands in the vagina and it is lubricated from the mucus secretion from the cervix. Vaginal lubrication also occurs from a transudate produced by engorgement of the vascular plexuses that encircle the vagina.
• The second layer is of collagen and elastic tissue- lamina propria. It is composed of fibrous connective tissue. This is rich in vascular and lymphatic channels.
• The muscular layer has many interlacing fibres. There is an inner circular layer and an outer longitudinal.
• The fourth layer consists of cellular areolar connective tissue containing a large plexus of blood vessels.
Blood supply: the vagina derives its blood supply from the vaginal artery and branches from the uterine, middle rectal, and internal pudendal arteries
The nerve supply of the vagina comes from the autonomic nervous system’s vaginal plexus, and sensory fibres come from the pudendal nerve. Pain fibres enter the spinal cord in sacral segments S2, S3, and S4.
The primary lymphatic drainage of the upper third of the vagina is to the external iliac nodes, the middle third of the vagina drains to the common and internal iliac nodes, and the lower third has a complex and variable distribution, including the common iliac, superficial inguinal, and pararectal nodes.
Uterus
The uterus is a thick-walled hollow fibromuscular organ located centrally in the female pelvis with the urinary bladder anteriorly and the rectum posteriorly. The fallopian tubes enter the uterine cavity at the cornua in the superolateral aspects. The uterus is often described as an inverted pear-shaped structure and is divided into the upper uterine body and lower cervix. The uterine body has a dome-shaped fundus superiorly and an isthmus inferiorly. The latter is a short area of constriction in the lower uterine segment. The lower edge of the fundus is limited by an imaginary line drawn between the attachments of each Fallopian tube. A typical nulliparous uterus measures 8 cm long, 5 cm wide, and 2.5 cm thick and weighs 40–50 g.
The uterus has three layers: the thin, external serosal layer; the middle muscular layer, the myometrium; and the inner mucous layer, the endometrium. The serosal layer is the visceral peritoneum. The peritoneum is firmly attached to the uterus in all areas except anteriorly at the level of the internal os of the cervix.
The muscular layer is 1.5–2.5 cm thick and has three indistinct layers of smooth muscle. The outer longitudinal layer is continuous with the muscle layers of the fallopian tubes and vagina. The middle layer has interlacing oblique, spiral bundles of smooth muscle, and large venous plexuses. The inner muscular layer is also longitudinal.
The endometrium is a reddish mucous membrane that varies from 1 to 6 mm in thickness, depending on hormonal stimulation. The uterine glands are tubular and composed of tall columnar epithelium. The endometrium may be divided into an inner stratum basale and an outer stratum functionale. The stratum functionale may be further subdivided into an inner compact stratum and a more superficial spongy stratum. Only the stratum functionale responds to fluctuating hormonal levels.
Blood supply: the blood supply to the uterus is the uterine artery which anastomoses with the ovarian and vaginal arteries.
The lymphatic drainage of the uterus is complex. The majority of lymphatics from the fundus and the body of the uterus go to the aortic, lumbar, and pelvic nodes surrounding the iliac vessels, especially the internal iliac nodes. However, it is possible for metastatic disease from the uterus to be found in the superior inguinal nodes transported via lymphatics in the round ligament. This is because the round ligament is attached to the fibrofatty tissue of the labia majora. Nerve supply to the uterus is via the uterovaginal plexus of nerves.
Cervix: the lower narrow portion of the uterus is the cylindrical shaped cervix. It is predominantly composed of fibrous tissue.
Its attachment to the vagina divides it into an upper supravaginal portion and a lower part in the vagina called the ectocervix or portio vaginalis The ureter runs about 1 cm laterally to the supravaginal cervix. The length of the endocervical canal is 2.5–3 cm and it opens proximally into the endometrial cavity at the internal os and distally into the vagina at the external os.
The ectocervix is lined by stratified squamous epithelium and the endocervix is lined by mucus-secreting columnar epithelium. The junction of these two epithelia, the ‘squamo-columnar junction’, is hormonal sensitive. This very active ‘transformation zone is believed to be the site of origin of cervical cancers.
The arterial supply of the cervix is from the descending branch of the uterine artery. There are numerous anastomoses between these vessels and the vaginal and middle rectal arteries. The major arterial supply to the cervix is located on the lateral cervical walls at the 3 and 9 o’clock positions, respectively. Therefore a deep figure-of-eight suture through the vaginal mucosa and cervical stroma at 3 and 9 o’clock helps to reduce blood loss during procedures such as cone biopsy.
The venous drainage accompanies these arteries. The lymphatic drainage of the cervix involves multiple chains of nodes. The principal regional lymph nodes are the obturator, common iliac, internal iliac, external iliac, and visceral nodes of the parametrium. Other possible lymphatic drainage includes the following chains of nodes: superior and inferior gluteal, sacral, rectal, lumbar, aortic, and visceral nodes over the posterior surface of the urinary bladder. The stroma of the endocervix is rich in free nerve endings. Pain fibres accompany the parasympathetic fibres to the second, third, and fourth sacral segments.
Fallopian tubes
The fallopian tubes are 10 cm long, paired hollow structures representing the ‘unfused’ Mullerian ducts. The fallopian tubes connect the cornua of the uterine cavity and the peritoneal cavity. They arise from the superolateral portion of the uterus and travel along the upper margin of the broad ligament and end in the peritoneal cavity close to the ovary.
Each tube is divided into four anatomic sections.
1. Intramural or interstitial: 1–2 cm in length and is surrounded by myometrium. It lies within the uterine wall and forms the tubal ostia at the endometrial cavity.
2. Isthmus: the isthmus is narrow and straight and begins as the fallopian tube exits the uterus. It is approximately 4 cm in length and has the most highly developed musculature.
3. Ampulla: this is 4–6 cm in length and approximately 6 mm in diameter. It is wider and more tortuous in its course than other segments. Fertilization normally occurs in the ampullary portion of the tube.
4. Infundibulum: this is the distal trumpet-shaped portion of the tube that is in close proximity to the ovary.
The abdominal ostia of the tube have numerous irregular finger-like projections called fimbriae. One of the largest fimbriae is attached to the ovary and this is called the fimbria ovarica.
The tubal mucosa is ciliated columnar epithelium and is most prominent near the ovarian end of the tube. The mucosa of the oviduct has three different cell types: Columnar ciliated epithelial cells that account for about 25% of the mucosal secretory cells; non-ciliated ‘columnar’ cells that account for about 60% of the epithelial lining and are more prominent in the isthmic segment. The narrow ‘peg cells’ are found between secretory and ciliated cells and are believed to be a morphological variant of secretory cells.
The smooth muscle of the tube is arranged into inner circular and outer longitudinal layers. The tubes are covered by peritoneum. The vascular supply to the fallopian tubes is from the uterine and ovarian arteries, which anastomose in the mesosalpinx. The uterine arteries supply the medial two-thirds of each tube. Lymphatic drainage includes the internal iliac nodes and the aortic nodes surrounding the aorta and the inferior vena cava at the level of the renal vessels. The innervations of the tubes are from the uterovaginal and the ovarian plexus.
Ovaries
The ovaries are paired gonadal structures that lie suspended between the pelvic wall and the uterus by the infundibulopelvic ligaments laterally and the utero-ovarian ligament medially. The infundibulopelvic ligament contains the ovarian artery, ovarian veins, and accompanying nerves. It attaches the upper pole of the ovary to the lateral pelvic wall.
Inferiorly the hilar surface of each ovary is attached to the broad ligament by mesentery (mesovarium).
The ovary is the only intra-abdominal structure not to be covered by the peritoneum. During reproductive years, ovaries weigh 3–6g and measure approximately 1.5 ? 2.5 ? 4 cm.
Each ovary consists of an outer cortex and an inner medulla. The ovarian surface is covered by a single layer of cuboidal epithelium, termed the germinal epithelium. This term is a misnomer because the cells are similar to those of the coelomic mesothelium, which forms the peritoneum. The germinal epithelium is not in any way related to the histogenesis of the Graafian follicles.
If the ovary is transected, numerous transparent, fluidfilled cysts are noted throughout the cortex. Microscopically these are Graafian follicles in various stages of development, active or regressing corpus luteum, and atretic follicles. The stroma of the cortex is composed primarily of closely packed cells around the follicles. These are specialized connective tissue cells that form the theca. The medulla contains the ovarian vascular supply and loose stroma.
Each of the ovarian arteries arises directly from the aorta just below the renal arteries. They descend in the retroperitoneal space, cross anterior to the psoas muscles and internal iliac vessels, and enter the infundibulopelvic ligaments, reaching the mesovarium in the broad ligament. The ovarian blood supply enters through the hilum of the ovary. The venous drainage of the ovary collects in the pampiniform plexus and consolidates into several large veins as it leaves the hilum of the ovary. The ovarian veins accompany the ovarian arteries, with the left ovarian vein draining into the left renal vein, whereas the right ovarian vein connects directly with the inferior vena cava.
The lymphatic drainage of the ovaries is primarily to the aortic nodes adjacent to the great vessels at the level of the renal veins. Nerve supply is from the ovarian plexus and uterovaginal plexus.
Ureters: the ureters are whitish, muscular tubes, 28–34 cm in length, extending from the renal pelvis to the urinary bladder. The ureter is divided into abdominal and pelvic segments.
The abdominal portion of the right ureter is lateral to the inferior vena cava. Throughout its course it is retroperitoneal and runs downwards and medially along the anteromedial surface of the psoas major muscle. It is crossed by four arteries and accompanying veins. They are the right colic artery, the ovarian vessels, the ileocolic artery, and the superior mesenteric artery.
The ureter enters the pelvis anterior to the sacroiliac joint and crosses the bifurcation of common iliac artery. There is a slight variation between the two sides of the female pelvis. The right ureter tends to cross at the bifurcation of the common iliac artery whereas usually the left ureter crosses 1–2 cm above the bifurcation. It then passes along the posterolateral aspect of the pelvis running in front and below the internal iliac artery and its anterior division medial to the obturator nerve and vessels.
Approximately at the level of the ischial spines, the ureter changes its course and runs forward and medially from the uterosacral ligaments to the base of the broad ligament, thereby entering the cardinal ligaments. In the pelvis, the ureter runs forwards and medially through the base of the broad ligament and lateral to the cervix. It is crossed superiorly from the lateral to medial side by the uterine artery. It continues forwards about 1.5 cm lateral to the cervix anterolateral to the upper part of the vagina. The ureter then runs upwards and medially in the vesical uterine ligaments to obliquely pierce the bladder wall. Just before entering the base of the bladder, the ureter is in close contact with the anterior vaginal wall and passing slightly medially enters the bladder at the trigone.
The ureteric mucosa is composed of transitional epithelium. The muscle layer has outer circular and inner longitudinal fibres and it has rich blood supply from renal, ovarian, common iliac, internal iliac uterine, and vesical arteries. These form a longitudinal plexus in the adventitia of the ureter. Nerve supply is through the ovarian and vesical plexus.
Urinary bladder
The urinary bladder is a hollow muscular organ designed for the storage of urine and lies between the symphysis pubis and the uterus. The size and shape of the bladder may vary with the volume of urine it contains. The bladder is divided into two areas which are of physiological significance.
• The base of the bladder lies directly adjacent to the endopelvic fascia over the anterior vaginal wall. It consists of urinary trigone posteriorly and a thickened area of detrusor muscle anteriorly. The three corners of the trigone are formed by the two ureteric orifices and the urethral opening into the bladder. The distance between the uretral orifices is approximately 2.5 cm when empty and 5 cm when the bladder is distended. It is innervated by α-adrenergic sympathetic fibres that maintain continence
• The dome of bladder is the remaining bladder area above the bladder base. This has parasympathetic innervations and is responsible for micturition.
The prevesical or retropubic space of Retzius is the area lying between the bladder and symphysis pubis and is bounded laterally by the obliterated hypogastric arteries. This space extends from the fascia covering the pelvic diaphragm to the umbilicus between the peritoneum and transversalis fascia. The bladder is anterior to the cervix, upper vagina, and part of the cardinal ligament. Laterally it is bounded by the pelvic diaphragm and the obturator internus muscle.
The bladder is lined by transitional cell epithelium. The muscle layer is intermeshing fibres called Detrusor muscle.
The arterial supply of the bladder originates from branches of the hypogastric (internal iliac) artery: the superior vesical, inferior vesical, and middle rectal arteries. The nerve supply to the bladder includes sympathetic and para-sympathetic fibres, with the external sphincter supplied by the pudendal nerve.
Urethra
The female urethra measures 3.5–5 cm in length and extends from the bladder to the vestibule. It runs anteroinferiorly behind the symphysis pubis immediately related to the anterior vaginal wall. It crosses the perineal membrane and ends at the external urethral orifice at the vestibule about 2.5 cm behind the clitoris. The Skene’s tubules, draining the paraurethral glands, open into the lower urethra. There is no true anatomical sphincter to the urethra.
The urethra contains an inner longitudinal layer and outer circular layer of smooth muscle. The perineal membrane begins at the junction of the middle and distal third of the urethra. Proximal to the middle and distal third of the urethra, voluntary muscle fibres derived from the urogenital diaphragm intermix with the outer layer of smooth muscle. This increases urethral resistance and contributing to continence. At the level of the urogenital diaphragm the urethra is encircled by voluntary muscle fibres arising from the inferior pubic ramus to form the so called external sphincter.
The mucosa of the proximal two-thirds of the urethra is composed of stratified transitional epithelium, whereas the distal one-third is stratified squamous epithelium. The distal orifice is 4–6 mm in diameter, and the mucosal edges grossly appear everted.
The vascular supply for the urethra is from the vesical and vaginal arteries and the branches from the internal pudendal artery. The nerve supply is from the vesical plexus and the pudendal nerve.
The rectum: the rectum is the terminal 12–14 cm portion of the large intestine. It begins at the level of third sacral vertebrae where the sigmoid colon loses its mesentery and follows the curve of the lower sacrum and coccyx, becoming entirely retroperitoneal at the level of the recto-uterine pouch. The rectum continues along the pelvic curve just posterior to the vagina until the level of the anal hiatus of the pelvic diaphragm. At this point, it takes a sharp 90° turn posteriorly, becoming the anal canal, and is separated by the vagina by the perineal body. The rectum, unlike other areas of the large intestine, does not have taeniae coli or appendices epiploicae.
The rectal mucosa is lined by a columnar epithelium and characterized by three transverse folds that contain mucosa, submucosa, and the inner circular layer of smooth muscle. The rectum receives a rich arterial supply originating from five arteries: the superior rectal artery, which is a continuation of the inferior mesenteric; the two middle rectal arteries; and the two inferior rectal arteries.
Anal canal
The anal canal is 3 cm long and passes downwards and backwards from the rectum. At the anorectal junction the mucosa changes to stratified squamous epithelium, which continues until the anal verge, where there is transition to perianal skin. The circular muscle of the rectum continues down to form the internal anal sphincter. The lower part of the anal canal is surrounded by striated muscle fibres, the external anal sphincter.
The anal canal is slit-like when empty but distends greatly during defaecation. Anteriorly it is related to perineal body and lower vagina, whereas posteriorly it is related to the anococcygeal body. Faecal continence is primarily provided by the puborectalis muscle and the internal and external anal sphincters. The blood supply is from the superior, middle, and inferior rectal arteries and the nerve supply is from the middle rectal plexus, inferior plexus and the pudendal nerve. Conclusion
Understanding the normal anatomy of the pelvis is vital for practising obstetricians and gynaecologists. This will help in diagnosis and management of gynaecological disorders as well as planning and performing pelvic surgery. Distortion of pelvic anatomy may result in inadvertent unintended damage to pelvic organs during surgery. Knowledge of anatomy may also help in the prevention and management of genital tract prolapse, and urinary and fecal incontinence that may result from childbirth. Further reading
Norton PA. Pelvic floor disorders: the role of fascia and ligaments. Clin Obstet Gynecol 1993;36:926–38.
Mukhopadhyay S, Arulkumaran S. Anatomy of the female pelvis. Chapter In: Essentials of obstetrics. Jaypee Brothers 2004.
Chandraharan E, Arulkumaran S. Female pelvis and details of operative delivery; shoulder dystocia and episiotomy. In: Arulkumaran S, Penna LK, Rao B (eds) Management of labour. Orient Longman 2005.
Healy JC. Female reproductive system. In: Standring S (ed) Grays anatomy. Churchill Livingstone 2008.
Chronic pelvic pain Definition
Chronic pelvic pain (CPP) is usually defined as ‘constant or intermittent pain in the lower abdomen or pelvis of at least 6 months’ duration’. Women with dysmenorrhoea and/or dyspareunia only are therefore excluded, as are those with pain related to pregnancy or malignancy. The definition solely considers the location and duration of the symptoms; no assumptions are made about the cause.
An alternative definition is ‘non-cyclical pain of at least 6 months’ duration that appears in locations such as the pelvis, anterior abdominal wall, lower back, or buttocks, and that is serious enough to cause disability or lead to medical care’. Epidemiology
The lack of an unambiguous definition makes studying the epidemiology difficult. Until recently, studies focused on the frequency of finding pelvic pathology at laparoscopy as an explanation for CPP, and on attempts to explain the symptoms when no such pathology was found.
The best estimate of the annual prevalence in primary care, in women aged 18–50, is 37/1000: a figure similar to that for asthma and back pain. The prevalence varies with age: from 18/1000 in 15–20-year-olds to 28/1000 in women older than 60.
In a community survey, 24% of women reported having CPP in the last three months; excluding ovulation-related pain reduced the estimate to 17%.
Contributory factors to the genesis of CPP
CPP is difficult to diagnose and treat, due to the wide range of possible causes with overlapping symptoms:
• endometriosis
• pelvic inflammatory disease (PID)
• adhesions
• irritable bowel syndrome (IBS)
• interstitial cystitis (IC)
• urethral syndrome
• muscle and mechanical pelvic pain
• pelvic pain posture
• nerve entrapment
• neuropathic and referred pain
• pelvic congestion syndrome
• psychosocial factors
• psychogenic pain
• physical and sexual abuse. Risk factors
In a recent systematic review, drug or alcohol abuse, miscarriage, heavy menstrual flow, previous Caesarean section, PID, pelvic pathology, abuse, and psychological comorbidity were associated with an increased risk of noncyclical pelvic pain. Initial consultation
As pain is perceived in the mind, the experience of CPP will inevitably be affected by factors in the sufferer’s physical and psychological environment, e.g. coexisting illness, stress levels or beliefs about the pain.
Thus, in assessing patients with CPP, it is imperative to see the individual as a whole, and not to dichotomize pain as either organic or psychological. In addition, adequate time should be given at the initial assessment, ideally in a multidisciplinary setting. Women with CPP need to feel they have been able to tell their story and that they have been listened to and believed.
As there is frequently more than one component to CPP, assessment should aim to identify all contributory factors, rather than assign causality to a single pathology.
Many women want an explanation for the pain, especially if they already have their own theories or concerns about its origin. These should be discussed, as consultations that elicit the woman’s own ideas result in a better doctor-patient relationship and improved concordance with investigation and treatment. Initial history
This should include questions about the pain pattern and its association with other problems, e.g. psychological, bladder and bowel symptoms, as well as the effects of movement and posture on the pain.
‘Red flag’ symptoms (those suggestive of serious disease) should be excluded and managed as appropriate:
• rectal bleeding
• NEW bowel symptoms (>50 years old)
• irregular vaginal bleeding (>40 years old)
• post-coital bleeding
• pelvic mass
• new pain after the menopause
• suicidal ideation
• excessive weight loss.
• Completing a daily pain diary for two to three menstrual cycles may help the clinician and patient identify provoking factors or temporal associations. The information may be useful in understanding the cause of the pain. Women should also be screened for IBS with a symptom-based tool, e.g. the Rome II criteria:
• At least 12 weeks continuous or recurrent abdominal pain/discomfort associated with ≥2 of the following:
• pain relieved by defaecation
• a change in frequency of stool
• abnormal appearance or form of stool. Examination
The examination is most usefully undertaken when there is sufficient time to explore the woman’s fears and anxieties, at which point new information may be revealed.
• Features to note include:
• signs of pelvic pathology, e.g. rectovaginal nodule of deeply infiltrating endometriosis
• patient attitude, as detachment may indicate disgust with this part of her body
• evidence of altered sensation (allodynia or hypersensitivity) before abdominal palpation is performed
• effects of movement on pain if a musculoskeletal cause is suspected
• altered sensation on vulva or perineum
• pelvic floor muscle tone
• Vaginismus, in which case more than a gentle one FINGER examination may be inappropriate. Investigations
• The following should be considered:
• transvaginal ultrasound for an ovarian mass
• transvaginal ultrasound or MRI for adenomyosis
• if there is any suspicion of PID, appropriate samples should be taken although, ideally, all sexually active women less than 25 should be offered opportunistic screening for chlamydia.
Laparoscopy
Laparoscopy has been the ‘gold standard’ diagnostic test in CPP as it is the only way to diagnose adhesions and peritoneal endometriosis. Therefore, gynaecologists have seen it as an essential tool to assess women with CPP. However, there are problems associated with its use as a first line investigation.
• Risks of anaesthesia, bleeding and organ injury: 3.3/100 000 mortality and 4.6/1000 morbidity during diagnostic and therapeutic laparoscopy in a study of 30,000 patients. Complications needing laparotomy (approx. 25% of which were missed at the initial laparoscopy) occurred in 3.2/1000 patients.
• Laparoscopy cannot diagnose many potential causes of CPP, e.g. adenomyosis, IC and IBS.
• The presence of visible ‘pathology’ e.g. peritoneal endometriosis, may be coincidental and not the cause of the woman’s symptoms.
• 30–50% of diagnostic laparoscopies are negative, which disappoints many women as they assume their doctor now thinks ‘the problem is all in my head’.
Consequently, laparoscopy should only be performed where (a) the index of suspicion of endometriosis and/or adhesions requiring surgical intervention is high and (b) other causes have been excluded.
Microlaparoscopy or ‘conscious pain mapping’ may be an alternative to laparoscopy as it avoids general anaesthetic. Although it may seem to confirm particular lesions as the source of the pain, it has not been widely adopted and questions remain as to its acceptability, reproducibility and validity. Empirical treatment
It has been suggested that women with cyclical pain should undergo a therapeutic trial using the combined oral contraceptive or a GnRH agonist for 3–6 months before being offered a diagnostic laparoscopy.
The rationale is that ovarian suppression is an effective treatment for pain associated with endometriosis (and some other causes such as pelvic congestion syndrome).
Women should also be offered appropriate analgesia to control their pain; this includes
• regular NSAIDs with or without paracetamol
• compound analgesics including opioids
• tricyclic antidepressants e.g. amitriptyline
• anticonvulsants e.g. gabapentin
• non-pharmacological modalities such as TENS may help some patients. Condition-specific treatment
Some conditions require specific treatments, e.g. women with IBS should be offered a trial with antispasmodics as a systematic review has concluded that smooth muscle relaxants such as mebevrine are beneficial in treating IBS where abdominal pain is a prominent feature. They should also try to amend their diet. Treatment options for CPP
The options are summarized extremely well in a recent systematic review of the literature (Cheong and Stones 2006), which identified 13 relevant RCTs. These included interventions with medroxyprogesterone acetate (MPA) alone or in combination with psychotherapy, goserelin, sertraline, lofexidine hydrochloride, ultrasound scanning to aid counselling and reassurance, i.v. dihydroergotamine for acute exacerbations and the use of a Polaroid print to assist in postoperative patient consultation.
Other interventions identified were writing therapy to improve symptoms, static magnetic fields to improve pain, adhesiolysis via laparoscopy or laparotomy, and a multidisciplinary approach to investigation, including physiotherapy, psychology, and attention to dietary and environmental factors.
The best available evidence provides some support for the use of ultrasound scanning as an aid to counselling and reassurance; MPA or goserelin for pelvic congestion, and a multidisciplinary approach to assessment and treatment. Adhesiolysis provides no benefit other than in women with severe adhesions. Short-term results for presacral neurectomy (PSN) and laparoscopic uterosacral nerve ablation (LUNA) are similar, although PSN has better results in the long term. SSRI antidepressants have not been shown to be of benefit. References
American College of Obstetricians and Gynecologists (ACOG) Practice Bulletin No. 51. Chronic pelvic pain. Obstet Gynecol 2004;103:589–605.
Chapron C, Querleu D, Bruhat M, et al. Surgical complications of diagnostic and operative gynaecological laparoscopy. Hum Reprod 1998;13:867–72.
Cheong Y, Stones W. Chronic pelvic pain: aetiology and therapy. Best Pract Res Clin Obstet Gynaecol 2006;20:695–711.
Latthe P, Mignini L, Gray R, et al. Factors predisposing women to chronic pelvic pain: systematic review. BMJ 2006;332:749–55.
Moore J, Kennedy S. Causes of chronic pelvic pain. Baillieres Clin Obstet Gynaecol 2000;14:389–402.
Royal College of Obstetricians and Gynaecologists (RCOG) The initial management of chronic pelvic pain. Greentop Guideline. London: RCOG 2005.
Vincent K. Chronic pelvic pain in women. Postgrad Med J 2009;85:24–9.
Williams RE, Hartmann KE, Steege JF. Documenting the current definitions of chronic pelvic pain: implications for research. Obstet Gynecol 2004;103:686–91.
Zondervan KT, Yudkin PL, Vessey MP, et al. Chronic pelvic pain in the community: symptomatology, investigations and diagnoses. Am J Obstet Gynecol 2001;184:1149–55. Internet resources
The International Pelvic Pain Society aims to educate health care professionals on how to diagnosis and manage CPP: www.pelvicpain.org/
The American Chronic Pain Society aims to facilitate peer support and education for individuals with chronic pain and their families so that they may live more fully in spite of their pain: www.theacpa.org/
European Association of Urology guideline on management of CPP: www.uroweb.org/
Summary written for Patient UK: www.patient.co.uk/showdoc/40000111/ Contraception Definition
When conception or impregnation has been intentionally prevented by a sexually active individual through the use of various devices, agents, drugs, sexual practices and or surgical procedures it is referred to as contraception. Epidemiology
Contraception has been practiced from time immemorial. The main objective of contraceptive provision is to permit sexually active individuals to enjoy positive aspects of their sexuality without it affecting their mental or physical health adversely.
It is estimated that about 4 million people utilize the National Health Service contraceptive services in the United Kingdom each year. Three-quarters see a general practitioner and the rest attend specialist community contraceptive ser-vices. Pathology
Contraceptive methods may be either temporary or permanent.
Temporary methods
User dependent
• Barrier
• Oral contraceptives (combined as well as progestogen-only preparations)
• Patches (containing oestrogen and progestogen)
• Spermicides either used alone or in combination with barrier method
• Fertility awareness methods.
User independent (long-acting reversible contraception) methods
• Intrauterine devices
• Implants (progestogen only)
• Vaginal rings (oestrogen and progestogen containing)
• Progestogen only injectables.
Permanent methods
• Female sterilization methods
• Male sterilization methods.
Factors influencing choice of method
• Peer opinion
• Lifestyle
• Duration of action
• Medical complications
• Return to fertility
• Side-effects
• Safety
• Efficacy.
Barriers preventing choice of contraception
• Myths
• ‘I can’t be at risk’ attitude
• Religious and cultural misconceptions. Safety
Contraceptive benefits to health
Contraception helps women have a planned pregnancy and thus avoid the emotional stress involved with an unplanned one.
Worldwide, 200 million unintended pregnancies occur each year to women not using an effective method of contraception. More than half of these end in abortion, half of which may be performed in an unsafe or unhygienic way. A strong correlation has been noted between unmet need for contraception, unintended pregnancy, and unsafe abortion. Increasing access to contraception would lower the incidence of unintended pregnancy, which then leads to decreased risk to the woman of lifelong injury or death.
The risk of ectopic pregnancy is also decreased with the use of contraception. Use of a contraceptive is known to decrease ectopics by an estimated 30–280 per 100 000 annually in monogamous relationships and by 680–920 per 100 000 non-monogamous relationships. Non-contraceptive benefits of contraception
Hormonal methods Combined oral contraceptives
• Lighter, regular, and less painful periods
• Decreased risk of benign breast disease
• Decreased ovarian cysts
• Decrease in both ovarian and endometrial cancer
• Decrease in acne.
Hormone releasing intrauterine devices(intrauterine systems)
• Decrease in menstrual blood flow
• Induce endometrial atrophy
• Some evidence that the pain of endometriosis is decreased.
Non-hormonal Barrier contraception
• Prevents sexually transmitted infections.
Risks
Barrier methods
• High failure rate
• Latex allergy
• High incidence of urinary tract infections with use of diaphragm
Oral contraceptives
• Bleeding irregularities in 20–30% of users.
• Mood changes, headaches, nausea, breast tenderness, or changes in libido.
• Risks of myocardial infarction in smokers increased with combined oral pill usage. Risk of death through cardiac causes increased fourfold if a smoker over 35 and using combined oral contraceptives.
• Venous thrombosis risk is raised. Risk in combined pill takers of non-fatal pulmonary embolism is 10–30/100 000 compared with 5/100 000 for non-pill users. However, in pregnancy the risk is 60/100 000. Aetiology
Mechanism of action
• Most hormonal contraceptives such as combined oral pills, patch, vaginal ring, implant, and injectables work by inhibiting ovulation.
• Progestogen-only preparations such as the mini pill, implants, injectables, and intrauterine systems thicken the cervical mucus, preventing entry of sperm through the cervical mucus plug barrier in addition to any other mechanism attributed to them.
• Intrauterine devices (IUDs) including hormone-releasing ones render implantation in uterine endometrium impossible by creating an inflammatory reaction locally. The copper in a copper IUD is spermicidal and toxic to the ovum.
• Barrier contraceptives prevent ascent of sperm into the uterine cavity.
• Fertility awareness methods are where the woman predicts the fertile time in her cycle by interpreting symptoms and signs in her body and avoids sexual intercourse during that period. Efficacy
The efficacy of contraceptive methods is usually quantitated by the pearl index, which is defined as the number of unintended pregnancies per 100 women per year.
The most effective methods are those that are not user dependent such as the permanent methods and the long-acting reversible contraceptives (LARCs). Their perfect use (theoretical efficacy) figures closely match typical use (actual efficacy), unlike user-dependent methods, where there is a wide discrepancy (Table 12.4.1). Prevalence by method
In the UK according to the Office of National statistics (ONS) the pill, including the mini pill, continue to be the most popular method with 27% of 16–49 year olds choosing it. The male condom was the next popular at 22%. LARCs were used by just 8% and sterilization, including male and female methods, by 20%.
In the USA, 62% use some form of contraception. The figures for 2002 showed the most frequently used were the oral contraceptives (30.6%), male condoms (18%), female sterilization (27%), male sterilization (9.2%), and injectables (5.3%) accounting in total for 90% of use.
The National Institute for Clinical Guidelines (2005) have calculated that all LARCs are more cost-effective at 12 months of use than oral contraception, as pregnancy rates are lower with much fewer visits to the clinician. Contraindications for contraception
Oestrogen-containing methods
• Past or current history of thrombosis
• Focal migraine
• Active disease of the liver
• Undiagnosed vaginal bleeding
• Oestrogen-dependent tumours
• Smokers over the age of 35
• Body mass index of ≥35.
Table 12.4.1 Percentage of unintended pregnancies per 100 women per year in the first year of use of contraceptive

Progestogen-only methods
• Bleeding abnormalities
• Hepatic adenoma or chronic liver condition such as porphyria
• Current cardiovascular disease
• Current breast cancer.
Intrauterine devices
• Undiagnosed vaginal bleeding
• Active pelvic infection
• Uterine abnormalities.
Fertility regulation procedures
• Menstrual abnormalities
• Chronic or active pelvic infection
• Immediately following childbirth, terminations, miscarriages or gynaecological surgery
• Those on medications
• Those with medical conditions such as hypothyroidism. Sterilization procedure
Couples need to be absolutely certain of their decision: 10% are known to regret their decision and 1% seek reversal. Reasons for regret are
• marital/relationship problems
• young age
• when done as postpartum or postabortal procedures
• psychiatric illness in either partner. Return to fertility
This is an important advantage of reversible methods. Except for injectables, where the return takes an average of 9 months, for all other methods 70–90% attempting to conceive do so within 12 months. Research
Contraceptive vaccines are under investigation and none are clinically available. They aim to target gamete production, gamete function, or gamete outcome.
Male hormonal contraception is not currently available. It is however undergoing clinical trial. It involves injecting a hormone every 2 months to turn off sperm production. However, as this could lower testosterone production this requires a testosterone implant injection every 4 months. Summary
Unintended pregnancy could carry significant health risks and the use of contraception helps avert it. Responsible societies aim towards ensuring all pregnancies are planned. Contraceptive measures should therefore be encouraged as an effective public measure. Further reading
Faculty of Sexual and Reproductive Healthcare Clinical Effectiveness Unit. Intrauterine methods of contraception. London: FSRH CEU 2007.
Faculty of Sexual and Reproductive Healthcare Clinical Effectiveness Unit. UK Medical eligibility criteria for contraceptive use. London: FSRH CEU 2009.
Harlap S, Kost K, Forrest JD. Preventing pregnancy, protecting health: a new look at birth control choices in the United States. New York: Alan Guttmacher Institute 1991.
Mesca D, Sines E. Unsafe abortion: facts and figures, 2006. Washington DC: Population Reference Bureau 2006.
Mosher WD, Martinez GM, Chandra α, et al. Use of contraception and use of family planning services in the United States: 1982–2002. Adv Data. 2004;350:1–36.
National Institute for Health and Clinical Excellence (NICE). Long-acting reversible contraception: the effective and appropriate use of long-acting reversible contraception. London: NICE 2005.
The National Health Service information centre KT31 return. Internet resources
http://www.emedicine.com Patient resources
www.fsrh.org
www.fpa.org.uk
Disorders of sex development Definition
Disorders of sex development (DSD) occur when the development of chromosomal, gonadal, or anatomical sex is atypical. Previous terminology used to describe this group of conditions included intersex, pseudohermaphroditism, and testicular feminization. These terms are inaccurate and misleading for clinicians and are perceived by patients as pejorative. The recent consensus statement on the management of intersex disorders recommended the adoption of the term DSD (Hughes et al. 2006). This terminology described by the consensus group encompasses a wide range of conditions and has been quickly adopted by the majority of units around the world managing this group of patients. The incidence of DSD is estimated to be in the region of 1 in 4500 births. Congenital adrenal hyperplasia
Congenital adrenal hyperplasia (CAH) is an autosomal recessive condition occurring in approximately 1 in 13 000 births. It results from a deficiency of an enzyme for the production of cortisol. Over 90% of cases are caused by 21-hydroxylase deficiency, leading to an excess of testosterone precursors. Affected individuals will have an androgen excess, which leads to virilization in the 46,XX female fetus. This results in clitoromegaly, labial fusion, and rugosity, with a urogenital sinus and most commonly presents with ambiguous genitalia at birth. The upper vagina, uterus, fallopian tubes, and ovaries are normally formed. Management includes steroid replacement therapy and surgical treatment to the genital area. The nature and timing of genital surgery is controversial. Virilization may persist or recur in those who are inadequately treated, and individuals require lifelong steroid replacement therapy. Both under- and overtreatment may result in short stature, and girls may have oligomenorrhoea or amenorrhoea, leading to fertility difficulties. Androgen insensitivity syndrome
Androgen insensitivity syndrome (AIS) occurs as a result of a defect in the gene coding for the androgen receptor, leading to insensitivity to circulating androgens. The condition is X-linked in two-thirds of cases, with an incidence of 1 in 40 000 births. Those with complete androgen insensitivity syndrome (CAIS) will have a 46,XY karyotype, with phenotypical female external genitalia. The vagina is blind ending and of variable length. The internal gonads are normal testes. Complete regression of the Müllerian ducts occurs and therefore no uterus is present. Partial AIS results in a variable degree of virilization, with appearances ranging from ambiguous genitalia to simple hypospadias. Management includes the creation of a vagina to facilitate penetrative intercourse and the option of elective gonadectomy with subsequent hormone replacement therapy. Disorders of testosterone biosynthesis
Rarer DSDs include those resulting from a deficiency in any enzyme required in the biosynthesis or metabolism of testosterone.
5-α-reductase converts testosterone to the more active metabolite dihydrotestosterone (DHT). Deficiency leads to the development of an undervirilized male (46,XY). The condition is autosomal recessive and individuals have normal testes. The external genitalia may be ambiguous or phenotypically female. The majority of individuals are reared as female, although subsequent virilization may occur at puberty if the gonads have not been removed. Fertility has been reported in those reared male, but is significantly reduced.
17 β-hydroxysteroid dehydrogenase deficiency occurs when there is an absence or reduction of the enzyme converting androstenedione to testosterone. This condition is autosomal recessive, and results in a 46,XY individual with ambiguous or phenotypically female genitalia. Virilization may occur at puberty. Turner syndrome
Turner syndrome results in gonadal dysgenesis due to the absence or anomaly of one of the X chromosomes. This includes those with 45,X, those with duplication of the long arm of the X chromosome, and those with mosaicism with one or more additional cell lineages. The incidence is approximately 1 in 3000 female births. Individuals have normal internal Müllerian structures with streak gonads and normal external female genitalia. Possible phenotypes include short stature, webbed neck, broad shield-shaped chest and drooping eyelids, although none of these features may be present. Additionally, heart defects, hypertension, obesity, diabetes, renal anomalies, Hashimoto’s thyroiditis, cataracts, arthritis, and scoliosis have been associated with the condition. Primordial follicles are initially present in the streak gonads, but these appear to undergo premature apoptosis and are usually absent by adult life. The vast majority of women with Turner syndrome will require induction of puberty and long-term hormone replacement therapy. Spontaneous fertility has been reported, but is rare. Owing to the presence of a normal uterus, fertility may be possible with assisted conception techniques. Swyer’s syndrome
Swyer’s syndrome, also known as pure gonadal dysgenesis, occurs as a result of bilateral dysgenetic testes. Individuals have normal 46,XY chromosomes. As the testes do not function, no testosterone is produced and hence no virilization occurs. In addition, normal internal Mullerian structures develop due to the lack of Mullerian inhibiting substance (MIS). Women are often taller than may have been expected, and this has been attributed to the presence of a Y chromosome. There is a failure of spontaneous puberty, with hormone replacement therapy being required. Fertility is possible with egg donation and assisted conception techniques. Ovotesticular DSD
This condition was previously known as true hermaphroditism and refers to the presence of both ovarian and testicular tissue in the same individual. The karyotype is 46,XX in over 70% of cases and the gonads may be a separate ovary and/or testes and/or an ovotestis. The external genital appearance may be ambiguous, with Müllerian and Wolffian structures present internally. Asymmetry of gonads and subsequent reproductive tracts and external genitalia may occur. Fertility may be possible depending upon karyotype and phenotype. Rokitansky syndrome
Also known as Mayer–Rokitansky–Kuster–Hauser (MRKH), this condition occurs in approximately 1 in 5000 births, and consists of the congenital absence of the uterus and upper vagina. Isolated fallopian tubes may persist with normal ovaries. The karyotype is 46,XX, with normal female external genital appearance. The vagina is blind ending and may be of variable length. As the ovaries are unaffected, puberty proceeds normally, with the development of normal secondary sexual characteristics. Individuals usually present with primary amenorrhoea, and may have no other signs or symptoms. There is an association with renal, skeletal, auditory, and cardiac anomalies. There appears to be a genetic component to the condition, but the aetiology remains elusive. Fertility is possible via in vitro fertilization (IVF) and a surrogate mother. Management consists of psychological support and the option of creating a vagina to enable penetrative intercourse. Presentation of DSDs
Conditions which include ambiguous genitalia will be apparent from birth. However, those with normal external genitalia may not present until later childhood or puberty with a herniated inguinal gonad, primary amenorrhoea or progressive virilization.
Features in a neonate that would warrant further assessment include bilateral undescended testes in an apparently full-term male child, hypospadias associated with separation of the scrotal sac, or an undescended testis, ambiguous genitalia, clitoral hypertrophy, single opening urogenital sinus, or an inguinal hernia containing a gonad.
Diagnosis
CAH is the most common cause of neonatal ambiguous genitalia. Chromosomal analysis, with specific fluorescent in situ hybridization for a Y fragment should be performed. Serum biochemical tests can identify a block in testosterone biosynthesis. A human chorionic gonadotrophin stimulation test may be necessary to assess response. Anti-Müllerian hormone and inhibin B are also playing an increasing role in determining the presence of testicular tissue. Ultrasound scans may be of value, but the neonatal Müllerian structures can be difficult to image clearly. A laparoscopy may be performed to inspect and biopsy the gonads. Medical management
DSDs are complex and rare conditions. It is essential that such conditions are managed within a multidisciplinary setting comprising paediatric endocrinology, urology, gynaecology, and psychology teams. Previously a policy of non-disclosure of diagnosis to patients was widespread. Patients were denied information about their condition and so the opportunity to access support groups and the option for genetic testing for unaffected relatives. This further reinforced the secrecy and shame felt by many patients. This policy is no longer practised and clinicians should disclose all information to patients as it becomes age appropriate, with concomitant psychological input. Many conditions now have peer-led support groups.
Sex of rearing
When an infant presents with ambiguous genitalia a decision as to appropriate sex of rearing is made, based upon a number of considerations: the potential for fertility, along with the likelihood of successful sexual functioning in adulthood, the outcomes of proposed surgery and the wishes of the parents. Surgical management
For those born without a vagina and being reared female, the option of creating a vagina is considered. This is necessary for those with a uterus to allow menstrual flow, and should be achieved before puberty. However, in the absence of a uterus, these procedures can be deferred until adolescence or later, depending on the wishes of the individual. Dilation therapy should always be considered as first-line treatment. A series of plastic cones are pressed against the vaginal dimple, to stretch the skin. Over 3–6 months, a vagina suitable for penetrative intercourse can be created. Dilation has success rates of 85% and avoids the risk of surgery. For those where dilation does not work, the laparoscopic Vecchietti procedure may be performed, where an acrylic olive is positioned in the vaginal dimple and winched up over 7 days, creating a vagina through the pressure effect. Other vaginoplasty techniques include the use of skin or bowel grafts to create a tissue tube, which is then fixed to the introitus. Both carry a risk of contracture and long-term carcinoma development. Bowel vaginoplasties are associated with the excessive production of mucus, and risk the development of diversion colitis.
Clitoral surgery is offered for cosmetic reasons and is often performed at the time of vaginal surgery. However, this damages function and increasingly is avoided for those with mild to moderate clitoromegaly. Surgery is irreversible and infants are unable to give consent. Deferring a decision for surgery until the child can be involved may be appropriate, with the option of surgery at a later date.
Gonadectomy
Dysgenetic gonads carry a 30% risk of malignant change, and gonadectomy is recommended at the time of diagnosis. This includes conditions where a Y fragment is present. For conditions with normal but intra-abdominal testes, such as CAIS, the malignancy risk is much lower in the order of 2–3%. Puberty is more successful with endogenous hormones and current practice is therefore elective gonadectomy after completion of puberty. Individuals may choose to retain their gonads longer than this but screening for potential malignancies is inaccurate. Further reading
Balen AH, Creighton SM, Davies, et al. Paediatric and adolescent gynaecology, 1st edn. Cambridge: Cambridge University Press 2004.
Hughes IA, Houk C Ahmed SF, Lee PA. Consensus statement on management of intersex disorders. Arch Dis Child 2006;91:554–63. Internet resources
Androgen Insensitivity Syndrome: www.aissg.org
Climb CAH Support Group: www.livingwithcah.org Donor insemination
Male factor infertility is diagnosed in a third of couples presenting to fertility clinics. Donor insemination (DI) was the only treatment available to couples where there were severe abnormalities in semen until the introduction of intracytoplasmic sperm injection (ICSI) in the mid-1990s. As long as a few viable sperm can be retrieved for ICSI, the couple are able to have a genetically related child, with IVF pregnancy rates well above donor insemination cycles. As a result, there has been a marked decline in donor insemination treatment. The number of cycles undertaken in the UK fell from 15 000 in 1996 to 4153 in 2006. Availability and regulation of treatment varies between countries; for example, donor anonymity is protected in Spain, gamete donation is prohibited in Italy, and donor payment is the norm in the USA. In 2005 the UK lifted anonymity from donors, enabling potential offspring to identify their biological father. This resulted in a significant fall in the number of volunteers willing to donate sperm; the supply of UK-sourced donor sperm is scarce and the number of donor cycles has fallen further. Indications
• In current practice, DI is usually reserved for severe male factor infertility where sperm cannot be obtained by masturbation or surgically. Absence of spermatogenesis may be congenital (e.g. Klinefelter’s syndrome) or acquired (e.g. cancer treatment). Some couples may choose DI as being less invasive and expensive than ICSI.
• Gamete donation may be used by couples who are carriers of serious inherited disease.
• Women without a male partner may be treated with DI: about a third of treatment cycles in the UK are for single women and lesbian couples. Recruitment of donors
Guidelines for recruitment of donors and the use of donated gametes are available; in the UK there are national regulations issued by the Human Fertilisation and Embryology Authority.
Donors should be aged 18–45, in good health, and carefully screened. They must be offered independent counselling to explore the implications of donation. The great majority of donors are anonymous to the recipient (although they may be identified to their offspring). A small minority of couples have known donors. Donations are altruistic with financial compensation only for time and travel. Only 10 pregnancies are permitted per donor. As a result of these restrictions many fertility clinics in the UK have found it difficult to recruit and are importing donated sperm from overseas. Recruitment is supported by the National Gamete Donation Trust. Screening of donors
Semen is a natural vector for a range of infectious diseases and also a potential source of inherited disorders. To minimize risk to the woman receiving the donor sperm and to potential offspring, every effort is made to screen donors for these conditions. All men donating sperm should be in good health and the initial evaluation should include a full history and clinical examination, paying attention to the presence of any genital lesions (genital warts, urethral discharge, or ulcers) which would indicate sexually transmissible infection.
Donors are screened for HIV 1 and 2, hepatitis B and C, cytomegalovirus, syphilis, gonorrhoea, and chlamydia.
Genetic screening comprises a family history, karyotype, and testing for carriage of cystic fibrosis in European donors and haemoglobinopathies in other ethnic groups. Blood group and Rhesus group are usually recorded.
To allow for the incubation period of transmissible viral infections, donated semen samples are frozen and quarantined for at least 6 months and the donor is retested before samples are released for use. Storage of semen
Semen is cryopreserved for storage and this reduces the sperm count and motility. The main hazard to survival of sperm is intracellular ice crystal formation during freezing; the sperm are dehydrated by exposure to serially increasing concentrations of cryoprotectants to minimize osmotic shock. The resultant frozen vial or straw containing sperm and cryoprotectant is sealed and stored in nitrogen vapour in order to minimize cross-contamination with other samples in the storage tank, which is regularly topped up with liquid nitrogen. Ideally, ejaculates should contain at least 40 million sperm per millilitre to ensure adequate sperm counts after thawing. However, many clinics will now accept donors who are unable to provide such quality samples. Intrauterine insemination of prepared sperm can compensate for this.
Couples may request that samples be saved for subsequent treatment to enable them to have more than one child with the same donor. Under UK regulations, samples can be stored for 10 years. Clinical aspects of donor insemination
Assessment of the female partner
• Full history and examination to identify any potential medical or gynaecological problems.
• Confirmation of ovulatory cycles (menstrual history, mid-luteal progesterone) and assessment of ovarian reserve (early follicular phase hormone profile, antral follicle count).
• Pelvic ultrasound scan to establish normal pelvic anatomy, preferably in the early follicular phase to determine the number of antral follicles.
• Tubal patency testing is usually performed by hysterosalpingogram.
• Screening for HIV 1 and 2, hepatitis B and C, and cytomegalovirus, and swabs to exclude genital infection including chlamydia.
• Pre-pregnancy assessment: discuss any relevant medical history, review medication, confirm rubella immunity, and ensure recent negative cervical cytology.
• Folic acid supplementation is recommended. Smoking, alcohol, diet, and exercise are discussed. Weight reduction is strongly advised for women with a BMI above 30 because of the implications for success rates and pregnancy outcome.
Counselling
Couples should see an independent counsellor to explore the implications of treatment, discuss any concerns about raising a child genetically unrelated to the male partner, and consider disclosure to the child of his or her origin.
Matching the donor
Donors are matched to the male partner so that any potential child will share as many characteristics as possible with the father. Matching will include:
• ethnicity
• hair and eye colour
• height and build
• blood group.
However, with the limited supply of donor sperm, these matching criteria may be relaxed to an extent.
The CMV status of the female partner is taken into account: CMV negative, i.e. non-immune, patients should be treated with CMV-negative donor sperm because of the small risk of congenital CMV infection. Management of treatment cycles
Intrauterine insemination is the preferred method of delivery of donor semen as this gives better pregnancy rates than intracervical insemination of frozen-thawed semen
In women who have normal investigations, the initial cycles should be unstimulated as these women are fertile and have a significant risk of multiple pregnancy with ovarian stimulation.
However, if there is no pregnancy after three unstimulated cycles or there are any mild female factors, such as mild endometriosis, then mild ovarian stimulation with either Clomiphene or gonadotrophins may be undertaken with the aim of producing not more than three follicles in each cycle. In anovulatory women, ovulation induction is used in a similar way but the aim here is to produce a single follicle in each cycle.
If there are significant problems identified, such as tubal blockage, then IVF can be performed with donor sperm. The law and regulation in the UK
In the UK, fertility treatment is regulated by the Human Fertilisation and Embryology Authority (HFEA), set up by an act of parliament, which issues a ‘Code of Practice’ and inspects and licenses clinics. The HFEA maintains a register of all gamete donors and records all donor treatment cycles carried out in UK clinics. Welfare of the child
All couples considering fertility treatment are required to complete a ‘Welfare of the Child’ assessment in order to identify any potential risks to the unborn child or existing children in the family. It is very unusual for a clinic to withhold treatment. Confidentiality
Gamete donation is a personal decision and treatment is kept private by many couples. In UK clinics the patient’s consent is required for disclosure even to other medical practitioners. The donor is also protected by confidentiality and only non-identifying information can be revealed to the recipient. Rights of the parents, donor, and child
The couple receiving treatment are the child’s legal parents and their names are on the child’s birth certificate. Married couples automatically have legal rights and duties towards the child called ‘parental responsibility’. Unmarried couples are advised to take legal advice to ensure that the male partner has parental responsibility. A child born to a single woman following donor insemination will have no legal father.
The donor has no legal rights or responsibilities towards the child. Conversely, the child has no claim on the donor. However, if donation has not taken place through a licensed clinic the legal position is less clear.
Children born from donor insemination have the right to obtain details of the identity of the donor from the UK national register once they reach adulthood (18 years). They may also apply to the register if they are planning to marry, to check that their partner is not genetically related (though this risk is very small because of the restricted number of donor pregnancies). Voluntary registers exist to help children born before this provision came into force. Success rates
Live birth rates for donor insemination average 11% per cycle. This is lower than IVF but insemination is a simple treatment which can be repeated, and up to 50% of couples will conceive in 6 months. Data from the HFEA show a clear trend of reducing success rates with advancing maternal age, with a live birth rate of 13.5% for women under 30 falling to 5.3% at age 40–42. Further reading
Byrd W, Bradshaw K. Carr B, et al. A prospective randomised study of pregnancy rates following intrauterine and intracervical insemination using frozen donor sperm. Fertil Steril 1990;53:521–7.
Hamilton MP. Working Party on Sperm Donation Services in the UK. Human Fertility 2008;11:147–58.
Human Fertilisation and Embryology Authority. Code of Practice. 2007.
Human Fertilisation and Embryology Authority. Disclosure of Donor Information Regulations (2004) Statutory Instrument 2004 No 1511. HMSO.
National Collaborating Centre for Women’s and Children’s Health on behalf of the National Institute of Clinical Excellence. (2004) Fertility: assessment and treatment for people with fertility problems. London: RCOG Press 104–6.
Practice Committee of the American Society for Reproductive Medicine and the Practice Committee of the Society for Assisted Reproductive Technology. Guidelines for Gamete and Embryo Donation. Fertility Sterility 2006; 86: S38–50.
Tomlinson M, Barratt C. Donor insemination. In: Serhal and Overton (eds) Good clinical practice in assisted reproduction. Cambridge 2004: 86–99. Internet resources
www.hfea.gov.uk
www.ngdt.co.uk/
www.bica.net/ Patient resources
HFEA Guide to Infertility. Human Fertilisation and Embryology Authority, London 2008 (also available online)
www.infertilitynetworkuk.com/
www.dcnetwork.org/
www.ukdonorlink.org.uk/ Heavy menstrual bleeding Definition
Heavy menstrual bleeding (HMB) is excessive menstrual bleeding that diminishes the woman’s physical, emotional, social, and material quality of life and which can occur alone or in combination with other symptoms (NCCWCH 2007). It is frequently termed dysfunctional uterine bleeding, which is abnormal bleeding from the uterus in the absence of any identifiable pathology or pregnancy. It can also be termed menorrhagia, but these terms should be avoided where possible since they mean different things to different people. Epidemiology
Between 4% and 51% of women experience HMB depending on the country and clinical setting of origin. In the UK, 5% of all women present with this problem. The incidence increases with both age and parity (Rybo 1966). Pathology
HMB may be associated with the presence of fibroids, adenomyosis, endometriosis, and possibly endometrial polyps, although in many instances, no pathological features are present. HMB may be the result of either ovulatory or anovulatory cycles. Aetiology
Disorders of endometrial function have been reported particularly related to the vasculature (Jabour et al. 2006). In particular, disordered production and metabolism of the prostaglandins has been well documented, as well as of a number of growth factors. Frequently ovarian function is normal in these women. HMB may occur in women with thyroid dysfunction and bleeding disorders, although this is unusual. Prognosis
Heavy bleeding increases with age and is greatest during the 30s. In addition, the number of anovulatory cycles reported increases as the menopause approaches making irregular bleeding commoner. Dysfunctional uterine bleeding is cured by the menopause. Clinical approach
Diagnosis
History
A full menstrual history should be taken, including length of bleeding, length of the cycle, the number of days of heavy bleeding, and the impact on the woman, such as flooding or the inability to get out of the house as well as the presence of other menstrual symptoms.
The presence of ‘red light’ symptoms must be excluded as these may indicate the presence of significant pathology. These symptoms are
• intermenstrual bleeding
• post-coital bleeding
• pelvic pain not related to the menses
• pressure symptoms.
Examination
The principal reason to carry out an abdominal examination in this context is to identify a pelvic mass.
Pelvic examination is required before a
• levonorgestrel-secreting interuterine system (LNG-IUS) fitting
• investigation for structural abnormality
• investigation for histological abnormality.
Pharmaceutical treatment can be started without examination in those where pathology is unlikely, i.e. regular heavy periods with no ‘red light’ symptoms
Investigations
These aim to detect whether pathology is causing the symptoms and, if present, whether the pathology is correctable (Critchley et al. 2001).
Ultrasound is the first-line diagnostic tool for identifying structural abnormalities.
It should be carried out in the following circumstances:
• the uterus is palpable abdominally
• vaginal examination reveals a pelvic mass
• pharmaceutical treatment fails.
However, hysteroscopy may be required if ultrasound is unsatisfactory or if an abnormality impacting on the cavity of the uterus is considered likely.
Endometrial biopsy
The incidence of endometrial cancer in women under 45 is extremely low. Biopsy is indicated
• when there is intermenstrual bleeding
• if the woman is aged over 45
• if there has been treatment failure
• if the woman is at high risk for endometrial cancer. Treatment
Medical treatment
These are useful where there is no significant structural abnormality or where small fibroids only are present (Fraser et al. 1991; Lethaby et al. 2004, 2005). The main issues for consideration are
• whether contraception is required
• whether dysmenorrhoea is present
• woman’s preference.
Where contraception is required, the following treatments are appropriate:
• LNG-IUS
• tranexamic acid
• non-steroidal anti-inflammatory agents or combined oral contraceptive pill
• Norethisterone 15 mg per day for days 5–26 of the cycle, or injected progestagens
Side-effects are unusual although women should be counselled about the prolonged nature of irregular bleeding when using the LNG-IUS.
Surgical treatment
Endometrial ablation
Endometrial ablation may be achieved by resecting the endometrium using a hysteroscope under direct vision or destroying the endometrium using a number of modalities (microwave, heat, radiofrequency). These latter methods (second generation techniques) do not require visualisation of the cavity and therefore less skill is required.
Ablation techniques (Cooper et al. 2005; Lethaby et al. 2005):
• are useful in women with a normal uterine cavity or very small fibroids.
• can be offered as an initial treatment for HMB if appropriate
• are NOT contraceptive and women must be advised to avoid subsequent pregnancy and to use contraception. Pregnancy, when it occurs, usually has a poor outcome.
Hysterectomy
The numbers performed for benign conditions have dropped significantly over the last ten years but it is still an appropriate option for some women, provided they are aware of all new possible alternatives (Garry et al. 2004; Maresh et al. 2002).
It should be used when:
• Other treatment options have failed, are contra-indicated or are declined.
• There is a wish for amenorrhoea
• The fully informed woman requests it and no longer wishes to retain her uterus and fertility.
The route by which hysterectomy will be performed will depend on a number of factors including the size of the uterus, its mobility and the preference of both the patient and the surgeon. Vaginal hysterectomy is to be preferred over abdominal where possible. Subtotal and total hysterectomy are both possibilities and whether the ovaries will be removed or retained also needs to be discussed.
Women who have uterine fibroids need to be counselled about the increased risk of complications over those with no fibroids.
Healthy ovaries should not be removed unless a woman specifically requests this. HRT administration should then be discussed.
Pain may start before the bleeding but usually gets better as the period progresses. It may be associated with other symptoms such as back ache, gastrointestinal symptoms or other menstrual symptoms. Further reading
Cooper KG, Bain C, Lawrie L, et al. A randomised comparison of microwave endometrial ablation with transcervical resection of the endometrium; follow up at a minimum of five years. Br J Obstet Gynaecol 2005;112:470–5.
Critchley HO, Warner P, Lee AJ, et al. Evaluation of abnormal uterine bleeding: comparison of three outpatient procedures within cohorts defined by age and menopausal status. Health Technol Assess 2001; 8: iii–iv, 1–139.
Fraser IS, McCarron G. Randomized trial of 2 hormonal and 2 prostaglandin-inhibiting agents in women with a complaint of menorrhagia. Aust NZ J Obstet Gynaecol 1991;31:66–70.
Garry R, Fountain J, Mason S, et al. The eVALuate study: two parallel randomised trials, one comparing laparoscopic with abdominal hysterectomy, the other comparing laparoscopic with vaginal hysterectomy. BMJ 2004;328:129–33. [erratum appears in BMJ 2004;328:494.
Hurskainen R, Teperi J, Rissanen P, et al. Clinical outcomes and costs with the levonorgestrel-releasing intrauterine system or hysterectomy for treatment of menorrhagia: randomized trial 5-year follow-up. JAMA 2004;291:1456–63.
Jabour HN, Kelly RW, Fraser HM, Critchly HOD. 2006. Endocrine regulation of menstruation. Endocrine Rev 27: 17–46.
Lethaby A, Augood C, Duckitt K. Nonsteroidal anti-inflammatory drugs for heavy menstrual bleeding. Cochrane Database Syst Rev 2004; 3: CD000400.
Lethaby A, Farquhar C, Cooke I. Antifibrinolytics for heavy menstrual bleeding. Cochrane Database Syst Rev 2004; 4 CD000249.
Lethaby A, Hickey M. Endometrial destruction techniques for heavy menstrual bleeding. Cochrane Database Syst Rev 2005; CD001501.
Lethaby A, Irvine G, Cameron I. Cyclical progestogens for heavy menstrual bleeding. Cochrane Database Syst Rev 2004; 4: CD001016.
Lethaby A, Shepperd S, Cooke I, Farquhar C. Endometrial resection and ablation versus hysterectomy for heavy menstrual bleeding. Cochrane Database Syst Rev 2004; 2: CD003855.
Lethaby AE, Cooke I, Rees M. Progesterone/progestogen releasing intrauterine systems for heavy menstrual bleeding. Cochrane Database Syst Rev 2005; 4.
Maresh MJ, Metcalfe MA, McPherson K, et al. The VALUE national hysterectomy study: description of the patients and their surgery. Br J Obstet Gynaecol 2002;109:302–12.
Marjoribanks J, Lethaby A, Farquhar C. Surgery versus medical therapy for heavy menstrual bleeding. (Cochrane Review). In: Cochrane Database of Systematic Reviews, Issue 2, 2006. Oxford: Update Software.
National Collaborating centre for Women’s and Children’s Health (NCCWCH). Heavy menstrual bleeding. Clinical Guideline. 2007: 20–30.
Rybo G. Menstrual blood loss in relation to parity and menstrual pattern. Acta Obstet Gynecol Scand 1966;45 (Suppl 7): 25–45. Internet resources
National Institute for Clinical Excellence. Fluid-filled thermal balloon and microwave endometrial ablation techniques for heavy menstrual bleeding. Technology Appraisal 78. London: NICE 2004 1–25: www.nice.org.uk
National Institute for Clinical Excellence. Impedance-controlled bipolar radiofrequency ablation for menorrhagia. London: NICE 2004: www.nice.org.uk
National Institute for Health and Clinical Excellence. Endometrial cryotherapy for menorrhagia. London: NICE 2006: www.nice.org.uk
Full Heavy menstrual Bleeding Guideline: http://nice.org.uk/CG044fullguideline Dysmenorrhoea Definition
Dysmenorrhoea is painful menstruation. Epidemiology
Primary dysmenorrhoea is found particularly in teenage girls and usually starts 1 or 2 years after the menarche. It is frequently relieved following pregnancy and labour. Secondary dysmenorrhoea occurs in older women in association with pathology as described below. It may also occur in women taking hormone replacement therapy (Andersch and Milsom 1982). Pathology
Dysmenorrhoea is often associated with endometriosis and may be the principal symptom associated with chronic pelvic pain. Other common causes are uterine fibroids or adenomyosis. In young women with dysmenorrhoea, pathology is unlikely although endometriosis does occur. Aetiology
Primary dysmenorrhoea is related to the presence of prostaglandins. The concentration within the endometrium and myometrium is increased, particularly of those that lead to vascoconstriction and increased uterine contractility. Uterine prostaglandin production may also be increased in adenomyosis and where fibroids are present (Lumsden et al. 1984).
The posterior pituitary peptides, vasopressin and oxytocin, have also been implicated in the aetiology (Akerlund et al. 1979; Stromberg et al. 1984). It is unclear if there is an interaction between the two pathways. Prognosis
The prognosis for primary dysmenorrhoea is good. It is very responsive to treatment and improves with age. The prognosis for secondary dysmenorrhoea depends on the cause. History
• Identify relationship with menstrual bleeding:
• the pain may precede the bleeding but is usually worse during the first 2 days of the menses.
• Quality of pain:
• it is a cramping pain.
• Age of onset:
• with onset of ovulatory cycles, 1–2 years following the menarche.
• Associated menstrual symptoms;
• heavy menstrual bleeding is more likely in those with pathology such as fibroids
• symptoms such as headache and gastrointestinal symptoms are common but improve as menses progress. Examination
• Abdominal and pelvic examination will usually be normal.
• In secondary dysmenorrhoea, pelvic examination may reveal an
• enlarged uterus (fibroids)
• enlarged ovaries (endometrioma)
• palpable fallopian tube (hydrosalpinx due to infection)
• tenderness (endometriosis, pelvic inflammatory disease)
• nodules (endometriosis). Investigation
No investigation is required unless there
• is treatment failure
• is an abnormality detected on examination
• are other associated symptoms present suggestive of pathology.
Investigation includes either ultrasonography or laparoscopy.
Ultrasonography
This can be used to identify structural abnormality such as fibroids or uterine abnormality.
Laparoscopy
This is the best method for the diagnosis of endometriosis or pelvic inflammatory disease. Treatment
Primary dysmenorrhoea
Non-steroidal anti-inflammatory agents (NSAIDs)
These should be taken regularly during the menses commencing with the onset of the pain or bleeding (whichever comes first and continued until the pain completely disappears. Ibuprofen, mefenamic acid, and naproxen are all effective (Dingfelder 1981; Elstrom et al. 1989; Courtland Robinson et al. 1992).
Combined oral contraceptive pill
This is useful in women desiring contraception.
These treatments decrease prostaglandin production and hence decrease uterine contractility and increase blood flow to the uterus. Of women with primary dysmenorrhoea, 80% will be treated successfully with these drugs alone or in combination.
The levonorgestrel-secreting intrauterine system (LNGIUS) is also very valuable, even in those who do not achieve amenorrhoea (see above). However, it may be difficult to insert through a nulliparous cervix.
Vasopressin receptor antagonists have also been trialled and shown to be successful, although no oral preparations are yet available for use (Bossmar et al. 1997).
Preparations that lead to amenorrhoea will also relieve the problem. These include the gonadotrophins-releasing hormone agonists. However, long-term use is limited due to osteopenic side-effects, unless hormonal add-back therapy is coadministered. Continuous administration of progestagens may be effective and Danazol is a further option, although the use of these two therapies is often limited by side-effects.
Surgical treatment
Laparoscopic uterine nerve ablation has been advocated but the evidence of efficacy is poor and it is no longer recommended. Hysterectomy will be an appropriate option for some women and is discussed in Section 12.24, Menorrhagia.
The treatment of secondary dysmenorrhoea depends on the underlying pathology. It is usually less responsive to medical treatment unless this leads to amenorrhoea and may require surgical intervention.
Alternative treatments
Patients often enquire about the many alternative treatments such as herbal preparations, Chinese medicine, spinal manipulation, acupuncture, and many others. However, convincing evidence that they are effective is absent. Further reading
Akerlund M, Stromberg P, Forsling ML. Primary dysmenorrhoea and vasopressin. Br J Obstet Gynaecol 1979;86:484–7.
Andersch B, Milsom I. An epidemiologic study of young women with dysmenorrhea. Am J Obstet Gynecol 1982;144:655–60.
Bossmar T, Brouard R, Doberl A, Akerlund M. Effects of SR 49059, an orally active V1a vasopressin receptor antagonist, on vasopressin-induced uterine contractions. Br J Obstet Gynaecol 1997;104:471–7.
Courtland Robinson J, Plichta S, Weisman CS, et al. Dysmenorrhoea and use of oral contraceptives in adolescent women attending a family planning clinic. Am J Obstet Gynecol 1992;166:578–83.
Dawood MY. Dysmenorrhoea. Clin Obstet Gynecol 1990;33:168–78.
Dawood MY. Primary dysmenorrhea: advances in pathogenesis and management. Obstet Gynecol 2006;108:428–41.
Dingfelder JR. Primary dysmenorrhoea treatment with prostaglandin inhibitors. Am J Obstet Gynecol 1981;140:874–9.
Elstrom P, Junicka E, Laudanski T, et al. Effect of an oral contraceptive in primary dysmenorrhoea: changes in uterine activity and reactivity to agonists. Contraception 1989;40:39–47.
Hauksson A, Akerlund M, Melin P. Uterine blood flow and myometrial activity at menstruation, and the action of vasopressin and a synthetic antagonist. Br J Obstet Gynaecol 1988;95:898–904.
Lumsden MA, Kelly RW, Baird DT. Primary dysmenorrhoea: the importance of both prostaglandins E2 and F2α. Br J Obstet Gynaecol 1983;90:1135–40.
Marjoribanks J, Proctor ML, Farquhar C. Nonsteroidal anti-inflammatory drugs for primary dysmenorrhoea. Cochrane Menstrual Disorders and Subfertility Group. Cochrane Database Syst Rev 2008; 4: CD001751.
Proctor ML, Latthe PM, Farquhar CM, et al. Surgical interruption of pelvic nerve pathways for primary and secondary dysmenorrhoea. Cochrane Menstrual Disorders and Subfertility Group. Cochrane Database Syst Rev 2008; 4: CD001896.
Proctor ML, Roberts H, Farquhar CM. Combined oral contraceptive pill (OCP) as treatment for primary dysmenorrhoea. Cochrane Menstrual Disorders and Subfertility Group. Cochrane Database Syst Rev 2008; 4: CD002120.
Stromberg P, Akerlund M, Forsling MI, et al. Vasopressin and prostaglandin in premenstrual pain and primary dysmenorrhoea. Acta Obstet Gyncecol Scand 1984;63:533–8.
Wenzloff NJ, Shimp L. Therapeutic management of primary dysmenorrhea. Drug Intell Clin Pharm 1984;18:22–6.
Yap C, Furness S, Farquhar C. Pre and post operative medical therapy for endometriosis surgery. Cochrane Menstrual Disorders and Subfertility Group. Cochrane Database Syst Rev 2008; 4: CD003678.
Ectopic pregnancy Definition
The word ectopic is derived from the Greek word ektopos, which means out of place; an ectopic pregnancy is defined as implantation of a fertilized ovum outside the uterine cavity. It is an important cause of morbidity and mortality in women of reproductive age and is responsible for 75% of pregnancy related deaths in the first trimester (CEMACH 2007).
An ectopic pregnancy should be suspected in any woman of reproductive age, with a positive pregnancy test, presenting with abdominal pain and/or vaginal bleeding. Epidemiology
Over 10 000 ectopic pregnancies are diagnosed annually in the UK, with an overall incidence of 11 in 1000 pregnancies (CEMACH 2007). However, it is likely that the number of ectopic pregnancies in the population is much higher, as many of them follow a benign course and tend to resolve spontaneously without causing significant clinical symptoms. Despite an increase in the incidence, the mortality due to ectopic pregnancies remains stable at 3.4% of all maternal mortalities in the UK (CEMACH 2007). Aetiology
The main cause of ectopic pregnancy is damage to the tubal epithelium, which leads to implantation into the Fallopian tube. In cases with no evidence of anatomical tubal damage, the cause of ectopic pregnancy may be a dysfunction in the tubal smooth muscle activity secondary to an altered oestrogen–progesterone ratio (Pulkkinen and Talo 1987). This may adversely affect the transport of the fertilized egg into the uterus.
A number of risk factors have been identified which increase the risk of an ectopic gestation (Ankum et al. 1996). These include
• history of previous ectopic pregnancy
• pelvic inflammatory disease/chlamydia infection
• early age of intercourse and multiple partners
• history of infertility
• previous pelvic surgery
• IUCD in situ or sterilization failure
• use of emergency contraception
• assisted conception
• increased maternal age.
The most common site of an ectopic pregnancy is the Fallopian tube, accounting for nearly 95% of the cases. Other possible sites include the interstitial segment of the tube, cervix, deficient Caesarean section scar, ovary, and abdominal cavity. Clinical approach
History: key points
The most common symptom of ectopic pregnancy is irregular vaginal bleeding, which typically starts at the time of expected menstruation. Abdominal pain is a late clinical feature, which usually indicates the presence of intra-abdominal bleeding. The location of pregnancy in the tube usually determines the clinical presentation. The majority of the tubal ectopics are ampullary, and they present relatively early with vaginal bleeding and pain. In ectopics that are located more proximal to the uterus, such as isthmic and interstitial pregnancies, early warning signs are often absent and they may present with sudden rupture and severe haematoperitoneum.
A careful history should include the duration and severity of symptoms and the presence or absence of risk factors. A urine pregnancy test is usually positive, but negative results do not rule out the possibility of ectopic pregnancy in women with typical clinical presentation. Some women with ruptured ectopics may predominantly complain of gastrointestinal symptoms. This may delay the diagnosis and treatment, as has been previously described in cases with fatal outcomes.
Examination: key points
Abdominal and vaginal examination can be unremarkable, or may demonstrate signs of acute abdomen with rebound tenderness. Cervical excitation and/or adnexal tenderness may be found on bimanual pelvic examination. Where transvaginal ultrasound is available, bimanual pelvic examination adds little to the diagnosis and does not need to be routinely carried out. Women with a positive pregnancy test and clinical signs of intra-abdominal bleeding and cardiovascular instability should be operated on without delay, regardless of the imaging results.
Investigations
Transvaginal ultrasound
This is the front-line investigation in assessing haemodynamically stable patients with a suspected ectopic pregnancy. The majority of clinically significant ectopic pregnancies can be diagnosed on ultrasound scan prior to surgery (Condous et al. 2005).
In the past an ectopic pregnancy was suspected in women with a positive pregnancy test and an ‘empty uterus’ on ultrasound scan. In modern practice an ectopic pregnancy should be directly visualized on ultrasound examination. The diagnosis of ectopic pregnancy is based on the detection of an adnexal swelling separate from the uterus and the ovaries. The morphology of ectopic pregnancy varies, but in most cases, an extrauterine gestational sac with or without a yolksac or embryo can be seen (Fig. 12.9.1). With high resolution ultrasound equipment an ectopic pregnancy is often seen as nonhomogeneous solid swelling that moves separate from the ovary on palpation (sliding organ sign) (Timor-Tritsch and Rottem 1987) (Fig. 12.9.2).
The presence of an intrauterine pregnancy cannot be used to rule out the possibility of a concomitant ectopic pregnancy in women with clinical symptoms suggestive of an ectopic pregnancy. In some cases bleeding into the empty uterine cavity may create features on ultrasound scan suggestive of an early intrauterine pregnancy, which can cause diagnostic errors and delay in the diagnosis of ectopic.
Biochemical markers
The measurement of serum β-human chorionic gonadotropin (β-hCG) and progesterone may aid the diagnosis in women with a high index of suspicion for ectopic pregnancy, in whom a pregnancy is not visualized on the ultrasound scan.
Serum β-hCG
In a normal intrauterine pregnancy, serum hCG doubles every 1.4 days before 5 weeks’ gestation and 2.4 days between 5 and 7 weeks. A slow rise in β-hCG indicates an abnormal pregnancy; however, it does not discriminate between early intrauterine miscarriages and ectopic pregnancies. Also, β-hCG levels show a normal rate of increase in some ectopic pregnancies.
Fig. 12.9.1 An ultrasound scan showing an empty uterus (U) and a small gestational sac with a yolk sac in the left adnexa (arrow). These findings were conclusive of a left tubal ectopic pregnancy.
Serum progesterone
The production of progesterone from the corpus luteum responds rapidly to changes in hCG production from the trophoblast. Measurements of serum progesterone can therefore be used to assess viability of pregnancy. Serum progesterone of >60 nmol indicates a normal rise in hCG levels, usually associated with normal intrauterine pregnancies. Low progesterone level ipsilateral tubal pathology or haemorrhage after attempts at tubal conservation.
Salpingotomy is a procedure in which the Fallopian tube is conserved by removing the ectopic pregnancy through a linear incision. It is attempted if there is evidence of contralateral tubal damage and the woman desires further pregnancies. There is a high risk of intraoperative and postoperative bleeding and a 10–15% risk of persistent trophoblast, which may require further surgical/medical treatment (Hajenius et al. 2007).
It is unclear whether future reproductive outcomes are better after salpingotomy; however, the data from observational studies show slightly higher rates of intrauterine pregnancies after tubal conservation (Bangsgaard et al. 2003). A prospective randomized trial that aims to address this issue is currently under way (Mol et al. 2008). Until then the choice between the two approaches should be decided on an individual case basis.
Medical management
Methotrexate is the most commonly used drug for the medical management of ectopic pregnancy. It is a folic acid antagonist that inhibits DNA synthesis and cell division in the trophoblast. It can be given either systemically or locally within the ectopic gestational sac. When given as a single dose there is a small risk of side-effects such as gastritis, alopecia, nausea, vomiting, hepatic or renal impairment, leucopenia, and thrombocytopenia.
There are strict selection criteria for patients suitable for methotrexate administration:
• minimal clinical symptoms
• certain ultrasound diagnosis of ectopic
• no evidence of embryonic cardiac activity
• size need for another fresh cycle.
• When patients have over-responded to stimulation, elective cryopreservation of all embryos and replacement at a later date can be used as a strategy to minimize the risk of a patient developing severe ovarian hyperstimulation (OHSS), as pregnancy in a fresh treatment cycle is a risk factor.
• Embryo cryopreservation can be used as a method of fertility preservation by women about to undergo cancer treatment that is likely to impair their ovarian function and reserve of eggs.
• The costs of simple frozen embryo replacement cycles are considerably less than the cost of a further fresh cycle.
• Effective freezing programmes are essential to the proposed move towards single embryo transfer to minimize the risk of multiple pregnancy following IVF treatment. Legal aspects and regulation in the UK
• Freezing and storage of human embryos and gametes can only take place in units that have been licensed by the Human Fertilisation and Embryology Authority (HFEA).
• Valid consent to store embryos must be obtained from both partners, and if one partner withdraws consent embryos can no longer be kept in storage.
• If the embryo(s) have been created using donor eggs or sperm, the embryos may only be stored if the donor has also consented to the storage of embryos created using their donated gametes.
• The duration of storage is specified on the consent form and is usually 5 years in the first instance. It can normally be extended to 10 years if necessary, and for patients who have undergone cancer treatment likely to permanently impair their fertility gametes and embryos can be stored to the age of 55 years.
• It is illegal for embryos to be stored without valid consent so it is very important for patients to keep in contact with units if they move or their circumstances change. If the first 5-year storage period has expired without patients using the embryos and it is not possible to contact the couple, the embryos must be allowed to perish. How and when are embryos frozen?
Challenges of freezing embryos
• Human embryos contain cells that are relatively large and the main constituent of the cytoplasm is water. On cooling below freezing, temperature ice crystals start to form damaging intracellular structure and cellular membranes.
• The concentration of solutes within cells also increases, which can be toxic.
• The microtubules of metaphase spindles are also temperature sensitive and depolymerize on cooling.
• The highest risk time for cellular damage is during the freezing or thawing processes. An embryo must have at least 50% of its cells intact following thawing to retain the potential for further development.
• Once embryos are frozen, if conditions are kept stable, they can remain in storage for many years without further deterioration.
• Embryos are stored in liquid nitrogen tanks or dewars, which require careful maintenance to ensure they remain topped up. Many IVF units use alarm systems to alert the embryology team in the event of failure of a tank and a drop in liquid nitrogen levels that could jeopardize the stored embryos.
• Many patients’ embryos are stored in one dewar, and careful labelling of straws and ampoules is essential, together with regular audits of stored material.
Use of cryoprotectants
Cryoprotectants are used during the freezing of embryos to increase cell survival. The use of glycerol as a cryoprotectant for human sperm was first described in 1949. Since that time other cryoprotectants have also been used including propanediol (PROH), dimethylsulphoxide (DMSO), and ethylene glycol. Cryoprotectants decrease the freezing point of solutions and reduce the amount of salts and other solutes present in the remaining liquid phase, reducing the incidence of lipoprotein denaturation. Some protocols also use high concentrations of sucrose together with cryoprotectants to assist the dehydration of cells and reduce the risk of ice crystals forming.
Stage of embryo development for freezing
Embryos may be stored soon after fertilization at the pronuclear (1 cell) stage, after early cleavage, or at the blasto-cyst stage
a. Pronuclear stage zygotes are relatively stable with high survival rates after freezing and PROH is often used as the cryoprotectant with sucrose. This is often the stage chosen to freeze embryos when all embryos are going to be stored without a fresh transfer (e.g. fertility preservation or reducing OHSS risk). When pronucleate embryos are thawed they are allowed to continue their development for a further 1–5 days before transfer to the uterus. Survival rates of around 70% are expected following pronucleate stage freezing with pregnancy rates of 17–31%.
b. Most embryos have been frozen at the cleavage (2–8 cell) stage following the transfer of fresh embryos 2 or 3 days after egg collection. DMSO or PROH are used as cryoprotectants at this stage. Cryopreservation of day 2 embryos has been shown to be associated with a 30% reduction in implantation potential.
c. Extended culture of embryos to the blastocyst stage of development is becoming more common in IVF units. Blastocyst culture allows identification of the embryo or embryos that have the best potential for continued development and implantation. This helps selection of a single embryo for replacement into the uterus to reduce the risk of multiple pregnancy. Other surplus blastocyst embryos can be cryopreserved by slow freezing or vitrification (see below). If this approach is adopted there are usually fewer embryos available for transfer and freezing as many human embryos exhibit developmental arrest before the blastocyst stage. Pregnancy rates as high as 60% per transfer have been reported following transfer of thawed vitrified blastocysts.
Slow cooling or vitrification
Embryos are stored in ampoules or vials in the freezing solutions and traditionally have been slow cooled to –30 to –40°C before being plunged into liquid nitrogen. To try and reduce the risk of ice crystal formation during cooling, an alternative approach of vitrification has been used. Vitrification uses high concentrations of cryoprotectants and sucrose and rapid cooling to –196°C resulting in a solid glass like state without ice crystal formation. Survival rates of 70–90% are reported following vitrification, with better embryonic survival, development, and pregnancy rates. Frozen embryo replacement cycles
Frozen thawed embryos can be replaced in natural cycles or artificially controlled cycles using hormone replacement therapy (HRT).
• In natural cycle replacement ultrasound is used to identify the dominant follicle and endometrial development. Ovulation is either detected by monitoring for the luteinizing hormone (LH) surge or initiated using an injection of LH or human chorionic gonadotrophin (hCG) once the follicle reaches 17–22 mm diameter. Embryos are thawed and transferred the appropriate number of days after ovulation depending on the stage at which they were frozen. The appropriate endometrial changes for implantation are produced by the normal ovarian secretion of oestradiol followed by oestradiol and progesterone in the luteal phase.
• For women that do not have regular ovulatory cycles it is possible to replicate the pattern of endometrial development artificially using oestradiol orally or transdermally followed by the addition of progesterone supplementation to create a secretory endometrium. Ultrasound is used to measure endometrial thickness, which ideally needs to be 8 mm or more. Some units routinely use HRT cycles for frozen embryo replacement as it may help in planning workload. In women who are ovulatory it may be important to suppress the natural cycle using gonadotropin-releasing hormone analogues before stimulating endometrial development.
Table 12.10.1 IVF and ICSI success rates 2006 UK (with permission from HFEA www.hfea.gov.uk)

Outcome of frozen embryo replacement cycles
Success rates
The implantation potential of frozen thawed embryos is not as good as fresh (Table 12.10.1), resulting in lower pregnancy and live birth rates per cycle. There is an age-related decline in pregnancy rates as seen in fresh cycles, although the drop is less marked in women 40 years and over. This is likely to reflect the following factors:
• Patients who have sufficient embryos to freeze tend to be better prognosis patients with a higher chance of pregnancy in the fresh cycle.
• Patients who have had a live birth following a fresh cycle are more likely to have a successful outcome from a subsequent frozen cycle.
• The age at which embryos are replaced for frozen cycles may be very different from the age at which embryos were originally created. Maternal age at the time of the fresh cycle influences the proportion of embryos that are aneuploid and live birth rates.
Congenital abnormalities
Studies examining the outcome of children born following frozen embryo replacement have been reassuring, with no increase in levels of congenital abnormalities to those born following fresh IVF cycles. Frequently asked questions
Are there any more abnormalities in babies born using frozen thawed embryos?
All pregnancies carry a small risk of babies being born with abnormalities, and studies have shown that this risk is no higher for babies born after frozen embryo replacement than after transfer of fresh embryos.
Do embryos deteriorate the longer they are kept in storage?
Some embryos do not survive the freezing and thawing process but this is due to the changes that occur to the embryo on cooling and warming. Once an embryo is frozen, studies have shown that the survival rates and pregnancy rates following frozen embryo replacement are not influenced by the length of time the embryo was stored. Further reading
Albuquerque LE, Saconato H, Maciel, MC. Depot versus daily administration of gonadotrophin-releasing hormone agonist protocols for pituitary desensitization in assisted reproduction cycles. Cochrane Database Syst Rev 2005; 1: CD002808.
Avery S, Marcus S, Spillane S, et al. Does the length of storage time affect the outcome of frozen embryo replacement? J Assist Reprod Genet 1995; 12: 675.
Balanban B, Urman B, Ata B, et al. A randomized controlled study of human day 3 embryo cryopreservation by slow freezing or vitrification: vitrification is associated with higher survival, metabolism and blastocyst formation. Hum Reprod 2008;23:1976–82.
Braude P. One Child at a time. Reducing multiple births after IVF. Human Fertilisation and Embryology Authority (HFEA) at www.hfea.gov.uk/docs/MOSET_report_Final_Dee_06.pdf.
Edgar DH, Bourne H, Jericho H, McBain JC. A quantitative analysis of the impact of cryopreservation on the implantation potential of human early cleavage stage embryos. Hum Reprod 2000;15:175–9.
El-Toukhy T, Khalaf Y, Al-Darazi K, et al. Cryo-thawed embryos obtained from conception cycles have double the implantation and pregnancy potential of those from unsuccessful cycles. Hum Reprod 2003;18:1313–18.
El-Toukhy T, Taylor A, Khalaf Y, et al. Pituitary suppression in ultrasound-monitored frozen replacement cycles. A randomized study. Hum Reprod 2004;19:874–9.
Granne I, Child T, Hartshorne G. Embryo cryopreservation: Evidence for practice. Hum Fertil 2008;11:159–72.
Loutradi KE, Kolibianakis EM, Venetis CA, et al. Cryopreservation of human embryos by vitrification or slow freezing: a systematic review and meta-analysis. Fertil Steril 2008;90:186–93.
Polge C, Smith AU, Parkes AS. Revival of spermatozoa after vitrification and dehydration at low temperature. Nature 1949; 154: 666.
Rama Raju GA, Jaya Prakash G, Murali Krishna K, Madan K. Neonatal outcome after vitrified day 3 embryo transfers: a preliminary study. Fertil Steril 2009;92:143–8.
Riggs R, Mayer J, Dowling-Lacey D, et al. Does storage time influence postthaw survival and pregnancy outcome? An analysis of 11,768 cryopreseved human embryos. Fertil Steril 2010;93:109–15.
Son WY, Yoon SH, Yoon HJ, et al. Pregnancy outcome following transfer of human blastocysts vitrified on electron microscopy grids after induced collapse of the blastocoele. Hum Reprod 2003;18:137–9.
Stachecki J, Garrisi J, Sabino S, et al. A new safe, simple, and successful vitrification method for bovine and human blastocysts. Reprod Biomed Online 2008;17:360–7.
Takahashi K, Mukaida T, Goto T, Oka C. Perinatal outcome of blastocyst transfer with vitrification using cryoloop: a 4-year follow-up study. Fertil Steril 2005;84:88–92.
Trounson A, Mohr L. Human pregnancy following cryopreservation, thawing and transfer of an eight-cell embryo. Nature 1983;305:707–9.
Vanderzwalmen P, Bertin G, Debauche Ch, et al. Births after vitrification at morula and blastocyst stages: effect of artificial reduction of the blastcoelic cavity before vitrification. Human Reprod 2002;17:744–51.
Emergency contraception
Ninety per cent of unplanned pregnancies are user related and 50% of women who present for a termination of pregnancy are current or recent users of a contraceptive. The need for a preventative post-coital method was recognized in ancient times and has been cited in medical folklore. Modern emergency contraceptives are either oral pills that are taken within a designated time after exposure or the use of a copper bearing intrauterine device.
In countries where no licensed products exist, woman resort to DIY emergency contraception using available combined or progestogen only pills to make up the recommended effective dosage. Types of emergency contraception
• Combined emergency hormonal contraception comprises two doses each of 100 μg of ethinyloestradiol and 500 μg of levonorgestral. The first dose is taken within 72 hours of unprotected intercourse followed by a second dose 12 hours later.
• Progestogen-only emergency hormonal contraception (PEHC) comprises a single dose of 1500 μg of levonorgestral taken within 72 hours of unprotected intercourse. This is now the predominant emergency oral contraceptive available worldwide and the only product that is available in the UK. The prescription-only product is called Levonelle 1500; the pharmacy over-the-counter product is called Levonelle One Step.
• A new emergency oral contraceptive to be introduced in 2009 is a single dose of a selective oestrogen receptor modulator that has sustained efficacy for up to 120 hours and has the advantage of being non-steroidal.
• Antiprogesterones in the form of Mifepristone have been successfully used for emergency contraception in a single dose of 10 mg used within 72 hours of unprotected intercourse. China has a licensed preparation.
• A copper-bearing intrauterine device is the most effective emergency contraceptive and can be used up to 5 days from unprotected intercourse. It has a number of other versatile features (see box).
• Ulipristal acetate 30 mg single dose is now licensed in the UK and USA for emergency contraception up to 120 hours after unprotected intercourse. Ulipristal is a selective progesterone receptor modulator and works after the LH surge to block follicular rupture, an action that the traditional levonorgestrel emergency contraception lacks. Mechanism of action
Emergency contraceptives are not abortifacients. Hormonal emergency contraception prevents or delays ovulation when taken before ovulation and is likely to interfere with endometrial, ovarian, and tubal mechanisms in a way that prevents or disrupts fertilization. The emergency IUD works in a similar way at endometrial and tubal levels disrupting fertilization. Prevention of implantation is the exception not the rule. Efficacy of emergency contraception
The efficacy of the PEHC was confirmed by two World Health Organization randomized controlled trials published in 1998 and 2002. At mid-cycle the risk of conception from a single unprotected intercourse can be up to 30%, with the average risk of conception for a single random act of intercourse being 4%. No cycle days can be deemed 100% safe. Efficacy is best expressed as the percentage of expected pregnancies prevented by emergency contraception. EHC prevents 8/10 pregnancies and an IUD 9/10 pregnancies. Women who take EHC within 24 hours of unprotected intercourse avoid 95% of expected pregnancies whereas those who take the pill beyond 48 hours would expect a protection rate of about 60%. Limited research suggests that this 60% protection is maintained up to 120 hours, but levonelle is not licensed for use beyond 72 hours.
Special advantages of an emergency IUD.
1. Failure rate extremely low
2. Effective up to 120 hours after intercourse
3. Effective up to 120 hours after earliest calculated date of ovulation
4. Can cover multiple exposures
5. An alternative to hormonal methods
6. Provide contraception for the rest of the cycle
7. Can be kept as an ongoing contraceptive
8. Conversely can be removed with the next menses
9. The traditional contraindications that apply to IUDs do not apply to the IUDs intended for emergency contraception, the exception being the risk of infection which needs to be excluded, tested for, or treated prophylactically
The copper IUD prevents up to 99% of expected pregnancies. Indications
The two main indications are unprotected intercourse, and condom breakage and slippage.
Special indications include missing pills. Impact
In the UK, emergency contraception has been promoted since the early 1980s. Over 1.5 million units of emergency hormonal contraception are dispensed every year, with the majority being provided by pharmacists. Every year 5% of women aged 16–49 use emergency contraception once, with 1% using it two or more times. The expectation that emergency contraception would reduce unplanned pregnancies and abortion rates cannot be ethically tested, but there is consensus that the method has not had the predicted impact on these variables. The main reason is that access to correct information and to free provision remains patchy and couples tend to underestimate the risk of unplanned pregnancy and therefore are unlikely to resort to the method in risky situations which they wrongly perceive as being safe.
Strategies to improve access include advance provision, increasing information about the emergency IUD and promoting immediate (so-called quick start) of an ongoing method of contraception following EHC. Safety
The emergency IUD is an extremely safe contraceptive as long as the woman is assessed for the risk of infection, preferably screened for sexually transmitted infections, and where there is a high sexually transmitted infection risk given prophylactic antibiotics. Depending on the result of the test, partner notification is also required.
The hormonal methods are also safe with the only contraindications being allergy to the component hormone, pregnancy where the method is unlikely to work, and porphyria. Inadvertent use of emergency contraception in early pregnancy is unlikely to lead to congenital abnormalities but counselling should stress the fact that a normal pregnancy outcome can never be guaranteed.
The side-effects of EHC are all minor and infrequent; they include nausea (14%), vomiting (1%), and breast pain (8%). Cycle disruption is the exception rather than the rule, with 90% of users having their next menses on time or within 7 days of the expected time of menstruation. Counselling points
• Estimate the pregnancy risk, describe the mechanism of action, and inform the woman about the failure risk.
• Prescribe the single dose Levonorgestral EHC.
• Emphasize that the IUD is the most effective form of emergency contraception.
• Emergency contraception is not effective if the woman is already pregnant and has no abortifacient action.
• Encourage the administration of emergency hormonal contraception as early as possible within the 72-hour window.
• The use of EHC up to 120 hours is permitted but unlicensed.
• Domperidone 10 mg is the antiemetic of choice.
• Broad-spectrum antibiotics do not interact with EHC but where liver enzyme inducers are used, a double dose of Levonorgestral should be taken stat.
• The protection of emergency hormonal contraception is not prospective and the woman should abstain or use condoms until her next period.
• Any ongoing contraceptive can be started immediately, provided the woman is fully counselled.
• Multiple doses of EHC can be administered in the same cycle but tend to be much less effective than a regular ongoing method of contraception.
• There is no need to perform tests or examinations prior to prescribing EHC.
• Follow-up is desirable, usually 3 weeks post treatment. Users should be encouraged to return if subsequent menstruation is delayed or abnormal in any way.
• EHC is unlikely to increase the risk of ectopic pregnancy but the risk of an ectopic should always be high in the awareness of the practitioner. Further reading
Anon. Faculty of Family Planning and Reproductive Health Care. Royal College of Obstetricians and Gynaecologists, Guidance April 2000. Emergency contraception: recommendations for clinical practice. Br J Fam Plann 2000;26:93–6.
Black K, Kubba A. Is there a link between ectopic pregnancy and progestogen-only emergency contraception? Trends Urol Gynaecol Sexual health 2003;8:5–6.
Croxatto HB. Emergency contraception pills: how do they work? IPPE Medical Bulletin 2002;336:1–2.
Glasier A, Baird D. The effects of self-administering emergency contraception. N Engl J Med 1998;339:1–4.
Glasier AF, Cameron ST Fine PM, et al. Ulipristal acetate versus levonorgestrel for emergency contraception a randomised noninferiority trial and meta-analysis. Lancet 2010;375:555–62.
IPPF International Medical Advisory Panel. Statement on emergency contraception. IPPF Medical Bulletin 2004;38:1–3.
Piaggio G, von Hertzen H, Grimes DA, et al. On behalf of the Task Force on Postovulatory Methods of Fertility Regulation. Timing of emergency contraception with levonorgestrel or the Yuzpe regimen. Lancet 1999; 335: 731.
Raman-Wilms L, Tseng Al Wighard TS, et al. Fetal genital effects of first-trimester sex hormone exposure; a meta-analysis. Obstet Gynecol 1995;85:141–9.
Task Force on Postovulatory Methods of Fertility Regualation. Randomised, controlled trial of levonorgestrel versus the Yuzpe regimen of combined oral contraceptive for emergency contraception. Lancet 1998;352:428–33.
UNDP/UNFPA/WHO/World Bank Special Programme of Research Development and Research Training in Human Reproduction. Task Force on Post-Ovulatory Methods of Fertility Regulation. Efficacy and side effects of immediate poscoital levonorgestrel used repeatedly for contraception. 2000;61:303–8.
Von Hertzen H, Piaggia G, Ding J, et al. Low dose mifepristone and two regimens of levonorgestrel for emergency contraception: a WHO multicentre randomised trial. Lancet 2002;306:1803–10.
Webb A, Shochet T, Bigrigg A, et al. Effect of hormal emergency contraception on bleeding patterns. Contraception 2004;69:133–5.
Wilcox AJ, Dunson DB, Weinberg CR, et al. Likelihood of conception with a single act of intercourse, providing benchmark rates for assessment of pos-coital contraceptives. Contraception 2002;63:211–15.
Yuzpe AA, Percival Smith R, Rademaker AW. A multi-center investigation employing ethinylestradiol combined with DL-norgestrel as a post-coital contraceptive agent. Fertil Steril 1982;37:508–13.
Yuzpe AA. Lance WJ. Ethinylestradiol and DL-norgestrel as a post-coital contraceptive. Feril Steril 1977;28:932–6. Internet resources
WHO emergency contraception database: www.who.int/reproductive-health/family_planning/methods.htm Patient resources
Princeton University’s emergency contraception website: http://ec.princeton.edu/
Endometriosis Definition
Endometriosis is defined by the presence of endometrial-like tissue in sites outside the uterus, e.g. the peritoneum, ovaries, and rectovaginal septum. It produces peritoneal inflammation and fibrosis, and can lead to the formation of endometriomas (ovarian cysts) and pelvic adhesions. Aetiology
The cause is still unknown but retrograde menstruation is probably a permissive factor. There is increasing evidence that the disease is inherited as a complex genetic trait.
Risk factors relate to oestrogen levels (smoking history and peripheral body fat) and increased menstruation (shorter cycle length and longer duration of flow). Associated symptoms
Some or all of the following symptoms may be present:
• severe dysmenorrhoea (painful periods)
• deep dyspareunia (pain on intercourse)
• chronic, non-menstrual pain
• pain at ovulation
• dyschezia (pain on defaecation)
• infertility
• cyclical or perimenstrual symptoms (often bowel or bladder related) ± abnormal bleeding
• chronic fatigue.
However, the predictive value of these symptoms for the diagnosis is poor, as each can have other causes and many affected women are asymptomatic. Impact on quality of life
Endometriosis has a major impact on quality of life and work productivity. Women may need multiple admissions for surgery and/or prolonged treatment with costly drugs, which often have problematic side-effects. Associated cancers
Large cohort studies suggest that endometriosis is a risk factor for ovarian cancer and non-Hodgkin’s lymphoma. Examination: key points
• Pelvic tenderness
• Fixed retroverted uterus
• Tender uterosacral ligaments ±deeply infiltrating nodules (especially if performed during menses)
• Enlarged ovaries
• Visible lesions in the vagina or on the cervix.
• Although these findings are suggestive of the diagnosis, the examination may be normal. Diagnosis
• Visual inspection of the pelvis at laparoscopy is the gold standard investigation to establish the diagnosis, unless disease is visible in the vagina or elsewhere.
• Histology should be obtained if endometriomas (>4 cm) or deeply infiltrating disease are present to confirm the diagnosis and exclude rare instances of malignancy. It is uncertain if histology is required for peritoneal disease.
• Disease severity is classified by a four-point scale (stage I–IV or minimal–severe) based on peritoneal lesion size and location, and the presence of endometriomas/adhesions. Investigations
• Transvaginal ultrasound is useful to both diagnose and exclude an ovarian endometrioma; it has no role in diagnosing peritoneal disease.
• Serum CA125 may be elevated, especially in severe disease, but it is not useful as a diagnostic test.
• MRI ±ultrasound ±barium/IVP studies may allow disease severity to be assessed when other organs are involved, e.g. bowel, ureter, or bladder. Empirical treatment
Empirical treatment for pain symptoms presumed to be endometriosis without a definitive diagnosis includes counselling, analgesia, progestagens, the combined oral contraceptive (COC), and nutritional therapy. COC use may be conventional, continuous, or in a tricycle regimen. Treatment: endometriosis-associated pain
Hormonal treatment
Ovarian suppression with COCs, danazol, gestrinone, medroxyprogesterone acetate, or gonadotropin-releasing hormone (GnRH) agonists reduces pain. The drugs are equally effective but their side-effects and cost profiles differ.
Treatment is usually given for 6 months. Longer use is problematic for GnRH agonists because of side-effects. Symptom recurrence after treatment is common.
The levonorgestrel intrauterine system is also effective.
GnRH agonist treatment plus ‘add-back’ therapy Side-effects of GnRH agonists include:
• menopausal symptoms e.g. hot flushes, headaches, loss of libido, vaginal dryness
• loss of bone mineral density that is usually reversible.
These can be prevented by using hormone replacement therapy (HRT), e.g. tibolone, as ‘add-back’, which allows treatment to be prolonged beyond the 6-month licence. The efficacy of the GnRH agonist is unaffected.
Surgical treatment
Ideal practice is to diagnose and treat disease surgically at the same operation, provided that informed consent has been obtained.
Ablating peritoneal lesions plus laparoscopic uterine nerve ablation (LUNA) in stage I–III disease reduces pain at 6 months compared with laparoscopy alone; the smallest effect is seen in stage I disease. However, LUNA is probably not a necessary component of the treatment.
Pain can be reduced in severe and deeply infiltrating disease by removing the entire lesions. If a hysterectomy is performed, all visible endometriotic tissue should be removed at the same time.
Bilateral salpingo-oophorectomy (BSO) at hysterectomy usually provides pain relief and leads to a reduced need for future surgery.
There is no benefit using pre- or postoperative hormonal treatment for additional pain relief.
Hormone replacement therapy
HRT is recommended after BSO in young women; the risk of recurrent disease taking oestrogen alone is small.
Adding a progestagen to HRT after hysterectomy is not necessary, unless there is residual disease present as there is a small risk of malignant transformation. Endometriosis-associated infertility
Numerous mechanisms have been proposed to explain the association between endometriosis and infertility, e.g. anatomical distortion due to ovarian endometriomas and dense adhesions. Whether other factors are causal is still uncertain, especially in peritoneal disease. They include
• abnormal folliculogenesis
• increased sperm phagocytosis
• peritoneal fluid toxicity
• elevated serum auto-antibody levels
• altered endometrial receptivity.
Treatment
Hormonal treatment
Ovarian suppression to improve pregnancy rates in stage I–II disease is not effective and should not be offered for this indication alone. Its role in more severe disease has not been assessed.
Surgical treatment
The results of a meta-analysis indicate that ablation of lesions ±adhesiolysis in stage I–II endometriosis improves pregnancy rates compared with laparoscopy alone, but the data have been challenged because of methodological problems with the studies. There is no role for postoperative hormonal treatment.
If an ovarian endometrioma >4 cm is present, performing a laparoscopic cystectomy is preferable to drainage and coagulation, as the latter procedures are associated with a higher risk of cyst recurrence and lower pregnancy rates. Assisted reproduction
Intrauterine insemination
Stimulated intrauterine insemination is effective in stage I–II disease.
In vitro fertilization
In vitro fertilization (IVF) is appropriate treatment for endometriosis, especially if there are other problems such as male factor infertility, or if other treatments have failed. Problems include
• decreased oocyte numbers
• difficulties with ovarian scanning and access to the follicles due to endometriomas
• increased infection rates (related to the presence of an endometrioma).
It has also been suggested that oocyte quality is affected, which might explain the lower pregnancy rates than tubal infertility reported in a meta-analysis of published studies.
However, pregnancy rates in large national databases are not lower in patients with endometriosis, which makes it difficult to decide whether the disease has an adverse effect on IVF outcome or not.
Pre-IVF ovarian cystectomy
If an ovarian endometrioma ≥4 cm is present, performing a laparoscopic cystectomy before IVF is sensible to
• improve access to follicles
• obtain a histological diagnosis
• possibly improve ovarian response
• reduce the risk of infection
• The principal risks are reduced ovarian function after surgery and the loss of the ovary. Coping with disease
Complementary therapies
Although there is evidence that vitamin B1, acupuncture, TENS and magnesium may help primary dysmenorrhoea, the role of complementary therapies in endometriosis is unclear.
Many sufferers report that nutritional therapy, as well as homeopathy, reflexology, traditional Chinese medicine, or herbal treatments, improve symptoms of pain. Patient support groups
Patient self-help groups provide invaluable counselling, support, and advice.
The website www.endometriosis.org/support.html gives a comprehensive list of all self-help groups in the world. Many deliver self-management programmes that may be beneficial in providing women with tools to enable them to live with a chronic disease. Further reading
Barlow DH, Kennedy S. Endometriosis: new genetic approaches and therapy. Annu Rev Med 2005;56:345–56.
Barnhart K, Dunsmoor-Su R, Coutifaris C. Effect of endometriosis on in vitro fertilization. Fertil Steril 2002;77:6–55.
D’Hooghe T, Hummelshoj L. Multi-disciplinary centres/networks of excellence for endometriosis management and research: a proposal. Hum Reprod 2006 11;21:2743–8.
Gambone JC, Mittman BS, Munro MG, et al, the Chronic Pelvic Pain/Endometriosis Working Group Consensus statement for the management of chronic pelvic pain and endometriosis: proceedings of an expert-panel consensus. Fertil Steril 2002;78:961–72.
Kennedy S, Bergqvist A, Chapron C, et al. ESHRE guideline for the diagnosis and treatment of endometriosis. Hum Reprod 2005;20:2698–704.
Practice Committee of ASRM. Endometriosis and infertility. Fertil Steril 2006; 86 (5 Suppl): S156–60.
Practice Committee of ASRM. Treatment of pelvic pain associated with endometriosis. Fertil Steril 2006; 86 (5 Suppl): S18–27.
Royal College of Obstetricians and Gynaecologists (RCOG) The investigation and management of endometriosis. Greentop Guideline. London: RCOG 2006 www.rcog.org.uk/resources
Simoens S, Hummelshoj L, D’Hooghe T. Endometriosis: cost estimates & methodological perspective. Hum Reprod Update. 2007;13:395–404. Patient resources
Support group: Endometriosis UK, Tel. 020 7222 2781: www.endometriosis-uk.org/
Female infertility Definition
Infertility may be defined as the inability of a couple to conceive after 2 years of unprotected intercourse, in the absence of known reproductive pathology. Approximately 84% of young couples attempting to conceive will do so within a year, and referral for further investigation is normally appropriate after this time. Around half of the remaining ‘infertile’ couples will conceive within the second year without treatment. No cause for infertility is found in approximately one-quarter of infertile couples, whereas 15% have multiple causes. Diagnosis
The diagnosis of infertility can be extremely emotionally distressing and should be handled with sensitivity. The initial investigation of the infertile woman will typically include a detailed history. Consider early investigation in women aged 35 and above, or with a history of
• amenorrhoea or oligomenorrhea
• previous infertility
• treatment for cancer
• fibroids, endometriosis or pelvic inflammatory disease (PID)
• cervical dysplasia
• pelvic or abdominal surgery.
Circulating hormone levels along with ultrasound scan may distinguish between ovulatory/hormonal and obstructive/developmental disorders. Blood tests include:
• Progesterone in the mid-luteal phase of the menstrual cycle. This is day 21 of a 28-day cycle; however, in the case of irregular or long menstrual cycles the test may be conducted later and/or repeated weekly until the commencement of the next cycle. Normal values are 3–20 ng/mL (9.54–63.6 nmol/L).
• Follicle-stimulating hormone (FSH): basal day 3 (range, days 2–5). Normal values are 3.0–20.0 U/L.
• Luteinizing hormone (LH) basal day 3 (range, days 2–5). Normal values are 2.0–15.0 U/L.
• Oestradiol basal day 3 (range, days 2–5) of the cycle. Normal values are 50–145 pg/mL (184-532 pmol/L).
• Prolactin. Normal premenopausal values are 2-20 ng/mL.
• Total serum testosterone. Normal values are 6–86 ng/dL (0.21–2.98 nmol/L).
• Dehydroepiandrosterone sulphate (DHEAS). Normal pre-menopausal values are 12–535 μg/dL.
• 17-hydroxyprogesterone basal day 3 (range, days 2–5) of the cycle. Normal values are 20–100 ng/dL (0.6–3.0 nmol/L).
• Anti-Müllerian hormone (AMH). Normal values are 15–28 pmol/L (2–4 ng/mL).
Ultrasound investigation
Ultrasound scan of the pelvis can be performed transabdominally or transvaginally. Transabdominal ultrasound provides a global assessment and normally precedes transvaginal scan. Hysterosalpingo-contrast sonography (HyCoSy) using a high contrast dye medium may also be conducted to assess tubal patency.
Saline infusion sonography (SIS) is a more recent development where saline is introduced into the uterine cavity by a small catheter prior to vaginal probe ultrasound. The liquid helps create an interface with the lining of the uterus and abnormal structures can be seen on imaging.
This technique may be combined with Doppler sonography, which estimates blood flow. Ultrasound may provide information regarding
• congenital abnormalities, including enlarged uterus, absence of uterus, uterus didelphys, bicornis bicollis, bicornis unicollis, uterus subseptae, uterus arcuatus, and uterus unicornis. A septate or double vagina may occur
• uterine cavity, endometrial thickness, and myometrium evaluation
• ovarian morphology and volume, including antral follicle count, cysts solid tumours, and endometriomas
• abnormalities of the fallopian tube commonly present as adnexal masses and generally result from salpingitis, endometriosis, or peritubal adhesions. Patency of fallopian tubes may be assessed by HyCoSy
• uterine and follicular blood flow.
Sexually transmitted infections
Further investigations in women include tests for infection, especially Chlamydia trachomatis, which can lead to pelvic inflammatory disease or tubal occlusion. Screening should be offered prior to uterine investigations, as with other sexually transmitted diseases. Ovulatory disorders
Premature ovarian failure
Aetiology
Premature ovarian failure (POF) is idiopathic in the majority of cases; however, known genetic causes include, Turner’s syndrome, ovarian agenesis, 46XY gonadal dysgenesis, familial POF, fragile X syndrome, gonadotrophin receptor gene mutations, and galactosaemia. Possible environmental causes are chemotherapy, pelvic radiation, autoimmunity, ovarian malignancy, viruses, toxins, or surgery.
Diagnosis
It is characterized by hypergonadotrophic ovulatory failure, leading to secondary hypergonadotrophism. Diagnosis is usually by the finding of amenorrhoea and low oestrogen or progesterone in the presence of normal or high gonadotrophins (FSH and LH). Low oestrogen concentrations may result in menopause-type symptoms, but these are common to other causes of amenorrhoea and in isolation do not necessarily indicate POF. In a minority of cases ovarian failure is temporary, and so hormone measurements taken some weeks apart may be advised. Genetic diagnosis is required to confirm specific genetic causes.
Treatment
Hormone replacement therapy (HRT) using conjugated oestrogens or oestradiol valerate, which may be delivered orally or by transdermal patch. Progesterone is advised for patients with an intact uterus in order to avoid oestrogen-induced endometrial hyperplasia. Testosterone administration is rarely required when the adrenal gland continues to supply androgens. Treatments have a neutral effect on fertility but return of reproductive function, sometimes spontaneously, has been reported. Embryo or egg donation, remain an option however.
Hypothalamic/pituitary dysfunction
Aetiology
Pulsatile hypothalamic secretions of gonadotrophin-releasing hormone (GnRH) are transported along the capillary plexus in the pituitary stalk and stimulate the anterior pituitary to secrete gonadotrophins, LH and FSH. Disorders in this axis are characterized by hypogonadotrophic hypogonadism, leading to ovulatory failure and amenorrhoea. Hypothalamic disorders account for approximately 35% of patients presenting with amenorrhoea.
Structural lesions to the hypothalamus or pituitary may lead to absence of GnRH secretion or failure of GnRH delivery to the pituitary. Constriction by tumours such as glioma and craniopharyngiomas may be the cause. Granulomas (resulting from tuberculosis or sarcoidosis) are also sometimes implicated. Other physical causes include trauma, cranial irradiation, or postpartum pituitary necrosis (Sheehan’s syndrome).
Disruption of neurotransmitters that control GnRH secretion may be precipitated by stress, or sudden weight loss and malnutrition (including anorexia nervosa). In addition, strenuous exercise may inhibit GnRH secretion by the hypothalamus via the action of endogenous opioids. Similarly, drug abuse can result in suboptimal functioning of the hypothalamus.
Rarely, congenital GnRH deficiency may manifest as Kallman’s syndrome, which can result from an inherited X-linked condition, an autosomal dominant condition, or as an autosomal recessive condition and can be accompanied by anosmia.
Diagnosis
Diagnosis is usually by the finding of amenorrhoea, anovulation and low oestrogen or progesterone along with low gonadotrophins (FSH and LH). If these are present consider the following causes:
• cerebral or pituitary tumours
• vascular malformations
• stress
• sudden weight loss (including anorexia nervosa)
• strenuous exercise
• drug abuse
• genetic disorders.
Treatment
Clomiphene citrate: the first line of treatment may be the anti-oestrogen, which induces ovulation by countering oestrogenic inhibition of the hypothalamus and causing the pituitary to release gonadotrophins. If alone is unsuccessful, gonadotrophins are given in order to apply stimulation directly to the ovary.
Gonadotrophin replacement: an alternative treatment involves initial pituitary downregulation using GnRH agonist/antagonist followed by gonadotrophin replacement using urinary derived menopausal human gonadotrophin (containing FSH and LH). Recombinant FSH preparations are also available. Complications include ovarian hyper-stimulation syndrome (OHSS) and multiple births.
GnRH replacement: pulsaltile delivery of synthetic GnRH via mini-infusion pump has been employed and has several theoretical advantages over exogenous gonadotrophins in that it enables the patients own gonadotrophins to be used for stimulation and instigates appropriate natural pituitary feedback mechanisms limiting endogenous FSH.
Hyperprolactinaemia
Aetiology
Prolactin suppresses GnRH and FSH secretion. Pituitary secretion of prolactin itself is normally suppressed by dopamine. The use of prescription drugs that block dopamine at the pituitary or deplete brain dopamine levels is a common cause of hyperprolactinaemia. These drugs include some tranquilizers, antiemetics, and antipsychotic medicines.
Alternatively, a prolactinoma directly secreting prolactin into the circulation, or other structural lesions inducing pressure on the pituitary stalk, thereby blocking the flow of dopamine to the prolactin secreting tissues, may be responsible. Stress and other mediators of neurotransmitters may also affect control mechanisms for prolactin secretion. Finally, hypothyroidism is an important cause of prolactinaemia via elevated levels of thyrotropin-releasing hormone.
Diagnosis
Symptoms of hyperprolactinaemia include
• oligomenorrhea
• amenorrhoea
• galactorrhea
• infertility.
High prolactin levels should be confirmed by repeat testing at least once before further diagnostic evaluation and treatment. It is also important to check for hypothyroidism by repeat thyroid function tests. Pituitary imaging by computerized tomography (CT) or nuclear magnetic imaging (MRI) scans may be included as part of a definitive diagnosis or ongoing surveillance of prolactinoma.
Treatment
Dopamine agonist: consider dopamine agonist treatment (e.g. bromocriptine) to restore the menstrual cycle. A more recent and long-acting dopamine agonist, cabergo-line, has fewer side-effects. Surgical resection or irradiation of the prolactinoma is generally restricted to the minority of patients with low tolerance or resistance to dopamine agonists. Withdrawal of antidopaminergic drugs should be attempted followed by repeat testing where this cause is suspected.
Polycystic ovary syndrome
Aetiology
Polycystic ovary syndrome (PCOS) affects 5–10% of all women. It is a collection of symptoms rather than a tightly defined single disease, but is characterized by a lack of follicular maturation, lack of ovulation, and formation of follicular cysts within the ovaries. PCOS may also be associated with higher than normal levels of androgens along with excessive mild symptoms of hyperandrogenism, such as acne, hyperseborrhea, or hirsutism. Insulin resistance, diabetes, and obesity are all strongly correlated with PCOS.
Polycystic ovaries develop when the ovaries are stimulated to produce excessive amounts of androgens, through the release of excessive LH or through hyperinsulinaemia, in women whose ovaries are sensitive to this stimulus.
Diagnosis
Diagnosis remains somewhat controversial, but generally given the exclusion of other endocrine disorders, two of the following three criteria should be met:
• oligoamenorrhoea and amenorrhoea
• excess androgen activity
• the presence of polycystic ovaries determined by ultrasound (12 or more follicles between 2 and 8 mm in size)
In many cases the LH/FSH ratio as measured between days 2–5 of the menstrual cycle is increased, but this appears to be a specific subgroup of patients with hyperinsulinaemia and increased adrenal androgenic activity.
Patients with regular menstrual cycles should be reassured that they are likely to be ovulating. Mid-luteal progesterone levels should be obtained to determine whether ovulation has occurred in patients with regular menstrual cycles but over 1 year of infertility.
Treatment
• Lifestyle modifications: the therapeutic approach may vary according to the individual endocrinopathy, but lifestyle modifications are an appropriate starting point for many women. Lifestyle modifications should include:
• moderate exercise (in general this should average 30 minutes sweat-inducing exercise daily)
• a healthy diet especially in women with a BMI greater than 30 kg/m2. Weight loss reduces testosterone and increases ovulation in many obese women
• advice to stop smoking.
• Ovulation induction: Clomiphene is generally used as the first-line agent to induce ovulation in departments that can provide transvaginal ultrasound monitoring to minimize the chances of multiple pregnancy. Many patients, however, are Clomiphene resistant. Metformin may improve pregnancy and ovulation rates; however, evidence demonstrating it improves live birth rates when used alone, or in combination with Clomiphene is lacking. Second-line treatments available for Clomiphene resistant patients may include low-dose step-up FSH ovulation induction.
• Laparoscopic ovarian drilling (LOD): this involves destroying part of the ovary by diathermy or laser at the time of laparoscopy. This is normally reserved for anovulatory patients with normal BMI who are undergoing laparoscopy for other reasons. LOD has been shown to be no more effective than gonadotrophin treatment, but carries a far lower risk of multiple pregnancy. The long-term effects of LOD on ovarian function are not fully understood and the patient should be informed of this minor risk.
• Assisted reproduction: patients with PCOS who do not ovulate in response to Clomiphene or FSH can be offered in vitro fertilization (IVF). This is especially the case where another contributory factor for infertility, such as poor semen quality or tubal disease have been identified. Generally pregnancy and live birth rates of PCOS patients undergoing IVF are similar to those reported with non-PCOS patients. Obstructive and developmental disorders
Tubal occlusion
Aetiology
Intraluminal tubal occlusions may result from salpingitis, endometriosis, or peritubal adhesions. The fallopian tubes constitute a complex organ carrying out functions supporting sperm capacitation, fertilization and maintenance of the zygote rather than being merely a conduit between ovary and uterus. Pelvic inflammatory disease, genital tuberculosis, sexually transmitted disease such as chlamydia trachomatis, gonorrhoea, intrauterine contraceptive devices, adhesions or post-surgical complications may contribute to tubal occlusion. Congenital absence or incomplete development of the fallopian tubes is also rarely encountered.
Diagnosis
Patency of fallopian tubes is most commonly assessed by HyCoSy. A catheter is passed transcervically into the uterus and held in place by a balloon before the introduction of echo contrast media, injected transcervically into the uterus, enabling the visualization of tubal patency and anatomical abnormality by ultrasound.
Another approach to the assessment of tubal patency is hysterosalpingogram (HSG). This is essentially similar to HyCoSy except a radio-contrast dye is used and visualized by X-ray. Contraindications for both techniques include, possibility of pregnancy, PID, endometriosis, urogenital infection, or recent curettage.
Laparoscopy of the pelvic cavity under general anaesthetic may be indicated in women with a history of endometriosis, PID, adhesions, or ectopic pregnancy. A methylene blue dye may also be injected transcervically during the procedure to determine tubal patency. In general, flushing the fallopian tubes with dye, ultrasound or X-ray contrast media may also have a therapeutic benefit by removing tubal occlusions.
Hysteroscopy, involving transcervical visualization of the uterine cavity by endoscopy is sometimes employed to detect intrauterine lesions such as polyps and fibroids.
Treatment
• Selective salpingography: selective salpingography in which a catheter containing a fine guidewire is passed transcervically into the fallopian tube under X-ray guidance may be considered. The procedure is similar to HSG but the fallopian tube is flushed using contrast medium that has been diluted to allow visualization of the catheter and guidewire in the uterine cavity. If a proximal fallopian tube obstruction is encountered recanalization and intratubal injection of contrast media may be attempted. This latter technique may distinguish between a tubal spasm and debris or mucal mucous plug.
• Hysteroscopic tubal cannulation: this provides a further option. It entails passing a fine guidewire through a hysteroscope introduced transcervically directly into the fallopian tube, removing any minor obstruction.
• Assisted reproductive techniques: if attempts to unblock the fallopian tubes are unsuccessful, assisted reproductive techniques such as IVF are preferred. It is likely that the presence of inflammation or hydrosalpinx is detrimental to implantation. Performing a surgical intervention such as salpingectomy, tubal occlusion, aspiration of the hydrosalpinx fluid, or salpingostomy prior to the IVF procedure in women with hydrosalpinges is thought to improve the likelihood of successful outcome.
Adhesions
Aetiology
Adhesion development occurs when damage to peritoneal surfaces induces a series of cellular and molecular tissue repair cascades, involving the fibrinolytic, immunological, and proliferative systems resulting in adhesion development. Sources of damage include, operative trauma, infection, endometriosis, PID, and allergic reaction. Adhesions may constrict or occlude fallopian tubes or the uterine cavity and are a relatively common cause of infertility.
Diagnosis
Diagnosis by pelvic ultrasound, hysteroscopy, or laparoscopy. Where adhesions occlude fallopian tubes HSG or HyCoSy may be used for diagnosis. Biopsies may be obtained for histological staging and grading.
Treatment
Hysteroscopic or laparoscopic adhesiolysis: adhesiolysis is the removal of intrauterine adhesions surgically under hysteroscopic guidance or laparoscopically depending upon extent and location.
Endometriosis
Aetiology
Ectopic endometrial tissue may form deposits attached to organs in the abdominal cavity, including the ovaries or fallopian tubes. These lesions could be sites of inflammation or obstruction, thereby impeding transport of the ovum or implantation of the zygote.
Diagnosis
Endometriosis is often asymptomatic, even in some cases where fertility is impaired. Where symptoms occur they are most commonly pelvic pain just before or during menstruation. The intensity and duration of pain can vary widely and may depend on the precise anatomic location and stage or grade of the lesions. The only certain way to establish a diagnosis for endometriosis is laparoscopic examination.
Treatment
• Laparoscopic surgical resection, ablation, and adhesiolysis: medical management of endometriosis does not enhance fertility. Mild disease may sometimes be ablated during laparoscopic diagnosis. Laparoscopic surgical ablation and resection of endometriosis is carried out. Patients with ovarian endometriomas may be offered laparoscopic cystectomy.
• Assisted reproduction techniques: this is indicated for those cases where treatment fails to restore fertility.
Uterine leiomyomas (fibroids)
Aetiology
Uterine leiomyomas are benign masses arising from the myometrium and associated connective tissues. Fibroids are clinically apparent in more than one-quarter of women, although malignant disease in the form of leiomyosarcoma is rare. Fibroids may be intramural, subserous, submucous, or cervical and possess oestrogen receptors, making them responsive to oestrogen. Fibroids can impinge on fertility by distortion and obstruction of the pelvic reproductive organs, or by interfering with implantation. Obstetric problems such as early pregnancy loss, premature labour or bleeding are uncommon.
Diagnosis
Generally symptoms relate to the size and location of the masses, small fibroids are often asymptomatic. Where symptoms are present they include heavy or painful periods, abdominal discomfort or bloating, back ache, urinary frequency/retention. Large masses may be detected by manual examination, although the standard diagnostic technique is by ultrasonography.
Treatment
• Laparoscopic/hysteroscopic/open pelvic myomectomy: fibroids are generally treated by laparoscopic surgical resection. In the case of submucous leiomyomas, ablation is via hysterocopic myomectomy, in which high frequency electrical energy is used to resect the fibroid. In cases of very large fibroids, laparotomy may be the only option.
• Non-surgical treatments: uterine artery embolization (UAE) is occlusion of the uterine artery via a catheter inserted in the femoral artery under imaging guidance. Also, radiofrequency ablation is occasionally used, which is a minimally invasive treatment involving the insertion of a needle-like device into the fibroid through the abdomen and heating it with low frequency electrical currents.
An even more recent non-invasive method is magnetic resonance focused ultrasound, in which high intensity ultrasound is focused on the lesion causing a localized temperature rise (>65°C) which destroys the tissue. The focused ultrasound is guided and monitored by MRI and has the advantage over radio-techniques in that passage of ultrasound through intervening tissues has a greatly reduced negative cumulative effect.
Medical treatments with GnRH analogues or oestrogen antagonists are not indicated for the infertile patient, nor is hysterectomy, which is the definitive treatment for women not wishing to bear children.
Endometrial polyp
Aetiology
Polyps are sessile or pedunculated masses arising from the endometrium; they may be a few millimetres to several centimetres in size. Their aetiology is probably the result of oestrogen stimulation in susceptible individuals. The contribution of polyps to infertility is unclear, but large polyps may obstruct sperm or interfere with implantation or fetal growth.
Diagnosis
Hysteroscopy is the gold standard for the diagnosis of polyp. SIS is preferred to transvaginal ultrasound and HSG as minimally invasive procedures.
Treatment
• Hysteroscopic polypectomy: this is often recommended as therapy for infertility, although supporting evidence for this is unclear. Polypectomy may also be achieved by curettage.
• Assisted reproductive technology (ART): patients should be advised and educated during assisted reproductive treatment so that they have the opportunity to make informed choices regarding their treatment based on evidence as an integral part of the decision-making process. Partners should be seen together as any decisions affect both of them. Clear information regarding possible side-effects of treatment such as nausea and vomiting, headache, ectopic pregnancy, and OHSS. In addition, the possibility of multiple pregnancy carries its own risks including miscarriage, premature birth and pre-eclampsia. Current evidence suggests no increased risk of ovarian cancer in nulligravid women with a family history of ovarian cancer receiving ovulation induction.
• Intrauterine insemination (IUI): this may be considered for couples with mild male factor infertility, unexplained infertility, and mild endometriosis. The procedure is sometimes combined with ovulation induction in cases of ovarian failure.
• Semen is collected by masturbation, normally after 3 days’ sexual abstinence. Sperm are usually washed by centrifugation and the most motile fraction resuspended in a small quantity of media. Prepared sperm are transferred directly into the uterus via transcervical catheter. A variation of the technique is fallopian sperm perfusion (FSP), where the sperm preparation is injected directly into the fallopian tube.
• In natural cycles, the time of ovulation may be determined by testing for the LH surge or ultrasound monitoring. Where follicular development is stimulated by Clomifene or exogenous gonadotrophins a human chorionic gonadotrophin (hCG) trigger injection of 10 000 IU is administered subcutaneously or intramuscularly. The timing of the hCG trigger is determined by ovarian ultrasound examination and is usually given when the leading follicle reaches 16–20 mm, depending upon stimulation protocol; ovulation occurs around 36 hours later.
• Success rates depend upon the underlying pathology, but may be up to 15% per cycle. A maximum of six natural or Clomifene stimulated cycles (three gonadotrophin stimulated cycles) should be offered. If no pregnancy results IVF may be considered.
In vitro fertilization
Summary
Standard protocols entail hypothalamic/pituitary down-regulation using GnRH analogues. This is followed by gonadotrophin stimulation, leading to the development of multiple oocytes, a process monitored by ultrasound and hormone testing. The final stages of follicular maturation are triggered using human chorionic gonadotrophin and mature oocytes collected. Fertilization takes place in vitro, and embryos are cultured between 3 and 5 days before transfer of a single embryo (or two embryos) to the uterine cavity under ultrasound guidance. Luteal phase support in the form of progesterone may be offered followed by pregnancy testing.
Down-regulation
Down-regulation using GnRH agonist is administered by daily nasal inhalation or injection, beginning during the luteal phase and continuing for approximately 1 week. Baseline ultrasound scan is then performed to confirm the absence of developing ovarian follicles and thin endometrium.
Ovarian stimulation
The administration of gonadotrophins (primarily FSH) then begins, coincident with a reduction in GnRH agonist. Human menopausal or recombinant gonadotrophins are available, but existing evidence does not favour one or another preparation overall. In general, higher doses of gonadotrophins are given than for IUI cycles in order to induce superovulation. The stimulation process lasts from 10–14 days and is monitored using ultrasound to allow adjustments in daily gonadotrophin dose.
hCG trigger
The final steps of ovarian maturation are triggered using hCG by injection when the leading follicles reach approximately 16 mm in diameter as determined by ultrasound.
Oocyte retrieval
Oocyte retrieval is performed approximately 36 hours after the hCG trigger. A needle is inserted transvaginally under ultrasound guidance and each mature follicle is aspirated by suction pump, between 6 and 12 oocytes are typically collected. Fresh semen from the partner is obtained and processed as for IUI on the same day as oocyte retrieval. Alternatively, a previously cryopreserved semen sample may be used, as is the case with donated sperm.
Fertilisation and embryo culture
Oocytes and prepared motile sperm are co-incubated in fertilization media overnight under tightly controlled temperature and pH. Fertilization checks are made after approximately 18 hours, the presence of two pro-nuclei confirming fertilization. Embryos are then cultured for 2–3 days before assessment and grading. At this time, the best embryos will have reached the eight-cell stage and may be selected for transfer. The remaining embryos of suitable quality can be cryopreserved.
Blastocyst culture
Embryos can be cultured for 5–6 days until they reach the blastocyst stage before transfer. There will sometimes be some embryos that fail to develop beyond day 3, so fewer embryos are likely be available for transfer; on the other hand, any embryo that develops to blastocyst in vitro is more likely to implant and survive. The decision to proceed to blastocyst depends on various factors such as the number and quality of embryos available and the pathology and history associated with the patient. If embryo biopsy for genetic testing or aneuploidy screening is intended, then blastocyst culture is essential.
Embryo transfer
Embryo transfer is performed transcervically by catheter, normally with ultrasound guidance. A maximum of two embryos may be transferred for women under 40 years old. Those patients over 40 may elect to have three embryos transferred. Transfer of a single embryo is highly desirable due to the risk of adverse health effects of multiple births on mother and child. Cryopreserved embryos from a previous stimulation cycle may be transferred after being thawed and re-established in vitro. Luteal phase support using progesterone may be provided after transfer, followed by pregnancy testing.
Intracytoplasmic sperm injection
This is indicated for male factor infertility, such as oligospermia, asthenospermia, congenital absence of vas deferens, previous vasectomy, and surgically recovered sperm. Sperm are directly injected into the oocytes microscopically via a fine glass capillary tube in vitro. Fertilization checks and subsequent steps are then carried out as normal.
Success rates
Maternal age is the primary factor predicting success rates in ART (Table 12.13.1).
Table 12.13.1 Percentage of live births per cycle started (own oocytes): summary of UK 2006 national statistics for IVF cycles

Further reading
Agdi M, Tulandi T. Endoscopic management of uterine fibroids. Best Pract Res Clin Obstet Gynaecol 2008;22:707–16.
American College of Obstetricians and Gynecologists (ACOG). Management of infertility caused by ovulatory dysfunction. ACOG Practice Bulletin, no. 34. Washington, DC: ACOG 2002.
American College of Obstetricians and Gynecologists (ACOG). Management of infertility caused by ovulatory dysfunction. Washington, DC: ACOG 2002.
Consensus on infertility treatment related to polycystic ovarian syndrome. Human Reproduction 2008;3:462–77.
Conway GS. Premature ovarian failure. Br Med Bull 2000;56:643–9.
Farquhar C, Lilford RJ, Marjoribanks J. et al. Laparoscopic ‘drilling’ by diathermy or laser for ovulation induction in anovulatory polycystic ovary syndrome. Cochrane Database Syst Rev 2007: CD001122.
Fischbach FT. A manual of laboratory and diagnostic tests. Philadelphia: Lippincott.
Human Fertilisation and Embryology Authority (HFEA) HFEA facts and figures 2006: fertility problems and treatment. London: HFEA 2008.
Human Fertilisation and Embryology Authority (HFEA). Code of practice, 6th edn. London: HFEA 2003.
National Collaborating Centre for Women’s and Children’s Health. Fertility: assessment and treatment for people with fertility problems. Clinical guideline 11. London: NICE 2004.
Polena V, Mergui JL, Perrot N, et al. Long-term results of hysteroscopic myomectomy in 235 patients. Eur J Obstet Gynecol Reproductive Biol 2007;130:232–7.
Royal College of Obstetricians and Gynaecologists (RCOG). Long-term consequences of polycystic ovary syndrome. Guideline No.33. London: RCOG 2007.
Silberstein T, Saphier O, van Hooris BJ, Plosker SM. Endometrial polyps in reproductive age and infertile women. IMAJ 2006;8:192–5.
Steinkeler JA, Woodfield CA, Lazarus E, Hillstrom MM. Female infertility: a systematic approach to radiologic imaging and diagnosis. Radiographics. 2009;29:1353–70.
Fertility in survivors of childhood malignancy Introduction
As the diagnosis and treatment of childhood cancer becomes increasingly successful, there are growing numbers of survivors with a variety of treatment effects. One of the major issues for patients is the impact of their disease on reproductive function and the implication for the health of their offspring.
Cancer and its treatment may cause a spectrum of damage to the reproductive axis and the potential effects upon fertility are diverse and complex depending upon the interaction between many patient and treatment factors. Some patients are unaffected, whereas others face infertility immediately after treatment. For many patients, there appears to be a ‘fertile window’ and it is the difficulty in assessing an individual’s risk of subfertility that leaves many patients, their families, and clinicians uncertain about a patient’s reproductive potential.
It is the clinician’s role to identify possible strategies to prevent subfertility, diagnose it, if and when it occurs, and explore any necessary fertility treatments.
The preservation of fertility and the treatment of subfertility in survivors of childhood cancer is a growing field of research and although many techniques of fertility preservation are in their infancy, there is a lot of promising initial data. (See the box for quick reference material). Definition
As survival rates for children treated for cancer continue to improve, a growing population of women emerges for whom issues of fertility are paramount. Cancer therapy may disrupt the neuroendocrine axis, damage the ovaries, and impair uterine function, resulting in pubertal delay or arrest, premature ovarian failure (POF), subfertility, or ovarian insufficiency. Epidemiology
Childhood cancer is rare, with approximately 1400 new cases per year in the UK (SIGN 2004). With long-term survival rates approaching 73%, it is estimated that 1 in 715 of the adult population will be a survivor of childhood cancer in 2010 (SIGN 2004).
One of the major issues for patients is the impact of their disease on reproductive function and the implication for the health of their offspring.
Cancer therapy may cause a spectrum of damage to the reproductive axis, and only a minority of females will develop POF failure immediately after completion of their treatment. However, fertility may be impaired even in women who are menstruating after cancer therapy. Survivors are at high risk of permanent POF with an 8% risk before the age of 40 years, compared with about the prevalence of spontaneous conception in this group of women. However, it is well documented that the offspring of such patients have no excess of congenital anomalies or other diseases (Li et al. 1979).
Advances in assisted reproduction have made pregnancy a possibility in women without ovarian function, providing there is normal uterine function. There are few data to provide an accurate prevalence of successful pregnancy with assisted reproduction. Most studies are however reassuring about reproductive outcome after chemotherapy alone. Successful pregnancy, with no excess risk of miscarriage, and healthy offspring are reported following multi-agent chemotherapy (Lee et al. 2006).
Pregnancy in all cancer survivors should be considered high risk, as pregnancy in this group is associated with an increased risk of adverse outcomes, particularly in patients with uterine dysfunction secondary to radiotherapy. Although study numbers are small, there appears to be an increased incidence of miscarriage, preterm delivery, and low birthweight neonates in women who have received radiotherapy (Lee et al. 2006). Increasing risk of preterm birth is associated with increasing radiotherapy doses (Lee et al. 2006). Low birthweight and prematurity are likely to be related to reduced elasticity of the uterine musculature with subsequent restriction of the uterine expansion required in pregnancy. Increased risk of abnormal placentation in the irradiated uterus has also been documented. Clinical approach
Considerations prior to treatment
The potential effects of cancer therapies on fertility should first be considered at the time of diagnosis. Pubertal status should be assessed and the risk of infertility estimated. Baseline tests should be completed after consideration of the potential short- and long-term effects of the cancer’s clinical course, its treatment and potential complications. If infertility is estimated to be a risk, then referral to a specialist assisted reproductive unit should be considered.
• Modern radiotherapy planning methods can be used to calculate the planned dose of radiotherapy to the ovaries. Depending on the clinical scenario the treatment can be planned to selectively avoid one ovary or modified to minimize the dose of radiation received by each ovary (Wallace et al. 2005a).
Following treatment
Girls treated for cancer should have their pubertal status and growth patterns assessed three times a year following treatment (SIGN 2004). If these parameters are below that expected for age, referral should be made. Ovarian function should be assessed using biochemical analysis of gonadotrophins and sex steroids, a menstrual history, and ultrasound examination of the uterus and ovaries. Recently anti-Müllerian hormone and inhibin B have been shown to be potential markers of ovarian reserve. Biochemical assessment before puberty is unreliable. Raised concentrations of follicle-stimulating hormone (FSH) in the early follicular phase are often seen in women who have impaired fertility, despite healthy ovulatory cycles. Results must be interpreted with care.
Primary or secondary amenorrhoea, infertility, or oestrogen-deficient symptoms should prompt investigation for POF. An elevated FSH and LH with low oestradiol, on two separate occasions is diagnostic of POF. Prolactin, thyroid function tests and an autoantibody screen should be completed to exclude other causes. Pelvic imaging is not required for diagnosis but uterine and ovarian dimensions should be measured and the endometrial thickness noted. Ultrasonic assessment of ovarian volume may be a potential predictor of reproductive potential, with volume correlating with the number of remaining follicles. In the event of a diagnosis of POF, a bone mineral density scan should be requested.
Management
All women with POF should be offered sex steroid replacement therapy to protect cardiovascular and skeletal health. This is currently offered in the convenient form of the combined OCP or HRT formulations designed for postmenopausal women. Further research is required to demonstrate the optimum formulation and dose of sex steroids that should be recommended for these younger women.
Fertility preservation
There is great awareness of the adverse effects of cancer therapy on fertility but fertility preservation techniques for children and young women remain investigational. At present, there are only two established practices of fertility preservation in female patients which are oophoropexy and cryopreservation of embryos after in vitro fertilization (Wallace et al. 2005b). Oophoropexy (surgically displacing the ovaries out of the radiation field) may preserve ovarian function but radiation-induced uterine damage may still affect the chances of successful pregnancy. Cryopreservation of embryos is only suitable for sexually mature women with a partner. Mature oocyte preservation is a potential solution for women without a partner but pregnancy rates are significantly lower as these cells sustain more damage during the freeze–thaw process than embryos (Oktay et al. 2006) Significant delays in cancer treatments may be sustained, as these techniques require ovarian stimulation with oocyte retrieval. These procedures are not without risk and the number of embryos or oocytes is also limited.
For prepubertal girls, or women without a partner, cortical ovarian tissue may be removed laparoscopically without delaying treatment, and reimplanted following successful cancer treatment (Donnez et al. 2006). There is concern, however, that this tissue may contain malignant cells capable of inducing relapse on reimplantation. Reports of embryo development following heterotopic transplantation of cryopreserved tissue and of six live births after orthotopic transplantation of cryopreserved tissue provide potential therapies for the future (Donnez et al. 2006).
Another approach to preserve fertility is the administration of a gonadotrophin-releasing hormone (GnRH) agonist. Provisional studies have demonstrated a lower rate of POF in patients treated with GnRH agonists prior to cancer treatment (53%). They may prolong the ‘fertility window’ but the beneficial effects are age related.
Informed consent is required for these experimental and invasive techniques and this is challenging in young people. In the UK if the patient is less than 16 years old they must be Gillick competent if they are to make their own informed decisions. The child must demonstrate to have sufficient intelligence to understand what has been proposed.
Many women who had already undergone cancer treatment and now face infertility did not have such technologies available to them. For these women, donor oocytes are the only available option at present. Uterine function is still important and success rates may be reduced in women with radiation-induced uterine damage.
Quick reference material
Cancer therapy may result in a range of disturbances to the neuroendocrine axis and may damage the ovaries and impair uterine function, resulting in diverse effects upon reproductive function
The prevalence of POF is dependent upon the treatment given, the agent used, the dose and age of patient when treatment is administered
Spontaneous ovulation and conception may occur Offspring of cancer patients have no excess of congenital anomalies or other diseases
Reproductive outcome after chemotherapy alone is good
There is an increased incidence of miscarriage, preterm delivery, and low birthweight neonates in women treated with radiotherapy
Pregnancy in all cancer survivors should be considered high risk
Fertility preservation should be considered prior to cancer treatment
Following treatment pubertal status and growth patterns should be assessed three times a year
All women with POF should be offered sex steroid replacement therapy
Fertility preservation techniques for children and young women remain investigational
Oophoropexy (surgically displacing the ovaries out of the radiation field) may preserve ovarian function
Cryopreservation of embryos after in vitro fertilization is an established practice for fertility preservation but is limited by the age of the patient and the need for a partner
Mature oocyte preservation, cortical ovarian tissue cryopreservation, and the administration of GnRH agonists are potential solutions for fertility preservation in younger women or those without partners at the time of treatment
The only established option for preservation of male fertility is cryopreservation of spermatozoa
The possibility of germ cell transplantation offers hope to restoring fertility in the prepubertal male
There are a wide variety of potentially serious and disabling comorbidities that are recognized in the survivors of childhood cancers and careful follow-up and monitoring should therefore be arranged
Counselling
Counselling for the patient and their family should be offered to all patients and detailed discussion with a specialist regarding the potential effects on fertility and fertility preservation techniques should be available.
Treatment of childhood cancer can have an impact on neurological, educational, and social function (SIGN 2004). Survivors are at increased risk of cognitive impairment as well as a range of psychological symptoms, including low mood and anxiety. Such problems should be reviewed at routine follow-up. Comorbidity
In the context of management of childhood cancer survivors it is important to recognize comorbidities may exist.
Growth problems
A number of factors are responsible for impaired growth following childhood cancer. These include the disease process itself, complications of treatment (infection), direct effects during treatment (anorexia), and late effects attributable to therapy (SIGN 2004). Localized tumour treatment may affect growth of individual bones and sex steroid deficiencies may have secondary effects on growth and pubertal development (SIGN 2004).
All children should have their height, weight, BMI, and bone age measured regularly until they reach final adult height.
Dental problems
Children undergoing cancer treatment should be advised about the possible effects on orofacial and dental development. Disturbances in mineralization, the development of crowns and roots of teeth are commonly seen (SIGN 2004). Facial asymmetry has also been observed after local radiotherapy.
Cardiac problems
Anthracyclines, as well as radiotherapy to the chest, are risk factors for cardiovascular disease and monitoring using echocardiography, is therefore necessary (SIGN 2004). Mediastinal irradiation increases the incidence of coronary artery disease and myocardial infarction. The risk increases with increasing doses.
Cardiac function should be monitored during pregnancy as the hyperdynamic circulation of pregnancy may precipitate cardiac failure.
Secondary cancers
The leading cause of death among 5-year survivors is recurrence of the original cancer with a significant excess mortality rate seen due to subsequent malignancies. Breast cancer risk increases with increasing radiation dose of supradiaphragmatic radiotherapy. The risk is greater for those women treated at a younger age.
Thyroid dysfunction
Thyroid dysfunction may be due to primary damage to the gland or secondary to damage to the hypothalamic-pituitary axis. Chemotherapy is an independent risk factor for thyroid dysfunction and thyroid function tests should be checked, following treatment and annually thereafter. Follow-up
All survivors of childhood cancer should ideally be followed up for life by a multidisciplinary team. A designated key worker should coordinate care. It is essential that all professionals involved are aware of the diagnosis and treatment received to allow vigilant observation for late effects. Male patients
The testes are also susceptible to cytotoxic cancer treatments with the extent of damage being dependent upon the agent used and its dose. Not all damage is permanent and a proportion of men achieve parenthood spontaneously.
Radiotherapy
The degree and duration of radiotherapy-induced testicular damage depends on the field of treatment, total dose and fractionation schedule (Howell and Shalet 1998). Radiation doses as low as 0.1–1.2 Gy can impair spermatogenesis, with doses of more than 4 Gy causing permanent damage (Howell and Shalet 1998).
Chemotherapy
The effects on fertility of chemotherapies are dependent upon the drug, the dose and the age of the patient.
Fertility preservation
The only established option for preservation of male fertility is cryopreservation of spermatozoa. This is dependent on the ability of the patient to produce a specimen. Alternative invasive sperm retrieval methods may be used in boys with testes >10 mL volume who are unable to produce a sample.
Although there may be impaired spermatogenesis following cancer treatment spontaneously conceived off-spring have no excess of congenital anomalies or other disease (Li et al. 1979). Modern assisted conception techniques such as intracytoplasmic sperm injection (ICSI) have allowed many men with poor semen quality to achieve parenthood.
Hormone suppression has not been shown to help reduce chemotherapy-induced testicular damage. The possibility of germ cell transplantation offers hope to restoring fertility in the prepubertal male, although techniques remain investigational. Further reading
Critchley HO, Wallace WH. Impact of cancer treatment on uterine function. J Natl Cancer Inst Monogr 2005;34:64–8.
Donnez J, Martinez-Madrid B, Jadoul P, et al. ovarian tissue cryop-reservation and transplantation: a review. Hum Reprod Update. 2006;12:519–35.
Howell S, Shalet SM. Gonadal damage from chemotherapy and radiotherapy. Endocrinol Metabol Clin N Am 1998 27: 927–43.
Lee SJ, Schover LR, Partridge AH, et al. American Society of Clinical Oncology. American Society of Clinical Oncology recommendations on fertility preservation in cancer patients. J Clin Oncol 2006;24:2917–31.
Li PP, Fine W, Jaffe N, et al. Offspring of patients treated for cancer in childhood. J Natl Cancer Inst 1979;62:1193–7.
Mertens AC, Yasui Y, Neglia JP, et al. Late mortality experience in five-year survivors of childhood and adolescent cancer: The Childhood Cancer Survivor Study. J Clin Oncol 2002;19:3163–72.
Multidisciplinary Working Group convened by the British Fertility Society. A strategy for fertility services of childhood cancer. Hum Fertil Camb 2003; 6: A1–A40.
Oktay K, Cil P, Bang H. Efficiency of oocyte cryopreservation: a meta-analysis. Fertil Steril 2006;86:70–80.
Scottish Intercollegiate Guidelines Network (SIGN). Longer follow-up of survivors of childhood cancer: a national clinical guideline. SIGN 2004; 76.
Sklar CA, Mertens AC, Mitby P, et al. Premature menopause in survivors of childhood cancer: a report from the Childhood Cancer Survivors Study. J Natl Cancer Survivor Study 2006;98:890–6.
Thomson AB, Critchley HO, Kelnar CJ, et al. Late reproductive sequelae following treatment of childhood cancer and options for fertility preservation. Best Pract Res Clin Endocrinol Metab 2002;16:311–34.
Wallace WH, Thomson AB, Kelsey TW. The radiosensitivity of the human oocyte. Hum Reprod 2003;18:117–21.
Wallace WH, Thomson AB, Saran F, et al. Predicting age of ovarian failure after radiation to a field that includes the ovaries. Int J Radiat Oncol Biol Phys 2005a; 62: 738–44.
Wallace WHB, Anderson RA, Irvine DS. Fertility preservation for young patients with cancer: who is at risk and what can be offered? Lancet Oncol 2005b; 6: 209–18. Patient resources
Teenage Cancer Trust: www.teencancer.org
The United Kingdom Children’s Cancer Study Group: www.ukccsg.org
Macmillan Cancerline: www.macmillan.org.uk
Imaging in reproductive medicine Ultrasound
Ultrasound (US), transvaginal ±transabdominal, is the primary imaging modality in reproductive medicine. Diagnostic pelvic ultrasound is part of the initial assessment of patients presenting with subfertility or recurrent miscarriage and aims to
• assess ovarian morphology
• exclude significant congenital uterine anomalies
• exclude potentially associated gynaecological disease such as endometriosis and fibroids.
Further indications for US in patients undergoing treatment for subfertility include
• monitoring ovarian response and follicular growth during ovulation induction
• assessment of endometrial response during ovulation induction
• assisting with egg collection and subsequent embryo transfer
• guiding percutaneous/transvaginal aspiration of cysts which might interfere with follicle monitoring and/or egg collection
• prevention/monitoring of ovarian hyperstimulation syndrome (OHSS). OHSS is accompanied by large ovaries (up to 10 cm) containing multiple follicles and associated with ascites and pleural effusions.
Ovarian morphology
Transvaginal ±transabdominal US should be able to identify at least one ovary in over 95% of premenopausal women. Ovaries are typically oval hypoechoic masses related to the iliac vessels and contain a variable number of small cysts/follicles. Follicular growth, ovulation, and development of the corpus luteum can be monitored.
Three main types of anovulatory ovaries can be distinguished on US:
• Polycystic ovaries (PCOs): the definition of a PCO has been under debate for some time. According to a recent consensus statement a PCO is defined as an ovary with a volume of >10 mL and/or >12 cyst/follicles measuring 2–9 mm (Balen et al. 2003).
• Hypothalamic hypogonadotrophism: in contrast, hypothalamic hypogonadotrophic ovaries, typically associated with amenorrhoea due to weight loss, in athletes, or stress are small/normal in size and contain a small number of follicles, similar to adolescent, prepubertal ovaries.
• Premature ovarian failure: the ovaries are small and quiescent with no evidence of follicular activity. However, this diagnosis requires biochemical confirmation.
Congenital uterine anomalies
The ability to differentiate endometrium from myometrium allows an experienced operator to diagnose many congenital uterine abnormalities using conventional 2D ultrasound. However, it is not always possible to obtain good coronal views of the uterus, and hence differentiating arcuate from mildly subseptate uteri and subseptate from bicornuate uteri (by indentifying a fundal notch) can be difficult. 3D ultrasound overcomes this problem and has been shown to be an accurate and reproducible technique for classifiying congenital uterine anomalies (Jurcovic 1995).
Associated gynaecological disease
Endometriosis/adenomyosis
US has poor sensitivity for deep pelvic endometriosis but is able to see significant endometriomas. Typically endometriomas are cysts containing diffuse internal echoes. However, they vary in appearance from apparently simple cysts to complex multilocculated masses containing varying amounts of internal echoes with thick internal septations and irregular walls, features which can be difficult to differentiate from malignant ovarian masses. Endometriosis involving the bowel is indicated by areas of low echogenicity and irregularly thickened bowel wall.
US has an approx 80% sensitivity for the diagnosis of adenomyosis (Dijkman et al. 2000). Features include areas of heterogeneity in the myometrium, subendometrial echogenic linear striations, small myometrial cysts, and displacement of the cavity.
Pelvic inflammatory disease
US also has a low sensitivity for pelvic inflammatory disease and cannot be used to exclude tubal occlusion. Hydrosalpinges may be visualized as elongated, frequently tortuous, cystic masses, with or without incomplete septations due to residual mucosal folds but are not always detectable. The ovary maybe visible abutting the cyst or may be involved in a complex tubo ovarian mass.
Fibroids
Fibroids are perhaps the most common abnormality seen on pelvic ultrasound but their significance in patients with subfertility or recurrent miscarriage is difficult to determine. US is able to determine the approximate number, size, and location of fibroids but more importantly it can describe the relationship of the fibroids to the cavity. Hystero contrast salpingography (HyCoSy)
HyCoSy involves cannulating the cervix and injecting an US contrast agent (e.g. Echovist or Sonovue) into the uterus while performing a transvaginal US. It is an alternative investigation to hysterosalpingography and has a similar sensitivity for the diagnosis of tubal patency (Dijkman et al. 2000). Some operators have also used saline rather than contrast. It has proved helpful when assessing the cavity for polyps and fibroids but is less accurate when assessing tubal patency. Hystero salpingography (HSG)
Hystero salpingography (HSG) is the transcervical injection of radiographic contrast under fluoroscopic guidance and has been used for many years for the assessment of tubal patency and the shape of the uterine cavity. It is performed in the first half of the menstrual cycle, after bleeding has ceased. Complications of the procedure include
• pain (particularly if the tubes are shown to be occluded)
• infection (nowadays most units recommend routine antibiotic prophylaxis)
• vasovagal reaction due to manipulation of the cervix
• contrast allergy (very rare)
In comparison with the ‘gold standard’ of laparoscopy and dye insufflation, HSG has been shown to be accurate in the detection of tubal patency but is less accurate in the detection of tubal occlusion and peritubal disease. However, the fact that it does not require any anaesthetic and is well tolerated by most women means it should be the initial investigation for patients with no suspicion of tubal disease (RCOG 2004). Congenital anomalies, filling defects in the cavity due to fibroids, polyps, or adhesions are well demonstrated and the site of tubal occlusion can be seen. The absence of mucosal folds in the distended ampulla of a hydrosalpinx suggests a poor prognosis following salpingostomy. Multiple tiny contrast-filled diverticula along the isthmic portions of the tubes indicate salpingitis isthmica nodosa, which is usually caused by endometriosis or pelvic inflammatory disease and associated with an increased incidence of subfertility and ectopic pregnancy.
Selective salpingography and tubal recanalization/fallopian tube catheterization
Catheterization of the tubes has a diagnostic and therapeutic role. Simple catheterization of the cornua immediately following a conventional HSG can be used to confirm or refute tubal occlusion particularly where doubt is caused by reflux of contrast through the cervix or preferential filling of the contralateral tube. Indeed, one study showed selective tubal catheterization to be superior to laparoscopy and dye insufflation in the diagnosis of proximal tubal occlusion.
Approximately 50% of apparent cornual occlusions are due to spasm or debris and minor adhesions, and these can be cleared by either injecting contrast directly into the tube or by probing with a guidewire. Under fluoroscopic guidance, following a standard HSG, preformed catheters are used to cannulate the cornua and contrast injected. If the tube is not demonstrated a guidewire is advanced into the tube and any obstruction cleared using gentle probing movements. Subsequent injection of contrast is then used to confirm patency. Studies have shown that approximately 70% of occluded tubes can be opened in this way with a resulting pregnancy rate of 10–20%. Complications of the procedure include tubal perforation (1–10%) and tubal pregnancy (0.4–8%) but it should be noted that patients requiring the procedure are likely to have an increased risk of ectopic pregnancy even in the absence of tubal catheterization by virtue of their pre-existing tubal disease. The procedure has been approved by the National Institute for Clinical Excellence (NICE) and is recommended by the Royal College of Obstetricians and Gynaecologists for use in patients with proximal tubal occlusion (NICE 2004; RCOG 2004). Magnetic resonance imaging
Congenital anomalies
Congenital Mullerian duct abnormalities are frequently suggested by US or HSG but accurate classification can prove difficult. Magnetic resonance imaging (MRI) has been shown to be more accurate than both these techniques and should be considered before laparoscopy/hysteroscopy if there is any doubt about the precise nature of an abnormality (Troiano and McCarthy 2004).
Associated gynaecological disease
MRI is the most accurate imaging technique for diagnosing adenomyosis. Features include widening of the so-called junctional zone (superficial layer of myometrium), high-intensity spots, asymmetrical thickening of the myometrium, and poorly defined low signal myometrial masses. Adenomyomas can be differentiated from fibroids, which is of considerable importance therapeutically.
Endometriomas are easily seen with MRI scans, which is also the most reliable technique for assessing deep pelvic endometriosis. Adhesions between the cervix, uterus and bowel are demonstrated as low signal bands causing distortion; thickening of the uterosacral ligaments is visible and rectovaginal nodules can be seen.
There are no specific features of pelvic inflammatory disease on MRI scans but the multiplanar imaging facility means that hydro- or haematosalpinges can be distinguished from other complex adnexal masses.
MRI is also of value in the management of fibroids. It can delineate the number, location, and size of fibroids and assess their vascularity and relation to overlying bowel and abdominal wall scars, important factors when considering MR-guided ablation with focused US or fibroid embolization. Focused US is only appropriate if there are less than six fibroids with diameters of 6 months)
• Oligomenorrhoea (cycle >42 days)
• Irregular menses (e.g. cycles varying between 2 and 6 weeks in duration). Causes
The commonest cause of anovulation is polycystic ovary syndrome (PCOS) (80%). Other endocrine disorders that commonly cause anovulation are hyperprolactinaemia, isolated gonadotropin-releasing hormone (GnRH) deficiency or GnRH dysfunction secondary to weight loss or exercise.
Many other endocrine disorders are rare causes of anovulation but commonly present with menstrual abnormalities.
Endocrine disorders associated with ovulatory dysfunction
Polycystic ovary syndrome
Hypothalamic-pituitary disease
GnRH deficiency isolated or identified cause
prolactinoma
acromegaly
Cushing’s
non-functioning tumours
Sheehan’s syndrome
Adrenal disease
CAH
virilizing tumours
Addison’s disease
Thyroid disease
hypothyroidism
hyperthyroidism Investigation of anovulation
A small number of investigations are necessary (see box)
• FSH, LH (normal range 3–11 u/L)
• Prolactin (50–500 mu/L)
• TSH (0.5–5.0 mu/L)
• Pelvic ultrasonography to assess ovarian morphology
• Testosterone (0.5–3.0 nmol/L)
• Assessment of oestrogen status (if amenorrhoeic, patients with oligomenorrhoea have adequate endogenous E2 production)
• Serum oestradiol 30 a 5–10 kg weight loss is associated with a significant improvement in androgen and insulin levels and improved chance of response to clomiphene.
Alternative treatment options
Alternatives should be considered for patients resistant to clomiphene or who have not conceived after nine cycles of clomiphene.

Fig. 12.16.1 Cumulative conception with clomiphene citrate.
Human menopausal gonadotrophin
Gonadotrophins LH and FSH extracted from urine, purified and reconstituted for daily injection. There are various degrees of purity with human menopausal gonadotrophin (hMG). The standard ampoule contains 75 IU FSH but the LH dose varies from 75 IU to additional steps to remove urinary proteins are undertaken during manufacture. Gonadotrophins are also available as recombinant LH and FSH that have no urinary contaminants.
Ovulation induction trials have shown no difference in clinical outcome comparing urinary or recombinant preparations.
Initial hMG protocols were associated with high (20%) rates of multiple pregnancy and OHSS.
Low-dose protocol for gonadotrophin therapy
Daily dose of gonadotrophin with step-up protocol aiming to find the threshold dose that is maintained to develop a single dominant follicle. Once the dominant follicle has reached the appropriate size, ovulation is triggered with 5000 IU of hCG; no luteal phase support is given and a midluteal phase progesterone is taken to confirm ovulation. With this protocol, 86% of completed ovulatory cycles are unifollicular. However, 15% of cycles are abandoned due to multiple follicular development. After six cycles of treatment there is cumulative conception >50%, a miscarriage rate of 20%, and a multiple pregnancy rate (all twins) are no sperm present in the ejaculate (azoospermia) due to obstruction in the genital tract, sperm can be surgically retrieved from the testis or epididymis. It has also been reported that sperm can be obtained when the primary problem is with the germinal epithelium: Sertoli cell only, maturation arrest, Kleinfelter’s syndrome, etc. (Palermo et al. 1998; Ramasamy et al. 2005). The numbers of sperm retrieved are, however, low and such sperm have virtually no endogenous motility and, therefore, no hope of spontaneously fertilizing an oocyte. ICSI bypasses the natural barriers to penetration and allows the nuclear DNA of that sperm access to that of the oocyte, thus permitting fertilization to occur.
ICSI is also indicated in less common procedures such as pre-implantation genetic diagnosis (PGDs) in order to decrease the chances of DNA contamination from other sperm in the molecular PCR-based laboratory techniques employed.
Counselling
As ICSI is an adjunct to IVF treatment, counselling should initially include all of the risks of IVF, such as hyperstimulation syndrome and multiple pregnancy. In addition, however, it is necessary to discuss the risks of fertility problems in any subsequent offspring and the increased rate of fetal abnormality (albeit small), in particular of the genital tract. Where OAT is profound (or = 32 weeks’ gestation) and a spontaneously conceived comparison group. Hum Reprod 2007;22:506–15.
Bhasin S. Approach to the infertile man. J Clin Endocrinol Metab 2007;92:1995–2004.
Bhattacharya S, Hamilton MP, Shaaban M, et al. Conventional invitro fertilisation versus intracytoplasmic sperm injection for the treatment of non-male-factor infertility: a randomised controlled trial. Lancet 2001;357:2075–9.
Bonduelle M, Wennerholm UB, Loft A, et al. A multicentre cohort study of the physical health of 5-year-old children conceived after intracytoplasmic sperm injection, in vitro fertilization and natural conception. Hum Reprod 2005;20:413–319.
ESHRE Capri Workshop Group. Intracytoplasmic sperm injection (ICSI) in 2006: evidence and evolution. Hum Reprod Update 2007;13:515–26.
Human Fertilisation and Embryology Authority (HFEA). A long term analysis of the HFEA Register data 1991-2006. London: HFEA 2007.
Human Fertilisation and Embryology Authority (HFEA). Facts and figures 2006 fertility problems and treatment. London: HFEA 2008.
Kinzer DR, Barrett CB, Powers RD. Prognosis for clinical pregnancy and delivery after total fertilization failure during conventional in vitro fertilization or intracytoplasmic sperm injection. Fertil Steril 2005;90:284–8.
Myers ER, McCrory DC, Mills AA, et al. Effectiveness of assisted reproductive technology (ART). Evid Rep Technol Assess (Full Rep) 2008;167:1–195.
Neri QV, Takeuchi T, Palermo GD. An update of assisted reproductive technologies results in the United States. Ann N Y Acad Sci 2008;1127:41–8.
Palermo G, Joris H, Devroey P, VanSteirteghem AC. Pregnancies after intracytoplasmic injection of single spermatozoon into and oocyte. Lancet 1992;340:17–18.
Palermo GD, Schlegel PN, Sills ES, et al. Births after intracytoplasmic injection of sperm obtained by testicular extraction from men with nonmosaic Klinefelter’s syndrome. N Engl J Med 1998;338:588–90.
Practice Committee of the American Society for Reproductive Medicine. Report on management of obstructive azoospermia. Fertil Steril 2006: 86: 259–63.
Ramasamy R, Yagan N, Schlegel PN. Structural and functional changes to the testis after conventional versus microdissection testicular sperm extraction. Urology 2005;65:1190–4.
Sarkar NN. Intracytoplasmic sperm injection: an assisted reproductive technique and its outcome to overcome infertility. Obstet Gynaecol 2007;27:347–53. Internet resources
www.hfea.gov.uk/
www.asrm.org/Patients/topics/icsi.html
www.britishfertilitysociety.org.uk/public/factsheets/docs/BFS-risks%20and%20complications%20of%20assisted%20conception%20.pdf Patient resources
www.fertilityconnect.com/index.htm
http://en.wikipedia.org/wiki/Intracytoplasmic_sperm_injection
www.ivf.net/ivf/icsi_intracytoplasmic_sperm_injection-o2109.html
www.infertilitynetworkuk.com/
www.britishfertilitysociety.org.uk/public/index.html
Intrauterine devices Definition
The intrauterine device (IUD) is a flexible rod or filament inserted into the uterus to prevent conception. Modern IUDs are medicated to enhance their contraceptive efficacy. Copper-releasing ones are referred to as IUDs or intrauterine contraceptives (IUCs) and the progestin-releasing ones are called intrauterine systems (IUS). For the purpose of this chapter all such devices will be referred to as IUD. Epidemiology
It is estimated that about 160 million people worldwide use the IUD for contraception. In China 50% of married women who practice contraception use the IUD compared with 4% in Britain and 2% in America. Despite the variations in its usage worldwide, it remains one of the most cost-effective and reversible methods of contraception and is underused in the developed world.
The first IUD was invented and marketed by Ernst Grafenberg, a Jewish German opthalmologist turned gynaecologist in 1928. Since then the IUD has been redesigned many a time to the ones that are presently available. Pathology
The IUD has certain characteristics that serve to fulfil its designed purpose. However, these can lead to complications if improperly chosen or handled.
In view of these factors, it is hardly surprising that IUDs have been credited with a number of ill effects and therefore are underutilized. Mode of action
All IUDs work by preventing fertilization. A sterile inflammatory reaction occurs within the uterus, and this in turn leads to inhibition of sperm motility, reduced sperm capacitation and survival, and sperm phagocytosis.
Fig. 12.18.1 Copper and progestin-releasing intrauterine devices. See also colour plate section.

In addition, the copper within the copper IUDs enhance a cytotoxic inflammatory reaction.
The progestins in progestin-releasing IUDs thicken the cervical mucus, which prevents sperm penetration into the uterine cavity. In addition, the decidualization and glandular atrophy caused in the endometrium prevents implantation of the blastocyst. Shape
The framed devices are in the shape of a T, which helps conform to the shape of the uterus. This then retains the device in utero. There is a thread/threads attached to the end that projects through the cervix when the device is in utero. The presence of the thread rules out expulsion and also aids removal of the device.
The frameless device has six copper sleeves threaded on a prolene filament with a knot at one end. It is this end that is pushed into the myometrium with an introducer and helps secure it to the tissues there. The advantage of a frameless device is that it can be inserted into cavities that are distorted and unable to retain a framed device. Similarly, they are also useful in an enlarged, puerperal uterus or in a small one. Medicated devices
Medicated devices enhance efficacy, such as copper in the copper IUDs and progestin in the progestin-releasing IUDs. The currently available copper coils have sleeves of copper on the horizontal arm, thereby increasing the available surface area of copper. This results in a much more efficient device that not only provides contraception for longer but also has a greatly reduced failure rate. Aetiology
The modern IUD is a very effective, long-acting, safe, and easily reversible method of contraception. It has few side-effects, rarely interferes with the spontaneity of sex and offers women the privacy they seek. The types of IUD in use include the following (see also Fig. 12.18.1):
• copper IUDs
• framed devices
• copper sleeves
• TCu380S
• TT380 Slimline
• TCu380A Quickload
• MiniTT 380 Slimline
• Flexi-T 380
• copper in stem only
• Multioad 375
• UT 380
• UT 380 Short
• NovaT380
• Flexi-T380
• frameless devices
• GyneFix
• progestin-releasing IUDs (also known as IUS)
• framed device
• Mirena
• Unmedicated (inert) IUDs
• Lippes loop
• Stainless steel flexible ring Efficacy
Copper IUDs with 380 mm2 of copper or more have a failure rate of less than 1 per 100 woman years, which is no different to the progestin-releasing IUDs. Duration of use
The second-generation copper IUDs are known to provide efficacy for up to 10 years following insertion. If inserted after the age of 40 they can be left in place until the menopause. Frameless copper IUDs and the shorter versions of copper IUDs, such as the mini TT380A, are efficient for up to 5 years
The progestin-releasing IUDs provide contraception as well as relief from menorrhagia for 5 years. However, when used to limit endometrial proliferation as in hormone replacement therapy combinations the efficacy does not last beyond 4 years. If used for contraceptive purpose and inserted beyond the age of 45 they may be retained until the menopause. Indications for intrauterine devices
• Most women regardless of age and parity.
• Those at low risk of acquiring sexually transmitted infections that may necessitate removal.
• Those seeking an easily reversible and effective agent.
• The copper IUD is a very effective emergency contraceptive agent. The progestin-releasing IUD cannot be used for this purpose. Contraindications for intrauterine devices
• Uterine distortion such as bicornuate uterus
• Active pelvic infection
• Suspected pregnancy
• Wilson’s disease or allergy to copper
• Unexplained uterine bleeding
• Current breast cancer: avoid progestin-releasing devices
• Active liver disease: avoid progestin-releasing devices. Prognosis
Perforation
The rate of perforation associated with intrauterine device usage is low (0–2.3 per 1000 insertions). No major difference was noted in the incidence of perforation between the various types available. Expulsion
About 5% of women expel IUDs and this occurs usually after within the first 3 months of insertion and more commonly during a period. The chance of expulsion is not affected to a great extent by the type of IUD inserted; however, recent studies have suggested that the risk may be increased with frameless IUDs. Risk of ectopic pregnancy
IUDs are so effective that the absolute risk of pregnancy (intrauterine or ectopic) is very low. A previous ectopic pregnancy is no longer a contraindication to the use of these devices and the overall risk is reduced compared to women using no contraception. In fact, IUD has been shown to lower the incidence of ectopic pregnancies when compared to no contraception. Return to fertility
IUDs have not been shown to delay a return to fertility. The mean time taken to fall pregnant following removal of either a copper or a progestin-releasing device was 3 months. Pelvic inflammatory disease
Development of pelvic inflammatory disease (PID) is most strongly related to the background risk of sexually transmitted infections (STIs) and the insertion procedure rather than the IUD itself. Low rates of PID have been noted in IUD users of 1.6/1000 woman years. The incidence of PID was noted to be highest in the first 20 days following insertion. Thereafter the risk drops to match non-users of IUD. Bleeding patterns and pain
Menstrual abnormalities and pain are the most common reasons for discontinuation of IUD. Copper IUDs have been noted to cause spotting, light bleeding, heavy or prolonged periods in the first 3–6 months following insertion. These symptoms are known to improve with time. Although they do not affect ovulation, a short luteal phase has been documented with these devices.
Irregular bleeding or spotting is common in the first 6 months of insertion of the progestin-releasing IUD but by 1 year amenorrhoea or light bleeding is the rule. Ovulation remains unaffected in almost 75% of women fitted with the progestin-releasing IUD. Hormonal side-effects
Some systemic absorption does occur, and side-effects as a result are most pronounced in the first 3 months after insertion. However, from the limited evidence available there are no clinically significant differences in hormonal side-effects (acne, headache) between a copper IUD and a progestin-releasing one. Ovarian cysts
One randomized trial has found increased incidence of ovarian cysts in progestin-releasing IUD users compared with the copper IUDs. Most resolve spontaneously and rarely become symptomatic. Non-contraceptive benefits
The progestin-releasing IUD has found an important place in the treatment of menorrhagia, with menstrual blood loss decreasing by more than 80% in its presence. In addition, it also provides endometrial protection from the stimulatory effects of oestrogen and thus works well as the progesterone arm of hormone replacement therapy. There is also some evidence that it is useful in decreasing the pain associated with endometriosis.
The copper IUDs have in one review of case–control studies found to be associated with a reduced risk of endometrial cancer; however, the mechanism of this remains unknown. Clinical approach
Prerequisites for IUD insertion
When deciding to have an IUD inserted, the first consideration should be the skill and experience of the operator. The Faculty of Sexual and Reproductive Health in the UK recommend that operators hold a letter of competence before undertaking these procedures. In order to maintain skills one should fit at least one device per month in an unanaesthetized woman.
IUD insertion should be considered a surgical procedure and as such should be performed under aseptic conditions. Equipment for resuscitation should be at hand and an assistant present throughout the procedure to aid the operator.
The operative technique should be explained to the patient as well as the side-effects. Verbal or written consent should be obtained prior to commencement.
A pelvic examination is important before insertion. This is the time to rule out any condition that may make insertion unsuitable. Obvious ulcers on vulva, vagina, or cervix, cervical excitation, adnexal tenderness, purulent cervical discharge, and a cervix that bleeds easily to touch all point towards a possible sexually transmitted infection or PID. Insertion should only proceed once these conditions have been ruled out. Similarly, suspicion of an excessively enlarged or distorted uterine cavity should discourage one from proceeding. If at examination, determining the size and position of uterus proves difficult, IUD insertion is best deferred. It will be impossible in such cases to ensure high placement of the coil resulting in an increased risk of perforation. The choice of IUD
Following counselling a woman with no contraindications may opt for either a copper or progestin-containing device. However, the effects of different IUDs on menstrual bleeding may be a determining factor when making the choice. If the copper IUD is chosen then the device with the lowest failure rate and longest duration of action should be first line, namely the TCu380S in the UK. In the event of the uterine cavity length being less than 6.5 cm then a device with a shorter stem or a frameless device is chosen. Timing of insertion
IUDs can be inserted at any time in the menstrual cycle, provided a pregnancy can be reliably excluded. Copper IUDs are effective as soon as inserted but the progestin only IUDs are not. If inserted beyond day 7 of the cycle the patient should use additional protection for 7 days. Insertion of IUD in a conscious patient
• A ‘no touch technique’ should be employed throughout the whole procedure so that only clean gloves need be worn. A no touch technique implies that any instrument/object that is to be inserted into the uterine cavity should not be allowed to come into contact with unsterile surfaces and should only be held by its handle. If any manipulation is needed of the sterile IUD in its holder then sterile gloves are to be used.
• The patient is made to lie in a modified lithotomy position and a bimanual examination is performed to assess the size and lie of the uterus.
• The cervix is exposed, cleansed with aseptic solution, and grasped with a 12-inch atraumatic forceps such as Alice Tissue forceps. While stabilizing the cervix this also helps to straighten the uterocervical canal, allowing a controlled IUD insertion and correct fundal placement.
• A malleable uterine sound passed gently into the cavity helps to determine its depth and direction as well as the patency and direction of the cervical canal.
• The device is loaded into the introducer in a manner that allows that upon release it will lie flat in the transverse plane of the uterine cavity.
• The device should not be left in the introducer for a prolonged period of time as it may lose its shape.
• Once the introducer is inserted into the cavity the IUD should be released according o the manufacturer’s direction
• High fundal placement is important to avoid the risk of expulsion and pregnancy. Further sounding of the canal following insertion therefore helps exclude a low-lying IUD.
• Threads are trimmed to 2.5–3 cm from the external os. Problems at insertion
Vasovagal syncope
Severe pain leading to ‘cervical shock’ or vasovagal syncope is rare. It is caused by distension of the internal cervical os. In mild cases one can proceed after waiting a short while for the patient to recover; 1% local analgesic gel or a local anaesthetic injection may be applied to the cervix before resuming. In severe cases, insertion should be halted, the patient placed head down and the airway maintained. If vasovagal syncope occurs as the insertion is being completed, the IUD can be left in place while allowing the patient to recover.
Epileptic attacks
In those prone to epilepsy, fits are sometimes precipitated by the insertion. These are not a direct result of pain and usually present a few minutes after the cervical stimulus.
Perforation
Although rare, once detected or suspected immediate gynaecological reviews is necessary. Laparoscopy and or laparotomy may be necessary to retrieve the IUD. Resuscitation measures
• IUD insertions are best carried out with a calm reassuring and unhurried approach. Patient anxieties need to be acknowledged and addressed as far as possible.
• In the event of a vasovagal attack, insertion should be deferred. The patient should remain supine but the head end of the touch examination should be lowered and legs elevated to restore blood flow.
• A clear airway must be maintained.
• Oxygen if available should be delivered through an Ambu bag.
• In the event of persistent bradycardia, atropine should be given intravenously in at dose of 0.6 mg.
• In the rare event of a patient failing to regain her consciousness she must be transferred to the nearest accident and emergency department or intensive care unit. Post insertion instructions
• The patient should be taught to check for the presence of threads in herself. It is best checked on a monthly basis soon after a period. The presence of threads alone implies the device has not been expelled or lost. If the threads are found to be missing it is important she seek medical help at the earliest and refrain from intercourse without alternative protection until seen.
• She should be warned to expect some degree of crampy abdominal pain, bleeding, and discharge over the next 48 hours. These can be managed symptomatically.
• There is no longer any necessity for the patient to return for a routine follow up. Provided she is capable of looking out for any untoward symptom and reporting it, the patient need return only when a removal is required. Pelvic actinomyces and IUD
In the asymptomatic patient there is no indication for removing the IUD in case actinomyces-like organisms (ALO) are detected on swab. Again there is no need for rescreening at a later stage.
Actinomyces israeli is a normal commensal of the vagina and consideration for removal is necessary only when there are signs of infection. STI and IUD
In the event of an STI developing with the IUD in situ there is no need for removal. It is unlikely for the STI to develop into PID due to presence of an IUD. Treatment can continue for the STI without the need to remove the IUD. Should PID develop, the IUD can remain in place while treatment continues. However, if the infection fails to resolve despite treatment with antibiotics, removal should be considered. Further reading
Belhadj H, Sivin I, Diaz S, et al. Recovery of fertility after use of the levonorgestrel 20 mcg/d or Copper T 380 Ag intrauterine device. Contraception 1986;34: 261–7.
Faculty of Sexual and Reproductive Healthcare Clinical Effectiveness Unit. Intrauterine methods of contraception. London: FSRH CEU 2007.
Haugan T, Skjeldestad FE, Halvorsen LE, Kahn H. A randomised trial on the clinical performance of Nova T380 and Gynae T380 Slimline copper IUDs. Contraception 2007:75:175–6.
National Institute for Health and Clinical Excellence (NICE). Long-acting reversible contraception: the effective and appropriate use of long-acting reversible contraception. London: NICE 2005.
Wu Shangchun, IUD: the key contraceptive method in China. Abstract, ESC. Congress, Istanbul, 2005.
Xiong X, Buekens P, Wollast E. IUD use and the risk of ectopic pregnancy: a meta-analysis of case control studies. Contraception 1995;52:23–34.
Contraception and Sexual Health, 2004/5 ONS 2005. Internet resources
www.emedicine.com Patient resources
www.fsrh.org
www.fpa.org.uk
In vitro fertilization Definition
Literally fertilization ‘in glass’, the term is widely used to describe the process of superovulation followed by oocyte collection, fertilization of the oocyte with sperm in a laboratory, with subsequent transfer of one or more embryos. The generic ‘ART’ (assisted reproductive technology) refers to all types of laboratory-based assisted conception treatments including in vitro fertilization (IVF), intracytoplasmic sperm injection (ICSI), intrauterine insemination (IUI), and donor insemination (DI) Epidemiology
Infertility affects about one couple in seven in the UK. The condition is becoming more common as women defer attempts to conceive until later in life. Obesity interferes with ovulation and sexually transmitted pelvic infections affect Fallopian tube and epididymal function (Hughes et al. 2007; ACOG 2008). The UK Human Fertilization and Embryology Authority (HFEA) recorded over 41 000 IVF cycles in 2006 which resulted in 9,600 births and nearly 12 000 babies (Table 12.19.1).
Table 12.19.1 shows the influence of the woman’s age on her chances of a live birth following IVF. The national average of 31% chance of live birth after fresh embryo transfer for women under 35 is the highest yet seen and reflects improvements in laboratory and clinical practice. Embryos remaining after fresh transfer can be frozen to be thawed and replaced later, usually in a natural menstrual cycle, albeit with lower chances of live birth per transfer.
In the UK, IVF contributes about 1.4% of all births. This is a modest figure compared with many Western European countries: in Denmark 6% of births are a result of IVF treatment. The proportion is rising steadily and projections suggest that some European countries will see greater than 10% of all births resulting from IVF conception by 2020.
Currently, the proportion of UK twin pregnancies resulting from IVF is above 20%. The number of triplet births arising from IVF has fallen sharply since the introduction of a ‘two embryo transfer’ policy for women under 40. However, twin pregnancy also carries significant excess morbidity and mortality compared with singleton birth (see www.oneatatime.org.uk). Several Scandinavian countries, Belgium, and Denmark have reduced this proportion by promoting single embryo transfer (SET) (Sunde 2007), and HFEA has now initiated a semi-voluntary code for clinics in an effort to reduce the proportion of IVF twin births in the UK. Pathology
The pathologies that cause infertility requiring IVF treatment are multiple. IVF was first developed as a treatment for tubal disease. Damage or blockage of the Fallopian tubes can be corrected surgically but restoration of tubal patency does not necessarily result in live birth. Damage to the microstructure of the tube (epithelial cilia and surrounding smooth muscle) may be permanent and frequently leads to failure of tubal transport with persistent infertility or ectopic pregnancy. IVF bypasses the tube, with collection of oocytes from the ovary and replacement of embryos into the uterine cavity. Since the first IVF birth 30 years ago, the technique has been widely applied to all causes of infertility. Introduction of intracytoplasmic sperm injection (ICSI) in the mid-1990s revolutionized treatment of male infertility. Couples with a male factor problem now have similar chances of a live birth compared to routine IVF. Anovulatory infertility resulting from polycystic ovary syndrome is best treated with simple ovulation induction with oral agents (Clomiphene citrate, aromatase inhibitors), laparoscopic ovarian drilling, or injectable gonadotropins. Polycystic ovary syndrome carries an increased risk of ovarian hyperstimulation syndrome (OHSS) after superovulation, which should be used only for resistant cases or where other factors are also involved. Unexplained infertility is also treated with IVF following a period of ‘watchful waiting’, usually of at least 3 years duration if the woman is under 35 years of age (Bhattacharya 2008). Prognosis
The most important prognostic factor in IVF treatment is the age of the woman at the time of treatment. Those under 35 years have over 30% chance of live birth per cycle, rising to 50% if ‘spare’ embryos can be transferred later after freeze–thaw. At age 40, IVF carries a 10% chance of live birth and births after 45 are rare (HFEA 2008). The fall in the chances of a live birth with advancing female age results from poor ovarian response to superovulation, with fewer eggs being obtained and a decline in oocyte ‘quality’ (increasing rates of aneuploidy and probably also increasing cytoplasmic dysfunction). Older women frequently resort to treatment with oocytes donated by younger women, which carry the potential for pregnancy and aneuploidy risk of the donor’s age rather than the recipient. However, older recipients of oocyte donation are at increased risk of pregnancy complications including pre-eclampsia, premature birth, and problems in labour.
Table 12.19.1 HFEA national data for IVF, 2006 (published October 2008) (with permission from HFEA www.hfea.gov.uk)

Ageing of the male partner seems to have less impact on IVF outcome, particularly since ICSI can be used to correct for sperm dysfunction. The presence of uterine abnormalities including fibroids and congenital abnormalities can adversely affect implantation, and ovarian endometriosis is also associated with a poorer outcome in age-matched studies. Hydrosalpynx, with resultant passage of tubal fluid into the endometrial cavity, reduces pregnancy chances and pre-IVF salpingectomy or tubal occlusion is widely performed in such cases (Johnson 2004). Clinical approach
The principle of IVF is simple. Eggs and sperm are mixed in the laboratory and the resultant embryos returned to the uterine cavity at the correct stage of the cycle. However, the complexity of practice has increased dramatically over the last two decades and ART is one of the most striking examples of successful collaboration between science and medicine.
The chances of obtaining good-quality embryos are increased if the laboratory has a number of oocytes to work with. Hence, from the 1980s onwards IVF treatment has started with superovulation, the use of injectable gonadotropins (recombinant FSH or urinary derived FSH or FSH/LH combinations) to induce multiple follicle development in the ovaries. Follicle growth is monitored by transvaginal ultrasound to count and measure the follicles. A ‘mature’ follicle secretes significant amounts of oestradiol into the circulation, providing a second marker of follicle growth and development. Left unchecked, rising concentrations of oestradiol would initiate an LH surge with ovulation and loss of the cohort of oocytes. Hence the practice of superovulation is combined with use of a gonadotropin-releasing hormone (GnRH) agonist or antagonist, also given by injection or, in the case of the GnRH agonist, intranasally. GnRH agonists cause an initial ‘flare’ in concentration of LH and FSH in serum, followed by pituitary receptor blockade and ‘downregulation’ of LH and FSH, thereby preventing an endogenous LH surge. The widely used ‘long protocol’ involves initiation of GnRH agonist in the mid-luteal phase of the cycle preceding the start of FSH superovulation. The woman will experience 2 weeks of menopausal symptoms in this period, which is followed by an ultrasound and hormonal check of downregulation (quiescent ovaries and thin endometrium on scan, suppressed concentrations of oestradiol, LH, and FSH in serum).
Over the last decade, GnRH antagonists have been introduced as an alternative to the long protocol. They act with immediate inhibition and can therefore be used in parallel with FSH superovulation without the preliminary period of downregulation. This makes the treatment cycle shorter and less unpleasant, reduces the risk of ovarian hyperstimulation, and is more cost effective than the long protocol, a process sometimes termed ‘mild’ IVF (Heijnen 2007).
Once ultrasound and endocrine criteria for follicle maturation have been met (usually at least two follicles of greater than 16 mm diameter), a single injection of human chorionic gonadotropin (hCG) is given. This is a cheap and simple surrogate for LH, and initiates final oocyte and follicular maturation with resumption of oocyte meiosis, expulsion of the first polar body, and progesterone synthesis by the granulosa cells. Ovulation will occur approximately 40 hours later, so oocyte collection is timed 34–36 hours after hCG administration.
In the early days of IVF, oocytes were collected laparoscopically, with the risks and organizational drawbacks of general anaesthesia and surgery. Transvaginal ultrasound-guided needle aspiration of follicles is a simpler and safer procedure, often performed with sedation and analgesia. Many units will encourage the husband/partner to be present for egg collection. Each follicle is aspirated in turn, with the follicular fluid being passed to the embryologist, who identifies the oocyte and transfers it into culture medium using a binocular microscope. Oocyte collection takes between 15 and 45 minutes depending on the number of follicles harvested. The patient can usually return home a few hours after the procedure.
Following oocyte collection, the male partner with normal sperm parameters will produce a semen sample by masturbation. Men who do not ejaculate sperm because of previous vasectomy or other blockage to the vas or epididymis, or due to such poor spermatogenesis that sperm can only be obtained by biopsy, will need to undergo percutaneous epididymal and/or testicular biopsies. Immediate microscopy will confirm the presence of sperm in the samples. Next the IVF is performed. The oocyte is stripped of its investment of cumulus cells and exposed in vitro to approximately 50 000 washed sperm, allowing normal fertilization. For couples with suboptimal sperm parameters, or who have only epididymal or testicular sperm available, the ICSI procedure is performed in which a single sperm is injected into each oocyte.
Idiopathic oligospermia or azoospermia requires investigation before sperm can be used for ICSI. Male carriers of genes for cystic fibrosis may have congenital absence of the vas deferens, leading to azoospermia, and those with karyotypic abnormalities that may produce problems in their offspring may have severe oligospermia. Both conditions should be routinely screened for before IVF/ICSI is offered. Oligo or azoospermic men may also have microdeletions on the Y chromosome. Some clinics offer screening for these deletions, although they do not appear to have implications for the health of the man or his male child, apart from the risk of inheritance of the defect in spermatogenesis. Once this is explained, few patients opt for the costly testing involved in confirming or excluding this diagnosis.
One of the major areas of improvement in quality of ART over the last decade has been in the laboratory handling of gametes and embryos. Stringent incubation conditions coupled with culture media carefully designed to meet the changing metabolic needs of the early embryo as its genome is activated, have played a large part in the improvement in success rates of IVF. Embryos are generally cultured for between 2 and 5 days following oocyte collection. Culture to the blastocyst stage provides considerably more information on the morphology of the embryo, allowing improved selection of those most likely to implant after transfer to the endometrial cavity. However, such prolonged culture adds to the cost of the procedure and some women who would have had embryos for transfer on day 2 or 3 are disappointed when none survive to day 5. The optimal strategy remains a topic for debate, although the move to SET makes correct embryo selection critically important and more clinics in the UK are moving to blastocyst culture for the younger patient as a prelude to SET.
Embryo transfer is usually a straightforward procedure involving passage of a Cusco’s speculum, gentle cleansing of the cervix with saline or culture medium, and transfer of the embryo(s) into the uterine cavity with a flexible catheter. This is often done under ultrasound guidance, with the optimum placement of the catheter tip approximately 1 cm from the fundus. Difficult embryo transfers are less likely to result in pregnancy: a fall in the temperature of embryos seems particularly detrimental, so it is critical to undertake a smooth and timely embryo transfer.
Once embryos have been transferred the couple have to wait for 2 weeks to know whether implantation has occurred. The luteal phase of the cycle is supported with progestagens, given vaginally or by injection. Randomized controlled trials have shown the superiority of progestagens over placebo but the optimum route and dose is not determined. Pregnancy testing is carried out by measuring hCG in a serum sample. A positive test will be repeated 7 days later, followed by early pregnancy transvaginal scan after a further week in order to detect miscarriage (blighted ovum) or ectopic pregnancy as soon as possible. Approximately 20% of IVF pregnancies will miscarry, more frequently if the woman is older, with ectopic pregnancy rates of up to 5% depending on the cause of the infertility. Both require medical intervention, which should be organized by the IVF clinic. Complications
IVF pregnancies have lost some of their high-risk status as the numbers of women pregnant after IVF has risen. The majority of the problems in pregnancy result from the consequences of multiple pregnancy rather than from IVF treatment per se (El-Toukhy 2006). However, even IVF singleton pregnancies end slightly earlier and produce babies that are slightly lighter than matched spontaneously conceived children. Children born after ICSI appear to have a slightly higher risk of congenital malformations, particularly of the urogenital system, than do IVF or spontaneously conceived children, and some studies have raised anxiety about the frequency of disorders of imprinting after ICSI. These statistics do not mean that the technologies should be abandoned, rather that ART should only be used when necessary and not as a lifestyle choice or substitute for other simpler and more natural approaches to infertility.
The processes of superovulation, oocyte collection, and embryo transfer are generally accepted as low risk when carried out in a reputable clinic. However, some patients, particularly younger women with polycystic ovaries, are at risk of developing OHSS. This iatrogenic condition is seen in its severe form in 1–2% of IVF treatment cycles. Serious morbidities including cerebrovascular thrombosis, and renal and pulmonary failure, and some deaths have been reported. The condition results from excessively high secretion of oestrogens and of vasoactive molecules, including vascular endothelial growth factor, leading to separation of the capillary endothelial cells. Leakage of plasma water and small molecules occurs, leading first to ascites and later to pleural and pericardial effusions. At the same time the intravascular compartment is fluid depleted, with haemoconcentration and risk of thrombotic phenomena occurring. Increased intra-abdominal pressure together with intravascular dehydration results in prerenal failure and multi-organ involvement with adult respiratory distress syndrome and cardiac failure can occur (RCOG).
The best form of ‘cure’ is prevention. Cancellation of the treatment cycle by withholding hCG injection if an excessive number of follicles are seen on ultrasound will avoid the syndrome developing, but at the cost of an abandoned cycle. The condition worsens with further hCG stimulation so elective cryopreservation of all embryos rather than fresh embryo transfer is often used to avoid pregnancy with rising hCG and worsening of the condition. Many specific treatments have been tried without much success, and randomized trials are difficult to perform given the relative rarity of the disorder. Excessive rehydration with crystalloids should be avoided, as should diuretics. OHSS is best managed by the Reproductive Medicine team, who should maintain overall charge of clinical decisions even if the patient requires intensive care. A conservative approach with anticoagulation, careful monitoring and abdominal paracentesis, if excessive ascites develops is usually effective. Surgery should be avoided if possible as the ovaries may be hyperaemic and uncontrollable bleeding can occur. Adjuncts to IVF
IVF allows access to embryonic DNA. Microbiopsy of one or two cells from an eight-cell embryo seems harmless. Each embryonic cell is toti-potent at this early stage and there does not seem to be any developmental detriment after biopsy. The cells can be probed with PCR or FISH (fluorescence in situ hybridization) or CGH (comparative genomic hybridization) to detect carriage of chromosomal or genetic disorders. This technique of pre-implantation genetic diagnosis has allowed families with a child affected by a serious genetic disorder such as Duchenne’s muscular dystrophy or thalassaemia major to select unaffected embryos for their subsequent child. This is clearly preferable to prenatal diagnosis followed by termination of pregnancy, although the relatively low chances of pregnancy after IVF can result in a requirement for several treatment cycles before a healthy pregnancy is established. More and more non-infertile couples are likely to use IVF to access embryonic DNA in the future. New uses of IVF technology include the conception of a ‘saviour sibling’: an HLA matched healthy child who can act as a donor of umbilical cord stem cells for transplantation to an older affected brother or sister (Sermon 2004).
Techniques for cryopreservation of embryos and gametes have also improved dramatically over the past decade. Embryo freezing gives a second chance at pregnancy after a fresh embryo transfer cycle and can also be used to preserve fertility for young women before gonadotoxic chemotherapy or radiotherapy. Embryos can be replaced some years later after successful but sterilizing treatment is completed. However, embryo freezing requires a stable relationship with the future father of the child, and many women are not yet at this stage of life when cancer occurs. Oocyte vitrification, ultrarapid freezing with cryopreservation by glassification, has improved success rates of oocyte freezing. The frozen eggs can be thawed and fertilized by ICSI years later once treatment is complete and a stable relationship established. This is a new technique and data on effectiveness and safety are lacking. Some clinics are also offering oocyte vitrification to healthy women who wish to delay motherhood. A recent statement by the Royal College of Obstetricians and Gynaecologists has warned of the hazards of this approach: there is no guarantee that the method will work and the safety to offspring remains to be proven. Regulation
HFEA was established following the 1984 Warnock Report. The Committee recommended a regulatory framework for this area of scientific and medical practice. It recognized the moral and the personal dimensions of advances in IVF technology and Parliament passed the Human Fertilization and Embryology Act in 1990.
The HFEA acts as regulator to provide key assurances, publishing a Code of Practice which sets out the standards for all clinics to ensure they are following both HFEA policy and the law (see below). Functions of the HFEA
• To license and monitor fertility clinics that carry out IVF and donor insemination
• To license and monitor clinics undertaking human embryo research
• To license and monitor the storage of gametes and embryos
• To produce a Code of Practice which gives guidelines to clinics about the proper conduct of HFEA licensed activities
• To maintain a formal register of information about donors, fertility treatments and children born as a result of those treatments
• To provide relevant advice and information to patients, donors and clinics
• To review information about human embryos, the provision of treatment services and activities governed by the HFE Act.
• To monitor any subsequent developments in this area and where appropriate, advise the Secretary of State for Health on developments in these fields Further reading
American College of Obstetricians and Gynecologists (ACOG) (The Committee on Gynecologic Practice) and the American Society for Reproductive Medicine (Practice Committee). Age-related fertility decline: a committee opinion. Fertil Steril 2008;90:486–7.
Bhattacharya S, Harrild K, Mollison J, et al. Clomifene citrate or unstimulated intrauterine insemination compared with expectant management for unexplained infertility: pragmatic randomised controlled trial. BMJ 2008; 337: a716.
El-Toukhy T, Khalaf Y, Braude P. IVF results: optimize not maximize. Am J Obstet Gynecol 2006;194:322–31.
Heijnen EM, Eijkemans MJ, De Klerk C, et al. A mild treatment strategy for in-vitro fertilisation: a randomised non-inferiority trial. Lancet 2007;369:743–9.
HFEA. A long term analysis of the HFEA register data 1991–2006. London: HFEA 2008.
Hughes G, Simms I, Leong G. Data from UK genitourinary medicine clinics, 2006: a mixed picture. Sex Transm Infect 2007;83:433–5.
Johnson NP, Mak W, Sowter MC. Surgical treatment for tubal disease in women due to undergo in vitro fertilisation. Cochrane Database Syst Rev 2004;(3): CD002125. Review.
Royal College of Obstetricians and Gynaecologists (RCOG). The management of ovarian hyperstimulation syndrome Green Top Guideline number 6. London: RCOG.
Sermon K, Van Steirteghem A, Liebaers I. Preimplantation genetic diagnosis. Lancet 2004 15;363:1633–41.
Sunde A. Significant reduction of twins with single embryo transfer in IVF. Reprod Biomed Online 2007; 15 (Suppl 3): 28–34. Internet resources
www.hfea.gov.uk
www.oneatatime.org.uk
www.nice.org.uk
www.basw.co.uk/progar
www.progress.org.uk
www.cancerbackup.org.uk Patient resources
www.hfea.gov.uk
www.oneatatime.org.uk
www.acebabes.co.uk
www.bica.net (British Infertility Counselling Association)
www.surrogacy.org.uk (Childlessness Overcome through Surrogacy)
www.daisynetwork.org.uk (Premature menopause support group)
www.dcnetwork.org (donor conception support group)
www.infertilitynetworkuk.com
www.miscarriageassociation.org.uk
www.multiplebirths.org.uk
www.endo.org.uk (endometriosis support group)
www.ngdt.co.uk (National Gamete Donation Trust)
www.ukdonorlink.org.uk
www.verity-pcos.org.uk
In vitro oocyte maturation Definition
In vitro maturation (IVM) refers to a form of assisted reproductive technology. The technique is similar to in vitro fertilization (IVF) in many aspects. The major difference is the absence of ovarian stimulation, with exogenous gonadotropins and oocytes being collected before they attain full maturity. The immature oocytes are cultured in the embryology laboratory until they complete the maturation process, i.e. ‘in vitro maturation’, and become amenable to fertilization or to cryopreservation. Upon fertilization of either fresh or frozen–thawed oocytes, the resultant embryos are transferred. Epidemiology
IVM can, in theory, be used to treat any woman who is a candidate for IVF. Women with polycystic ovaries (PCO) or polycystic ovarian syndrome (PCOS) represent the group who achieve the highest pregnancy rates using this method, because IVM pregnancy rates correlate with the number of antral follicles and eggs collected. IVM has therefore become an established treatment for this group of patients. More recently, the indications have been extended to poor responders to ovarian stimulation for IVF or oocyte donors. IVM is also considered as an innovative fertility preservation method for patients with various diseases that preclude treatment with conventional IVF. However, compared with widespread application of IVF, IVM is still practised by relatively few clinics worldwide. Technique
The IVM technique aims to make use of the multiple immature oocytes that already exist in the ovaries of a reproductive age woman. Early in the follicular phase, these immature oocytes are harboured in small antral follicles, and are arrested at the prophase stage of the first meiotic division. These oocytes are shown to resume meiosis upon removal from the follicle, have the capacity to complete meiotic division, and can be fertilized in vitro. More than 80% of oocytes were reported to resume meiosis independent of the day of the menstrual cycle and gonadotropin support in IVM culture medium.
In fact, the first pregnancy and live birth from in vitro matured oocytes in humans was reported in the context of a stimulated IVF cycle. However, recovery of mature oocytes following ovarian stimulation with gonadotropins and gonadotropin-releasing hormone analogues had already become the method of choice, and IVM did not attract much attention until 1991, when Cha and colleagues reported collecting immature oocytes from women undergoing gynecological surgery, fertilizing these donated oocytes following IVM and transferring the resulting embryos to a recipient woman with premature ovarian failure. The recipient delivered healthy triplet girls. Three years later, the collection of immature oocytes from women with PCOS was reported. The immature oocytes collected were matured in vitro with gonadotropin-enriched medium, then fertilized, and a healthy live birth following transfer of resultant embryos was reported. Currently pregnancy rates are above 30% per cycle in appropriately selected patient groups. Indications
IVM has become an established treatment option for women with PCO or PCOS who need antiretroviral therapy (ART). Young women with PCO seem to be the best candidates for IVM treatment. Pregnancy rates seem to be significantly higher when an in vivo matured oocyte has been collected. However, the clinical application of IVM technology is not limited to these women alone, and can be extended to benefit other patient populations.
Over-responders to gonadotropin stimulation
IVM combined with IVF can be a valid option for patients who demonstrate an over-response to COS and are considered to be at risk of varian hyperstimulation Syndrome (OHSS) during an already started IVF cycle. Although several strategies are available for the prevention of OHSS, the only method to prevent it completely is to avoid the injection of human chorionic gonadotropin (hCG) for final oocyte maturation. However, this strategy requires cancellation of the treatment cycle, leading to frustration for both the patient and the physician. Giving the hCG injection when the leading follicle size is 12–14 mm, before the conventional hCG criteria for IVF is met, followed by oocyte collection 36–38 hours later may prove to be an effective strategy. It is possible to collect some mature oocytes together with immature oocytes at this stage of follicle development. Satisfactory high pregnancy and low OHSS rates in such women has been achieved with this strategy.
Poor responders to gonadotropin stimulation
The benefit of ovarian stimulation is the availability of a higher number of mature oocytes that can be fertilized in vitro, and the success of conventional IVF depends on, among other factors, the response to ovarian stimulation with exogenous gonadotropins. Unfortunately, not all women respond similarly to gonadotropin stimulation, and some fail to develop a reasonable number of mature follicles in stimulated IVF cycles. The most common cause of poor response seems to be the age-related decline in ovarian reserve, but it also occurs in some younger women. Numerous stimulation protocols have been developed to increase ovarian responsiveness. However, none has proven to provide a significant improvement over others. Given the fact that gonadotropin stimulation fails to provide the desired number of in vivo matured oocytes in such women, IVM in an unstimulated cycle or combined with natural-cycle IVF may provide a reasonable option.
Oocyte donation
Oocyte donation has become a recognized treatment option for women with severely decreased ovarian reserve, women of advanced reproductive age, women affected by/carriers of certain genetic disorders, women who repeatedly have poor oocyte and/or embryo quality, or multiple unexplained failed treatment cycles.
Oocyte donors are usually young women with high ovarian reserve. This places them at higher risk of early OHSS in stimulated IVF cycles. Besides the risk of OHSS, the inconvenience of the numerous injections required and the concern over the theoretical risk of cancer associated with repeated use of ovulation induction drugs are factors that may cause reluctance on the part of some potential oocyte donors. IVM can become the method of choice for oocyte donation cycles as young women with high antral follicle counts comprise the best candidates for IVM and yield good pregnancy rates. Avoiding ovarian stimulation may decrease the risks and inconvenience for oocyte donors. Such an approach may also serve to increase the availability of altruistic oocyte donors in countries where donation for a fee is not allowed.
Fertility preservation
Improvements in both diagnosis and treatment of cancer have led to an increase in numbers of cancer survivors. However, certain therapeutic agents bear the potential to permanently damage these prepubertal or reproductive age women’s gonads. Chemotherapy for non-oncological conditions such as systemic lupus erythematosus, or other autoimmune disorders, surgery for endometriosis and non-malignant ovarian neoplasms, and genetic disorders such as Turner’s syndrome and fragile X premutation are among other factors that can cause irreversible gonadal damage and seriously decrease future fertility potential.
The American Society of Clinical Oncology and American Society of Reproductive Medicine have endorsed IVF and embryo cryopreservation (EC) as the only methods of female fertility preservation. However, conventional IVF and embryo cryopreservation requires 2–5 weeks to complete, produces relatively high oestradiol levels, which may be deleterious in certain hormone-sensitive malignancies, and requires a male partner.
IVM expands the fertility preservation options for women who are not candidates for IVF-EC for various medical and social reasons. Women with hormone-sensitive tumours may undergo immature oocyte collection and cryopreserve resultant embryos.
IVM not only eliminates the risks and cost associated with gonadotropins but it also enables oocyte retrieval at any phase of the menstrual cycle and completion of the fertility preservation procedure in 2–10 days, preventing a delay in treatment of the primary disease.
For patients without a male partner, oocyte cryopreservation represents a less invasive option than ovarian tissue cryopreservation. Recent advances in vitrification techniques have markedly improved the efficacy of oocyte cryopreservation. Immature oocytes can also be harvested from ovarian biopsy specimens and can be vitrified following IVM. A novel fertility preservation strategy involves immature oocyte retrieval in an unstimulated menstrual cycle or from ovarian tissue biopsies, followed by IVM and oocyte vitrification or EC.
In conclusion, IVM combined with embryo or oocyte vitrification provides previously unavailable options for some patients and improves the services provided by a fertility preservation programme. Primary-care physicians and oncologists need to be made aware of the fertility preservation options in order to provide early discussion with their patients, followed by referral, if desired, to an ART centre that offers the full range of fertility preservation options. Prognosis
Pregnancy rates
The most important determinants of pregnancy following an IVM cycle are the female age and the number of oocytes collected. Young women with PCO seem to be the best candidates for IVM treatment. In 2007, we achieved an embryo implantation rate of 15% and a clinical pregnancy rate per embryo transfer (CPR) of 36.7% in women younger than 35 years of age. However, for women aged between 35 and 40 years, implantation and CPR were 10.1% and 29.3%, respectively, in the same period. Pregnancy rates seem to be significantly higher when an in vivo matured oocyte has been collected. In 2009, we achieved a >50% clinical pregnancy rate in such cycles in young women with PCO. The two major changes in our protocols were delaying hCG administration until the leading follicle was 10–12 mm in size and endometrial thickness was ≥6 mm, and performing oocyte collection 38 hours after hCG injection.
Pregnancy losses
In a retrospective analysis of 1581 women who had a positive pregnancy test following ART with IVM, IVF, or ICSI in our unit during a 5-year period, biochemical pregnancy loss rates were similar among these patients (17.5% for IVM pregnancies, 17% for IVF, and 18% for ICSI pregnancies, p = 0.08). However, the clinical miscarriage rate was significantly higher in IVM pregnancies (25.3%) than in IVF (15.7%) and ICSI (12.6%) pregnancies (p as the former stimulates the growth of both follicles and the endometrium. On the other hand, when the leading follicle is close to meeting the collection criteria, oestrogen is preferred as it slows down follicular growth while stimulating endometrial proliferation.
Oocyte collection procedure
The principles of transvaginal ultrasound-guided oocyte retrieval for IVM are the same as those for IVF oocyte collection with a few modifications in both the technique and the equipment. Most patients easily tolerate the procedure under conscious sedation with intravenous midazolam and fentanyl. Paracervical block is achieved with 1% bupivacain injection after cleaning the vagina with sterile saline. As the follicles are smaller than mature follicles aspirated in IVF cycles, a smaller gauge needle (19–20G) with a shorter bevel is used. The aspiration pressure is set at 75–80 mmHg, approximately half the conventional IVF aspiration pressure, in order to minimize the risk of oocyte denudation during aspiration. This precaution is carried out because immature oocytes need the presence of surrounding granulosa cells during the nuclear maturation process. The fine-bore needle may be blocked frequently with bloodstained aspirate and ovarian stroma. Therefore, multiple punctures are often needed and flushing the needle lumen with heparinized saline between punctures is required. Sometimes external abdominal pressure may be required to fix the mobile ovaries during collection. Patients with difficult-to-reach ovaries or poor pain control may do better under limited general anaesthesia with propofol.
Embryology laboratory procedures
Similar to IVF, the follicular aspirate is first examined under a stereomicroscope to identify cumulus–oocyte complexes (COCs). Since the identification of small immature oocytes is more difficult, they can be overlooked with the conventional technique. Therefore, the follicular aspirate is filtered through a nylon mesh strainer with 70 μm pores after removal of initially identified COCs. The filtered aspirate can be re-examined after washing with HEPES buffered human serum albumin-containing medium. The maturation status of the oocytes is assessed immediately after collection; a mature oocyte at the meiosis II stage can be identified by the presence of the first polar body in the perivitelline space. The cytoplasm of immature oocytes is examined for the presence of a germinal vesicle (GV). An oocyte is defined as being at the germinal-vesicle breakdown stage if no GV can be identified in the absence of a polar body.
Oocytes reaching the MII stage on the day of collection are denuded and fertilized together with any in vivo matured oocytes, while immature oocytes are cultured in IVM medium and periodically assessed for maturation status. They are denuded and fertilized upon completion of nuclear maturation.
Although similar implantation and pregnancy rates have been reported following fertilization of in vitro matured oocytes with ICSI or IVF, ICSI has been commonly practised in IVM cycles because of a theoretical risk of zonal hardening during the in vitro culture period. Another reason for preferring ICSI over IVF in IVM cycles is some immature oocytes being denuded for assessment of polar-body extrusion. Oocytes devoid of cumulus cells can have decreased chemotactic potential for sperm in the medium. The preferred time for ICSI is 2–4 hours after polar-body extrusion.
Culture conditions for fertilized oocytes and cleavage stage embryos derived from in vitro matured oocytes are the same as those in IVF cycles. Embryo development and quality are similarly assessed, based on the number of blastomeres and the amount of anuclear fragments.
Embryo transfer
The timing of embryo transfer and the number of embryos to be transferred are dictated by the number and quality of available embryos. Embryo transfer is commonly performed on the third day after oocyte collection. Growth and quality of available embryos are evaluated with regard to fertilization time of each embryo. A group of best embryos for days is transferred using essentially the same technique as that employed in IVF cycles. In general, embryo implantation rates in IVM cycles are lower than in IVF cycles. Therefore, on average, one or two more embryos are transferred in order to maintain similar pregnancy rates. However, as expected, this fact does not seem to increase multiple pregnancy rates after IVM.
High implantation and pregnancy rates have been achieved by performing blastocyst transfers in selected IVM patients. Assisted hatching is commonly employed before embryo transfer because of the above-mentioned concerns about zonal hardening.
Luteal-phase support
The luteal-phase support protocol employed in our IVM programme includes 50 mg/day i.m. progesterone injections and oestradiol valerate 6 mg/day po in three divided doses. Luteal-phase support is continued until completion of the first trimester for pregnant patients. Further reading
Ao A, Jin S, Rao D, Son WY, Chian RC, Tan SL. First successful pregnancy outcome after preimplantation genetic diagnosis for aneuploidy screening in embryos generated from natural-cycle in vitro fertilization combined with an in vitro maturation procedure. Fertil Steril 2006; 85: 1510 e9–11.
Buckett WM, Chian RC, Dean NL, et al. Pregnancy loss in pregnancies conceived after in vitro oocyte maturation, conventional in vitro fertilization, and intracytoplasmic sperm injection. Fertil Steril 2008;90:546–50.
Buckett WM, Chian RC, Holzer H, et al. Obstetric outcomes and congenital abnormalities after in vitro maturation, in vitro fertilization, and intracytoplasmic sperm injection. Obstet Gynecol 2007;110:885–91.
Cha KY, Koo JJ, Ko JJ, et al. Pregnancy after in vitro fertilization of human follicular oocytes collected from nonstimulated cycles, their culture in vitro and their transfer in a donor oocyte program, Fertil Steril 1991;55:109–13.
Chian RC, Buckett WM, Abdul Jalil AK, et al. Natural-cycle in vitro fertilization combined with in vitro maturation of immature oocytes is a potential approach in infertility treatment. Fertil Steril 2004;82:1675–8.
Chian RC, Buckett WM, Tulandi T, Tan SL. Prospective randomized study of human chorionic gonadotrophin priming before immature oocyte retrieval from unstimulated women with polycystic ovarian syndrome. Hum Reprod 2000;15:165–70.
Chian RC, Gulekli B, Buckett WM, Tan SL. Priming with human chorionic gonadotropin before retrieval of immature oocytes in women with infertility due to the polycystic ovary syndrome. N Engl J Med 1999;341:1624–1626.
Chian RC, Huang JY, Gilbert L, et al. Obstetric outcomes following vitrification of in vitro and in vivo matured oocytes. Fertil Steril 2009;91:2391–8.
Child TJ, Gulekli B, Chian RC, Abdul-Jalil AK, Tan SL. In-Vitro Maturation (IVM) of Oocytes from Unstimulated Normal Ovaries of Women with a Previous Poor Response to IVF. Fertility and sterility 2000; 74: S45-S.
Demirtas E, Elizur SE, Holzer H, et al. Immature oocyte retrieval in the luteal phase to preserve fertility in cancer patients. Reprod Biomed Online 2008;17:520–3.
Elizur SE, Son WY, Yap R, et al. Comparison of low-dose human menopausal gonadotropin and micronized 17beta-estradiol supplementation in in vitro maturation cycles with thin endometrial lining. Fertil Steril 2009;92:907–12.
Holzer H, Scharf E, Chian RC, Demirtas E, Buckett W, Tan SL. In vitro maturation of oocytes collected from unstimulated ovaries for oocyte donation. Fertil Steril 2007;88:62–7.
Huang JY, Buckett WM, Gilbert L, Tan SL, Chian RC. Retrieval of immature oocytes followed by in vitro maturation and vitrification: a case report on a new strategy of fertility preservation in women with borderline ovarian malignancy. Gynecol Oncol 2007;105:542–4.
Huang JY, Tulandi T, Holzer H, et al. Cryopreservation of ovarian tissue and in vitro matured oocytes in a female with mosaic Turner syndrome: Case Report. Hum Reprod 2008;23:336–9.
Huang JY, Tulandi T, Holzer H, et al. Combining ovarian tissue cryobanking with retrieval of immature oocytes followed by in vitro maturation and vitrification: an additional strategy of fertility preservation. Fertil Steril 2008;89:567–72.
Shu-Chi M, Jiann-Loung H, Yu-Hung L, et al. Growth and development of children conceived by in-vitro maturation of human oocytes. Early Hum Dev 2006;82:677–82.
Soderstrom-Anttila V, Makinen S, Tuuri T, Suikkari AM. Favourable pregnancy results with insemination of in vitro matured oocytes from unstimulated patients. Hum Reprod 2005;20:1534–40.
Soderstrom-Anttila V, Salokorpi T, Pihlaja M, et al. Obstetric and perinatal outcome and preliminary results of development of children born after in vitro maturation of oocytes. Hum Reprod 2006;21:1508–13.
Son WY, Chung JT, Demirtas E, et al. Comparison of in-vitro maturation cycles with and without in-vivo matured oocytes retrieved. Reprod Biomed Online 2008;17:59–67.
Son WY, Chung JT, Herrero B, et al. Selection of the optimal day for oocyte retrieval based on the diameter of the dominant follicle in hCG-primed in vitro maturation cycles. Hum Reprod 2008;23:2680–5.
Tan SL, Child TJ, Gulekli B. In vitro maturation and fertilization of oocytes from unstimulated ovaries: predicting the number of immature oocytes retrieved by early follicular phase ultrasonography. Am J Obst Gynecol 2002;186:684–9.
Tan SL, Chian RC, Buckett WM (eds). In vitro maturation of human oocytes: basic science to clinical applications. Informa Healthcare Books 2006. Internet resources
www.mcgillivf.com
www.ivf-worldwide.com
Malformations of the genital tract Background
The internal female genital tract develops from the two paramesonephric (Müllerian) ducts, whose caudal ends grow medially and fuse in the midline by the eighth week of embryonic life to form the uterovaginal primordium. The septum uniting the two ducts gradually regresses, leading to the formation of the uterine body and cervix and the upper part of the vagina. As the uterovaginal primordium reaches the urogenital sinus, it triggers the formation of two sinovaginal bulbs. Their fusion forms a solid vaginal plate, which canalizes to form the vaginal lumen (Acien 1992).
Anomalies of the genital tract can occur as a result of any of the following events:
• incomplete development of a Müllerian duct: uterine agenesis, unicornuate uterus
• incomplete fusion of the paramesonephric ducts: uterus didelphys, bicornuate uterus
• failure of regression of the midline septum: septate uterus
• incomplete canalization of the vaginal plate: transverse vaginal septum, vaginal agenesis (Grimbizis et al. 2001). Clinical approach
History: key points
• Normal development of secondary sexual characteristics.
• Primary amenorrhoea, dysmenorrhoea or cyclical pelvic pain.
Examination: key points
• Abdominal palpation may reveal a pelvic mass.
• Perineal examination to assess the presence of the vagina and its length.
Special investigations
• Magnetic resonance imaging (MRI)
• Three-dimensional ultrasound
• Intravenous urogram (IVU) to identify any associated renal anomalies
• Diagnostic laparoscopy/hysteroscopy. Vaginal anomalies
Imperforate hymen
The hymen is the embryological remnant of a septum that forms between the sinovaginal bulbs and the urogenital sinus. The septum normally perforates late in fetal life to allow the passage of mucous and blood during menstruation. It is estimated that in 1 in 1000 females, the septum remains imperforate. This is typically an isolated anomaly, which is not associated with any other Müllerian malformations.
Presentation is usually around the time of menarche, when menstrual flow accumulates above the obstruction and leads to the formation of haematocolpos and haematometra. Cyclical pain around the time of menstruation is followed by constant pain or urinary retention as the vagina becomes more distended with menstrual blood.
A pelvic mass may be palpated abdominally, or demonstrated on ultrasound scan or MRI. This usually represents the distended vagina, which pushes the uterus upwards. On inspection of the perineum a bulging vaginal membrane of bluish hue may be visible.
Treatment consists of a cruciate incision of the membrane and excision of hymenal tissue to allow the menstrual blood to drain.
In rarer cases, an imperforate hymen may become apparent at birth, as discharge and secretions accumulate above the obstruction, leading to the formation of a mucocolpos.
Vaginal agenesis
Isolated vaginal atresia (transverse vaginal septum)
A transverse vaginal septum occurs either because of failure of canalization of the vaginal plate, or because of an incomplete union between the uterovaginal primordium and the urogenital sinus during embryogenesis. In the majority of cases, the septum lies in the upper or middle third of the vagina and usually, the higher the location of the septum the thicker it is (Rock et al. 1982). The condition presents with primary amenorrhoea and cyclical pelvic pain. The pain (as in the case of an imperforate hymen) is due to the build up of blood above the obstruction.
Surgical treatment is required in order to resect the septum and anastomose the proximal and distal edge of the vagina. Preoperatively the patient’s menstruation is usually suppressed with gonadotropin-releasing hormone (GnRH) analogues in order to alleviate pain. An MRI of the pelvis will help to assess the thickness and level of the septum, as this will determine the surgical route to entertain. In cases of a thin lower septum, then a perineal approach is appropriate, whereas in cases of thicker and higher septa, it is advisable to proceed to an abdominoperineal approach, and if necessary use a graft of bowel to bridge the gap between the two portions of the vagina.
Postoperatively, the patient should perform regular dilatation, in order to prevent vaginal stenosis.
Mayer Rokitansky Küster Hauser syndrome (MRKH—combined uterine and vaginal agenesis)
This condition occurs in 1 in 5000 female births. The vagina is absent or consists of a short vaginal dimple and the uterus is absent. Often two rudimentary uterine buds can be identified on either side of the pelvis. As the patients have normal ovarian function, secondary sexual characteristics develop normally and presentation is usually in the late teenage years with primary amenorrhoea.
Clinical examination will reveal a short blind-ending vagina and the diagnosis is usually confirmed by performing pelvic imaging, usually MRI. Up to 30% of patients have associated renal anomalies and approximately 10% will have skeletal anomalies.
The condition has devastating implications for sexuality and fertility, and thus adequate specialized psychological support is required. Although women with MRKH will not be able to carry a pregnancy, they are capable of having their own genetic children via IVF and a surrogate uterus.
Treatment also involves creating a vagina to enable penetrative intercourse. In the majority of patients this can be achieved conservatively by using vaginal dilators. The patient is asked to insert vaginal moulds of gradually increasing size into the vaginal dimple and apply pressure. This method of lengthening of the vagina has been shown to be successful in 80% of patients, especially where there is adequate motivation and support (Ismail-Pratt et al. 2007).
In the minority of patients where dilation is unsuccessful, a surgical procedure is required. Various methods exist to create a neovagina and these can be divided into three categories:
• Williams vaginoplasty where a pouch is created on the perineum by suturing the labia majora. This procedure is no longer in favour, as the neovagina is external and the angle of sexual penetration is non physiological.
• Methods where the existing short vagina is lengthened by applying pressure on the vaginal dimple. The Vecchietti procedure was first described in 1965 and has since been modified to be performed laparoscopically. It consists of inserting an acrylic olive within the vaginal dimple, which is then attached to threads that pass through the rectovesical space and on to the abdominal wall. The threads are connected to a traction device that allows their gradual pulling by a centimetre a day. The patient is usually discharged after 1 week, at which time the traction device and bead are removed (Fedele et al. 2000)
• Procedures where a neovagina is created within the rectovesical space and then lined with autologous tissue graft, such as peritoneum (Davydov procedure), skin (McIndoe–Reed), or bowel (ileo- or colovaginoplasty). Both the Davydov procedure and the colovaginopastly have been modified to be performed laparoscopically (Giannesi et al. 2005).
Timing of the vaginoplasty should be carefully considered. In the absence of functioning endometrium and menstrual obstruction there is no urgency to perform an operation early. Creation of a neovagina is only required for sexual intercourse, and therefore could be delayed until the patient reaches adequate maturity to contemplate sexual activity and has the necessary understanding and motivation to perform postoperative dilation.
Longitudinal vaginal septum
A longitudinal septum can vary in length and thickness. In its extreme form, the septum extends from the cervix to the introitus and creates a true double vagina. This is usually associated with a duplication of the cervix and uterus. Rarely, one hemivagina is obstructed, leading to the formation of a unilateral haematocolpos, while menstruation flows normally from the unaffected side. In its more benign forms, the septum remains asymptomatic until the patient attempts to use tampons or becomes sexually active. Rarely, it may only become apparent on having a gynaecological examination, or during labour.
The excision of the septum is a simple vaginal procedure. However, care has to be taken to ensure that it has been fully removed, as scar tissue and stenosis may occur. Uterine anomalies
Müllerian anomalies are commonly classified under the American Fertility Society System in seven categories, which reflect the degree of developmental failure and allow for the classification of abnormalities with similar clinical manifestations, treatment and prognosis (AFS 1988):
• Type I: hypoplasia/agenesis (vaginal, cervical, fundal, tubal, or combined)
• Type II: unicornuate uterus (with the presence of an ipsilateral rudimentary horn, or not)
• Type III: uterus didelphus
• Type IV: bicornuate uterus
• Type V: septate uterus
• Type VI: arcuate uterus
• Type VII: related to diethylstilboestrol use.
Uterine anomalies are estimated to be present in 4.3% of the fertile population (Grimbizis et al.). In their milder form, they may be entirely asymptomatic. More complex anomalies however can lead to dysmenorrhoea and obstetric complications, such as preterm labour, abnormal fetal lie and an increased risk of Caesarean section. Because of the close embryological origin of the renal and genital tracts, uterine malformations are commonly associated with renal anomalies, such as renal agenesis, ectopy, and duplication of the collecting system (Buttram and Gibbons 1979).
Cervical agenesis
This is a rare condition occurring in approximately 1 in 80 000 females. As with other obstructive anomalies, it is associated with primary amenorrhoea and cyclical pelvic pain. Treatment has evolved over the years and now focuses on preserving fertility and anastomosing the uterine body to the vagina. A number of successful pregnancies have been reported following conservative treatment (Defarges et al. 2001) and the uterovaginal anastomosis can now be performed laparoscopically (Creighton et al. 2006).
Unicornuate uterus
A unicornuate uterus results from failure of one of the paramesonephric ducts to develop. In approximately two-thirds of cases, a rudimentary non communicating horn exists and a proportion of those contain functioning endometrial tissue (Shulman 2008). Severe dysmenorrhoea ensues as a result of obstructed menstruation and endometriosis. Although pain presents at the time of menarche, diagnosis is often delayed, as the condition is relatively rare and the patient menstruates from the unobstructed unicornuate uterus.
Treatment consists of resecting the obstructed uterine horn and this can be done laparoscopically (Strawbridge et al. 2007). Preoperative assessment, in the form of MRI and IVU is required to determine the exact level of the anomaly and the number and anatomical position of the ureters.
In management both cervical agenesis and an obstructed uterine horn, menstrual suppression with GnRH analogues is commonplace to alleviate symptoms and reduce the level of endometriosis thereby facilitating the surgical procedure.
Bicornuate uterus
This accounts for 10% of uterine anomalies. Treatment is usually not required. Traditional metroplasty techniques such as the Strassman operation may be used to unify the two cavities and restore the contour of the external uterus. However, it breaches the musculature of the uterus, potentially rendering it more feeble for carrying a pregnancy.
Septate uterus
This is the most common uterine anomaly, accounting for 50% of all. It is estimated that it affects 2–3% of the population and has a marked effect on fertility. The septum can be resected hysteroscopically but no randomized controlled trials have been performed to establish that the procedure improves reproductive outcome. Further reading
Acien P. Embryological observations on the female genital tract. Hum Reprod 1992;7:437–45.
American Fertility Society: The American Fertility Society classification of adnexal adhesions, distal tubal occlusion, tubal occlusion secondary to tubal ligation, tubal pregnancies, Müllerian anomalies and intrauterine adhesions. Fertil Steril 1988;49:944–55.
Buttram VC Jr, Gibbons WE. Müllerian anomalies: a proposed classification (an analysis of 144 cases). Fertil Steril 1979;32:40–6.
Creighton SM, Davies MC. Cutner as laparoscopic management of cervical agenesis. Fertil Steril 2006;85:1510–15.
Deffarges JV, Haddad B, Musset R, Paniel BJ. Utero-vaginal anastomosis in women with uterine cervix atresia: long-term follow-up and reproductive performance. A study of 18 cases. Hum Reprod 2001;16:1722–25.
Fedele L, Bianchi S, Zanconato G, Raffaelli R. Laparoscopic creation of a neovagina in patients with Rokitansky syndrome: analysis of 52 cases. Fertil Steril 2000;74:384–9.
Giannesi A, Marchiole P, Benchaib M, et al. Sexuality after laparoscopic Davydov in patients affected by congenital complete vaginal agenesis associated with uterine agenesis or hypoplasia. Hum Reprod 2005;20:2954–7.
Grimbizis GF, Camus M, Tarlatzis BC, et al. Clinical implications of uterine malformations and hysteroscopic treatment results. Hum Reprod Update 2001;7:161–74.
Ismail-Pratt IS, Bikoo M, Liao LM, et al. Normalization of the vagina by dilator treatment alone in complete androgen insensitivity syndrome and Mayer-Rokitansky-Kuster-Hauser syndrome. Hum Reprod 2007;22:2020–4.
Rock JA, Zakur HA, Dlugi AM, et al. Pregnancy success following surgical correction of imperforate hymen and complete transverse vaginal septum. Obstet Gynecol 1982;59:448–51.
Shulman LP. Müllerian anomalies. Clinical Obst Gynecol 2008;51:214–22.
Strawbridge LC, Crouch NS, Cutner AS, Creighton SM. Obstructive müllerian anomalies and modern laparoscopic management. J Pediatr Adolesc Gynecol 2007;20:195–200. Patient resources
MRKH Organization.inc, American support group for women with Rokitansky syndrome, www.mrkh.org
Male subfertility Definition
Male subfertility can be defined where a seminal, endocrine, genetic, or psychosexual deficiency inhibits a couple achieving a pregnancy within 12 months of attempting where no significant pathology has been identified in the female partner. Additionally, the immune system and structure of reproductive organs can also impact on male subfertility. It is also important to consider the definition of a couple’s subfertility: a couple is considered as infertile if they are not able to conceive after 2 years of contraceptive-free intercourse. Infertility is thought to affect approximately 14% of couples of reproductive age.
Defining male subfertility is not clear and straightforward. The only true means to measure whether the male partner is fertile is to assess his ability of either achieving a pregnancy, which can be dependent on the reproductive health of the female partner, or by assessment of the defining characteristics of a semen sample. It has been clearly demonstrated that the reproducibility of the basic semen analysis is not reliable, and natural pregnancy can be achieved where the male partner demonstrates a low level of sperm concentration. Confounding the problem are men who present with satisfactory sperm concentrations and possess abundant progressive motile cells but suffer from a subtle defect in the functional sperm population, inhibiting their ability to capacitate, recognize, or combine with ova or undergo the later reactions essential for fertilization. Unexplained or idiopathic infertility may have these subtle features; unfortunately they cannot be determined by routine semen analysis. Epidemiology
A World Health Organization (WHO) survey demonstrated from a study of 25 countries that approximately 5% of men of reproductive age suffer from male subfertility. The literature suggests that 8–15% of couples suffer from subfertility. Figures suggest that 30–50% of couples have a significant male factor contribution to this problem. These are conservative estimates, which increase when the proportion of couples who are defined as suffering from idiopathic infertility but in fact have a male factor contribution to their inability to achieve pregnancy are included. Aetiology
Although difficult to elucidate, there is a probable genetic basis for the aetiology of the majority of mechanical, physiological, and functional reasons for male factor subfertility. The genetic effect manifests itself by influencing physiological processes such as hormonal homeostasis, spermatogenesis, and sperm quality. Applications to define subfertile phenotypes are in the developmental stages; therefore, our efforts lie with identifying markers that are apparent in response to defective gene(s) and the transfer of epigenetic information.
The clear indicators of subfertility are
• hormonal deficiencies
• hypothalamic/pituitary or thyroid disorders
• hypogonadotrophic hypogonadism
• testicular disorders
• maturation arrest
• germ cell aplasia
• Sertoli cell-only syndrome
• defective spermatogenesis
• azoospermia
• low sperm concentration and motility
• sperm dysfunction
• chromosomal abnormalities
• Klinefelters
• varicocele (Grade 3 or greater severity)
• systemic disease
• liver disease
• renal failure
• sickle cell disease
• neurological disease
• UTI, mycoplasma and STD. Clinical approach
Diagnosis
The WHO recommends that at least two semen analyses are performed with a time period of at least 3 months between each assessment. A detailed clinical history should be taken to determine potential pathology and to determine an individualized investigation, assessment, and treatment programme.
History Medical history
• Fevers (within the last 3 months)
• Recurrent chest infection, sinusitis, or bronchiectasis
• History of cystic fibrosis (agenesis of the vas deferens)
• Previous genitourinary infections in the form of orchitis (mumps, syphilis, leprosy, tuberculosis), epididymitis, (gonorrhoea, chlamydia, tuberculosis, schistosomiasis, and chronic infection of the prostate and seminal vesicle (painful ejaculation and haematospermia)
• Sport-related testicular torsion
• Chronic disorders (renal failure, liver disease, maliganancy, or diabetes)
• Anosmia (lack of smell), galactorrhoea, visual field defects, and sudden loss of field defects suggest signs of pituitary tumour.
Childhood disorders
• Herniorraphy or testicular torsion
• Mumps
• Precocious puberty before 9 years suggestive of endocrine disorder
• Delayed onset of puberty (gonadotrophin deficiency)
• Cryptorchadism
• Hypospadias
• Midline defects
• End-organ androgen insensitivity.
Previous surgery
• Epididymal obstruction (Yong’s syndrome)
• Testicular trauma or torsion
• Pelvic, bladder, or retroperitoneal surgery.
Fertility history
• Establish frequency and timing of vaginal intercourse.
• Duration of infertility
• History of pregnancies in present and past relationships
• Erection dysfunction
• Psychosexual dysfunction.
Social history
• Use of recreational drugs.
• Excessive alcohol or tobacco use
• Anabolic steroids
• Excessive heat from saunas, hot tubs, and work environment affects sperm production.
History of occupational hazards
• Excessive mental stress
• Exposure to testicular toxins
• Excessive exposure to heat
• Paints and solvents
• Herbicides or pesticides (ethylene dibromide, dibromochloropropane)
• Prolonged exposure to heavy metals (lead, cadmium; suppresses hypothalamopituitary axis, etc.).
• Nitrous oxide
• X-ray
• Non-ionizing and ionizing radiation.
Medications
• Antineoplastics
• Antibiotics
• Cytotoxic agents
• Suphasalazine
• Psychotropic drugs
• Antihypertensive drugs
• Cimetidine
• Nitrofurntoin
• Anticonvulsants.
Investigations
The clinical approach to assessing or considering the male contribution to the couples subfertility has traditionally fallen short compared with the time and dedication given to determining a female diagnosis. Unfortunately, examples exist where an exhaustive testing regime using expensive assays and invasive operative procedures have been performed on the female partner, which have taken years to complete, before the semen characteristics have been analysed and shown to highlight an obvious pathology.
The WHO have reassessed the values given to indicate the normal range (Table 12.22.1).
Initiate the investigation procedure by requesting at least two thorough semen analyses. They must be performed by trained staff in a recognized laboratory that employs rigorous quality control. The laboratory must have access to pathology services to enable further investigations, including collaboration with a histology service with an experienced electron microscopy team (Fig. 12.22.1). In many cases the results of a semen analysis cannot definitively assure fertility, or rule out the possibility of a man being able to sire his own children, regardless of the concentration and percentage of progressively motile sperm. Apart from some cases of azoospermia (2% of the male population are found to be azoospermic), a cautious approach should be taken when considering labelling a patient as fertile, subfertile, or sterile on the basis of the results. The semen analysis can be considered as an inexpensive starting point in determining a treatment or management strategy for a couple.
Table 12.22.1 WHO comparisons of the normal range


Fig. 12.22.1 Electron micrograph of a spermatozoon exhibiting the lack of an acrosomal membrane. The patient’s concentration of sperm was in excess of 20 million per millilitre and greater than 60% of sperm were motile. The couple would require intracytoplasmic sperm micro-injection to achieve a pregnancy. See also colour plate section.
Where medical management leads to an undefined aetiology or there is a time pressure due to the partner’s age the approach from Guzick et al. (2001) may help direct the clinician to advising a couple whether to continue to attempt natural conception or to move directly to an appropriate type of assisted conception by considering the results in terms of ranges, not a clear-cut categorization into fertile and subfertile. Sperm concentrations of above 48.0 million per millilitre will give a good probability of pregnancy, 13.5–48.0 a moderate chance and below 13.5 significantly reduces the possibility to the point where assisted conception should be considered immediately or counselled that pregnancy with their own sperm is unlikely. Although sometimes difficult, a man may have to consider the use of donor gametes or adoption in order to become a father.
Hormone analysis
Indications from the clinical history with a combination of semen analysis results will indicate whether evaluations of the male reproductive hormone levels are necessary. An endocrine assessment is not necessary for a man with normal semen parameters.
Evaluating the hormone profile of men with moderate to low semen samples has not been shown to improve chances of pregnancy. There seems to be no benefit prescribing supplementation with androgens or gonadotrophins. Measurements of serum testosterone and follicle-stimulating hormone (FSH) should be performed initially. A low testosterone level directs the need for a repeat assay. Assessing the level of total and free testosterone, with additional measurements of luteinizing hormone and prolactin levels, will identify whether there is a treatable endocrine pathology. An elevated FSH is a clear indication of an abnormality in spermatogenesis. Caution should be exhibited with endocrine patterns. Although abnormal hormone levels have been identified in 10% of patients who have been tested, the result is only clinically significant in less than 2% of men.
Genetic causes of male subfertility
The contribution of a genetic factor to male subfertility is not fully understood. It is considered that 15–30% of men diagnosed as subfertile have a chromosomal or single gene defect that leads to deficient spermatogenesis. The implementation of techniques such as ICSI, especially when combined with testicular surgical sperm retrieval, has provided treatment for men who would otherwise be unable to father a child. These treatment options have increased the need for an appreciation of the negative consequences and impact of inheritable mutations on the next generation. Despite the absence of evidence of an increase in imprinting disorders with the use of these technologies, there is a concern that bypassing natural selection mechanisms will have an impact on an epigenetic level.
Chromosomal analysis
An incorrect chromosomal number accounts for the majority of genetic causes for male factor infertility. Aneuploidy can lead to non-obstructive azoospermia, cryptozoospermia, and severe oligozoospermia. A karyotype is essential for men with extremely low sperm concentrations (less than 1 million sperm per millilitre) because the incidence of anueploidy is increased in this group. Klinefelter’s syndrome is the most common chromosomal abnormality caused by aneuploidy, yet only a third of suffers will be diagnosed (Table 12.22.2). Spermatogenesis is normally arrested at the germ cell stage, but in some cases sperm development can be seen.
Y chromosome gene defects
Despite the presence of gene defects in many autosomal chromosomes, there is an obvious focus on the Y chromosome. The male sex chromosome contains the majority of genes that are involved in the development of the testis and that are crucial for spermatogenesis. Regions of the Y chromosome have been found to be missing or mutated in subfertile men and a clear link between subfertility and infertility has been demonstrated. Yet care should be employed when referring men for Y chromosome microdeletion assessment, it is essential to highlight the potential of the transmission of aberrant genetic information to male offspring and perpetuating male factor subfertility but the significance of partial microdeletions is still under study and oligo- and cryptozoospermia may have other genetic origins. The NICE guidelines state that it is unnecessary to assess all patients for assessment.
Table 12.22.2 Genetic causes of male factor infertility. Reprinted from Fertility and Sterility, Vol. 93, Iss. 1, Flynn, K, Varghese and Agarwal, The genetic causes of male factor infertility: A review (2010), with permission from Elsevier

DNA fragmentation
The recent sperm function literature has also placed a focus on the effects of damage to sperm DNA and a reduction in the potential to generate a healthy pregnancy. DNA damage may be caused at any point during spermatogenesis, spermiogenesis, and while cells are stored in the epididymis. There are suggestions that subfertile men have a higher proportion of sperm that have suffered DNA damage, either as a result of being marked for apoptosis during production or exposure to deleterious agents. Numerous agents can cause a negative effect on the sperm DNA despite naturally occurring protective mechanisms in the testes and seminal fluid. Sperm that have suffered damage may achieve normal levels of fertilization in IVF situations, yet there is a suggestion that embryo progression is negatively affected and spontaneous pregnancy loss may be increased. The Association of Sexual and Reproductive Medicine has stated that DNA damage is potentially detrimental to the chances of pregnancy but the testing methods and data in the literature require further analysis before this application is adopted into routine practice. Examination
A general physical examination should be performed, initially concentrating on height, weight, and secondary sexual characteristics. This should include examination of testes, penis, and vas deferens. The Testes should be manipulated between the thumb, index, and middle finger to determine the size and consistency. In androgen-deficient men look for gynacomastia, cryptorchidism, hypospadias, and anosmia. Measurement of testicular volume is necessary. An irregular contour, induration, or abnormal consistency may suggest a previous orchitis, surgery, or malignancy. Obstructive azoospermia can be identified by assessment of the caput epididymis; if engorged, further examination by ultrasound or digital rectal examination may be necessary. The presence of a varicocele can be identified by manipulation or by observing the man while in a standing position. Counselling
Psychological support should be provided for couples seeking fertility treatment and investigation. Support from an independent counsellor is generally recommended. The added esteem issues surrounding the label of male factor subfertility increases the potential chance of psychological stress and relationship disharmony. It is essential that the difference between virility and infertility is clearly understood by the man.
Abnormalities on the Y chromosome are thought to be associated with deficient spermatogenesis; therefore, couples undergoing assisted reproductive treatment for significantly poor sperm characteristics should have access to general genetic counselling. Further specific genetic counselling and testing should be available in cases where there is a specific genetic defect associated with failure to achieve a pregnancy.
Before a couple undergo ICSI the potential genetic risks to the resulting child should be explained in terms of the
• inherent risks of the procedure.
• potential for inheritable specific genetic defects as the cause of subfertility. Management
Management of the potentially subfertile male should follow the clear guidance given by NICE for fertility assessments. Gonadotrophins can be utilized for men with hypogonadotrophic hypogonadism. These are effective in improving the chance of fertility without the need to resorting to assisted reproductive technology (ART):
• conservative/non-medical
• medical
• lifestyle changes
• antibiotics where infection is indicated
• diet with the addition vitamin C and E, zinc, fish oil, and selenium
• low-level fertility treatment
• intrauterine insemination
• ART. Surgical
NICE guideline recommendations
Obstructive azoospermia can be effectively managed with surgical correction without the need to refer to assisted reproduction. Epididymal blockage can be reversed by surgery and the duct can be cleared. The chances of pregnancy are not improved by recommending that men with varicoceles are offered surgery. Potential problems associated with testicular surgery are likely to cause the production of antisperm antibodies (ASABs) in response to the breach to the blood–testes barrier. Retrograde ejaculation
Retrograde ejaculation occurs when seminal fluid flows along the line of least resistance, after orgasm, into the bladder instead of the urethra. Failure of the bladder sphincter to close after ejaculation allows a retrograde flow of semen.
Complications after genitourinary surgery for prostate or urethral conditions can cause bladder neck muscle weakness. A common cause for retrograde ejaculation is caused by medication to treat unrelated conditions. Prescription drugs that treat high blood pressure, neurological disorders, and diabetes can affect the muscles that surround the bladder neck. General muscle relaxants can also initiate this trait. Males suffering from diabetes have been identified to have a neuropathy of the bladder sphincter.
Absence or a small ejaculate volume combined with cloudy urine after sexual intercourse can be indicative symptoms. Semen in the bladder does not cause any harm to the man and will leave the body during urination. Employing simple modifications to medication or intercourse with a full bladder can allow a couple to achieve pregnancy with resorting to ART. If necessary, successful pregnancy can be achieved with ART by preparing a sperm suspension for insemination from alkalized urine. Complications/side-effects/sequelae
Men with idiopathic semen abnormalities and mild oligasthenoteratozoospermia should not be given antioestrogens, gonadotrophins, androgens, or kinin-enhancing drugs, since the significance in improving semen characteristics is unclear. Unnecessary use of potential carcinogens is not recommended.
Sections of the literature describe a reduced chance of pregnancy when significant levels of ASABs are identified in semen. This autoimmune response or antibody cross-reactivity can inhibit normal sperm–oocyte interaction and sperm function. NICE guidelines state that the evidence for a significant contribution to male factor subfertility is unfounded. ASAB relevance is debated and any treatment for the male is unnecessary. Corticosteroid treatment has been suggested in the past to have side-effects which outweigh any benefit in achieving pregnancy.
Despite a low rate of complication noted after corrective varicocele surgery (5%) it is recommended that the incidence of localized testicular dysfunction outweighs the benefit of redirecting venous blood flow. Prognosis
Timely investigation and diagnosis will hopefully enable a man to contribute to a pregnancy if there is no significant pathology in the female (Table 12.22.3). The probability of pregnancy, the time involved for investigation, potential for a genetic component, and cost should be considered with the incidence of severe male factor subfertility. Treatment options
• Time of sexual intercourse (TSI)
• Ovulation induction (OI)
• Intrauterine insemination (IUI)
• In vitro fertilization IVF
• Intracytoplasmic sperm microinjection (ICSI).
Table 12.22.3 Suggested management options in male infertility and prognosis

Further reading
Hull M, Glazner C, Kelly NJ. et al. Population study of causes, treatment and outcome of infertility Br Med J (Clin Res Ed) 1985;291:1693–7.
Cooper T, Noonan E, Sigrid von Eckardstein, et al. World Health Organization reference values for human semen characteristics. Human Reprod Update 2010;16:231–45.
O’Flynn O’Brien K, Varghese A, Agarwal A. The genetic causes of male factor infertility: A review. Fert Steril 2010;93:1–12.
NICE. Fertility assessment and treatment for people with fertility problems. NICE Clinical Guidelines February 2004.
Guzick DS, Overstreet JW, Factor-Litvak P, et al. Sperm morphology, motility and concentration in fertile and infertile men. N Engl J Med 2001;345:1388–93 Internet resources
www.asrm.org/uploadedFiles/ASRM_Content/News_and_Publications/Practice_Guidelines/Committee_Opiions/optimal_ evaluation_of_the_infertile_male (1).pdf
www.nice.org.uk/nicemedia/pdf/CG011fullguideline.pdf
www.rcog.org.uk/files/rcog-corp/uploaded-files/NEBFertilityAlgorithm.pdf
www.rcog.org.uk/files/rcog-corp/uploaded-files/NEBFertilitySummary.pdf
www.rcog.org.uk/files/rcog-corp/uploaded-files/NEBFertilityTables.pdf
www.rcog.org.uk/womens-health/clinical-guidance/fertility-assessment-and-treatment-people-fertility-problems Patient resources
www.hfea.gov.uk
Menopause and hormone replacement therapy Definitions
The word menopause is derived from the Greek menos (month) and pausis (Cessation). It is defined as the last menstrual period. As such, the diagnosis can only be made retrospectively after a minimum of 1 year’s amenorrhoea. Although the menopause occurs at an average age of 51, the physiological changes which result in the final menstrual period can start up to 10 years prior to this. Hormonal changes can continue long after the final menstrual period. This episode of rapid neuroendocrine change is characterized by ‘the climacteric’, from the Greek klimax, ladder, i.e. the climb to the menopause during which symptoms occur in most women. Epidemiology
We live at a time when the population is ageing. One hundred years ago only 30% of women lived through a menopause; now, more than 90% will. Thus, the menopause transition and postmenopause is very much a condition of the twentieth and twenty-first centuries. Life expectancy is now 82 years of age for a woman living in the UK. The majority of women can therefore expect to live over a third of their lives in a menopausal state. It is estimated that 15% of women will have an early menopause below the age of 45 and 1% will have premature ovarian failure below the age of 40. Pathophysiology
A newborn female infant has over a million follicles; the follicle cohort shrinks throughout life such that there are only a few thousand follicles left as a woman enters her 40s and few or none in the postmenopause. It is the depletion of follicles which leads to the cessation of menstruation, the cardinal sign of the menopause. Initially, ovarian failure is compensated by gonadotrophin levels starting to rise, in some women from the age of 30 years. During this time there is evidence for a reduced number of gonadotrophin receptors in perimenopausal ovaries, and inhibin production from granulosa cells falls. Decompensated failure then occurs due to the critical decline in the follicle pool leading to further rises in follicle-stimulating hormone (FSH) (10–20-fold); luteinizing hormone (LH) rises only threefold because of its shorter half-life. Oestrogen levels drop due to a reduction in follicle number and qualitative effect on granulosa cell ageing. There is permanent cessation of progesterone production. These changes have been tracked by annual sampling in large populations of women.
Premature ovarian failure/dysfunction
Premature ovarian failure is said to have occurred when menstruation ceases before the age of 40 years and early menopause before the age of 45 years. The author prefers the term premature ovarian dysfunction to signify that the transition into menopause can be lengthy and occasionally may even reverse itself. Although there are many causes of early ovarian failure, the main cause is spontaneous or idiopathic. The main identified genetic causes are Turner’s syndrome and Fragile X. Recently, forkhead genes (FOX03A defect) have been discovered which lead to early follicular activation and thus premature depletion of the follicle pool. Other causes include FSH receptor polymorphisms, first characterized in Finnish populations where follicles are present but unable to respond due to the loss of the FSH receptor. The proportion of women with iatrogenic premature ovarian failure is growing as increasing numbers of women survive leukaemias, lymphomas, and gynaecological cancers due to improved surgical techniques, radiotherapy, and chemotherapeutic regimens.
Other hormonal changes
Adrenal and ovarian androgen levels start to decline from 20 years of age through to the perimenopause, stabilizing by the time of the final menstral period. Some testosterone production continues from the ovarian theca cells. The drop in androgen levels is particularly profound in premature ovarian failure, spontaneous or iatrogenic. The main postmenopausal oestrogen is oestrone, which is produced in peripheral adipose tissue and the postmenopausal ovary by aromatization of adrenal androstenedione. The somatotrophic axis becomes less active with ageing, leading to insulin resistance and a rise in central adiposity. This in turn leads to the change in body shape from the female gynaecoid shape to the male android shape, an independent risk factor for coronary heart disease. There are a number of factors involved in perimenopausal weight gain, including genetic predisposition, socioeconomic influences, reduction in caloric need and expenditure, reduced lean body mass, and a reduction in the resting basal metabolic rate.
The menstrual cycle
Anovulatory cycles become progressively common heading towards the menopause transition. There can be continued oestrogen production in the absence of progesterone leading to endometrial proliferation, hyperplasia, and at its extreme carcinoma. As a result, menstruation can become heavy, prolonged, and unpredictable with intermenstrual bleeding.
Consequences of the menopause
Immediate
Seventy per cent of Caucasian and Afro-Caribbean women suffer from vasomotor symptoms (hot flushes and sweats), the commonest menopausal symptoms. This compares with 10–20% of Japanese and Chinese women, and may reflect cultural differences or may be diet related (isoflavone consumption). Hot flushes are thought to arise due to loss of oestrogen-induced opioid activity in the hypothalamus leading to thermodysregulation. Noradrenaline and serotonin mediate this activity, hence the rationale for using the α-agonist clonidine and the selective serotonin and noradrenaline reuptake inhibitors as alternatives to HRT. Obese women are relatively protected from these symptoms because of their production of oestrone and low sex hormone binding globulin levels, which leaves more of the free active hormone. Other typical immediate menopausal symptoms include insomnia, anxiety, irritability, memory loss, tiredness, and poor concentration. Mood disturbances can occur due to fluctuation in hormone levels, leading to perimenopausal depression. Falling oestrogen levels are thought to lead to similar falls in neurotransmitter levels such as serotonin, which trigger these symptoms. Women who have suffered from postnatal depression and premenstrual syndrome appear to be particularly predisposed to depression in the perimenopause. The menopause transition can also be associated with a significant reduction in sexuality and libido. This is not only because of decreased vaginal lubrication leading to dyspareunia, but also due to the reduction in androgen levels discussed earlier.
Intermediate
Oestrogen deficiency leads to the rapid loss of collagen, which contributes to the generalized atrophy that occurs after the menopause. In the genital tract this is manifested by dyspareunia and vaginal bleeding from fragile atrophic skin. In the lower urinary tract, atrophy of the urethral epithelium occurs with decreased sensitivity of urethral smooth muscle and a decreased amount of collagen in periurethral collagen. All this results in dysuria, urgency and frequency, commonly termed the urethral syndrome. More generalized changes are seen in the older woman as increased bruising and thin translucent skin, which is vulnerable to trauma and infection. A similar loss of collagen from ligaments and joints may cause generalized aches and pains.
Long term
Osteoporosis, cardiovascular disease, and dementia are three long-term health problems that have been linked to the menopause.
• Osteoporosis: osteoporosis is a disorder of the bone matrix resulting in a reduction of bone strength to the extent that there is a significant increased risk of fracture. These fractures cause considerable morbidity in older people, requiring prolonged hospital care and difficulties in remobilization. Osteoporosis is predominantly a disease of women, who achieve a lower peak bone mass than men and are then subjected to an accelerated loss of bone density following the menopause. The hypo-oestrogenic state leads to activation of the bone remodelling units with an excess of bone resorption relative to formation. Women lose 50% of their skeleton by the age of 70 years, but men only lose 25% by the age of 90 years. Loss of height can occur not only due to vertebral fractures but also loss of the intervertebral disc space.
• Cardiovascular: Women are protected against cardiovascular disease before the menopause, after which the incidence rapidly increases reaching a similar frequency to men by the age of 70 years. The protective effect of oestrogen in premenopausal women is thought to be mediated by an increase in high-density lipoprotein (HDL) and a decrease in low-density lipoprotein (LDL), nitric oxide-mediated vasodilatation leading to increased myocardial blood flow, an antioxidant effect on endothelial cells and a direct effect on the aorta decreasing atheroma. Cross-sectional and prospective observational studies have shown that women going through the menopause transition have elevation of cholesterol, triglyceride, and LDL levels and a reduction in HDL2 levels. A key study showed that oestrogen status was an independent predictor of atherosclerotic plaque area after controlling for age, hypertension, diabetes, etc.
• Central nervous system: oestrogen appears to have a direct effect on the vasculature of the central nervous system and promotes neuronal growth and neurotransmission. Studies have demonstrated that oestrogen may improve cerebral perfusion and cognition in women. In the long term this may prevent diseases with a vascular aetiology such as vascular dementia and Alzheimer’s as the vasculature is clearly involved in this. In addition to the effect on vasculature in Alzheimer’s disease, oestrogen may also intervene at the level of amyloid precursor protein. The failure to show benefit for dementia in older populations, and possibly an increased risk with HRT in some studies (Shumaker et al. 2003), may reflect the predominance of the prothrombotic effect of oestrogen in this age group. Diagnosis of menopause
Prediction of ovarian reserve
Until recently, early follicular phase follicle-stimulating hormone (FSH) levels were used to predict ovarian reserve with a level of >10 IU/L indicating reduced reserve and >30 IU/L regarded as being diagnostic of the menopause. However, this test can be misleading; levels vary according to the timing of the sample and often change in subsequent cycles depending on ovarian activity. The most accurate predictors of ovarian reserve currently available appear to be measurement of anti-Müllerian hormone (AMH) production by the primordial follicles and estimation of the antral follicle count on ultrasonographic estimation. AMH is independent of the day of cycle and its predictive value is claimed to last for up to 2 years from when the sample was taken.
Diagnosis of natural menopause
The diagnosis of natural menopause can usually be ascertained from a characteristic history of the vasomotor symptoms of hot flushes and night sweats and prolonged episodes of amenorrhoea. Measurement of plasma hormone levels (oestradiol, FSH, LH) in women in their late 40s onwards with classical symptoms, are not essential as they do not change clinical management. However, in the young patient or in a woman after hysterectomy, where the diagnosis is more difficult and the metabolic implications are serious, measurement of FSH levels may be helpful, in which case repeated measurements of 15 IU/L or above may be regarded as climacteric. Women diagnosed with spontaneous premature ovarian dysfunction should, in addition to hormonal investigations, also have an autoantibody screen and karyotype performed, although the aetiology is usually idiopathic.
In patients still menstruating, persistent hot flushes and night sweats are suggestive of the climacteric, but in those patients with psychological symptoms the diagnosis may be more difficult. In such cases it may be justified to give a trial of oestrogen therapy and monitor the response before discounting a hormonal aetiology. In those women complaining of lack of energy and/or libido a free androgen index and thyroid function tests should be performed as female androgen deficiency and/or hypothyroidism may be contributing to the symptoms.
Ongoing monitoring
After the diagnosis has been established, investigations should be no more than the annual screening which is normally applicable to middle-aged women. This should include assessment of weight, blood pressure and routine cervical cytology. A recent consensus between menopause experts and cardiologists has highlighted the important role that gynaecologists can play in cardiovascular screening (see Further reading). Fasting lipid profile and insulin resistance estimation are recommended in women with risk factors, e.g. increased waist circumference or personal/family history of diabetes/cardiovascular disease.
Routine breast palpation and pelvic examination is unnecessary; these need only be performed if clinically indicated. Mammography should be performed as part of the national screening programme every 3 years unless more frequent examinations are clinically indicated. However, if a woman chooses to use HRT beyond the current age of breast screening cessation (70 years), mammographic screening should also continue. In women over 45 years of age it is best to arrange screening before starting oestrogen therapy to identify patients with sub-clinical disease. Ultrasound examination of the pelvis and/or endometrial biopsy are not a necessary prerequisite to treatment with HRT unless there is undiagnosed bleeding. In the few cases where an underlying pathology is present, bleeding will be irregular after starting treatment, indicating the need for immediate further investigation.
The best currently available measurement of osteoporosis risk is dual energy X-ray absorptiometry (DEXA) measurement of the lumbar spine and hip. Other assessment techniques such as peripheral X-ray screening, e.g. proximal phalynx and calcaneal, and ultrasound screening are improving in terms of their sensitivity and correlation with DEXA, but DEXA still remains the gold standard. Markers of bone formation and breakdown can be useful in that changes occur more rapidly than with bone density but their use is largely confined to research. The Royal College of Physicians (RCP) has issued guidelines as to which high-risk patients should be targeted for DEXA screening (see website). The RCP advises that DEXAs are performed no more than every 2 years because changes in bone mineral density are so small that they often do not exceed the margin of error of the equipment and assessor. The WHO have advised that the decision to treat osteoporosis is made by taking into account not only the bone mineral density, but also age and body mass index (see FRAX website).
Service delivery
The future delivery of menopause services should be both horizontally and vertically integrated. Vertically, in that care of the menopause patient should be in close liaison between primary, secondary, and tertiary care. Horizontally, in that care within specialist units should be multidisciplinary where patients can be cared for not only by menopause specialists but also by other affiliated specialists such as breast cancer surgeons, cardiovascular physicians, psychologists, dieticians, and nurse specialists. This is particularly important in units that look after women with premature ovarian failure and complex medical problems. Guidelines for care of menopause patients should be drawn up in collaboration with local Primary Care Trusts and key primary care specialists, in order to provide a universally high standard of management for all menopausal patients. Currently, services are threatened by lack of inclusion of menopause/HRT/osteoporosis in the new GP contract and limitation of new to follow-up ratios. Interventions
Lifestyle measures
Every woman should be encouraged to take plenty of regular exercise in addition to having a well-balanced diet and to avoid smoking. Data suggest that women who are more active tend to suffer less from the symptoms of the menopause. Not all types of activity lead to an improvement in symptoms. High impact infrequent exercise can actually make symptoms worse; the best activity is aerobic sustained regular exercise. Women who take regular weight-bearing exercise have higher bone mineral densities than sedentary controls. Exercise appears to reduce bone loss rather than reverse osteoporosis. It also improves muscle tone thus reducing falls. There is also evidence for reduction in bone loss by the daily use of calcium (approximately 1500 mg elemental calcium) and vitamin D (400–600 IU) supplements. Avoidance or reduction of intake of alcohol and caffeine can reduce the severity and frequency of vasomotor symptoms. In view of the rise in insulin resistance during the menopause transition, it is advisable that a low glycaemic index/load diet is instituted if weight gain is a problem.
Hormone therapy regimens
Dosage of oestrogen
There is general agreement now that we should be starting with the minimum effective dose of oestradiol and increasing the dose if needed to alleviate symptoms. Although there is no direct evidence that higher doses of exogenous oestrogen are associated with increased risk of breast cancer or heart disease, there is a link with venous thromboembolic risk. Importantly, lower doses of oestrogen are less likely to produce breast tenderness and bleeding problems (less endometrial stimulation), which will reduce continuance of therapy.
The dosages of currently available systemic oestrogen are as follows:
• 0.3–0.625 mg of oral conjugated equine oestrogens
• 1 mg of oral micronized oestradiol or oestradiol valerate
• 25–50 μg transdermal oestradiol
• 25–50 mg of implanted oestradiol.
Recent data suggest that the benefits of a 1-mg dose of oestradiol for symptoms and bone protection can be achieved with a 0.5 mg dose. Exceptions to this ‘low dose rule’ are women who suffer premature ovarian failure, who need higher doses of oestrogen to reproduce the physiological hormone levels which would have been present if the ovaries had not failed early. Sadly, very little work has been carried out to determine what the optimum route of administration or dosage is in this group of young women. The author of this section aims to set up a working group with the Royal College of Obstetricians and Gynaecologists to study this neglected area.
Route of administration
If we adhere to the principle that we should try to reproduce the most physiological state possible with a 2:1 oestradiol–oestrone ratio, then we should avoid the oral route altogether. Oral oestradiol preparations are partially metabolized to oestrone by hepatic first-pass metabolism and therefore do not fully restore this ratio. There are twice weekly or once weekly transdermal systems containing both oestrogen and progestogen that can be used either sequentially or as continuous combined HRT. The hormone is adsorbed onto the adhesive matrix, which avoids the skin reactions caused by the old alcohol reservoir patches. Oestradiol is also available as a low volume daily transdermal gel and work is ongoing to produce an oral tab/wafer that maintains the ease of oral administration while absorption avoids first-pass metabolism.
Local (vaginal) oestrogen
Recently developed vaginal HRT regimens have managed to avoid the problem of endometrial stimulation. Creams using oestriol do not produce endometrial hyperplasia and the 17β oestradiol vaginal tablet and silicone vaginal ring also provide effective relief of local symptoms without any significant endometrial effects. These preparations can be used without progestogenic opposition but are only licensed for 3 months use in the UK and 1 year in Europe. Options for local vaginal oestrogen are as follows:
• 0.01% oestriol cream and pessaries
• 0.1% oestriol cream
• 25 μg/24 hour oestradiol vaginal tablets
• 7.5 μg/24 hour oestradiol-releasing silicone ring
• Premarin cream (this preparation can potentially cause endometrial hyperplasia and should not be used without progestogenic opposition for more than 3 months).
Progestogens
Regimens
Oestrogen was originally used unopposed in non-hysterectomized women. It was noted that this led to endometrial hyperplasia in up to 30% of cases. Progestogen has therefore been added to oestrogen therapy for the last 30 years in order to avoid hyperplasia and carcinoma. It is generally accepted that women commencing HRT should start on a sequential regimen, i.e. continuous oestrogen with progestogen for 12–14 days per month. The typical dosages of the more commonly used progestogens are shown in Table 12.23.1.
Bleeding problems
If bleeding is heavy or erratic the dose of progestogen can be doubled or duration increased to 21 days. Persistent bleeding problems beyond 6 months warrant investigation with ultrasound scan and/or endometrial biopsy. After 1 year of therapy women can switch to a continuous combined regimen, which aims to give a bleed free HRT regimen and will also minimize the risk of endometrial hyperplasia. Alternatively, women can be switched to the tissue selective agent tibolone. With both these regimens there may be some erratic bleeding to begin with, but 90% of those that persist with this regimen will eventually be completely bleed free. If starting HRT de novo a bleed-free regimen can be used from the outset if the last menstrual period was over a year ago.
Table 12.23.1 Minimum doses of progestogen given orally in HRT as endometrial protection

Side-effects
It is vital that we maximize compliance if patients are to receive the full benefits from HRT. One of the main factors for reduced compliance is that of progestogen intolerance. Progestogens have a variety of effects apart from the one for which their use was intended, that of secretory transformation of the endometrium. Symptoms of fluid retention are produced by the sodium-retaining effect of the renin–aldosterone system, which is triggered by stimulation of the mineralocorticoid receptor. Androgenic side-effects such as acne and hirsuitism are a problem of the testosterone-derived progestogen due to stimulation of the androgen receptors. Mood swings and PMS-like side-effects result from stimulation of the central nervous system progesterone receptors.
Minimizing progestogen intolerance: the dose can be halved and duration of progestogen can be reduced to 7–10 days. However, this may result in bleeding problems and hyperplasia in a few cases (5–10%) so there should be a low threshold for performing ultrasound scans and endometrial sampling in these women. Natural progesterone has fewer side-effects due to progesterone receptor specificity and is now available in an oral micronized form, vaginal pessaries, and gel (Table 12.23.1). The levonorgestrel intrauterine system, recently granted a 4-year licence in the UK for progestogenic opposition, also minimizes systemic progestogenic side-effects by releasing the progestogen directly into the endometrium with low systemic levels. Drospirenone, a spironolactone analogue, has recently been incorporated with low-dose oestrogen in a continuous combined formulation. It is not only progesterone receptor specific but also has antiandrogenic and antimineralocorticoid properties, the former making it useful for hirsuitism and the latter for fluid retention. Also, it may have blood pressure-lowering effects. It is imperative that we continue to seek improved ways of administering the progestogens, which are important in protecting the endometrium in order to avoid progestogenic side-effects, and minimize effects on breast tissue, e.g. vaginal and intrauterine progestogens and natural progesterone. However, we still lack data about the risk of breast cancer in women using oestrogen with a levonorgestrel intrauterine system.
Risks of HRT
The Women’s Health Inititiative (WHI) and Million Women Study (MWS) studies have demonstrated an excess risk of cardiovascular disease, stroke, and breast cancer in women using combined oestrogen and progestogen HRT. However, these studies were heavily criticized because their design, particularly the WHI study, where the average age of recruitment was 63 years and with an excess of obesity, hypertension, and pre-existing cardiovascular disease leading to prothrombotic problems. In contrast, a recent subanalysis of the WHI has shown that the cardiovascular risks were confined to the oldest age group. The absolute excess risk of coronary heart disease per 10 000 person years was –2 for women aged 50–59 years at randomization, –1 for those who were 60–69 years, and it increased to +19 for those in the 70–79-year age group. This shows that women in the youngest cohort (typically seen in our clinics with menopausal symptoms) had a trend towards improvement of cardiovascular risk and significant reduction in all causes of mortality. Guidance issued by the International Menopause Society has emphasized that in the WHI study the risks of breast cancer did not become significant until 7 years of usage (approximately one extra case per 1000 women per annum); they stated that for women in the normal menopause transition, the benefits of HRT far outweigh the risks and may even confer cardiovascular benefits.
Testosterone preparations/regimens
For women with distressing low sexual desire and tiredness only 100-mg implanted testosterone pellets were licensed until recently. The realization that there was an unfilled niche in the market for female androgen replacement led to the development of the 300 μg per day testosterone transdermal system to treat ‘hypo sexual desire disorder’. The current licence for this product is in surgically menopausal women on concomitant oestrogen, but it is expected that licences will be granted for naturally menopausal women and women using testosterone without oestrogen. Unlicensed options include testosterone gel, which comes in 50 mg, 5-mL sachets, or tubes at a dose of 0.5–1.0 mL/day. In the author’s experience if the free androgen index is kept within the physiological range there are rarely any side-effects such as hirsutism. Levels can be checked at baseline and repeated at 4–6 weeks. Alternatives to this include scaled down dosages of testosterone injections and oral preparations, although many avoid the latter route because of hepatic concerns. Concerns regarding cardiovascular and breast cancer risks have not been realized in clinical studies.
Contraindications to HRT
HRT is contraindicated in women with a history of cardiovascular disease and stroke. Although contraindicated in venous thromboembolic disease, there is some evidence that transdermal preparations are safer by avoiding first-pass metabolism.
Natural oestrogens when given to normotensive or hypertensive women do not cause an elevation in blood pressure, and when given in combination with oral progesterone may actually lower blood pressure; therefore, there is no justification for withholding HRT from hypertensive women.
Fibroids are responsive to oestrogens, and involute after the menopause. HRT may continue to stimulate these benign tumours causing some to increase in size. This can produce an increase in menstrual blood loss, but in practice does not usually represent a problem as treatment can easily be discontinued. However, in patients with a good indication who wish to continue therapy, fibroid resection or a hysterectomy is a possible compromise.
Endometriosis which is stimulated by cyclical ovarian activity can cause considerable pain and many patients with severe disease may require hysterectomy, often with bilateral oophorectomy. Unfortunately, because of a fear of using oestrogens, the ovaries are often conserved at operation and continue to stimulate the endometriosis causing continued pain in these women. Approximately 50% of women will continue to have pain until all ovarian tissue is removed, after which continuous oestrogen may be administered with a reduced risk of recurrence of endometriosis. In cases where the endometriosis has been severe and complete clearance may not have been achieved, it may be sensible to give low-dose continuous combined HRT or tibolone to reduce the risk of recurrence.
Treatment of patients with a past history of endometrial cancer is controversial, but there are reports of oestrogen use without any detrimental effects in stage I–III disease. Squamous cervical cancer is not oestrogen sensitive. There are no adverse data in ovarian cancer survivors, although there may be a very small increased risk of ovarian cancer with long-term unopposed oestrogen use in healthy women. There are no data for adenocarcinoma of the cervix, vaginal, or vulval cancer.
Breast cancer must be regarded as the principal contraindication to oestrogen treatment, but high-risk women with a strong family history of breast malignancy or those with benign breast disease should not necessarily be denied treatment. It is unclear what the precise risk of breast cancer recurrence is with HRT use. A study in breast cancer survivors using HRT was terminated because of an apparent excess risk. Unfortunately, this led to the premature termination of two other studies running concomitantly in which no excess risk had been detected. A large randomized placebo-controlled study (LIBERATE) in breast cancer survivors using tibolone recently demonstrated a marginal increase in recurrence rates (RR 1.4).
Duration of therapy
It is recognized that symptoms often return when HRT is ceased, even after many years of use. If the underpinning principle of HRT is that it should be used to improve and maintain a good quality of life, in women in whom this principle is maintained it is difficult to argue that they should have arbitrary deadlines imposed on them. Although breast cancer risks appear to be duration dependent, evidence suggests that overall mortality is actually reduced in women commencing HRT before the age of 60. Thus, duration of therapy requires careful judgement of benefits and risks on an individual basis. If therapy is to be discontinued, the dose should be reduced in a stepwise fashion over a minimum of 6 months to reduce the risk of immediate severe symptom resurgence.
Official prescribing advice
How are health professionals supposed to react to these data and advise their patients? Guidance from the Medicine’s & Healthcare Products Regulatory Agency (see website) has advised that HRT should not be recommended for primary or secondary prevention of heart disease. This advice is mirrored by the European Medicine’s Agency (see website) and by the North American Menopause Society (NAMS position paper). It is recommended that HRT be used merely for symptom relief in the short term at the lowest effective dose and alternatives should be considered in the long term for prevention of osteoporosis. Annual reappraisal of HRT use should be carried out with weighing up of the pros and cons on an individual basis. However, the British Menopause Society (see website) consensus statement advises that prescribing habits need not be changed by the recent studies because HRT use in the UK was primarily for symptom relief anyway rather than primary or secondary prevention. Similar statements were made by the European and International Menopause Societies (see websites).
Complementary therapies/alternatives to HRT
The concern from the recent studies regarding the risks of HRT has led to an increasing demand for alternatives to HRT for the management of menopausal symptoms. There is little scientific evidence that complementary and alternative therapies can help menopausal symptoms or provide the same benefits as conventional therapies. Yet many women use them, believing them to be safer and ‘more natural’, especially following the current controversies regarding HRT. The choice of treatments is confusing and, unlike conventional medicines, not much is known about their active ingredients, safety or side-effects, or how they may interact with other therapies. They can interfere with warfarin, antidepressants, and anti-epileptics with potentially fatal consequences. Some herbal preparations may contain oestrogenic compounds and this is of concern for women with hormone-dependent disease such as breast cancer. There is also concern about contaminants such as mercury, arsenic, lead, and pesticides. Legislation is soon to be introduced which will make it mandatory for herbal preparations to at least be registered with the MHRA. This will at least allow some control over what is being sold over the counter, which currently may be completely ineffective or dangerous. It is essential that alternatives to licensed preparations should be judged by similar standards.

Fig. 12.23.1 Vasomotor treatment algorithm: a conservative, clinical approach.
An integrated approach to the management of vasomotor symptoms should be considered in women wanting to consider alternatives to (or contraindicated to) HRT. An algorithm drawn up by a consensus group of international experts integrating lifestyle, complementary, and pharmacological interventions is shown below (Fig. 12.23.1). Lifestyle changes and supplements such as red clover and soy isoflavones and other alternatives can be incorporated into the routine management of women with vasomotor symptoms. In conjunction with the algorithm a five-step approach is suggested:
• initial patient consultation and general health assessment
• establishment of menopause as basis of symptoms, i.e. exclusion of other conditions
• discussion of all symptom management options from very outset
• patient asked to self-rate her symptom severity
• management choice individualized based on symptom severity.
The algorithm is not intended for women with premature menopause or for those with other risk factors such as osteoporosis. It should also be remembered that certain groups of women may have contraindications to the use of complementary therapies. For instance, some women may have intolerance to soy or lignans. High-dose isoflavones should probably be avoided in breast cancer sufferers; also, those with low libido could have a deterioration due to reduction in free testosterone via SHBG. Finally, if complementary therapies have been ineffective and traditional HRT has been started there is little reason to continue the original product as this is unlikely to have an additive effect and may even interfere with the efficacy of exogenously administered hormones.
Non-pharmacological alternatives (Rees and Panay 2006) Gels for vaginal symptoms
Replens: this vaginal bioadhesive moisturizer is a more physiological way of replacing vaginal secretions than with lubricant vaginal gels such as KY jelly. It actually rehydrates the tissues and provides a reasonable alternative to systemic or vaginal HRT.
Pharmacological alternatives
α-2 agonists
Clonidine, a centrally active α-2 agonist, has been one of the most popular alternative preparations for the treatment of vasomotor symptoms. A recent meta-analysis of the few randomized controlled trials has shown a marginal benefit of clonidine over placebo.
Selective serotonin reuptake inhibitors SSRIs/noradrenaline reuptake inhibitors SNRIs
A significant amount of evidence exists for the efficacy of SSRIs and SNRIs in the treatment of vasomotor symptoms. Although there are some data for SSRIs such as fluoxetine and paroxetine, the most convincing data are for the SNRI (venlafaxine) at a dose of 37.5 mg bd. The key effect with these preparations appears to be stimulation of the noradrenergic as opposed to the serotonergic pathways, hence the preferential effect of SNRIs. The trials demonstrate a 50–60% reduction in hot flush frequency and severity. The main drawback with these preparations (especially the SNRIs) is the high incidence of nausea, which often leads to withdrawal from therapy before maximum efficacy has been achieved.
Gabapentin
Recent work with the antiepileptic drug gabapentin has shown efficacy for hot flush reduction compared with placebo. In a recent study using gabapentin at a dose of 900 mg per day, a 45% reduction of hot flush frequency and a 54% reduction of symptom severity was demonstrated. Further work is being conducted to confirm the efficacy and safety of this preparation but for the moment its use is restricted to specialist centres. Once again, its use is limited by the frequency of often severe side-effects.
Complementary therapies: phytoestrogens
Phytoestrogens are plant substances that have effects similar to those of oestrogens. Since the first discovery of the oestrogenic activity of plant compounds, over 300 plants have been found to have phytoestrogenic activity. Preparations vary from enriched foods such as bread or drinks (soy milk) to more concentrated tablets. The most important groups are called isoflavones and lignans. The major isoflavones are genistein and daidzein. The major lignans are enterolactone and enterodiol. Isoflavones are found in soybeans, chick peas, red clover, and probably other legumes (beans and peas). Oilseeds such as flaxseed are rich in lignans, and they are also found in cereal bran, whole cereals, vegetables, legumes, and fruit. The role of phytoestrogens has stimulated considerable interest since populations, such as the Japanese, consuming a diet high in isoflavones appear to have lower rates of menopausal vasomotor symptoms, cardiovascular disease, osteoporosis, and breast, colon, endometrial, and ovarian cancers. The normal Japanese diet contains 200 mg of phytoestrogens per day compared with the average Western diet, which contains less than 1 mg. However, epidemiological studies need to be supported by data, with analyses of the isoflavone content of foods and measures of their bioavailability. The evidence from randomized placebo-controlled trials in Western populations is conflicting for both soy and derivatives from red clover, with marginal benefits demonstrated in meta-analyses of randomized trials. Similarly, there are also debates about the effects on breast cancer, lipoproteins, endothelial function, and blood pressure. Currently other studies are under way, including a European Union study (Phytos—see website), which should help quantify the relative importance and optimal doses for symptom relief, bone preserving effects, and safety. Conclusion
Effective management of the menopause is taking on ever-increasing importance in view of our ageing population. The overzealous reporting of recent clinical trials has made it imperative that physicians involved in this area can access well-balanced evidence-based information. In the author’s opinion, current best practice should involve the following:
• discussion of lifestyle measures, HRT, and alternatives should take place from the outset.
• management should be individualized taking into account risks and benefits.
• the main indication for use of HRT should be for symptom relief rather than for prevention of long-term problems
• low-dose HRT should usually be commenced and increased if necessary to achieve effective symptom relief, except in premature ovarian failure where higher doses are physiological.
• androgen therapy should be considered in women with persistent low libido and energy levels
• rigid cut offs in the duration of therapy should be avoided, with regular reappraisal (at least annual) of the benefits and risks for each individual
• delivery of services should be from a multidisciplinary team if possible with close liaison with allied specialties and experts.
It is unlikely that the ultimate menopause therapy which truly has all the benefits without any side-effects and risks will ever be developed. Clinicians should therefore aim to provide the best evidence-based advice possible in order to allow women to make an informed choice about how to manage their menopause transition and beyond. Further reading
Bjarnason NH. Postmenopausal bone remodelling and hormone replacement. Climacteric 1998;1:72–9.
Christian RC, Harrington S., Edwards WD, et al. Estrogen status correlates with the calcium content of coronary atherosclerotic plaques in women. J Clin Endocrinol Metab 2002;87:1062–7.
Davis SR, Moreau M, Kroll R, et al. Testosterone for low libido in postmenopausal women not taking estrogen. N Engl J Med 2008;359:2005–17.
Davison SL, Bell R, Donath S, et al. Androgen Levels in Adult Females: changes with Age, Menopause and Oophorectomy. J Clin Endocrinol Metab 2005;90:3847–53.
Kalu E, Panay N. Spontaneous premature ovarian failure: management challenges. Gynecol Endocrinol 2008;24:273–9.
Kenemans P, Bundred NJ, Foidart JM, et al. Safety and efficacy of tibolone in breast-cancer patients with vasomotor symptoms: a double-blind, randomised, non-inferiority trial. Lancet Oncol 2009;10:135–46.
Landgren BM, Collins A, Csemiczky G, et al. Menopause transition: annual changes in serum hormonal patterns over the menstrual cycle in women during a 9 year period prior to menopause. J Clin Endocrinol Metab 2004;89:2763–9.
Lindh-Astrand L, Nedstrand E, Wyon Y, Hammar M. Vasomotor symptoms and quality of life in previously sedentary postmenopausal women randomised to physical activity or estrogen therapy. Maturitas 2004;48:97–105.
Loprinzi CL, Kugler JW, Sloan JA, et al. Venlafaxine in the management of hot flashes in survivors of breast cancer: a randomised controlled trial Lancet 2000;356:2059–63.
Million Women Study Collaborators. Breast cancer and HRT in the Million Women Study. Lancet 2003;362:419–27.
Muscat Baron Y, Brincat MP, Galea R, Calleja N. Low intervertebral disc height in postmenopausal women with osteoporotic vertebral fractures compared to hormone-treated and untreated postmenopausal women and premenopausal women without fractures. Climacteric 2007;10:314–9.
Nardo LG, Christodoulou D, Gould D, et al. Anti-Müllerian hormone levels and antral follicle count in women enrolled in in vitro fertilization cycles: relationship to lifestyle factors, chronological age and reproductive history. Gynecol Endocrinol 2007;24:1–8.
Nelson HD, Vesco KK, Haney, et al. Non-hormonal therapies for menopausal hot flashes: systematic review and meta–analysis. JAMA 2006;295:2057–71.
Panay N Fenton A. The role of testosterone in women. Climacteric 2009;12:185–7
Panay N, Fenton A. Premature ovarian failure: a growing concern. Climacteric 2008;11:1–3.
Panay N, Studd JWW. Progestogen intolerance and compliance with hormone replacement therapy in menopausal women. Hum Reprod Update 1997;3:159–71.
Panay N, Studd JWW. The psychotherapeutic effects of estrogens Gynaecol Endocrinol 1998;12:353–65.
Panay N, Ylikorkala O, Archer DF, et al. Ultra low-dose estradiol and norethisterone acetate: effective menopausal symptom relief. Climacteric 2007;10:120–31.
Panay N. Integrating phytoestrogens with prescription medicines–A conservative clinical approach to vasomotor symptom management. Maturitas 2007;57:90–4.
Pines A, Sturdee DW, Birkhauser MH, et al. IMS Updated Recommendations on postmenopausal HRT. Climacteric 2007;10:181–94.
Powles TJ, Howell A, Evans DG, et al. Red Clover Isoflavones are safe and well tolerated in women with a family history of breast cancer. Menopause Int 2008;14:6–12.
Rees M, Mander A (eds) Managing the menopause without oestrogen. London: RSM Press 2004.
Rees M, Purdie D (eds). Management of the menopause: the handbook, 4th edn. London: RSM Press 2006.
Rees M., Panay N. The use of alternatives to HRT for the Management of menopause symptoms RCOG Scientific Advisory Committee 2006; Opinion Paper 6.
Rossouw JE, Prentice RL, Manson JE, et al. Postmenopausal hormone therapy and risk of cardiovascular disease by age and years since menopause. JAMA 2007;297:1465–77.
Salpeter SR, Walsh JM, Greyber E., et al. Mortality associated with hormone replacement therapy in younger and older women: a meta-analysis. J Gen Intern Med 2004;19:791–804.
Scarabin PY, Olger E, Plu-Bureau G. Differential association of oral and transdermal oestrogen replacement therapy with venous thromboembolism risk. Lancet 2003;362:428–32.
Shumaker SA, Legault C, Rapp SR, et al. Estrogen plus progestin and the incidence of dementia and mild cognitive impairment in postmenopausal women: the Women’s Health Initiative Memory Study: a randomized controlled study. JAMA 2003;289:2651–62.
Singer D, Hunter M (eds). Premature menopause: a multidisciplinary approach. London: WileyBlackwell.
Thompson Coon J, Pittler MH, Ernst E. The role of red clover (Trifolium pratense) isoflavones in women’s reproductive health: a systematic review and meta-analysis of randomised clinical trials. Focus Altern Complement Ther 2003; 8: 544.
Tunstall-Pedoe H. Myth and paradox of coronary risk and the menopause. Lancet 1998;351:1425–7.
Writing Group for the Women’s Health Initiative Investigators.
Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results From Women’s Health Initiative randomized controlled trial. JAMA 2002;288:321–33. Internet resources
British Menopause Society site—see consensus statements: www.the-bms.org
International Menopause Society—see consensus statements: www.imsociety.org
European Menopause Society: http://emas.obgyn.net/
The medical and Healthcare Products Regulatory Agency: www.mhra.gov.uk
WHO osteoporosis fracture risk calculator: www.shef.ac.uk/FRAX/
National Osteoporosis Society—professionals and patients: www.nos.org.uk
North American Menopause Society: www.menopause.org
European Medicines Agency: www.emea.eu.int/
National Centre for Complementary and Alternative Medicine. Alternative therapies for managing menopausal symptoms: http://nccam.nih.gov/health/alerts/menopause/
The PHYTOHEALTH Network aims to establish a pan-European network of institutions dealing with safety and health effect of phytoestrogens, identification of optimal sources and processing technologies: www.phytohealth.org
The NIH Office of Dietary Supplements: http://dietary-supplements. info.nih.gov
Women’s Health Initiative Website: www.whi.org
Royal College of Physicians Guidelines on Osteoporosis: www.rcplondon.ac.uk/pubs/wp_osteo_update.htm Patient resources
Informative menopause website: www.menopausematters.co.uk
Premenstrual Syndrome website: www.pms.org.uk
National Osteoporosis Society—professionals and patients: www.nos.org.uk
Women’s Health Group—including ‘ask the experts’: www.womens-health-concern.org/
Menorrhagia Definition
Menorrhagia may be defined as heavy menstrual bleeding over several cycles. The traditional, objective, definition of menorrhagia is of menstrual blood loss of 80 mL or more per cycle. Measured blood loss has been shown to have little correlation with women’s own perceptions of bleeding heaviness and so the clinical definition typically used is that of excessively heavy bleeding for an individual.
In practice, any blood loss that is perceived by a woman to be excessive or as having a negative impact on her quality of life warrants counselling and possibly treatment. Epidemiology
Prevalence rates for menorrhagia of between 4% and 51% in women of reproductive years have been reported from around the world. This reflects the variety of definitions in use for the condition, the subjective nature of its reporting, and cultural differences in how bleeding is perceived. Evidence also suggests that increasing age is a risk factor for menorrhagia.
In fact, the majority of women will experience menstrual bleeding which they consider excessive at some time in their life, although this may be short-lived and self-limiting. In the UK, menorrhagia accounts for 12% of all gynaecology referrals. Pathology
In approximately half of women presenting with menorrhagia no pathological cause will be found and their loss is therefore ‘unexplained’.
Common causes include those listed below.
• Fibroids: uterine leiomyomas (fibroids) are common benign tumours of the myometrium, occurring in approximately 20% of women of reproductive age. They are associated with increased menstrual blood loss in approximately one-third of cases, with submucous fibroids distorting the uterine cavity particularly implicated. Despite this association, the presence of fibroids in a woman presenting with menorrhagia should not be assumed to be causative. In particular small intramural or subserosal fibroids may be a purely incidental finding.
• Endometrial polyps: focal overgrowth of endometrial glands and stroma to form polyps are a cause of menorrhagia, particularly in older women.
• Endometrial hyperplasia and carcinoma: malignant and premalignant conditions may present with menorrhagia, although the presence of other symptoms such as intermenstrual bleeding may increase suspicion. The major risk factor is age, with others being related to increased oestrogenic stimulation of the endometrium, e.g. obesity, polycystic ovary syndrome, and tamoxifen therapy. Simple and complex hyperplasia carries a 1–3% risk of potential malignant change and with atypical hyperplasia the risk is approximately 20% (Table 12.24.1).
• Coagulation disorders and iatrogenic anticoagulation: conditions such as von Willebrand disease and platelet disorders as well as treatment, especially at therapeutic doses with heparin or warfarin are associated with menorrhagia.
• Medical conditions: it is thought that most chronic illness can lead to menstrual disturbance. Specific associations with menorrhagia include hypothyroidism, systemic lupus erythematosus and liver disease (Table 12.24.2).
Table 12.24.1 Risk factors for endometrial carcinoma

• Dysfunctional uterine bleeding: this is excessive uterine bleeding that is not due to demonstrable pelvic pathology, complications of pregnancy, or systemic disease. It includes heavy bleeding due to the non-ovulatory cycles, which occur at the extremes of reproductive life, around menarche and in the perimenopause, the latter being the commonest time for women to present with menorrhagia. Dysfunctional uterine bleeding is a diagnosis of exclusion. The causes of abnormal uterine bleeding can be classified as pelvic, systemic or functional (see Table 12.24.3). Prognosis
Prognosis is good and women can expect a significant improvement in their quality of life with appropriate management. However, it may prove more challenging to find effective treatments for those currently wishing to conceive or to preserve their fertility, as well as for those with underlying medical conditions (Table 12.24.2). Clinical approach
Diagnosis
History, examination, and investigations should be directed towards identifying the cause and severity of menorrhagia in order to plan appropriate treatment.
History
Points to note are listed below.
Table 12.24.2 Medical disorders associated with menorrhagia

• The pattern and nature of the bleeding. The use of a menstrual calendar and questions focused on the type and frequency of changing of sanitary products, and a measure of how day-to-day activities are disturbed may be helpful.
Table 12.24.3 Causes of abnormal uterine bleeding

• The presence of associated symptoms such as intermenstrual or post-coital bleeding and abdominal or pelvic pain and pressure impact on quality of life.
• Last menstrual period and exclusion of pregnancy.
• Risk factors for endometrial carcinoma.
• Background gynaecological history, e.g. smear tests, contraception.
• Obstetric history and whether family is complete.
• General medical, surgical and drug history.
The taking of a good history should involve an exploration of the patients concerns and their aims and expectations, having sought medical help.
Examination
• General examination for signs of anaemia or thyroid disease.
• Abdominal examination to exclude a palpable fibroid uterus.
• Inspection of the genital tract including the cervix should be performed. Bimanual pelvic examination allows assessment of uterine size, mobility, tenderness, or adnexal masses.
Quantification of menstrual blood loss
Objective methods for the quantification of menstrual bleeding have been described such as the alkaline haematin method, involving the chemical extraction of haemoglobin from sanitary pads. These are no longer seen to have clinical relevance, with the emphasis now being on improving quality of life for any woman who feels her periods are problematic.
There remains a role for aids to women’s own assessments of blood loss such as pictorial blood loss assessment charts and menstrual calendars.
Investigations
The majority of patients do not require the full range of investigations for menorrhagia, as described below. Relevant tests should be carefully selected based on the history and examination findings in order to avoid unnecessary intervention and anxiety and to prevent delays in treatment.
Blood tests
A full blood count should be performed in all women with menorrhagia requiring investigation.
Serum ferritin should not be performed routinely but only where there is uncertainty as to the nature of any anaemia.
Thyroid function tests should only be performed where there are specific signs or symptoms of thyroid disease.
Testing for von Willebrand disease or other coagulation disorders should only be performed in cases where there is a history of menorrhagia from menarche or relevant family history.
A hormone profile has not been shown to be of benefit.
Assessment of the uterus and endometrium
This is required when the history and examination suggest significant structural or histological abnormalities. For example, where there is a palpable uterus or a pelvic mass, there are features suggestive of endometrial carcinoma or significant risk factors such as age over 45 years. In addition, endometrial assessment may be indicated in cases of persistent menorrhagia and failure of initial treatment.
Assessment may be by
• ultrasound
• endometrial biopsy
• hysteroscopy.
Each may be used alone or in conjunction with the other modalities. Particular methods are better at identifying particular pathologies and the choice of which tools to use will depend upon the individual presentation.
• Ultrasound: this is the first line modality for the investigation of structural abnormalities and is particularly useful for the identification and localization of fibroids. Transvaginal scanning has advantages over transabdominal scanning for the normally sized uterus. Ultrasound measurement of endometrial thickness to exclude endometrial carcinoma is of less benefit in the premenopausal woman.
• Endometrial biopsy: this must be performed where there is suspicion of histological abnormality, as described above. The pipelle endometrial sampler has become the generally accepted device for outpatient sampling. Although there is some evidence to suggest that it has comparable sensitivity for the diagnosis of endometrial carcinoma as hysteroscopically directed biopsy, concerns remain over the risk of missing serious pathology with such ‘blind’ sampling techniques. It also is ineffective in the removal of polyps.
• Hysteroscopy: Traditionally the ‘gold standard’ investigation for abnormal bleeding and suspected endometrial carcinoma, its role has been replaced in many circumstances by transvaginal ultrasound and pipelle biopsy. However, hysteroscopy remains superior to ultrasound for the detection of endometrial polyps and allows directed biopsy of suspicious lesions, although it is associated with greater patient discomfort. Furthermore, modern techniques and miniaturized scopes have led to outpatient hysteroscopy clinics, with no need for general anaesthetic and greater patient acceptability. Hysteroscopy may also be therapeutic, with treatment to polyps, submucous fibroids or endometrial ablation possible.
Management
There are a wide variety of treatments available for menorrhagia. The woman should be an active participant in deciding management and ample time should be provided for her to make appropriate choices. High standards of communication and counselling, supported by evidence-based information are essential to allow women to make informed decisions.
Counselling
For some women simple reassurance regarding the nature of their bleeding is sufficient and no other intervention may be necessary. Specific advice that no malignancy or other serious pathology is present is often welcome
Conservative/non-medical
If the patient is coping with her menstrual loss and declines any therapeutic intervention, she can be safely discharged. Advice about ensuring adequate iron intake and the offer of review, if required, is typically all that is needed.
Medical
Recent guidelines from the National Institute for Health and Clinical Excellence have suggested that pharmaceutical therapies are considered in the order below.
First line
• Levonorgestrel-releasing intrauterine system: the slow release of progestogen prevents proliferation of the endometrium, thereby reducing menstrual blood loss. The device is also contraceptive. Following its removal fertility returns to baseline levels quickly. Side-effects may include persistent irregular bleeding together with headaches, breast tenderness, and acne, which are generally mild and transient.
Second line
• Tranexamic acid: these oral antifibrinolytic tablets help to reduce menstrual flow. They can be commenced while appropriate investigations are performed. Improvement in symptoms would be expected within three cycles. Tranexamic acid has no impact on fertility. Minor side-effects include indigestion, diarrhoea, and headache.
• Non-steroidal anti-inflammatory drugs: this group of oral medications reduce prostaglandin production. They can be used in conjunction with tranexamic acid and can also be commenced while investigations are being undertaken. Improvement in symptoms should be seen within three cycles. They are especially useful when menorrhagia and dysmenorrhoea coexist. Non-steroidal anti-inflammatory drugs are not contraceptive. Women may experience side-effects of indigestion and diarrhoea. Asthma may be exacerbated in sensitive women and gastritis may progress to peptic ulcer disease with its associated risks of gastrointestinal bleeding, perforation, and peritonitis.
• Combined oral contraceptives: as well as providing contraception, combined oral contraceptives also reduce menstrual loss by preventing proliferation of the endometrium. Fertility levels will return to baseline within a short time after discontinuation. Women on the combined oral contraceptive have an increased risk of venous thromboembolism, cerebrovascular accident and myocardial infarction.
Third line
• Oral progestogen: oral progestogens prevent proliferation of the endometrium. The recommended regime of norethisterone 15 mg daily from days 5 to 26 is not contraceptive but may adversely affect the woman’s ability to conceive. Common side-effects of oral progestogens include weight gain, bloating, breast tenderness, headaches, and acne.
• Injected progestogen: injected progestogens also prevent proliferation of the endometrium. They are contraceptive and there may be a delay in return of fertility once injections cease. Injections are usually administered every 12 weeks. The side-effects are similar to oral progestogens. Long-term use can be associated with bone mineral density loss.
Fourth line
• Gonadotrophin-releasing hormone analogue: the production of oestrogen and progesterone is stopped by gonadotrophin-releasing hormone analogues, thereby inducing a temporary menopause and associated amen-orrhoea. Common side-effects are those of the climacteric: hot flushes, increased sweating, and vaginal dryness. If used for greater than 6 months, add-back hormone replacement therapy is recommended to reduce the risk of osteoporosis.
Surgical and radiological
• Endometrial ablation: various techniques are now available to destroy the endometrium and thereby reduce or cease menstrual blood loss. They include the first-generation techniques of transcervical resection of the endometrium. Second-generation techniques include microwave, balloon thermal, and impedance-controlled bipolar radiofrequency ablation. Appropriate patient selection is vital: women should have no fertility desires, a uterus no greater than 10-week pregnant size, no fibroids or fibroids less than 3 cm, and no histological abnormalities of the endometrium. The procedure itself is not contraceptive but pregnancy following endometrial ablation is likely to have a poor outcome, hence effective ongoing contraception is vital. The potential intraoperative complication of uterine perforation is rare and the risk is reduced further with the second generation techniques. Women may experience vaginal discharge post endometrial ablation and increased symptoms of dysmenorrhoea, even when rendered amenorrhoeic.
• Uterine artery embolization: this interventional radiology technique is suitable for women with fibroids greater than 3 cm. Small particles are injected into the uterine arteries, which shrink the fibroids by reducing their blood supply. It is particularly useful for women who are experiencing pain and pressure symptoms associated with fibroids. This technique is likely to preserve fertility, although long-term data are limited. Persistent vaginal discharge is not uncommon post-uterine artery embolization. Women may experience pain, nausea, vomiting. and fever: the post-embolization syndrome. Rarely there may be non-target embolization resulting in tissue necrosis, haemorrhage, and infection leading to septicaemia or ovarian failure.
• MRI-guided focused ultrasound: in research trials this technique is reported to be successful in reducing unacceptable menstrual flow, especially in combination with pretreatment downregulation with gonadotrophin-releasing hormone analogue therapy.
• Hysteroscopic myomectomy: submucous fibroids can be resected hysteroscopically. The procedure preserves fertility, although intrauterine adhesions can occur postoperatively, which may impair fertility. The size of the fibroids to be resected can be reduced with preoperative use of gonadotropin-releasing hormone (GnRH) analogues. If ongoing fertility is not desired, the remaining areas of endometrium can also be resected at the same procedure. Intraoperative uterine perforation, fluid overload, and postoperative infection or fibroid recurrence (especially those fibroids with a significant intramural element) are recognized unwanted outcomes.
• Myomectomy: fibroids can be removed abdominally by either open or laparoscopic procedures. Fibroid size can be reduced preoperatively with GnRH analogues. Once again fertility is theoretically preserved but the development of postoperative pelvic adhesions adversely affects tubal functions and compromises future fertility. A myomectomy in which the uterine cavity is breached perioperatively would normally lead to the recommendation that any future successful pregnancies should be delivered by elective Caesarean section.
• Hysterectomy: previously the most common procedure performed for menorrhagia, hysterectomy is becoming increasingly uncommon due to advances in medical and alternative surgical treatments. Vaginal hysterectomy is recommended as the first-line procedure, although the route of hysterectomy must be personalized for each woman. Healthy ovaries from premenopausal women should not be removed. The surgical complications of hysterectomy include infection, haemorrhage, urinary tract or bowel injury, postoperative urinary dysfunction, and venous thromboembolism.
Complications/side-effects/sequelae
Prior to embarking on treatment for menorrhagia, it is important to explore a woman’s expectations of treatment: amenorrhoea may be the perfect result for one woman but psychologically distressing for others. Relevant complications and side-effects for each treatment modality are outlined above.
Follow up/recurrence/future pregnancy planning
Some women will progress through the various treatments for menorrhagia before finally requiring a hysterectomy. However, for the majority of women, long-term relief from their menorrhagia will be provided by a levonorgestrel-releasing intrauterine system. This device needs to be changed every 5 years. It can also be used for endometrial protection for women taking oestrogen hormone replacement therapy. Hence, a device fitted for management of perimenopausal menorrhagia may have uses beyond its initial indication.
Women with menorrhagia who are currently trying to conceive have limited treatment options. In addition, those women whose symptoms do not resolve with pharmacological methods may have to consider treatments which may adversely affect their future fertility. Therefore, the importance of exploring a woman’s reproductive plans prior to commencing treatment is vital. Further reading
National Collaborating Centre for Women’s and Children’s Health. Heavy menstrual bleeding. Clinical Guideline. London: NICE 2007. Internet resources
www.nice.org.uk
www.bnf.org
www.novasure.com/
www.microsulis.co.uk/ Patient resources
Fibroid Network, info@fibroid.co.uk, www.fibroidnetwork online.com
The Hysterectomy Association, 0871 7811141, www.hysterectomy-association.org.uk
Women’s Health Concern, 0845 123 2319, www.womens-health-concern.org
Menstrual cycle: physiology Introduction
The normal menstrual cycle can vary considerably between women and may range in length from 25 to 35 days. A woman’s menstrual cycle pattern relies on a complex interaction of hormones exerted via her hypothalamic-pituitary-ovarian axis. The menstrual cycle
Classically the 28-day menstrual cycle is used because it splits neatly into two halves, defined by the follicular and endometrial changes that occur before and after ovulation. Ovulation may still occur in cycles that are 25–35 days in length.
The first half of the cycle is marked by the start of bleeding on day 1 of the cycle. The ‘proliferative phase’ follows this as endometrial thickness increases under the influence of oestrogen secretion. This stage is also termed the ‘follicular phase’ because ovarian follicles begin to develop and mature in preparation for ovulation.
The second half of the cycle commences once ovulation has taken place. The ‘secretory phase’ describes the endometrial changes that take place in preparation for implantation of a fertilized egg. This stage is also termed the ‘luteal phase’, as the corpus luteum, left behind after ovulation, provides hormonal support to an early pregnancy. Endocrinology
Several key hormones regulate the ovarian and endometrial changes during each cycle:
• gonadotrophin releasing hormone (GnRH)
• follicle-stimulating hormone (FSH)
• luteinizing hormone (LH)
• oestrogen
• progesterone.
The hypothalamus secretes GnRH in a pulsatile manner, and this stimulates the anterior pituitary to release the gonadotrophins FSH and LH, which in turn trigger the release of oestrogen and progesterone from the ovary. Each hormone plays an important role in the course of a normal menstrual cycle. Follicular development
Follicular development within the ovary begins in early fetal life. ‘Primordial germ cells’ multiply by mitosis and differentiate to produce 7 000 000 ‘primordial follicles’ by 32 weeks’ gestation. Each primordial follicle contains a primary oocyte arrested in prophase of the first meiotic division. The primordial follicle remains in this state until menarche.
At birth the number of primordial follicles has fallen to 3 000 000 and by puberty only 40 0000 remain. At the onset of puberty 15–20 primordial follicles will differentiate into primary follicles with each menstrual cycle.
A primary follicle contains a primary oocyte surrounded by the zona pellucida and a single layer of granulosa cells. FSH induces proliferation of granulosa cells and up regulates FSH receptors to maximize this effect. LH drives the outer follicular thecal cells to differentiate into the ‘theca interna’ and ‘theca externa’. The normal menstrual cycle
Menarche is followed by 5–7 years period during which the menstral cycles tend to become shorter and more regular as an abitary pattern develops. The highest incidence of anovulatory cycles is below the age of 20 years and over the age of 40 years.
At age 25, over 40% of cycles are between 25 and 28 days in length. From 25–35, over 60% are between 25 and 28 days.
Approximately 5 years before the menopause, the menstrual cycle tends to lengthen again.
A normal menstrual period may last from 2 to 7 days and results in the loss of 30–40 mL of blood. Menstrual bleeding in excess of 80 mL per cycle is associated with iron deficiency anaemia. Endometrial cycle
Endometrium consists of two anatomical layers. The ‘lamina functionalis’ proliferates and is then shed each month in response to the rise and fall of oestrogen and progesterone levels. The ‘lamina basalis’ is unchanged but regenerates to provide the functionalis each month. Menstrual cycle phases
Assuming a 28-day cycle the endocrine and physiological changes that occur during the menstrual cycle can be understood conveniently in five phases.
These five phases apply in all normal cycles (25–35 days). Despite a changeable cycle length the ‘luteal phase’ remains fairly constant (13 ±1 day) and it is the ‘follicular phase’ that shortens and lengthens.
Early follicular phase (days 1–6)
• Menstruation signifies the start of the early follicular phase of the cycle as the ‘lamina functionalis’ is shed.
• Oestrogen and progesterone levels are low.
• Baseline FSH and LH levels rise with the influence of GnRH on the anterior pituitary.
• FSH triggers 15–20 primordial follicles to continue to grow and mature into multilaminar follicles.
Late follicular phase (days 7–14)
• Primordial follicles continue to develop into multilaminar follicles under the influence of FSH.
• FSH up regulates LH receptors on the granulosa cells.
• Granulosa cells proliferate under the influence of FSH to release oestradiol.
• Negative feedback at the pituitary level eventually causes FSH levels to fall.
• The rising oestrogen levels cause the lamina functionalis to proliferate from stem cells in the basalis layer and the endometrium thickens.
• The endometrium becomes more glandular.
Pre-ovulation and ovulation phase (days 13–14)
• The lamina functionalis and non-secretory glandular endometrium is at maximal thickness just prior to ovulation.
• High levels of oestrogen result in positive feedback at the pituitary causing a brief surge in LH and FSH levels.
• The dominant follicle, known as the graafian follicle, develops and completes the first meiotic division (Fig. 12.25.1).
• High LH levels are believed to be involved in ovulation
• At ovulation the secondary oocyte is expelled
• LH and FSH levels then return rapidly to baseline.

Fig. 12.25.1 A follicle on ultrasound scan (a) and at laparoscopy (b)
Early luteal phase (days 15–21)
• The granulosa and thecal cells of the dominant follicle left behind after ovulation form the corpus luteum (Fig. 12.25.2).
• Progesterone and to a lesser extent oestrogen are produced by the corpus luteum.
• Negative feedback by progesterone and oestrogen maintain FSH and LH at low levels
• The secretory endometrium forms as progesterone stimulates the secretion of glycogen, mucus and other substances.
Late luteal phase (days 22–28)
• The corpus luteum degenerates in the absence of fertilization.
• Falling oestrogen and progesterone levels remove the negative feedback effect on the pituitary gland and FSH and LH levels begin to rise
• The endometrium undergoes involution
• On days 25–26 the spiral arteries vasoconstrict
• This ischaemia causes apoptosis of the lamina functionalis and menstruation begins on or around day 28. Clinical approach: top tips
• Most ovulatory cycles are between 25 and 35 days.
• Menstrual cycles tend to have a relatively constant ‘luteal phase of 13–14 days. It is the ‘follicular phase’ that usually shortens or lengthens to produce the variability in cycle length.
• Progesterone causes a rise in body temperature of half a degree Celsius. Temperature will remain elevated if pregnancy occurs and will return to normal if not.
• Luteal phase progesterone peaks 7 days before menstruation. An elevated reading (at least 21 nmol/L and preferably 32 nmol/L or more) confirms ovulation in that cycle. Hence, to test for mid-luteal progesterone subtract 7 days from the cycle length. Example: in a 40-day cycle progesterone should be taken on day 33 (40–7 = 33)
• LH dipsticks can be used to detect ovulation based on the menstrual cycle changes and LH surge.
• Note that in women with polycystic ovarian syndrome endogenously high levels of LH may give a false-positive dipstick result.
• Endometrium that has not been oestrogen primed will not be capable of a withdrawal bleed following progestagen challenge. Hence, women with amenorrhoea secondary to polycystic ovarian syndrome will have normal oestrogen levels and a withdrawal bleed after a progestagen challenge.
• Women with amenorrhoea secondary to hyperprolactinaemia or the menopause will have low oestrogen levels and no withdrawal bleed after a progestagen challenge.
• There are two rare situations when oestrogen is adequate, but there is no withdrawal bleed. In both, the endometrium is decidualized, either due to high androgen levels or high progesterone levels due to a specific adrenal enzyme deficiency.

Fig. 12.25.2 A corpus luteum on ultrasound scan. Miscarriage: early Definition
Sporadic first trimester or early miscarriage is the commonest complication of pregnancy and is defined as a spontaneous loss of pregnancy up to 12 weeks’ gestation. The European Society for Human Reproduction Special Interest Group for Early Pregnancy has published a revised nomenclature to define early pregnancy loss to improve clarity and consistency the in definitions (Table 12.26.1). Epidemiology
Miscarriage occurs in 10–20% of clinical pregnancies (viable pregnancy defined by ultrasound examination) and is responsible for 50 000 inpatient admissions in the UK per annum (RCOG 2006). The chance of a subsequent successful pregnancy following one early miscarriage is over 95% and in women with three consecutive miscarriages is over 70%. Factors influencing the probability of a chromosomal aberration carrier status in women with sporadic miscarriages are maternal age at second miscarriage, a history of three or more miscarriages (recurrent miscarriage), and a history of over two miscarriages in the sibling or parents of either partner. The probability of carrier status in couples referred for chromosome analysis after two or more miscarriages varies between 0.5% and 10.2% and the chances of having a healthy child are as high as a non-carrier couple despite a higher risk of miscarriage (Franssen et al., 2006). Risk factors
Assessment of women with a possible early pregnancy loss
The clinical and economic benefits of a dedicated outpatient early pregnancy assessment service are well established. Early pregnancy assessment units (EPAU) offer the advantages of efficient and high-quality service for women with threatened, inevitable early pregnancy loss. A streamlined approach to management can avoid a hospital admission altogether in 40% of cases and reduce the length of hospital stay in a further 20% (Bigrigg et al., 1991).
Table 12.26.1 Nomenclature of early pregnancy loss (adapted from Farquaharson et al. 2005)

The National Service Framework recommends that EPAU should be universally available and easily accessible. The service should be comprehensive and appropriately staffed, with an efficient appointments system, ideally sited in a dedicated area with ultrasound equipment and easy access to laboratory facilities. The service should be available on a daily basis, with direct access for GPs and selected patient groups. Standardized information leaflets, referral and discharge letters should be available and regularly reviewed. Miscarriage is associated with significant psychological morbidity. Therefore, appropriate support and counselling offered to women after miscarriage is shown to have significant beneficial effects (Nielsen et al., 1996). Diagnosis
Special investigations
Pelvic ultrasound examination
Transvaginal pelvic ultrasound examination is the mainstay in the diagnosis of early miscarriage. Diagnosis is based on a combination of the clinical presentation correlated with ultrasound scan findings.
• Threatened miscarriage: viable pregnancy on ultrasound examination in a patient presenting with vaginal bleeding. On vaginal examination the cervix is closed.
• Complete miscarriage: the patient presents with vaginal bleeding, the passage of tissue vaginally (products of conception) and cramping abdominal pain. On ultrasound examination the uterine cavity is empty, has a thin endometrium, and vaginal examination confirms the cervix to be closed.
• Incomplete miscarriage: the patient presents with vaginal bleeding, passing products of conception, and abdominal cramping pain. On ultrasound examination the uterus has evidence of retained products of conception (RPOC) within the uterine cavity, which measures ≥15 mm diameter.
• Early pregnancy failure: the patient presents with or without vaginal bleeding and possibly receding symptoms of pregnancy. An ultrasound examination confirms an intrauterine pregnancy; however, the following observations are made:
• fetal pole (crown–rump length (CRL)) = 6 mm, no fetal heart activity noted
• fetal pole CRL management of incomplete miscarriage average 97% (range 80–100%) (Neilson et al., 2005). However, medical management is 2.8-fold more likely to induce complete miscarriage than expectant management. Misoprostol is the drug of choice. The advantages of medical management are that morbidities normally associated with surgical management and the risks of infection (2%) and of haemorrhage requiring blood transfusion (0.1%) are minimal.
Women undergoing expectant or medical management should be informed that the completion of miscarriage may take up to 4 weeks. The provision of this information increases the acceptability of these management modes and the success rates. They should also be informed that the success rate is higher when their follow up is based on clinical findings rather than based on ultrasound examination.
Surgical
If the patient opts for surgical management, an informed consent should be obtained and information leaflets on surgical evacuation should be provided. She should be informed of the success rate of surgical evacuation as 97–100%, and the risks of anaesthesia, infection (2%), haemorrhage requiring blood transfusion (0.1%), cervical trauma (1%), and uterine perforation (0.1–0.2%) (NICE 2004; Trinder et al., 2006).
Management of early pregnancy demise or missed miscarriage
• Sympathetically inform of the diagnosis
• Offer counselling and support
• Offer the options of
• expectant management
• medical management
• surgical management
• Counsel about all three options
• Provide written information and leaflets.
Expectant
The success rate varies between 25% and 85% (Bagratee et al., 2004); therefore, the patient should be advised of the higher failure rate. Expectant management for early pregnancy demise is associated with a higher risk of incomplete miscarriage and the need for emergency surgical uterine evacuation in the event of bleeding. However, there is a lower risk of infection than with surgical management. Both modes of management are equally effective and the woman’s preference should be taken into consideration (Nanda et al., 2006).
It is essential that there is open access to EPAU to these women and they should be followed up within 4 weeks.
Medical
Medical evacuation of early miscarriage is an effective alternative to surgical evacuation and achieved with the use of prostaglandin analogues (gemeprost or misoprostol) with or without antiprogesterone priming (mifepris-tone). Efficacy rates vary widely from 13% to 96% and are influenced by factors such as type of miscarriage, gestational sac size, total dose, duration, route of administration of prostaglandin, and whether the patient’s follow-up is based on clinical or ultrasound findings. Higher success rates (70–96%) are associated with incomplete miscarriage, high dose of misoprostol (1200–1400 μg), prostaglandins administered vaginally, and clinical follow-up without routine ultrasound (Oi-Shan et al., 2006, NICE 2004, Trinder et al., 2005). The prior use of mifepristone does not significantly affect the success rates, which range from 82% to 95% (Oi San Tang et al., 2003). Vaginal misoprostol is more effective and has fewer side-effects than the oral route. The rate of expulsion of RPOC ranges between 80% and 90% in women up to 13 weeks’ gestation.
If the patient opts for medical management, it is important that informed consent is obtained and relevant investigations are performed. Women ≤10 weeks’ gestation on ultrasound examination can be managed as an outpatient. Women ≥10 weeks’ gestation on ultrasound examination should be informed of a lower success rate and a higher risk of excessive bleeding. The usual protocol is as follows: day 1, 800 μg of misoprostol administered vaginally; day 2, the patient takes two further doses of misoprostol 400 μg 3 hours apart. The side effects of the medication are nausea, vomiting, diarrhoea, and mild pyrexia. The medication is used with caution in conditions where hypotension may precipitate severe complications (cerebrovascular disease and cardiovascular disease). The complications are those of infection (2%) and haemorrhage requiring blood transfusion (0.1%) (NICE 2004).
Women undergoing expectant or medical management should be informed that the completion of miscarriage may take up to 4 weeks. The provision of this information increases the acceptability of these management modes and the success rates (Creinin et al., 1996). They should also be informed that the success rate is higher when their follow up is based on clinical findings rather than based on ultrasound examination (Wagaarachchi et al., 2002).
All women should be provided with analgesia and offered open access to EPAU and supportive contact numbers. Follow-up examination should be arranged in 4 weeks at which a pelvic scan be performed.
• If the miscarriage is complete, the patient may be discharged with access to EPAU during her next pregnancy
• If the miscarriage is incomplete a repeat scan should be arranged in 2 weeks.
• Advise her that she may choose other management options such as surgical evacuation of uterus.
• If 6 weeks later the miscarriage is incomplete, she should be advised of alternative management options.
Following discharge the couple should be offered an appointment for counselling for psychological support (RCOG 2006).
Surgical
Women undergoing surgical evacuation should be screened for infection including Chlamydia trachomatis and bacterial vaginosis.
They should also have their full blood count (FBC) checked to ensure that they are not anaemic and a blood group and Rh antibody test should be performed to evaluate the need for anti-D immunoglobulin. If the patient is Rh negative she should receive 250 IU of anti-D immunoglobulin intramuscularly.
Tissue obtained at the time of miscarriage should be examined histologically to confirm pregnancy and to exclude ectopic pregnancy or unsuspected gestational trophoblastic disease.
An objective assessment of the psychological morbidity associated with expectant and surgical management of miscarriage revealed no differences related to the procedure itself. However, women with miscarriage who chose their own treatment option had the best health-related quality-of-life (HRQL) assessments compared with women who were randomized to one or other treatment modality (Nielsen et al., 1996, Wieringa-De Waard et al., 2002). It is therefore important to encourage patient choice in the management of early miscarriage.
Information on the sensitive disposal of fetal remains can be obtained from the RCOG Good Practice Guideline No. 5, Disposal following pregnancy loss before 24 weeks of gestation, the Stillbirth and Neonatal Death Society’s (SANDS) Pregnancy loss and the death of a baby: guide-lines for professionals (1995) and the Institute of Burial and Cremation Administration (IBCA) Policy document: disposal of fetal remains (2001). The Royal College of Nursing, Sensitive disposal of all fetal remains, guidance for nurses and midwives is also available at www.rcn.org.uk/members/downloads/disposal_fetal_remains.pdf. Expert adviser
The Recurrent Miscarriage Clinic, St Mary’s Hospital, London. Further reading
Bagratee J, Khullar V. A randomised controlled trial comparing medical and expectant management of first trimester miscarriage. Hum Reprod 2004;19:266–71.
Bigrigg MA, Read MD. Management of women referred to early pregnancy assessment unit: care and effectiveness. Br Med J 1991;302:577–9.
Creinin MD, Burke AE. Methotrexate and misoprostol for early abortion: A multicentre trial. Acceptability. Contraception 1996;54:19–20.
Farquharson RG, Jauniaux E, Exalto N. ESHRE Special Interest Group for Early Pregnancy (SIGEP). Updated and revised nomenclature for description of early pregnancy events. Hum Reprod 2005;20:3008–11.
Franssen M, Korevaar J, Fulco van der Veen, et al. Reproductive outcome after chromosome analysis in couples with two or more miscarriages: case-control study. BMJ 2006;332:759–763.
Konrad G, First-trimester bleeding with falling HCG. Don’t assume miscarriage. PMCID 2007;53(5).
Nanda K, Peloggia A. Expectant care versus surgical treatment for miscarriage. Cochrane Database Syst Rev. 2006 Apr 19;(2): CD003518. Review.
Neilson JP, Hickey M. Medical treatment for early fetal death (less than 24 weeks). Cochrane Database Syst Rev. 2006 Jul 19; 3: CD002253.
NICE. The care of women requesting induced abortion. September 2004.
Nielsen S, Hahlin M, Moller A, Granberg S. Bereavement, grieving and psychological morbidity after first trimester spontaneous abortion: comparing expectant management with surgical evacuation. Hum Reprod 1996;11:1767–70.
Nielson S, Hamlin M. Expectant management of first-trimester spontaneous abortion. Lancet 1995;345:84–6.
Nielson S, Platz J. Randomised trial comparing expectant with medical management for first trimester miscarriage. Br J Obstet Gynaecol 1999;106:804–7.
Oi San Tang, Winnie Nga Ting Lau. A prospective randomised study to compare the use of repeated doses of vaginal with sublingual misoprostol in the management of first trimester silent miscarriages. Hum Reprod 2003;18:176–81.
Oi Shan T, Charas YT. A randomised trial to compare the use of sublingual misoprostol with or without an additional 1 week course for the management of first trimester silent miscarriage. Hum Reprod 2006;21:189–92.
Royal College of Obstetricians and Gynaecologists (RCOG) The management of early pregnancy loss. Green Top Guideline no 25. London: RCOG 2006.
Sairam S, Khare. The role of ultrasound in the expectant management of early pregnancy loss. Ultrasound Obstet Gynecol 2001;17:506–9.
Shelly J, David H. A randomised trial of surgical, medical and expectant management of first trimester spontaneous miscarriage. Aust N Z J Obstet Gynaecol 2005;45:122–7.
Trinder J, Rocklehurst P. Management of miscarriage: expectant, medical, or surgical? Results of randomised controlled trial (miscarriage treatment (MIST) trial). BMJ 2006;332:1235–40.
Wagaarachchi P, Ashok P. Medical management of early fetal demise using sublingual misoprostol. Br J Obstet Gynaecol 2002;109:462–5.
Wieringa-De Waard M, Hartman E, Ankum W, et al. Expectant management versus surgical evacuation in first trimester miscarriage: health-related quality of life in randomised and nonrandomized patients. Hum Reprod 2002;17:1638–42. Patient resources
Association of Early Pregnancy Units: www.earlypregnancy.org.uk
Miscarriage Association (Registered Charity No. 1076829) c/o Clayton Hospital, Northgate, Wakefield, West Yorkshire WF1 3JS. Telephone: 01924 200799: www.miscarriageassociation.org.uk.
Oocyte donation
Oocyte donation offers the prospect of pregnancy to women who are unable to use their own oocytes. The fertility potential with this treatment is high, with a low miscarriage rate being reflective of the donor’s fertility status rather than the recipient. However, the process is not without risk to both parties, as the donor has to undergo an in vitro fertilization (IVF) cycle up to oocyte collection and the recipient then has to embark on a pregnancy that poses its own specific challenges. Indications
Women who require oocyte donation fall into two groups.
Women with primary or secondary ovarian failure
• gonadal dysgenesis (Turner’s syndrome, XY karyotype)
• premature ovarian failure (natural or iatrogenic)
• menopause.
Women with menstrual cycles
• repeated IVF failure (poor response to stimulation, persistent oocyte abnormality)
• carrier of severe genetic disease. Recruitment of donors
There are three potential sources of donated oocytes:
• anonymous donors: altruistic individuals who volunteer, either by themselves or in response to advertisements in the media, to be oocyte donors
• known donors: women who are known to the recipient, usually sisters or friends
• ‘egg sharing’: women undergoing IVF treatment who donate a proportion of their oocytes, either altruistically or, more commonly, to reduce the cost of their own treatment.
Egg sharing is allowed in the UK, but direct payment to donors is limited by the HFEA Code of Practice to ‘reasonable expenses’. Payment is accepted in several other countries: the American Society for Reproductive Medicine states that ‘financial compensation … is justified on ethical grounds’.
There is a severe shortage of oocyte donors in the UK, with waiting lists of 1–2 years being common even in the private sector, and the demand for treatment is rising. Thus, many couples seek treatment overseas (so-called ‘reproductive tourism’). Assessment of donors
• Age: the HFEA recommends that unless there are exceptional circumstances, eggs should not be taken for the treatment of others from donors aged 36 or over.
• Donors should be free of any significant medical or psychiatric history and should not have a history of familial genetic disorders.
• Donors should be provided with psychological counselling as well as a full medical examination.
• Screening: blood should be taken for hepatitis B and C, HIV, cytomegalovirus, venereal disease research laboratory (VDRL) tests, karyotype, and blood group; donors from ethnic groups susceptible to cystic fibrosis, haemoglobinopathies and Tay–Sachs disease should be appropriately screened. Managing the donor
In general, oocyte donors (except oocyte sharers) are young, fertile women. Therefore, these women are sensitive to ovarian stimulation and the consequences of this. Careful management of the stimulation cycle is essential to minimize the risk of ovarian hyperstimulation syndrome (OHSS). The initial consultation should include information on the risk of OHSS, which in its severe form is relatively rare but can be fatal. No long-term risks of ovarian stimulation have been demonstrated. Donors must be advised on contraception to avoid unplanned pregnancy. Managing the recipient
Women with ovarian failure
• In these women, there is no endogenous sex steroid production from the ovaries and therefore there is no oestrogen-driven development of the endometrium and subsequent decidualization by progesterone.
• Oestrogen is replaced using the oral, transdermal, or intravaginal route with ultrasound monitoring to assess the adequacy of the endometrial response, with a higher pregnancy rate associated with the ‘triple layered’ appearance and thickness of at least 8 mm. Oestrogen supplementation is usually required for at least 2 weeks, but individual response varies. For this reason, many fertility clinics will perform a ‘dummy’ endometrial preparation cycle.
• Progesterone is supplemented 1 day before oocyte collection (i.e. after hCG injection to the donor) and can be given intramuscularly or vaginally. Hormone replacement is continued until the pregnancy test.
Women with menstrual cycles
• The recipient in this situation has her own endogenous pituitary: ovarian activity and her menstrual cycle must be in synchrony with the donor in order to achieve implantation.
• Several approaches have been used, including cryop-reservation of donor oocyte embryos and subsequent thawing for replacement on the appropriate day of the recipient’s natural cycle.
• In contemporary practice, the preferred method is to suppress the recipient’s menstrual cycle using short-acting GnRH analogues to downregulate her endogenous pituitary activity. Hormone replacement is then given as for the menopausal woman (see above). Both donor and recipient may be given the combined oral contraceptive pill to synchronize their withdrawal bleeds. Laboratory aspects
Donated oocytes are fertilized in vitro with sperm from the recipient’s male partner (or donor sperm) and the resulting embryos are cultured using standard laboratory protocols until transferred to the recipient’s uterus.
In contrast to donor insemination, where sperm samples are quarantined before use, donor oocytes are utilized for fresh embryo transfer. Thus there is a theoretical risk of viral transmission. Recent advances in freezing technology allow vitrification of oocytes with good survival rates, and pregnancy rates approaching fresh oocytes; this raises the possibility of donor ‘egg banking’. This would give a great advantage over current practice in avoiding the need to synchronize donor and recipient cycles, and also allow a quarantine period while the donor is retested for transmissible infections. Cross-border treatment might be reduced as vitrified oocytes could be imported. Embryo transfer and maintenance of pregnancy
• Timing of embryo transfer should be based on embryonic development in the laboratory. As most oocyte donors are young and fertile, the developmental potential of their embryos is above average and a higher proportion of these embryos will be suitable for blastocyst stage transfer. These embryos have the highest implantation potential and therefore special consideration should be given to the risk of multiple pregnancy.
• Maintenance of the steroid environment is essential to support the early conceptus. Although the early placenta secretes sufficient progesterone and oestrogen to support the pregnancy independently of the corpus luteum by 6–8 weeks’ gestation, oocyte recipients usually receive exogenous hormone support until at least 10 weeks’ gestation. Success rates and the outcome of pregnancy
• Oocyte donation leads to pregnancy rates above those of standard IVF. The latest published UK figures show a live birth rate of 31.5% per fresh cycle carried out in 2006, and a quarter of these were multiple births. More recent results from individual clinics show pregnancy rates around 50% per cycle.
• The age of the donor is unimportant, and pregnancy rates are maintained in older women receiving hormone replacement for uterine preparation. Women with premature ovarian failure due to pelvic irradiation have reduced pregnancy rates and poorer outcome of pregnancy consequent upon uterine irradiation.
• Donor oocyte pregnancies are obstetrically high risk. Multiple pregnancies carry their own inherent risks to both mother and babies, and these are well recognized; however, specific to oocyte donor pregnancies is the significant risk of pre-eclampsia, which can often be severe in these cases. Additionally, increasing numbers of recipients are undergoing oocyte donation because their own biological age has limited their reproductive potential. Older women are at greater risk of obstetric complications and should be considered as high risk cases. The cumulative risk of maternal age, oocyte donor pregnancy and multiple pregnancy warrant obstetricianled care throughout pregnancy. The law and regulation of oocyte donation
Gamete donation is strictly regulated in the UK (see Chapter 12.6, Donor insemination). Recipients of donated oocytes may be more likely to disclose their child’s origins than infertile couples receiving donor insemination. Donor anonymity is protected in some countries, and this is seen as an advantage of overseas treatment by some infertile couples. Further reading
ASRM Ethics Committee. Financial compensation of oocyte donors. Fertil Steril 2007;88:305–9.
Critchley HO, Bath LE, Wallace WH. Radiation damage to the uterus: review of the effects of treatment of childhood cancer. Hum Fertil 2002;5:61–6.
Csapo AI, Pulkkinen, MO, Ruttner B, et al. The significance of the human corpus luteum in pregnancy maintenance. I. Preliminary studies. Am J Obstet Gynecol 1972;112:1061–7.
Gosden RG. Maternal age: a major factor affecting the prospects and outcome of pregnancy. Ann NY Acad Sci 1985;442:45–7.
Human Fertilisation and Embryology Authority. A long-term analysis of the HFEA Register data (1991–2006). 2008
Human Fertilisation and Embryology Authority. Guidance on egg sharing arrangements CH(00)09 2000; www.hfea.gov.uk/en/657.html Serhal P, Craft I. Oocyte donation in 61 patients. Lancet 1989;1:1185–7.
Serhal P, Craft I. Ovum donation: a simplified approach. Fertil Steril 1987;48:265–9.
Serhal P. Oocyte donation. In: Serhal P, Overton (eds). Good clinical practice in assisted reproduction. Cambridge 2004: 86–99.
Wiggins DA, Main E. Outcomes of pregnancies achieved by donor egg in vitro fertilization: a comparison with standard in vitro fertilization pregnancies. Am J Obstet Gynecol 2005;192:2002–6.
Zaidi J, Campbell S, et al. Endometrial thickness, morphology, vascular penetration and velocimetry in predicting implantation in an in vitro fertilization program. Ultrasound Obstet Gynaecol 1995;6:191–8. Internet resources
www.hfea.gov.uk
www.ngdt.co.uk/
www.bica.net/ Patient resources
HFEA Guide to Infertility. Human Fertilisation and Embryology Authority, London 2008 (also available online)
www.infertilitynetworkuk.com/
www.dcnetwork.org/
The Daisy Network (patient support group for premature menopause): www.daisynetwork.org.uk/
Oligomenorrhoea and amenorrhoea Definition
Oligomenorrhoea refers to a reduction in the frequency of periods where menstrual intervals may vary between 6 weeks and 6 months.
Amenorrhoea is the complete cessation of periods for more than 6 months. Primary amenorrhoea is defined as the absence of spontaneous onset of menstrual periods by age 16 years. Secondary amenorrhoea is the absence of periods for 6 months or more when a patient has previously had regular periods and 12 months or more when the patient has had irregular cycles since her menarche. Epidemiology
The prevalence of amenorrhea not due to pregnancy, lactation or menopause is approximately 3–4% and depends on the age group studied: 7.6%, 3.0%, and 3.7% in women aged 15–24, 25–34, and 35–44 years respectively (Münster et al., 1992). Aetiology
The occurrence of regular monthly periods in women of reproductive age reflects cyclic ovarian activity, which is finely controlled by a sequence of hypothalamic–pituitary–ovarian interactions. Oligomenorrhoea and amenorrhoea may result from similar causes, which are more commonly due to endocrine dysfunction of the hypothalamic-pituitary-ovarian axis. In addition, amenorrhoea may be due to anatomical anomalies of the genital tract.
Women are amenorrhoeic before puberty, during pregnancy and lactation, and in the postmenopausal period. The four most common causes of amenorrhoea are: polycystic ovary syndrome (PCOS), hypothalamic amenorrhoea, ovarian failure, and hyperprolactinaemia.
Anatomical anomalies of the genital tract
These account for about 1% of cases of amenorrhoea.
Congenital
• Absence of uterus (with or without absent vagina)
• Testicular feminization syndrome
• Outflow tract obstruction (imperforate hymen or transverse vaginal septum).
Acquired
• Endometrial damage: traumatic (Asherman’s syndrome), chronic endometritis (pelvic tuberculosis), endometrial resection or ablation
• Cervical stenosis (extremely rare): surgical trauma, infective
• Vaginal stenosis (extremely rare): chemical inflammation.
Endocrine dysfunction
Hypothalamic-pituitary-ovarian axis
• Ovarian
• ovarian failure: genetic, autoimmune, post surgery/chemotherapy/radiotherapy, galactosaemia, and idiopathic
• polycystic ovary syndrome
• hormone-secreting tumours (rare).
• Pituitary
• pituitary failure: adenoma, infarction (Sheehan’s syndrome), infection (encephalitis), irradiation
• hyperprolactinaemia: prolactinoma, primary hypothyroidism, chronic renal failure, and drug induced.
• Hypothalamic
• congenital (Kallmann’s syndrome)
• functional causes: obesity, weight loss, anorexia nervosa, excessive exercise, psychological stress, debilitating illness.
Others
• Thyroid disease
• Adrenal disease. Clinical approach
History
• Detailed menstrual history, e.g. onset of menarche, cycle length, and duration
• Sexual and contraceptive history
• Developmental age of secondary sexual characteristics, e.g. breast and pubic hair development
• Cyclical abdominal pain
• Body weight fluctuations (loss and gain)
• Hyperandrogenism, e.g. acne, excessive hair, baldness
• Presence of galactorrhoea
• Vasomotor symptoms, e.g. hot flushes, night sweats
• Symptoms of intracranial space occupying lesion, e.g. headache, vomiting, visual disturbance
• Psychological stress or excessive exercise
• Drugs history and current exposure
• History of previous surgery, e.g. surgical termination of pregnancy, endometrial ablation
• Family history of early menopause, polycystic ovary syndrome
Physical examination
• Height, weight, and body mass index (BMI)
• Secondary sexual characteristics, e.g. breast and pubic hair development
• Galactorrhoea
• Hyperandrogenism, e.g. acne, excessive hair, baldness
• Gynaecological examination: imperforate hymen, presence of uterus/vagina
• Detailed neurological (including smell and ophthalmic) examinations.
Investigations
• Urinary pregnancy test should be performed prior to any further investigation to exclude pregnancy in case of doubt.
• Pelvic ultrasound to identify the presence of a uterus and to establish ovarian morphology. Polycystic ovaries (PCO) are characterized by 12 or more follicles measuring 2–9 mm in diameter, or increased ovarian volume (>10 cm3) (Balen et al., 2003).
• Hormonal tests including serum FSH, LH, prolactin and TSH are required to establish the endocrine causes of oligomenorrhoea/amenorrhoea. A raised prolactin level should be confirmed by repeat testing.
• Measurement of serum androgens is indicated when there is clinical evidence of hyperandrogenism such as hirsutism. Serum testosterone levels are usually elevated in patients with PCOS. When testosterone levels exceed 5 mol/L further investigations to exclude adrenal pathology are indicated. They include 17 α-hydroxyprogesterone, dehydroepiandrosterone sulphate, low-dose and high-dose dexamethasone suppression, and cortisol secretion tests, along with ultrasound (US), computer tomography (CT), or magnetic resonance imaging (MRI) of the adrenal gland.
• Pituitary imaging with CT or MRI is required to detect a prolactin-producing adenoma or an empty sella. It is also indicated in patients with low gonadotrophin levels to exclude space-occupying lesions. A full assessment of pituitary hormone secretion is essential to evaluate the impairment of pituitary function. CT of the skull should be performed to exclude any space-occupying lesion around the hypothalamic and pituitary regions, which can disturb gonadotrophin secretion.
• Patients with premature ovarian failure should undergo karyotyping and autoantibody screening.
Management
The appropriate management is dependent upon accurate diagnosis and careful assessment of the individual needs of the patient. This may include treatments to promote or control fertility, improve hyperangdrogenism, prevent osteoporosis, or protect the endometrium from unopposed oestrogen action.
The causes of amenorrhoea can be divided into five distinct categories (Fig. 12.28.1). Ovulation induction can be offered to anovulatory women who wish to become pregnant (Ng and Ho, 2002).
Anatomical causes
• Patients with congenital absence of the uterus do not require hormonal replacement therapy (HRT) since they have functioning ovaries. Pregnancy may be possible following in vitro fertilization (IVF) and embryo transfer to a surrogate mother.
• Those with hypoplastic or absent vagina may benefit from vaginal dilators or vaginoplasty. In girls with imperforate hymen incision and drainage should be performed.
• Hysteroscopic lysis of intrauterine adhesions and placement of an intrauterine contraceptive device followed by oestrogen therapy in the postoperative period to restore the menstrual cyclicity in patients with Asherman’s syndrome (Yu et al., 2008).
• Patients with testicular feminization should undergo gonadectomy after puberty to prevent malignant transformation (dysgerminoma), which occurs in about 5% of cases. Oestrogen replacement therapy is required but not progestogens in the absence of a uterus. Careful psychological counseling is essential to achieve patient understanding of the need to remove the gonads and future hormone therapy.
• All gonads in phenotypic females containing a Y chromosome are at an increased risk of developing malignancy, and women with 46XY gonadal dysgenesis (Swyer’s syndrome) should undergo gonadectomy as soon as the diagnosis is made (see Chapter 12.5 Disorders of sex development).
Hyperprolactinaemia
• The treatment of choice is dopamine agonists such as bromocriptine or carbergoline, which lower prolactin concentrations and cause shrinkage of a prolactinoma, if present. Restoration of ovulatory menstrual cycles may occur within a few months of commencing dopamine agonists and contraception will be required for women who are not planning to get pregnant.
• Surgery in the form of trans-sphenoidal pituitary adenomectomy is seldom indicated in the presence of a prolactinoma because of the high recurrence rate and possibility of pan-hypopituitarism.

Fig. 12.28.1 Flowchart of diagnosis and treatment. This figure was published in Gynaecology, RW Shaw, WP Soutter and SL Stanton, Copyright Elsevier (2002) pp. 245–258.
Hypergonadotrophic hypogonadism
• These women should be offered HRT to protect their bones from the deleterious effects of endogenous hypooestrogenism. In women with primary amenorrhoea, HRT may help to develop the secondary sexual characteristics. In women with premature ovarian failure, HRT can help to alleviate climacteric symptoms and prevent vaginal atrophic changes which may lead to dyspareunia.
• There have been case reports of spontaneous pregnancies and successful ovulation induction therapy for women with ovarian failure. However, the only realistic treatment for these patients is the use of donor eggs in an in vitro fertilization treatment setting.
Hypogonadotrophic hypogonadism
• Surgery is clearly indicated in patients with central nervous system tumours.
• Patients with anorexia nervosa may benefit from psychotherapy and weight gain after extensive counselling.
• Pulsatile GnRH or gonadotrophin therapy may be offered to patients with other hypogonadotrophic causes or with persisting anovulation despite weight gain, if the patient wishes to conceive.
• HRT can be considered for those with no desire to get pregnant.
Normogonadotrophic hypogonadism
• The majority of these patients will have PCOS. The diagnosis of PCOS requires the presence of two from the following three diagnostic criteria: (i) oligo- and/or anovulation; (ii) clinical and/or biochemical features of hyperandrogenism; and (iii) the presence of polycystic ovary (PCO) morphology (The Rotterdam ESHRE/ASRM-sponsored PCOS consensus workshop group, 2004).
• Obese PCOS women will benefit from weight loss, as this will not only improve their response to ovulation induction therapies but may also result in spontaneous ovulation.
• Women with PCO usually respond well to clomiphene citrate or, failing that, to gonadotrophins for induction of ovulation. Insulin-sensitizing agents or laparoscopic ovarian drilling may be considered in those not responding to clomiphene citrate (Thessaloniki ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group, 2008).
• Other causes include congenital adrenal hyperplasia, adrenal tumours and androgen-producing ovarian tumours. The patient may have clinical symptoms or signs of hyperandrogenism such as hirsutism, prompting more detailed investigations (see earlier). Congenital adrenal hyperplasia responds to corticosteroid replacement therapy. Surgical removal is required for any adrenal or ovarian tumours. Further reading
Balen AH, Laven JSE, Tan SL, Dewailly D. Ultrasound assessment of the polycystic ovary: international consensus definitions. Hum Reprod Update 2003;9:505–14.
Münster K, Helm P, Schmidt L. Secondary amenorrhoea: prevalence and medical contact–a cross-sectional study from a Danish county. Br J Obstet Gynaecol 1992;99:430–3.
Ng EHY, Ho PC. Ovulation induction. In: Shaw RW, Soutter WP, Stanton SL (eds) Gynaecology, 3rd edn. Churchill Livingstone, 2003: 245–58.
Practice Committee of the American Society for Reproductive Medicine. Current evaluation of amenorrhea. Fertil Steril 2008; 90(Suppl 3): S219–225.
The Rotterdam ESHRE/ASRM-sponsored PCOS consensus workshop group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Hum Reprod 2004;19:41–7.
Thessaloniki ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Consensus on infertility treatment related to polycystic ovary syndrome. Hum Reprod 2008;23:462–77.
Warren MP. Clinical review 77: evaluation of secondary amenorrhea. J Clin Endocrinol Metab. 1996;81:437–442.
Yu D, Wong YM, Cheong Y, Xia E, Li TC. Asherman syndrome–one century later. Fertil Steril 2008;89:759–79. Internet resources
www.patient.co.uk/showdoc/40000034/
Ovarian hyperstimulation syndrome Introduction
Ovarian hyperstimulation syndrome (OHSS) is a serious iatrogenic complication of ovarian stimulation treatment such as in vitro fertilization (IVF) and ovulation induction (OI) using gonadotrophins (follicle-stimulating hormone (FSH), luteinizing hormone (LH), human menopausal gonadotrophin (hMG), human chorionic gonadotropin (hCG)) and/or antioestrogens (clomiphene). All methods of ovulation induction can cause OHSS. It may even result from the use of oral antioestrogen, which is often unwisely used outside specialized fertility settings. On rare occasions, however, it is known to occur spontaneously in natural cycles. OHSS is a risk management issue in gynaecology as it can be potentially lethal. Moreover, there has been a stupendous rise in the number of women undergoing IVF treatment since Steptoe and Edwards pioneered its use 30 years ago. Over a million IVF cycles are being performed worldwide every year, and the incident of IVF cycles from is at least five or six times the number. Prevalence
The prevalence of OHSS during IVF treatment varies from mild in 20–33%, moderate in 3–8% and that of severe forms in 0.5–5% of all cycles. However, there has been an alarming and disproportionate rise in the number of women developing severe OHSS (20-fold rise) compared with the total number of women having IVF treatment (sixfold increase) as more women have turned towards assisted conception treatment globally (Rizk 2006). It is generally accepted that due to inconsistencies in OHSS reporting policies compounded by the fact that OHSS may present with multisystem complications, often to medical specialties who are not familiar with this complication and lack the expertise to deal with the myriad of complications of OHSS, figures of true incidence and fatalities due to OHSS are likely to be underestimated. Classification
OHSS is classified to aid its appropriate management and for epidemiological surveys. Based on the severity of signs, symptoms, and biochemical parameters, this syndrome has traditionally been graded into three categories as mild, moderate, and severe OHSS. Since severe OHSS causes significant morbidity and requires intensive management, it is further classified into three grades (A, B, C) the severest form of which is critical OHSS. OHSS may also occur early (3–7 days after hCG stimulus) or as late OHSS (12–17 days after hCG stimulus). However, clinical experience shows that such classifications may often be misleading since OHSS has a broad spectrum of clinical signs, symptoms, and biochemical alterations that often overlap and which may change rapidly over time. Pathophysiology
The basic pathology is enormous cystic ovarian enlargement, pathological extravascular fluid shift, and intravascular fluid volume depletion. This exudative fluid accumulates primarily in the peritoneal cavity causing protein-rich ascites, and in pleural and pericardial cavities causing effusions. Loss of fluid into the third space causes a profound fall in the intravascular volume. Mechanisms
Vascular endothelial growth factor
The vascular endothelial growth factor (VEGF) system, composed of ligands and receptors, plays a pivotal role in the pathophysiology of OHSS. VEGF is the prototypical member of the family of angiogenic factors which include angiopoetin, PlGF, bFGF and VEGF A, B, C, D, E which regulate physiological and pathological angiogenesis. Exposure of ovaries to hCG/LH causes a VEGF-mediated increase in vascular permeability (VP), which is cardinal to OHSS. VEGF is expressed in granluosa lutein cells of the ovary and its soluble forms are found in serum, follicular, ascitic, and pleural fluid of women with OHSS. The undisputed role of VEGF as a mediator of OHSS is exemplified by the fact that blocking VEGF action in vivo prevents development of OHSS in the murine model.
Role of oestradiol
High circulating oestradiol (E2) concentrations are an immediate precursor of the syndrome; however, E2 does not cause the increase VP associated with OHSS.
Ovarian renin angiotensin system
Excessive levels of ovarian derived renin, angiotensinII and aldosterone in women developing OHSS establishes a positive correlation between renin angiotensin system (RAS) and OHSS.
Cytokines
Proinflammatory cytokines (TNF- α, IL-1, 2, 6, 8, 10, 18, PG) play a role in ovarian paracrine interactions and VP. They may therefore contribute to pathogenesis of OHSS.
Kallikrein–kinin system
Tissue kallikreins are expressed in ovarian granulosa cells and are essential to inflammatory process. They may therefore contribute to the VP associated with OHSS.
Selectins and ICAM
Selectins and intracellular adhesion molecules are mediators of inflammatory reaction (sICAM) and of angiogenesis (VE-cadherin). They may cause the altered VP of OHSS. Prediction and risk factors
Although there is now a better understanding of the pathophysiology, the treatment remains non-specific; OHSS is therefore better prevented. Predicting OHSS with known risk factors is the key to its prevention.
Prior to starting IVF
• Presence of polycystic ovaries (PCO) on pelvic ultrasound examination and/or pre treatment diagnosis of polycystic ovary syndrome (PCOS): women with PCO/PCOS respond by a profound multifollicular response (threefold higher) compared with women with normal ovaries. A higher expression of VEGF in serum and in the hyperthecotic stroma of PCO and consequently higher stromal blood flow in PCO link OHSS to PCO. Moreover, PCO is more frequently seen in women undergoing fertility treatment (40% versus 22%) than in the general population. Other predictive factors described in literature such as the necklace sign of ovaries, ovarian volume, high antral follicle count, and low intravascular ovarian resistance are largely features of a PCO. Isolated features of PCOS such as raised LH–FSH ratio, hyperandrogenism, oligomenorrhoea, and hyperinsulism have been described as risk factors for developing OHSS.
• Age, BMI and previous OHSS: younger women are more likely to develop OHSS, consistent with greater ovarian reserve/responsiveness than older women. Obese women are more likely to have a higher threshold of gonadotrophin requirement for ovarian stimulation and may therefore underrespond with standard doses of gonadotrophins. They are therefore less likely to develop OHSS. Women are more likely to develop OHSS if they have previously done so.
• Baseline serum FSH, inhibin B and AMH (anti-Müllerian hormone): these have all been investigated as markers of OHSS. Low baseline FSH and high inhibin B and AMH are markers of a greater ovarian reserve and, therefore, indirect predictors of the risk of developing OHSS.
• Genetic predisposition: FSH receptor single nucleotide polymorphism(SNP) genotype may help predict ovarian response.
During ovarian stimulation treatment
• Higher dose and longer duration of gonadotrophin treatment irrespective of the type of gonadotrophins (FSH or hMG).
• Use of GnRH analogues for pituitary down regulation increases the risk of OHSS sixfold, by abolishing endogenous LH surge thereby promoting uninhibited follicular growth when stimulated with gonadotrophins.
• Development of large number of follicles, in response to gonadotrophin stimulation. There is no agreed cut off (varies between 10 and 35) for the number of follicles that would predict OHSS. Developing >25 follicles predict OHSS with 25% positive predictive value.
• Exposure of ovaries to LH/hCG mediates VP. OHSS therefore occurs after hCG/LH administration and during pregnancy. Pregnant women develop late onset OHSS that is often severe and of longer duration.
• Greater number of oocytes retrieved which is reflective of greater ovarian responsiveness to ovarian stimulation. There is no agreed cut-off, which varies between 14 and 30; retrieving >15 oocytes has a 35% PPV.
• High E2 concentrations predict a quarter of cases of OHSS: there is no agreed cut-off for E2 concentrations that would predict OHSS. It varies widely between 2642 and 6000 ng/mL (10 000–22 020 pmol/L).
• Circulating VEGF and its receptor sflt-1 concentrations provide a non-steroidal index of ovarian response. The use of VEGF and sflt-1 measurements, however, still need to be validated prospectively and easily reproduced for its utility in clinical practice.
• High circulating concentrations of renin angiotensin, cytokines(IL-6, 8) and von Willebrand factor are observed in women developing OHSS; these however are not validated for use in clinical practice.
Prediction of OHSS by multiple markers
A combination of some or all of the above markers predicts the development of OHSS with greater accuracy. Prevention
Identifying women at risk, judicious ovarian stimulation, and using multiple preventative factors remains the mainstay of preventing OHSS.
Prior to starting IVF
Treatment of anovulation by methods other than OI with gonadotrophins and antioestrogen:
• Lifestyle modification and weight reduction
• insulin-sensitizing agents, e.g. metformin, which increases ovarian responsiveness in hyperandrogenic, hyperinsulinaemic and often obese women with PCOS. Current evidence supports the view that co-treatment of metformin with gonadotrophins during IVF treatment in women with PCOS reduces the risk of developing OHSS.
• Laparoscopic ovarian diathermy(LOD) is a safer alternative to OI agents in women with anovulatory PCOS however current evidence does not support the view that LOD prior to IVF reduces risk of OHSS.
• Aromatase inhibitors are being used for OI at present time with no reports of OHSS. The use of ketoconazole, octreotide and pentoxyfylline has no proven benefit in reducing OHSS during OI.
• Pulsatile GnRH pump rather than hMG for OI in women with hypogonadotrophic hypogonadism causes a more physiological ovarian response.
Finally, if gonadotrophin remains the only option for OI, its judicious use and unifollicular ovulation avoids OHSS.
During IVF: prior to oocyte retrieval
• Careful regulation of dose and duration of gonadotrophins by ultrasound monitoring thereby avoiding exuberant response of ovaries.
• Current evidence suggests that the GnRH antagonist protocol of IVF results in significantly lower incidence of severe OHSS; however, the pregnancy rate is lower than the long protocol of the GnRH analogue treatment cycle.
• Cancellation of treatment cycles by withholding hCG in women with prolific ovarian response reduces the likelihood of developing OHSS. Thereafter, follicular aspiration along with continued suppression of pituitary by GnRH analogues further reduces OHSS risk.
• The use of GnRH analogues (but not rLH), to trigger ovulation instead of hCG reduces the likelihood of developing OHSS but also results in a lower clinical pregnancy rate (Griesinger et al., 2006).
• Coasting assumes the principle of withdrawing ovarian stimulation when follicular response and/or E2 concentrations reach a threshold above which the risk of developing OHSS is significant, until the E2 concentrations drops. Although coasting may reduce the risk of developing OHSS it also reduces the likelihood of pregnancy, particularly if coasting exceeds 3 days.
• Reducing the hCG dose (irrespective of human or recombinant types) reduces the severity of early-onset OHSS but not risk of developing OHSS. Current evidence does not support the view that substituting hCG with LH reduces the likelihood of developing OHSS.
• Pre-hCG unilateral follicular aspiration does not reduce the risk of developing OHSS.
During IVF: after oocyte retrieval
• Cryopreservation of embryos resulting from IVF treatment reduces the risk of developing late OHSS by eliminating endogenous hCG exposure due to a resulting pregnancy; however, it does not reduce the risk of early OHSS, which is related to ovulatory dose of hCG. A recent Cochrane review confirms no benefit of elective cryopreservation versus fresh embryo transfer.
• Single embryo transfer in women at risk of OHSS avoids multiple pregnancies. This reduces the severity of late onset OHSS as the intensity of OHSS is related to amount of circulating endogenous hCG.
• Progesterone instead of hCG for luteal support is associated with a lower risk of developing OHSS.
• Although it is largely accepted that use of i.v. albumin does not reduce the risk of OHSS, a recent Cochrane review supports the use of i.v. albumin for preventing OHSS. The mechanism of action is twofold; first, it increases plasma oncotic pressure and secondly its binding properties may result in inactivation of vasoactive peptides which cause OHSS.
• There is insufficient evidence at the present time on the beneficial effects of hydroxylethylstarch (synthetic plasma expander), which is a safer and cost-effective alternative to albumin for preventing OHSS.
• Intravenous hydrocortisone has proven to be ineffective in preventing OHSS.
• Dopamine receptor 2 agonist, cabergoline, inactivates VEGFR and may prevent the VP of OHSS.
• In vitro maturation (IVM) of oocytes in women at risk of OHSS (e.g. those with PCO/PCOS) may provide a safer alternative to traditional IVF. IVM minimizes the dose and duration of ovarian stimulation and avoids hCG injection, thereby eliminating the two important risk factors of OHSS development. Complications
OHSS may present itself with multisystem complications. Intravascular fluid depletion results in hypovolaemia (55% of all OHSS) and haemoconcentration (50% of all and 70–95% of severe OHSS), which poses a risk of thromboembolism (TE) and renal failure. Complications associated with TE occur in 0.06–10% of all severe cases of OHSS and contribute to a largest morbidity and mortality associated with OHSS. Other complications are liver dysfunction (30% of all OHSS), hepatorenal failure, pleural effusions (10–30% of severe OHSS), adult respiratory distress syndrome, and pericardial effusions resulting in cardiac tamponade. Morbidity may also be related to ovarian torsion, infection, cyst rupture, and haemorrhage prior to and during pregnancy. Complications during pregnancy in women who develop OHSS are largely related to multiple gestations and prematurity. Diagnosis
A history of ovarian stimulation treatment in almost all women with OHSS. Early-onset OHSS occurs within 3–7 days and late-onset OHSS 12–17 days after hCG administration and is often associated with pregnancy.
Symptoms
Abdominal discomfort, pain, distension, nausea, vomiting, diarrhoea, shortness of breath, oligura, and those related to complications of severe OHSS such as TE, hepatorenal failure, and hydrothorax.
Signs
Cystic ovarian enlargement and free fluid in the abdomen diagnosed on ultrasound examination. Ovarian size does not correlate to the severity of OHSS but with larger ovaries, OHSS severity is likely to be worse. Signs related to infection and hypovolemia included hypotension, tachycardia and tachypnoea. Signs related to specific complications of severe OHSS such as TE, hepatorenal failure, ascites, and hydrothorax.
Biochemical parameters
Although biochemical alterations have traditionally been categorized in severe OHSS, in clinical practice, marginal hypoalbuminaemia, altered liver enzymes and electrolyte imbalances may be observed in women with sign/symptoms of mild and moderate OHSS. A haematocrit of >45 l/L is categorised in moderate and >55% in severe OHSS. WBC count of >15 m/l is categorised in moderate and >25 m/ml in severe OHSS. Creatinine concentration of >100 μmol/L is categorized as severe OHSS. Management
• Centres providing IVF/OI should provide verbal/written information to women prior to and after undergoing treatment on the risk of OHSS, signs/symptoms expected, and advice to seek prompt expert medical advice should symptoms develop.
• Mild and moderate OHSS may be managed supportively in outpatient settings. It requires monitoring by ultrasound examination, blood tests (include βhCG, full blood count, electrolytes, kidney, liver function tests, and clotting profile) and relief of symptoms with analgesics and antiemetics. Optimum fluid intake is encouraged. Follow-up is mandatory until complete resolution. Strenuous exercise is to be avoided as it may cause cyst rupture or ovarian torsion.
• Worsening signs/symptoms requires close monitoring as severe OHSS requires hospitalization and multidiscipli-nary medical management. Critical OHSS requires ITU management.
• Monitoring by weight, abdominal girth, vital signs, fluid balance charts, blood tests as mentioned, and ultrasound examination of pelvis/abdomen/chest. Radiographic investigations may be required in complications such as TE and hydrothorax. However, it should be avoided if possible in women who are likely to be pregnant.
• Treatment modalities are aimed at maintaining fluid balance and circulation with use of intravenous crystalloids/colloids. If oligo/anuria or respiratory compromise occurs, ultrasound-guided culdocenteses/paracenteses of ascitic fluid and pleurocentesis relieve respiratory distress and maintain renal function. Use of diuretics is not advisable as it worsens the existing hypovolaemia. Heparinization is required to reduce the risk of TE. Surgical treatment of OHSS is not recommended except in complications such as ovarian torsion and haemorrhage. VEGF antagonists may in future develop as a new form of treatment for OHSS.
• Supportive counselling and reassurance should be provided to woman and family. Conclusions
OHSS is a complication of ovarian stimulation that has risen over recent years with advances in technology and the global rise in consumerism for fertility treatment. Understanding its pathophysiology, strategies of prevention, and multidisciplinary approach to treatment are important for its appropriate management. Surveillance
Central, judicious reporting policy of OHSS for risk management and epidemiological survey are mandatory. Further reading
Aboulghar M, Evers J, Al-Inany H. IV albumin for preventing severe OHSS. Review Cochrane Collaboration 2008;2:1–12.
Adamson D, deMouzon J, Lancaster P, et al. International Committee for Monitoring Assisted Reproductive Technology (ICMART), World collaborative report, Fertil Steril 2006;85:1586–622.
Agrawal R, Sladkevicius P, Engmann L, et al. Serum VEGF and ovarian blood flow are increased in women with polycystic ovaries. Hum Reprod 1998;13:651–5.
Al-Inany H, Abou-Setta A, Aboulghar M. GnRH antagonist for ART. Cochrane review. Repro Med Online 2007;14:640–9.
Delvigne A, Rozenberg. Review of clinical course and treatment of OHSS. Hum Reprod Update 2003;9:77–96.
Fauser B, Diedrich K, Devroey P. (EVAR workshop). Predictors of ovarian response: progress towards individualised treatment in OI & ovarian stimulation. Hum Reprod Update 2008;14:1–14.
Griesinger G, Diedrich K, Devroey P, Kolibiankis E. GnRHa for final maturation in GnRH antagonist protocol: systematic review & meta analysis. Hum Reprod Update 2006;12:327–8.
Mathur R, Kailasam C, Jenkins J. Review of evidence base strategies to prevent OHSS. Hum Fertil 2007;10:75–85.
Rizk B. Epidemiology, pathophysiology, prevention and management of OHSS. In: Ovarian hyperstimulation syndrome. Cambridge University Press 2006: 3–210.
Soares S, Gomez R, Simon C, et al. Targeting VEGF system to prevent OHSS. Hum Reprod Update 2008;14:321–33.
Paediatric and adolescent problems Definitions
Adolescence is a variable period between childhood and adulthood characterized by rapid development in psychological, social, and biological domains (RCPCH 2003). The WHO defines adolescence as between 10 and 20 years. Children and adolescents may present with gynaecological problems that include menstrual disorders (oligo and amenorrhoea, irregular menorraghia. and dysmenorrhoea), delayed puberty, hyperandrogenism, vulvovaginitis, labial adhesions, and sexually transmitted diseases as well as, more rarely, ovarian failure after treatment of childhood malignancy and disorders of sexual differentiation (DSD).
Thelarche (breast development) and pubarche (development of pubic and axillary hair) usually occur 1 year before menarche and before 13 years. Menarche occurs at a mean of 13 years and less than 4 years after thelarche. Most cycles initially vary between 20 and 40 days with a median cycle length of 31 days and mean length of bleeding of 5 days (WHO 1986). Epidemiology
Nearly 25% of the UK population are children or adolescents. Up to 50% of adolescent cycles are anovular in the first year and it can take up to 7 years to establish a regular cycle. Clinical approach
Consultation
The consultation with an adolescent can be challenging; adolescents find it difficult to volunteer information and discuss sexually related issues, whereas doctors find that mothers often dominate, daughter and mother have different agendas, and adolescents use different language and have different values and perceptions. They also mature at different rates. The gynaecologist needs to make the adolescent central to the consultation. Sensitive involvement of the parents is important, but it is also essential to respect confidentiality: ask about sexual activity away from the parent. Summarize and agree management plans with the adolescent present; avoid separate conversations with the parents.
Diagnosis
History
In addition to the normal gynaecological history, questions should include birth history, growth and pubertal milestones, relevant symptoms (galactorrohea, headaches, hyperandrogenism, weight change) a detailed family history, dieting, stress, and exercise patterns. In certain presentations (for example vulvovaginitis, prepubertal bleeding, pelvic pain) it is important to explore sensitively the possibility of sexual abuse. Gynaecologists should try to assess psychological factors that may be impacting on physical symptoms and assess the parent–child or adolescent relationship.
Examination
This should include measurement of height and weight and compared with child centile charts and BMI and waist circumference in adolescents. Record Tanner staging, and Ferriman–Gallwey scores for hirsutism. The external genitalia can be inspected, with consent, for normality and virilization. Speculum and bimanual examination should only be performed in the sexually active. Rectal examination as an alternative to vaginal examination is not indicated.
Investigations
These depend on the presentation.
In oligo/amenorrhea, investigations include a pregnancy test, measurement of LH/FSH/E2/PRL/TFTs and androgens if hirsute (testosterone and 17-hydroxyprogesterone) and an USS pelvis. An MRI of the pelvis is helpful if a Müllerian duct anomaly (MDA) is suspected. If a MDA is confirmed then the renal tracts should be visualized. Check the karyotype if there is primary amenorrhea or ovarian failure. A dexamethasone suppression test will exclude Cushing’s syndrome.
In menorraghia, measurement of haemoglobin guides management. Coagulation abnormalities (including platelet dysfunction, von Willebrand’s factor deficiency) may occur in up to 47% of adolescents, so coagulation (PT, PTT, BT, PFA 100, and VWF) should be checked in those with acute menorraghia, menorraghia since menarche, positive bleeding history, and/or iron deficiency. In adolescents with an irregular cycle a menstrual calendar helps to clarify these; it is also a useful educational tool.
It is important to recognize rare conditions and manage or refer as appropriate.
Counselling
Management of most conditions involves patient (and parent) education, support and counselling for both the condition itself and its long-term effects on general health and fertility. Management of individual conditions
Common conditions
Vulvovaginitis
This is a common condition in prepubertal girls and is usually secondary to poor perineal hygiene. It is important to exclude a dermatological condition (e.g. lichen sclerosus), foreign body, or sexual abuse. An EUA with vaginoscopy (use a paediatric cystoscope) is indicated if the history is suggestive of a foreign body or if there is constant offensive vaginal discharge or vaginal bleeding. Vaginal bleeding is rare in young children. The differential diagnosis includes precocious puberty, tumours, foreign bodies, or trauma.
Labial adhesions
These are common and may present as ‘no vagina’. The diagnosis is made from the history and examination. No other investigations are indicated. Oestrogen cream applied at night will dissolve labial adhesions over 1–2 weeks. However, provided there is no interference with micturition, treatment is unnecessary apart from education to improve perineal hygiene. Surgical division should be avoided as this causes recurrence and scarring.
Amenorrhoea
Investigate when thelarche and pubarche are absent at 13 years or menarche delayed to more than 4 yrs after thelarche or if there is primary amenorrhoea at 15 years. Secondary amenorrhoea can be defined as no bleeds for over 6 months.
History, examination, and investigations should focus on establishing the cause. Treatment depends on the aetiology. Causes can be classified in terms of the hypothalamic pituitary ovarian pathway, for example weight-related, pituitary lesions, hyperprolactinaemia, polycystic ovarian syndrome (PCOS), ovarian failure, and DSD.
Oligomenorrhoea
Defined as cycles longer than 35 days, oligomenorrhoea is common in the first 2 years after menarche. If it fails to resolve, or bleeds are less frequent than every 3 months, further investigation is indicated. The most common cause is PCOS. Other causes include those listed above for amenorrhoea.
Hyperandrogenism
Causes include PCOS, congenital adrenal hyperplasia (CAH), Cushing’s syndrome, and adrenal secreting tumours of the ovary or adrenal gland.
Polycystic ovarian syndrome
PCOS often presents during adolescence and is diagnosed when patients have two out of the following three criteria: oligo or anovulation, hyperandrogenism (clinical or biochemical) and PCO morphology on ultrasound scan following the exclusion of other aetiologies including CAH, Cushing’s syndrome, or androgen secreting tumours (Fauser et al. 2004).
PCOS is managed by identifying and prioritizing the patients’ concerns and being aware of their long-term risks (type 2 diabetes, insulin resistance, dyslipidaemia, and endometrial hyperplasia). In adolescents, the main concerns relate to irregular menorraghia, hirsutism, and obesity. It is generally the adolescent’s mother who is concerned about her fertility. Weight loss and exercise should be encouraged in all adolescents with PCOS who have a BMI above the normal range, and those with a normal BMI should be encouraged to maintain this. If bleeds are less frequent than every 3 months then 3-monthly courses of progestogens or the combined oral contraceptive pill (COCP) should prevent the development of endometrial hyperplasia. If hirsute, then management may involve treatment with Dianette with or without additional antiandrogens (cyproterone acetate or finasteride) or spironolactone or metformin. Long-term screening of blood glucose and lipids should be considered. Evidence is lacking for the prophylactic use of metformin in adolescents with PCOS. However, there is a role for metformin in the subgroup of obese adolescents with PCOS who have signs of hyperinsulinanaemia (acanthosis nigricans) and in those with impaired glucose tolerance.
Menstrual dysfunction
Treatment, particularly if the adolescent is anaemic, may include the OCP, tranexamic acid (TEXA), cyclical progestogens, or rarely a Mirena IUS.
The acute bleed requires immediate circulatory management, volume replacement, haemostatic agents, and/or high doses of hormones (e.g. progestogens or more rarely IV premarin) with subsequent cyclical progestogens or the COCP.
Adolescents with learning difficulties and menstrual problems can be managed with continuous COCP, Depoprovera, or a Mirena IUS.
Dysmenorrohea/pelvic pain
Good history taking is key to the diagnosis and management of pelvic pain in the adolescent. Pregnancy and infection need to be excluded and the possibility of previous or current sexual abuse considered. Other causes of pelvic pain include endometriosis or Müllerian anomalies (for example a functioning non-communicating uterine horn), and laparoscopy to diagnose endometriosis and a magnetic resonance imaging (MRI) scan to clarify uterine anatomy may be indicated. Treatment includes non-steroidal anti-inflammatory drugs (NSAIDs), the COCP (which can be tricycled, especially if dysmenorrohea is present), Cerazette, or a Mirena IUS.
Ovarian cysts/masses
Even large cysts may resolve in adolescents. Provided tumour markers are negative (CA125, CEA, hCG, AFP, LDH) and the patient is asymptomatic; management should initially be conservative with scan follow-up. If surgery is indicated this should be performed laparoscopically with conservation of as much ovarian tissue as possible. If tumour markers are positive, gynaecological oncologists should be involved in further management.
Premature ovarian failure
Premature ovarian failure (POF) is common after treatment of childhood malignancy and also occurs in Turner’s syndrome and in some DSDs. The diagnosis is made when FSH and LH are elevated and oestradiol low on at least two occasions more than 1 month apart. Thyroid function tests, full blood count, and autoimmune screen (to include ovarian, thyroid, coeliac, adrenal antibodies, and intrinsic factor) should be checked annually. Induction of puberty using low-dose, sequentially increased oestrogen may be necessary. Consideration should be given to cryopreservation of oocytes or ovarian tissue prior to treatment for malignancy (Lobo 2005). This group of patients often requires counselling and psychological support.
Rare conditions
Precocious puberty
Menarche before 8 years is described as being ‘precocious’. Investigation and management is best organized in liaison with paediatric endocrinologists so that unusual and important diagnoses can be excluded.
Delayed puberty
Normal development with amenorrhoea may be caused by outlet obstruction (imperforate hymen, transverse vaginal septum), the Mayer–Rokitansky–Kuster–Hauser (MRKH) syndrome or resistant ovaries, or premature ovarian failure. Poor or absent development may be caused by anorexia, pituitary or hypothalamic lesions, or gonadal dysgenesis (e.g. Turner’s). Heterosexual development can occur in XY females, CAH, adrenal and ovarian tumours, and Cushing’s syndrome.
‘No vagina’
Children or adolescents who present with an ‘absent vagina’ may be a XY female, or have MRKH syndrome, CAH, a transverse vaginal septum, an intact hymen, or labial adhesions.
Disorders of sexual differentiation (previously referred to as intersex disorders)
Historically classification of these disorders has been confusing. A recent consensus group (Hughes et al. 2006) has attempted to clarify this. DSDs may be due to:
• abnormal genetic development
• germ cell failure
• failure to develop normal internal genitalia (Müllerian duct anomalies)
• failure to develop external genitalia (masculinization of female genitaliia or underdevelopment of male genitalia)
• deficiencies in hormonal biosynthesis.
These patients often have complex needs and are best managed in tertiary centres where there is an established multidisciplinary, multiprofessional DSD/intersex service with access to paediatric and adult endocrinologists, paediatric gynaecologists, paediatric and plastic surgeons, geneticists, and psychologists.
Management of the commoner conditions is described below. Most need genetic advice and psychological support. Disclosure of diagnoses must be handled sensitively. Currently, there is controversy over surgery, both its timing and need (Creighton and Minto 2001). A minimalist approach that aims to restore function (rather than anatomy) is increasingly favoured. HRT should be individualized and bone density monitored every two years in most conditions.
• Sex chromosome DSD, Turner’s syndrome (45,X, DSD, and variants): commonly presents with poor growth as a child, or later with delayed puberty, primary, or premature ovarian failure. Management includes optimization of growth, induction of puberty, hormone replacement, and screening for other health problems (e.g. cardiac, renal, thyroid and auditory problems) (Saenger et al. 2001). A few cases need gonadectomy (which should be performed laparoscopically) if Y chromosome mosaic material is present (45,X/46,XY). Girls with Turner’s should be provided with information about support groups and oocyte donation.
• 46,XY, DSD: this can be divided into disorders of gonadal (testicular) development (e.g. Swyer’s syndrome) or disorders in androgen synthesis or action (complete androgen insensitivity syndrome, 5-α-reductase deficiency, Leydig cell hypoplasia).
• Swyer’s syndrome (XY complete gonadal dysgenesis): presents with primary amenorrhoea or with a pelvic mass. Dysgenetic gonads require early removal as there is a high risk of malignancy. Subsequent HRT should include progestogens as these patients have a uterus. They can therefore carry a pregnancy conceived with donated oocytes and need appropriate counselling. Disclosure, genetics referral and psychological support are important.
• Complete androgen insensitivity syndrome (CAIS): this may present with inguinal herniae in a female child or with primary amenorrhoea. Disclosure is important but often difficult and psychological support helpful. Management involves laparoscopic gonadectomy, which can be deferred until after puberty, subsequent hormone replacement, with monitoring of bone density, creation of a functional vagina (generally with dilators, more rarely with surgery), genetic advice, and provision of information about support societies and surrogacy.
• 46,XX DSD: this includes disorders of ovarian development (gonadal dysgenesis) and of androgen excess (e.g. congenital adrenal hyperplasia). Other DSDs include MRKH syndrome, cloacal extrophy, and vaginal atresia.
• Congenital adrenal hyperplasia (CAH): CAH (salt losing or non-salt losing) commonly presents in the newborn with ambiguous genitalia. They are brought up as girls as they have normal internal genitalia and are potentially fertile. The main issues in the adolescent relate to menstruation, sexuality, fertility, and the need for further surgery or the use of dilators (Ogilvie et al. 2006). The effectiveness of treatment (steroids ±fludrocortisone) can be assessed by the control of the menstrual cycle and hyperandrogenism. There is currently debate about operations to restore the anatomy in babies with CAH and their timing. Many girls with CAH will require further surgery as adolescents/adults. Sexual dysfunction is common in these patients and it is important to plan surgery carefully.
• Müllerian agenesis (MRKH syndrome): this involves congenital aplasia of the uterus and upper part of vagina. Usually presents as primary amenorrhoea with normal secondary sexual characteristics. Ovaries and hormone levels are normal. A small amount of uterine tissue may sometimes be identified on MRI. Other anomalies (spinal/renal) should be excluded. Management may involve the creation of a vagina with dilators or surgery. Genetic advice is important. Surrogacy using their own oocytes can be discussed, although this has implications for resulting children. They often require psychological support.
• Müllerian duct anomalies: these include vaginal septae (longitudinal and transverse), uterus didelphys, and unicornuate uteri with rudimentary horns. MRI scans are useful in clarifying anatomy and EUAs with vaginoscopy may help in diagnosis. Remember associated renal anomalies. It is important to distinguish between an intact hymen (blue, bulging membrane) and transverse vaginal septum (pink flat vaginal skin), as excision of the latter requires a different surgical technique and patients should be referred to tertiary centres. If the septum is incompletely excised there is a high risk of vaginal stenosis and recurrence. Longitudinal septae can be excised if symptomatic. A functioning non-communicating uterine horn can cause dysmenorrhoea from haematometra and/or endometriosis and should be excised preferably laparoscopically. Management of other uterine anomalies rarely involves surgery. Conclusions
The healthcare encounter with the child or adolescent does provide an opportunity for healthcare education; adolescents in particular need to learn how to take responsibility for their own healthcare and to use healthcare systems appropriately. Gynaecologists need to be able to manage common conditions presenting in this age group as well as recognizing rarer and more complex problems that need onward referral and multidisciplinary care. Further reading
Creighton S, Minto C. Managing intersex. Editorial. BMJ 2001;323:1264–5.
Fauser B, Tarlatzis B, et al. The Rotterdam ESHRE/ASRM sponsored PCOS consensus workshop group. Revised 2003 consensus on diagnostic criteria and long term health risks related to polycystic ovary syndrome. Hum Reprod 2004;19:41–7 or Fertil Steril 2004;81:19–25.
General Medical Council (GMC). 0–18 years: guidance for all doctors. London: GMC 2007.
Hughes IA, Houk C, et al. Consensus statement on management of intersex disorders. J Pediatric Urology 2006;2:148–62.
Lobo, RA. Potential options for preservation of fertility in women. N Engl J Med 2005;353:64–73.
Ogilvie CM, et al. Congenital adrenal hyperplasia in adults: a review of medical, surgical & psychological issues. Clin Endo 2006;64:2–11.
RCPCH. Bridging the gaps. Intercollegiate Working party. 2003.
Saenger, P, Albertsson Wikland, K et al. Recommendations for diagnosis and management of Turner syndrome. J Clin Endo Metabol 2001;86:3061–9.
World Health Organization Task Force on Adolescent Reproductive Health. World Health Organisation multicenter study on menstrual and ovulatory patterns in adolescent girls. II. J Adolesc Health Care 1986;7:236–44.
Balen, A, Creighton SC, Davies MC, et al. (eds) Paediatric and adolescent gynaecology: a multidisciplinary approach. Cambridge: Cambridge University Press 2004.
Sanflippo JS, Muram D, Dewhurst J, Lee PA (eds). Pediatric and adolescent gynaecology. Philadelphia: WB Saunders 2001.
Garden AS, Topping J. Paediatric and adolescent gynaecology for the MRCOG and beyond. RCOG Press 2001. Internet resources
British Society of Paediatric and Adolescent Gynaecology: www.britspag.org.uk
British Association of Paediatric Surgeons: www.baps.org.uk
British Society for Paediatric Endocrinology & Diabetes: www.bsped.org.uk
The North American Society for Paediatric & Adolescent Gynaecology: www.naspag.org/index.html Patient resources
Turner Syndrome Society: www.tsss.org.uk
Congenital adrenal hyperplasia support group: www.ahn.org.uk
Androgen insensitivity syndrome support group: www.aissg.org The Daisy network. A support group for Premature Ovarian
Failure: www.daisynetwork.org.uk
Polycystic ovary syndrome Definition
Polycystic ovary syndrome (PCOS) is a syndrome of ovarian dysfunction with the cardinal features hyperandrogenism and polycystic ovarian morphology (PCO) morphology. It is a clinical definition based on the presence of at least two of the following features after the exclusion of other aetiologies:
• PCO
• oligo/anovulation or oligo/amenorrhoea
• clinical or biochemical hyperandrogenism (PCOS Workgroup 2004).
This definition therefore includes women who have PCO and androgenic symptoms but regular menstrual cycles, as well as those who have the ‘classical’ symptoms of menstrual disturbance and hyperandrogenism. It excludes asymptomatic women who have an incidental finding of PCO.
The commonest symptoms of PCOS are irregular menses and hirsutism, with up to 75% of affected women having either or both. Acne features in up to a third. Thinning of the scalp hair in a male pattern may also be present. Obesity is not a symptom of PCOS but it is a common association. Epidemiology
PCOS is the commonest endocrine disorder in women of reproductive age and has an estimated prevalence of 5–10% in this age group. By contrast, 23% of asymptomatic women (who therefore do not have PCOS) will have the ultrasound finding of polycystic ovarian morphology (Polson et al. 1988). Pathology
The PCO has an increased number of antral follicles which have arrested their development at a size of less than 10 mm in diameter. This is due, at least in part, to high serum luteinizing hormone (LH) levels, high insulin levels (insulin is a weak gonadotrophin), or a combination of both. These two hormones also drive the production of androgens from the theca cells of these follicles, which is increased in those from PCO (Gilling-Smith et al. 1994).
Women with PCO are generally more insulin resistant (due to a post-receptor abnormality) and have higher insulin levels (due to hypersecretion from pancreatic beta-cells) than weight-matched controls with normal ovarian morphology, although the difference is most marked in those with irregular cycles (Robinson et al. 1993). This abnormality of insulin metabolism is thought to be one of the predisposing factors to obesity in PCOS. Obesity, which also raises serum insulin levels in response to insulin insensitivity (via a reduction in the number of insulin receptors), potentiates the abnormality. Thus the menstrual cycles of a woman with PCOS usually become more prolonged (reflecting anovulation) as her weight increases above the norm. These metabolic factors do not fully explain the appearance of the PCO. Abnormalities of follicle number and development are also present during the early, gonadotrophin-independent pre-antral stages of follicle growth (Webber et al. 2003). Aetiology
PCOS is an inherited disorder (Franks et al. 2009), with a presentation similar to that of an autosomal dominant condition. In fact, it is likely to be polygenetic, although the genes responsible are yet to be identified. Long-term consequences
• Diabetes: obese women with PCOS are at increased risk of gestational diabetes, impaired glucose tolerance, and diabetes. For women with a BMI ≥30 kg/m2 the risk of developing impaired glucose tolerance is 30% per year.
• Cardiovascular disease: hypertension, an unfavourable lipid profile, and reduced endothelial elasticity are all more common in obese women with PCOS. However, a large epidemiological study did not show an increase in cardiovascular mortality in women with documented PCOS. Possible explanations for this finding include a protective effect on the cardiovascular system of PCOS, an improvement of cardiovascular risk factors by wedge resection (a procedure that had been performed on the majority of women included in the study) or that the average age of follow-up (56 years old) was too young to demonstrate any attributable mortality.
• Endometrial carcinoma: amenorrhoeic women with PCOS have an increased risk of endometrial carcinoma, especially if obese. It is not clear from the published literature whether this is due to an unopposed oestrogen effect alone or simply that this group of PCOS patients share the general risk factors for endometrial carcinoma (obesity, nulliparity, diabetes).
• Psychological: psychological morbidity is secondary to the symptoms of PCOS (particularly acne, facial hirsutism and infertility). Whether there are direct psychological consequences of elevated serum androgens associated with PCOS is unclear. Clinical approach
Diagnosis
The diagnosis of PCOS is clinical. Investigations are aimed at excluding other causes for the symptoms.
History
• Menstrual cycle: age of menarche, cycle length, variability, duration and heaviness of bleeding. Anovulatory cycles can present with irregular vaginal spotting or episodes of prolonged or heavy bleeding.
• Weight variations and associated changes in menstrual cycle.
• Acne or hirsutism and duration of symptoms: rapidly developing hirsutism suggests an androgen secreting tumour.
• Past obstetric history: gestational diabetes, birthweight.
• Contraception and/or plans to conceive.
• Past medical history: diabetes, hypertension, thromboembolism.
• Family history: diabetes in first degree relatives.
Examination
• Weight, height, calculate BMI, ±waist circumference.
• Presence or absence of hirsutism: male pattern terminal hair growth. Enquire about any areas that have been treated by hair removal.
• Presence or absence of acne and greasy skin.
• Acanthosis nigricans (slightly raised, velvety, pigmented areas at back of neck or in axillae): a reliable indicator of insulin resistance.
• Pattern of scalp hair thinning.
• Signs of virilisation (deepening of voice, clitoromegaly) suggest other causes of hyperandrogenaemia.
• Cushingoid appearance suggests Cushing’s syndrome and not PCOS.
Investigations
Blood tests
• Follicle stimulating hormone (FSH), LH, and oestradiol in early follicular phase if cycling or random timing if not. FSH and oestradiol are normal in PCOS. LH may be raised but an elevated FSH ratio is not required to make the diagnosis.
• Testosterone or androstenedione should be measured but not both. In most laboratories, testosterone is an automated assay and therefore cheaper. There is no benefit in measuring Sex hormone-binding globulin (SHBG) to calculate the free androgen index since SHBG falls as central adiposity increases. This can be assessed visually or by recording the waist circumference.
• Assess thyroid function if there is oligo- or amenorrhoea. Measure prolactin if menstrual cycle is disturbed. Prolactin may be mildly elevated (≤1000) in PCOS with irregular cycles and is of no clinical significance.
• Measure fasting lipids if BMI ≥30 kg/m2.
• Perform oral glucose tolerance test (OGTT) if BMI ≥30/m2, BMI of 26–30 kg/m2 and first-degree relative with Type 2 diabetes; all Asian women with BMI ≥26 kg/m2.
Preconception OGTT is informative for the above groups.
• Serum insulin is of no clinical benefit.
Ultrasound scan
• Ovarian morphology is best assessed with transvaginal ultrasound, especially if the BMI is raised.
• An ovary can be described as polycystic if there are 12 or more antral follicles measuring 2–9 mm and/or the ovarian volume is increased above 10 mL (volume = 0.5 ? length ? width ? thickness) (PCOS Workgroup 2004). Although both ovaries usually share the same appearance, the morphology can be described as PCO if only one meets these criteria (but see differential diagnosis below).
• Endometrial thickness should be assessed, particularly if there is oligo- or amenorrhoea.
Differential diagnosis
These only need to be formally excluded if clinically indicated.
• Congenital adrenal hyperplasia can usually be excluded by measuring serum 17-hydroxyprogesterone. If that is elevated, a short Synacthen test should be performed measuring 17-hydroxyprogesterone, cortisol, and androstenedione at 0, 30, and 60 minutes.
• Cushing’s syndrome can be excluded measuring urinary cortisol in two 24-hour collections.
• An androgen-secreting tumour should be suspected if there is a short history of androgenic symptoms and/or a high serum testosterone (>5 nmol/L). Rarely, unilateral PCO appearance can be due to an ovarian tumour. Detailed ultrasound examination of the ovaries should be performed together with a magnetic resonance imaging of the adrenal glands. Management
The treatment of PCOS remains symptomatic and some treatments are mutually exclusive, e.g. antitestosterone treatment and conception.
• Weight loss should be advised in all cases where the BMI is greater than ideal. All symptoms of PCOS are exacerbated by obesity and will improve with weight loss, including androgenic symptoms. Patients should be counselled that it will be difficult and realistic targets should be agreed. Ovulation and conception rates increase with a reduction only 5–10% of the starting weight. Although there is some limited evidence that low carbohydrate diets may be beneficial, it is much more important that a sustainable change in lifestyle is achieved than any particular type of diet is followed. Exercise is vital to success. Referral to an appropriate dietician may help as can weight management groups. Consideration should be given to pharmacotherapy and bariatric surgery if appropriate.
• Acne and hirsutism can be treated with anti-androgens: daily spironolactone in the dose range 50–150 mg orally or cyproterone acetate 25–50 mg orally for the first 10 days of the menstrual cycle are the commonest. Flutamide 250 mg is an alternative but has no advantage and may be more likely to cause abnormal liver function tests. Reliable contraception must be used during treatment with any anti-androgen due to the potential detrimental effect on the development of a male fetus. The main disadvantage of any anti-androgen is that they often cause further menstrual cycle disturbance. Cycle control is best in combination with an oestrogen, such as Dianette (which contains cyproterone acetate) or Yasmin (which contains drospirenone, a derivative of spironolactone). This combination also provides the required contraception and raises serum SHBG levels, thereby reducing the effective concentration of active androgen. When treating acne, results may be seen in 3–6 months but an improvement in hirsutism may take 9–12 months. Hair removal may still be required but treatments intervals will be prolonged. Suppression of hirsutism may be more rapid with the addition of cyproterone acetate to Dianette (for the first 10 days of each packet), although the end result is the same as with Dianette alone. However, additional cyproterone acetate may be required in the treatment of acne.
• Eflornithine cream (Vaniqa) blocks the action of the enzyme required to make hair and so reduces or stops its growth. It is useful for small areas such as on the face. It can be used in combination with an anti-androgen and like these drugs is only effective during regular use.
• Finasteride blocks the peripheral conversion of testosterone to its active counterpart dihydrotestosterone. Addition of 5 mg daily to anti-androgen treatment may be beneficial in extreme cases of hirsutism although, like flutamide, it is unlicensed for this treatment and should probably be reserved for use within specialist clinics.
• Alopecia may be stabilized with an anti-androgen although new hair growth may not occur. Serum ferritin should be kept above 70 ng/L to optimize hair growth.
• Menstrual disturbance can be treated with the contraceptive pill or with a cyclical progesterone, medroxyprogesterone acetate 10 mg for 10 days per calendar month being the most usual choice as it has few androgenic side-effects. If the woman has no androgenic symptoms, she can be treated with any contraceptive pill, although those containing norethisterone are generally best avoided. The Mirena intrauterine system can also be used. Endometrial protection should be advised using any of these methods if episodes of amenorrhoea repeatedly last longer than 3 or 4 months. Otherwise ultrasonographic measurement of endometrial thickness with sampling if required should probably be done annually.
• Induction of ovulation is covered in Chapter 12 p. 578. Long-term follow-up
• Those at risk of diabetes should have annual OGTT.
• Amenorrhoeic patients should have an annual ultrasound assessment of endometrial thickness with endometrial sampling if necessary. Those with irregular vaginal spotting or episodes of prolonged or heavy bleeding should be similarly assessed.
• Deranged liver function rarely occurs with spironolac-tone or cyproterone acetate, but annual liver function tests should be routine along with serum electrolyte measurement for those on spironolactone due to its diuretic action.
• Women should be advised not to rely on anovulatory cycles for contraception. When wanting to conceive, PCOS women with menstrual irregularity should be referred for cycle monitoring and ovulation induction 3–6 months after discontinuing contraception, depending on cycle length. Further reading
Franks S, Webber LJ, Goh M, et al. Ovarian morphology is a marker of heritable biochemical traits in sisters with polycystic ovaries. J Clin Endocrinol Metab 2008;93:3396–402.
Gilling-Smith C, Willis D, Beard RW, Franks S. Hypersecretion of androstenedione by isolated theca cells from polycystic ovaries. Clin Endocrinol 1994;47:93–9.
PCOS Workgroup. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Hum Reprod 2004;19:41–47/Fertil Steril 81: 19–25.
Polson DW, Adams J, Wadsworth J, Franks S. Polycystic ovaries: a common finding in normal women. Lancet 1988;1:870–2.
Robinson S, Kiddy D, Gelding SV, et al. The relationship of insulin insensitivity to menstrual pattern in women with hyperandrogenism and polycystic ovaries. Clin Endocrinol 1993;39:351–5.
Webber LJ, Stubbs S, Stark S, et al. Formation and early development of follicles in the polycystic ovary. Lancet 2003;362:1017–21.
Wild S, Pierpoint T, McKeigue P, Jacobs H. Cardiovascular disease in women with polycystic ovary syndrome at long-term follow up: a retrospective cohort study. Clin Endocrinol 2000;52:595–600. Internet resources
www.pcos-uk.org.uk Patient resources
www.verity-pcos.org.uk
Preimplantation genetic diagnosis Definition
Preimplantation genetic diagnosis (PGD) is a recent alternative to prenatal diagnosis and termination of pregnancy (qv) (see chapter 12.37) which may be suitable for individuals or couples who carry a significant risk of transmitting a serious genetic disorder to their offspring (Lashwood 2005; Braude et al. 2002). It differs from prenatal diagnosis in that the genetic test is performed on an egg, or an early developing embryo in vitro prior to implantation into the uterus, and before pregnancy is initiated. The procedure
PGD requires a representative sample or biopsy to be taken as a single cell from an early (day 3 or 5) embryo created in vitro by the use of IVF (qv) (see chapter 12.19) and tested for the specific disorder. IVF is undertaken, not necessarily because of infertility, but in order to gain access to early embryos for the purpose of PGD. Indications
There are three main indications for the use of PGD.
• In autosomal single gene disorders (recessive or dominant; early or late onset).
• In sex-linked gene disorders (carried by female but expressed in males).
• For chromosome rearrangements, commonly reciprocal or Robertsonian translocations. These present with physical or mental disability or repeated miscarriage due to inheritance of unbalanced chromosomal products. Clinical approach
In autosomal recessive gene disorders the embryo must inherit a copy of both the mutated maternal and paternal recessive genes for the disorder to manifest. Carrier embryos, which will have only one copy of the mutated gene and will usually be symptom free, may thus also be considered for replacement after PGD. This is not the case in autosomal dominant gene disorders where carriage of a single copy of the mutated gene (either matermal or paternal) is sufficient to result in the disease. Some genetic diseases manifest immediately or shortly after birth and may be lethal (e.g. spinal muscular atrophy), whereas others may result in chronic disease (e.g. cystic fibrosis). Others may not manifest until well into adult life and are thus considered late onset (e.g. Huntington’s disease). Each of these examples presents different moral judgments as to whether the conditions are appropriate grounds on which to discard mutation-carrying embryos (El-Toukhy et al. 2008). The process
• The woman’s ovaries are stimulated to produce multiple Graafian follicles from which the oocytes are retrieved transvaginally using ultrasound guided needle aspiration.
• The oocytes are exposed to the partners sperm in vitro (IVF qv) (see chapter 12.19) or are individually injected with single sperm (ICSI qv) (see chapter 12.17). ICSI is preferable where a molecular rather than a FISH-based test is to be performed on the biopsy in order to minimize DNA contamination by extraneous sperm.
• Only those embryos that have reached 6–10 cells on day 3 and of sufficient morphological calibre are suitable for biopsy.

Fig. 12.32.1 Single cell being removed as a biopsy from a day 3 human preimplantation morula for genetic testing. See also colour plate section.
• A hole is made in the zona pellucida of embryo using acid or a laser, and one, sometimes two, cell is removed (Fig. 12.32.1) and is subjected to the genetic test. For a molecular based test, the DNA is amplified using a PCR to provide sufficient material for assay; or for a FISH based test, the cell is spread and stained for cytogenetic analysis (Fig. 12.32.2).
• Only those embryos found free of the mutation or chromosomally normal are considered for replacement into the uterus in order to generate a pregnancy. Variations
• Polar body biopsy: the first and second polar bodies can be removed from the oocyte retrieved from the follicle on which a genetic test can be performed (Verlinsky 1990). This has the advantage of assessing the genetic status of the egg before any postzygotic changes during cleavage may have occurred. However, it is less reliable, more difficult to perform, and is only useful in recessive conditions or maternally inherited dominant conditions, and for some aneuploidies and chromosomal rearrangements (Fig. 12.32.3).

Fig. 12.32.2 Principle of preimplantation genetic testing. See also colour plate section.
• Blastocyst biopsy: the embryo is biopsied on day 5 when it has formed the immediate preimplantation stage and contains many more cells. It thus has the advantage that more cells can be removed safely, providing a more reliable test (McArthuret et al. 2008). The disadvantage is that the result is needed within 24 hours so that an unaffected blastocyst can be transferred within the implantation window (by day 6).
Fig. 12.32.3 Stages at which biopsy can be undertaken for PGD. See also colour plate section.

Estimate of use
Although it is estimated that some 10 000 cases of PGD for serious genetic disorders have been performed worldwide since its first use in 1990 (Handyside et al. 1990; Verlinsky et al. 2004), its use is trivial compared with the number of IVF cycles performed for infertility each year (33 000 per year in the UK alone, see Table 3.19.1). PGD should be distinguished from screening for sporadic age-related aneuploidies (aneuploidy screening, preimplantation genetic screening; PGS), which also uses embryo biopsy as an adjunctive fertility enhancing procedure. Chromosome analysis by FISH or CGH of biopsies is used in order to try and improve outcome of IVF in those older infertile patients with repeated implantation failure, or repeated miscarriage (Gianaroli et al. 2005). Despite its ubiquitous use, it is the most common reason given for embryo biopsy internationally, randomized trials have cast significant doubt over its efficacy and safety (Jansen et al. 2008; Mastenbroek et al. 2008,10). Further reading
Braude P, Flinter F. Use and misuse of preimplantation genetic testing. BMJ 2007;335:752–4.
Braude P, Pickering S, Flinter F, Ogilvie CM. Preimplantation genetic diagnosis. Nat Rev Genet 2002;3:941–53.
Braude P. Preimplantation diagnosis for genetic susceptibility. N Engl J Med 2006;355:541–3.
Edwards RG. Ethics of PGD: thoughts on the consequences of typing HLA in embryos. Reprod Biomed Online 2004;9:222–4.
El-Toukhy T, Williams C, Braude P. The ethics of preimplantation genetic diagnosis. Obstet Gynaecol 2008;10:49–54.
Gianaroli L, Magli MC, Ferraretti AP, et al. The beneficial effects of preimplantation genetic diagnosis for aneuploidy support extensive clinical application. Reprod Biomed Online 2005;10:633–40.
Goossens V, Harton G, Moutou C, et al. ESHRE PGD Consortium data collection IX: cycles from January to December 2006 with pregnancy follow-up to October 2007. Hum Reprod 2009 24: 1786–1810.
Handyside AH, Kontogianni EH, Hardy K, Winston RM. Pregnancies from biopsied human preimplantation embryos sexed by Y-specific DNA amplification. Nature 1990;344:768–70.
Jansen RP, Bowman MC, de Boer KA, et al. What next for preim-plantation genetic screening (PGS)? Experience with blastocyst biopsy and testing for aneuploidy. Hum Reprod 2008;23:1476–8.
Lashwood A. Preimplantation genetic diagnosis to prevent disorders in children. Br J Nurs 2005;14:64–70.
Mastenbroek S, Scriven P, Twisk M, et al. What next for preimplantation genetic screening? More randomized controlled trials needed? Hum Reprod 2008;23:2626–8.
McArthur SJ, Leigh D, Marshall JT, et al. Blastocyst trophectoderm biopsy and preimplantation genetic diagnosis for familial monogenic disorders and chromosomal translocations. Prenat Diagn 2008;28:434–42.
Verlinsky Y, Cohen J, Munne S, et al. Over a decade of experience with preimplantation genetic diagnosis: a multicenter report. Fertil Steril 2004;82:292–4.
Verlinsky Y, Ginsberg N, Lifchez A, et al. Analysis of the first polar body: preconception genetic diagnosis. Hum Reprod 1990;5:826–9. Internet resources
ESHRE PGD consortium: www.eshre.com/ESHRE/English/SIG/Reproductive-Genetics/PGD-Consortium/page.aspx/201
Preimplantation Genetics Diagnosis International Society: www.pgdis.org/
Sex Selection and PGD: ASRM statement: www.asrm.org/Media/Ethics/Sex_Selection.pdf
HFEA information on Genetic Testing of Embryos: www.hfea.gov.uk/172.html
Premature ovarian failure Definition
Premature ovarian failure (POF) is an ovarian defect characterized by primary or secondary amenorrhea before the age of 40 years. Approximately 1% of women under 40 years of age, 0.1% of women under 30 years of age, and 0.01% of women under 20 years of age suffer from POF. The cessation of ovarian function after puberty and before the age of 40 years strongly interferes with fertility and family planning. In most instances the aetiology is unknown but several specific causes have been identified so far. POF can be primary (spontaneous POF) or secondary (induced by radiation, chemotherapy, or surgery). Although the aetiology is very heterogeneous, the treatment and principles remain the same.
Cure rates for cancers in young women continue to improve, and therefore it is likely that the incidence of POF patients will rise rapidly. Aetiology
The causes of POF are highly heterogeneous. There are two ways that ovarian failure can occur prematurely: failure to attain the appropriate peak follicle number; and accelerated loss of oocytes and follicles.
Many cases follow treatment for neoplastic diseases such as leukaemia, non-Hodgkin lymphoma, and ovarian/cervical carcinoma. Different chemotherapeutic agents, alkylating cytotoxics in particular, have the potential to cause progressive and irreversible damage to the ovaries. The age of the woman and the dose of chemotherapy and/or radiation are the major predictive factors in the development of ovarian dysfunction. When ovarian failure presents with primary amenorrhea, approximately 50% will be associated with an abnormal karyotype. Two genes (POF1, POF2) have been localized on the basis of deletions in various patients and families. The most common X chromosome abnormality is Turner’s syndrome, which accounts for 1 in 2000 female live births.
Of the women with POF, 10–30% have a concurrent autoimmune disease. The most common is hypothyroidism. There is also an association with Crohn’s disease, rheumatoid arthritis, myasthenia gravis, and systemic lupus erythematosis. However, most cases present with secondary amenorrhea and are classified as spontaneous POF. It is not uncommon to have a positive family history but there are still few epidemiological data. Clinical presentation
The main symptom in patients with premature ovarian failure is the cessation of menses before the age of 40 years. The symptoms vary from patient to patient and they may occur abruptly or spontaneously or develop gradually over several years. There appears to be no characteristic antecedent menstrual history. Some women develop amenorrhoea acutely after having established regular menses; some women report failure of menstruation after discontinuation of contraceptives or after completion of a pregnancy. Some women present with an irregular bleeding pattern before becoming amenorrheic. Hot flushes can be a prodromal symptom before the development of ovarian dysfunction and vasomotor symptoms, sleep disturbances, vaginal dryness, decreased libido, mood changes, and fatigue can be a result of hypo- oestrogenism. Young women who have not received oestrogen treatment are at high risk for osteoporosis of the trabecular bone of the spine with associated fractures and height loss.
Infertility is an obvious and mostly irreversible consequence of POF. There are few cases of temporary premature ovarian failure reported in the literature but the chance of subsequent spontaneous conception is 5%. There are no therapies to improve ovarian function and the only method of achieving a pregnancy is fertilization of a donor oocyte. Diagnosis
The definition of premature ovarian failure is cessation of ovarian function in women less then 40 years of age with primary or secondary amenorrhea and high follicle-stimulating hormone (FSH) levels. The first challenge is to make the diagnosis of premature ovarian failure in a timely manner. It is a difficult diagnosis for women to accept and a carefully planned and sensitive approach is required when informing women of their diagnosis. Alzubaidi et al. (2002) quoted in their paper that 50% of women with secondary amenorrhea saw three or more clinicians before any laboratory testing was performed; 25% of women presenting with secondary amenorrhea in a general gynaecology clinic have premature ovarian failure. As a guide, it is recommended that women younger then 40 years of age suffering 3 or more months without periods should have appropriate evaluation in their first clinic appointment after excluding pregnancy. Initial evaluation
• At the initial visit a thorough history should be taken focusing on the positive family history and concurrent autoimmune disorders.
• Hormone levels (LH/FSH, oestradiol, prolactin, TSH/T4) should be performed at least 2 occassions, and 6 weeks apart.
• Peptide factors (inhibin B and anti-Müllerian Hormone) of ovarian origin may be useful to determine the follicular reserve especially if fertility is an issue
• Karyotyping is only of interest for women with primary amenorrhoea to exclude any chromosome defects.
• Antibody screening for ovarian antibodies shows positive immunofluorescence in a few women.
• Pelvic scanning to exclude any pathology in the uterus and ovaries and to measure ovarian volume.
• Bone mineral density (BMD): estimation of BMD through DEXA. Treatment
POF is a devastating diagnosis and many young women undergo a reactive depression in association with their diagnosis. The associated infertility is a major life change that often generates a series of symptoms similar to grief reaction. The clinician is confronted with communicating information about a sudden and unexpected diagnosis. Fogarty et al. (1999) demonstrated in their controlled study that simple statements of concern, which take very little time, can go a long way to helping women see their clinician as being more caring, sensitive, and compassionate.
The management of women with POF should be multidisciplinary with professionals from the various specialities providing the appropriate care to meet the different needs of these women.
The initial concern of women with premature ovarian failure is the need to replace oestrogen to relieve symptoms of oestrogen deficiency, maintain bone density, and reduce the risk of cardiovascular disease. Many types and route of administration of oestrogen are available and the pros and cons should be discussed. The choice of oestrogen and route of administration must be made on an individual basis. There are no controlled studies regarding the ideal hormone replacement strategy for women with premature ovarian failure. In our own database of women with premature ovarian failure, 70% of women are on oral treatment. This seems to be the most convenient way for these young women as it is easier to administer than the transdermal route in the form of a patch. On the other hand, the latter is a more physiological route of administration. Women on oestrogen treatment still need progestogen for the prevention of endometrial hyperplasia. Progestogen can be taken cyclically or continuously from an intrauterine system (Mirena IUS).
It is important to counsel women taking HRT about the possibility of a return of ovarian function and the 5% risk of pregnancy. Contraception should therefore be mentioned for women who do not want to get pregnant. Future objectives
A multidisciplinary working group should be established to
• identify clinics with premature ovarian failure patients
• develop a national register of premature ovarian failure patients
• establish national guidelines for the treatment of premature ovarian failure patients
• propose future research to determine optimum therapeutic regimens. Summary points
• Young women who develop premature ovarian failure have unique needs that require special care. A dedicated multidisciplinary clinic will provide ample time and the appropriate professionals to meet the needs of these emotionally traumatized women.
• The menstrual cycle is a reliable biological marker of hypothalamo-pituitary-gonadal function; disruption of regular cycles should be investigated with proper endocrine testing.
• The delay in diagnosis contributes to reduced bone density by delaying appropriate oestrogen therapy.
• HRT in POF women simply replaces ovarian hormones that should normally be produced at this age and it is of paramount importance that the women understand this in view of the general risks on HRT over the age of 50 years.
• Approximately 50% of young women with premature ovarian failure have intermittent and unpredictable ovarian function and 5% may even conceive spontaneously and unexpectedly.
• Learning the diagnosis of premature ovarian failure can be emotionally traumatic and difficult for women, therefore clinicians should spent more time with them and provide more information about their condition.
• Counselling should include explanation that remission and spontaneous pregnancy could still occur and the difference between POF and menopause should be emphasized. Further reading
Alzubaidi NH, Chapin HL, Vanderhoof VH, et al. Meeting the needs of young women with secondary amenorrhea and spontaneous premature ovarian failure. Obstet Gynecol 2002;99:720–5.
Bondy CA, Bakalov VK. Investigation of cardiac status and bone mineral density in turner syndrome. Growth Horm IGF Res 2006; 16(Suppl A): S103–8.
Coulam CB. Premature gonadal failure. Fertil Steril 1982;38:645–55.
Falsetti L, Scalchi S, Villani MT, Bugari G, Premature ovarian failure. Gynecol Endocrinol 1999;13:189–95.
Fogarty LA, Curbow BA, Wingard JR, et al. Can 40 seconds of compassion reduce patient anxiety? J Clin Oncol 1999;17:371–9.
Horner E, Kay A, Mohan E, Panay N. Management of women with premature ovarian failure at a main teaching hospital. Maturitas 2006; 54S: 50.
Lobo RA. Benefits and risks of estrogen replacement therapy. Am J Obstet Gynecol 1995;173:982–9.
Massin N, Czernichow C, Thibaud E, et al. Idiopathic premature ovarian failure in 63 young women. Horm Res 2006;65:89–95.
Mishell DRJ, Stenchever MA, Droegemueller W, Herbst AL, Emotional aspects of gynecology. In: Comprehensive gynecology. St Louis: Mosby 1997: 171–95.
Nelson LM, Covington SN, Rebar RW. An update: spontaneous premature ovarian failure is not an early menopause. Fertil Steril 2005;83:1327–32.
Panay N, Fenton A, Premature Ovarian Failure: a growing concern, Climacteric. 2008, 11: 1–3
Panay N, Kalu E. Mangement of premature ovarian failure. In: Best practice and research clinical obstetrics and gynaecology. 2008 1–12.
Portnoi MF, Aboura A, Tachdjian G, et al. Molecular cytogenetic studies of Xq critical regions in premature ovarian failure patients. Hum Reprod 2006;21:2329–34.
Singer, Hunter. Premature Menopause: a multidisciplinary approach 2000.
Sybert PV, McCauley E, Turner’s syndrome. N Engl J Med 2004;351:1227–38.
Van Kasteren YM, Schoemaker J. Premature ovarian failure: a systematic review on therapeutic interventions to restore ovarian function and achieve pregnancy. Hum Reprod Up Date 1999;5:483–92. Internet resources
Royal College of Obstetricians and Gynaecologists: www.rcog.co.uk
The British Menopause Society: www.thebms.org.uk
The Daisy Network: www.daisynetwork.org.uk
Early Menopause UK: www.earlymenopause.org
International Menopause Society: www.imsociety.org
Premenstrual syndrome Definition
Premenstrual syndrome (PMS) has been defined as distressing physical, behavioural, and psychological symptoms not due to organic disease, which regularly occur during the same phase of each menstrual cycle and which significantly regress or disappear during the remainder of the cycle. The typical psychological symptoms can include anxiety, anger, depression, and irritability. Physical symptoms consist of bloating, weight gain, headaches, breast tenderness, and joint or muscle pain. The symptoms of PMS markedly interfere with work, regular activities, and/or relationships with others. Epidemiology
Recent studies suggest that severe PMS affects 12–30% of menstruating women, with prevalence estimates depending on the diagnostic criteria employed.
Most women have one or more mild emotional or physical symptom in the premenstrual phase of their cycle; 5–8% have moderate to severe symptoms in association with substantial distress and interference with normal activities to an extent that interpersonal relationships can breakdown (Freeman 2007). Some studies even suggest that up to 20% of all women in their reproductive years have premenstrual complaints that could be regarded as clinically relevant (BorensteinJ et al. 2003).
Retrospectively, many adult women have noted the onset of their premenstrual symptoms as teenagers (Keye 1983). However, the peak age of presentation with severe PMS symptoms is mostly in the late 20s, but many women state they have been symptomatic for as long as 10 years before seeking advice or receiving treatment (Robinson and Swindle 2000). Pathophysiology and aetiology
Approximately 50% of women experience a few mild symptoms for several days in the luteal phase and probably should not be diagnosed as suffering from PMS (Johnson 2004).
The exact cause of the condition is unknown, although it is almost certainly due to hormonal changes which follow ovulation or even anovulatory mid-cycle ovarian activity.
The symptoms are mostly triggered by the rise and fall of ovarian hormones after ovulation in predisposed women. The levels of sex steroids, oestrogen, progesterone, and testosterone are normal but women with PMS may be more vulnerable to normal fluctuations. Women with PMS show an alteration in their GABA receptor complex response. Studies have demonstrated reduced GABA receptor sensitivity and reduced plasma GABA levels in the luteal phase. Serotonin dysregulation with reduced serotonergic function in the luteal phase offers some plausible explanation for many cases of PMS.
There is a clear picture of ‘reproductive depression’ in women due to hormonal fluctuations that should be more frequently recognized (Studd and Panay 2004). There are women vulnerable to changes of ovarian hormones whose psychological symptoms start at puberty, are worse before a period, improve markedly during pregnancy, and are worse after delivery. The symptoms are worse as their periods return and in the few years before the cessation of periods. They exhibit the ‘triad of hormone responsive mood disorders’: premenstrual depression, postnatal depression, and perimenopausal depression.
The importance of ovulation in the aetiology of PMS is clear from the observation that women with PMS do not have symptoms before puberty, after the menopause, or during pregnancy, when they have no cyclical fluctuation of their hormone levels. They are also asymptomatic following hysterectomy and oophorectomy, many choosing to go without oestrogen replacement because they prefer to have the climacteric symptoms of hot flushes and night sweats instead of PMS symptoms. However, if the uterus is removed with conservation of ovaries, the cyclical symptoms remain in the form of PMS symptoms or menstrual migraine (without periods). Clinical manifestations and diagnosis
More than 150 symptoms of PMS have been described in the literature, ranging from mild symptoms to those severe enough to interfere with normal life (Cronje and Studd 1989).
The physical symptoms consist of breast discomfort, headaches, bloating, and weight gain. Even more distressing are the psychological symptoms of irritability, irrational, aggressive, sometimes violent behaviour, depression, loss of self-confidence, loss of energy, and loss of libido. These may occur for up to 10–20 days per month following ovulation usually ceasing ‘like flicking a switch’ on the first day of menstruation. However, they may well have menstrual headaches or, like any women, heavy painful periods during this time, so they may have only about 7 good days a month. This question of ‘how many good days a month do you have?’ is important as it gives a measure of the severity of the condition and a baseline when assessing any improvement with therapy.
Correct diagnosis is crucial in the management of PMS. This cannot be accurately established by retrospective evaluation but needs to be made with daily prospective documentation of relevant symptoms for at least two cycles (symptom questionnaire). The initial completed questionnaires should be kept to give an objective indication of response to therapy. Treatment
There is no single treatment universally acceptable as effective. Many treatment options have been touted as effective for PMS but only a few are supported by clinical evidence. Lifestyle changes
Prior to any medical treatment a healthy lifestyle of reduced alcohol, caffeine, and nicotine intake, regular exercise and low fat and high-fibre diet should be the first step. Social and environmental factors can aggravate PMS symptoms. During holidays PMS symptoms seem to be less severe than during daily life. Diet plays a crucial role in the treatment of PMS and it is believed that many women experience exacerbated symptoms of PMS when their blood sugar is not under control. Herbal preparations and other treatments
In addition to dietary changes adding specific supplements such as vitamin B6, calcium, magnesium and evening primrose oil can improve PMS symptoms. Regular exercise increases the neurotransmitter endorphin that is associated with mood changes. Complementary and alternative therapies (CAM) are widely used but in fact there is very little scientific data to support the use of CAM in PMS (Watson et al. 1989). These remedies are all commonly used in the treatment of mild PMS where medicalization of the condition is not wanted.
If symptoms of stress are more significant, psychological counselling including cognitive behavioural therapy can be beneficial (Blake et al. 1998). Ovulation suppression
It follows that the logical hormonal treatment of severe PMS is to suppress ovulation. This can be done by transdermal oestrogens either patches or gel (Cronje et al. 2004). Occasionally hormonal implantation every 6 months can be used. Monthly injections of gonadotropin-releasing hormone (GnRH) analogues such as Gonapeptyl or Zoladex act as a medical oophorectomy and certainly eradicate all symptom clusters of PMS although ‘add-back’ HRT is required to prevent vasomotor symptoms and osteoporosis (Leather et al. 1999).
Oestradiol patches are the most frequently used hormonal therapy and doses of 100 μg or 200 μg, being more than the usual dose for the menopause, are recommended producing plasma oestradiol levels of about 600–800 pmol, which will usually stop ovulation and ablate the hormonal changes that follow ovulation.
These women have a uterus and it is necessary for them to have protection by progestogen usually by the oral route. However, as they have progestogen intolerance they often have a recurrence of their PMS symptoms with the orthodox 14-day course. Thus it is justifiable and indeed correct to shorten the duration to 7 days a month, which is adequate to prevent hyperplasia in 97% of women. If there are still unacceptable PMS symptoms then a Mirena IUS should be considered for many of these patients.
The combined oral contraceptive pill is not usually effective in spite of stopping ovulation. Although it ablates the cycle, the daily progestogen component produces PMS-like symptoms for most days of the month in these women ultra-sensitive to all gestagens. However, a new type of combined contraceptive pill contains an anti-mineral corticoid and anti-androgenic progestogen drospirenone. There are no progestogenic side-effects but has a mild diuretic and anti-androgenic effect. The hormone free interval should also be less then 7 days or even being used back to back (Pearlstein et al. 2005).
In spite of the efficacy of these therapies there are still women who may have cyclical symptoms or may have bleeding. The ultimate form of ovulation suppression and possibly the only true cure for PMS is a hysterectomy and bilateral salpingo-oophorectomy (Domoney and Studd 2003). Clearly this procedure is only rarely performed as an alternative can usually be found. A hysterectomy with ovarian conservation will continue to have cyclical symptoms in the absence of cyclical bleeding. Selective serotonin reuptake inhibitors
Placebo controlled studies have shown that selective serotonin reuptake inhibitors (SSRIs) are effective for severe PMS and improve both mood and physical symptoms (Wyatt et al. 2005). Fluoexetine, citalopram, sertraline, and paroxetine can all be implemented and are all effective. Randomized studies have also shown that half-cycle treatment is as efficacious as continuous administration (Freeman et al. 1999). Unlike treating women for depression, symptoms improve within 24–48 hours of initiating therapy and there are no reports of discontinuation symptoms. The dose of fluoexetine or citalopram is 20 mg od for the continuous or cyclical treatment. Further reading
Blake F, Salkovskis P, Gath D, et al. Cognitive therapy for premenstrual syndrome: A controlled trial. J Psychosomatic Res 1998; 45: 307.
BorensteinJ, Dean B, Endicott J, et al. Heath and economic impact of the premenstrual syndrome. J Reprod Med 2003;48:515–24.
Cronje W, Studd J. Premenstrual syndrome and premenstrual dysphoric disorder. Prim Care 2002;29:1–12.
Cronje WH, Vashist A, Studd JWW. Hysterectomy and bilateral oophorectomy for severe premenstrual syndrome. Hum Reprod 2004;19:2152–5.
Domoney Vashist A, Studd JWW. Premenstrual syndrome and the use of alternative therapies. Ann N Acad Sci 2003;997:330–40.
Freeman E, Rickels K, Arredondo F, et al. Full-half-cycle treatment of severe premenstrual syndrome with serotonergic antidepressant. J Clin Psychopharmacol 1999;19:3–18.
Freeman E. The clinical presentation and course of premenstrual symptoms. In: O’Brien PMS, Rapkin AJ, Schmidt PJ (eds) The premenstrual syndromes: PMS and PMDD. Bocca Raton: Taylor&Francis 2007: 55–61.
Johnson SR. Premenstrual syndrome, premenstrual dysphoric disorder, and beyond: A clinical primer for practitioners. Obstet Gynecol 2004; 104: 845.
Keye W. Premenstrual syndrome. In: Proceedings of a conference on PMS and related behavioural disorders. Provo: BYU Division of conferences 1983: 1–10.
Leather AT, Studd JWW, Watson NR, Holland NF. The treatment of severe premenstrual syndrome with goserelin with and without ‘add-back’ estrogen therapy: a placebo-controlled study. Gynecol Endocrinol 1999;13:48–55.
Pearlstein T, Bachmann G, Zacur H, Yonkers K. Treatment of premenstrual dysphoric disorder with a new drospirenone-containing oral contraceptive formulation. Contraception 2005;72:414–21.
Robinson RL, Swindle RW. Premenstrual symptom severity: impact on social functioning and treatment-seeking behaviours. J Womens Health Gend Based Med 2000;9:757–68.
Royal College of Obstetricians and Gynaecologists. Management of premenstrual syndrome. Green-top guideline No 48, RCOG: London 2007.
Studd J, Panay N. Hormones and depression in women. Climacteric 2004;7:338–46.
Watson NR, Studd JWW, Savaas M, et al. Treatment with severe premenstrual syndrome with oestradiol patches and cyclical oral norethisterone. Lancet ii: 1989; 730–4.
Wyatt KM, Dimmock PW, O’Brien PM. Selective serotonin reuptake inhibitors for premenstrual syndrome. Cochrane Database Syst Rev 2005; 3. Internet resources
National Association for Premenstrual Syndrome (NAPS): www.pms.org.uk.
Womens Health Concerns: www.womens-health-concern.org.
Royal College of Obstetricians and Gynaecologists: www.rcog.co.uk.
FPA: www.fpa.org.uk
Society for endocrinology: www.endocrinology.org.
Patient UK; www.patient.co.uk.
Psychosexual problems
Psychosexual problems are common in both men and women, their prevalence depending on the definition of a dysfunction. This is a contentious issue currently but the most important factor is whether the individual is distressed by their symptoms (Table 12.35.1). The rate of female sexual dysfunction (FSD) may be up to 43% and in men up to 31% in a North American population. The International Consensus conference panel modified the framework of the International Classification of Diseases-10 and DSM-IV (Diagnostic and Statistical Manual of Mental Disorders of the American Psychiatric Association) to categorize clinical sexual disorders and thereby improve diagnosis and treatment. The improvements in physical treatment of male sexual disorders (erectile and ejaculatory disorders in particular) have led to a search for the equivalent treatments of FSD. Yet female sexual function is less easily quantifiable, as satisfaction is qualitative rather than the more quantitative measurements of male sexual function. The use of questionnaires may be helpful in a research setting but have a more limited role in clinical practice. A list of questionnaires for specific patient groups is available in the Further reading section. Asking patients about sexual activity is an important part of a gynaecological consultation. Opening questions within a consultation may be as follows and adapted to individual needs. Assumptions regarding sexual activity and orientation are likely to cause major difficulties within the doctor–patient relationship; therefore, great care should be taken to avoid them.
• Do you have a partner? Are you in a sexual relationship?
• Do you have any difficulties? Do you have pain during intercourse?
• Are these difficulties a problem for you? Female sexual function models
It is important to have an understanding of current thinking with respect to normal functioning and when the female sexual cycle is affected to understand the categorization of FSD and its treatment. The model of Masters and Johnson has been developed over the decades into a less linear model that incorporates the multifactorial influences on female sexual activity and its modifiers. Relationship issues and the need for intimacy as expressed by physicality may be more important for women within relationships than men.
Table 12.35.1 Common presentation of sexual problems in gynaecological consultations

Classification of female sexual function disorders
Desire disorders
Hypoactive desire disorder (HSDD): persistent or recurrent deficiency or absence of sexual desire/sexual fantasies/thoughts, and/or the desire for or receptivity to sexual activity that causes distress. The focus on sexual thoughts allows flexibility of definition to include those who are not in a relationship or have lost their relationships secondary to their HSDD.
Sexual aversion disorder is the persistence of phobic aversion to and avoidance of sexual activity that causes personal distress.
Sexual arousal disorder
Low sexual arousal disorder is defined as the persistent or recurrent inability to attain or maintain sexual excitement causing personal distress, which may be described as subjective feelings and/or lack of physical changes.
Persistent arousal disorder is rare but distressing and may be physical and/or psychological.
Orgasmic disorder
The persistence or recurrent difficulty or absence of achieving orgasm following sufficient stimulation and arousal. It may follow from both desire or arousal disorders or be truly independent.
Sexual pain disorders
These include dyspareunia, defined as persistent or recurrent genital pain associated with sexual intercourse. This may be physical and/or psychological, i.e. psychosomatic in origin. These origins must be explored before undertaking invasive investigations.
Vaginismus has been described by the International Consensus group as recurrent or persistent involuntary spasm of the pelvic musculature that interferes with intercourse. However, it may be situational, i.e. with only certain partners or just at speculum examination. This should be more often interpreted as a sign not a symptom of pelvic symptoms and therefore not considered a diagnosis alone.
Non-coital sexual pain disorders
Genital pain disorders induced by non-sexual stimulation, most commonly vulval pain disorders.
The prevalence of these disorders is varied depending on the population and age group. They can vary from 16–75% with desire disorder, 12–64% arousal, 16–48% orgasm, 7–68% with sexual pain, with considerable overlap. At various stages of life, sexual function and activity may change and with this an increase in sexual difficulties. An awareness of these changes may facilitate a discussion with health professionals before the behavioural changes are well established and more difficult to change. Sexual history
It is rarely necessary to ask a comprehensive sexual history in most gynaecological settings but it is useful to be aware of the other features that may or may not be relevant to the individual patient.
• What sexual problems (primary and secondary)?
• Why is she presenting now?
• Onset? lifelong/acquired, situational/generalized, gradual/rapid onset
• Potential aetiologies: organic/psychogenic/mixed?
• Comorbidities and concurrent disease (surgery/pain/cancer/incontinence)
• Hormonal factors
• Pelvic floor dysfunction
• Psychological health
• Relationship factors. Investigations
For most women, investigations are unnecessary as the history and examination are likely to be most revealing. However, there may be features of the consultation that invite consideration of some further tests, whether specific to gynaecological or general wellbeing. A hormone profile may or not may not reveal raised pituitary hormones in a perimenopausal woman. Thyroid function tests may provide a cause for generalized lack of vitality. If a primary diagnosis presents with a secondary sexual difficulty, this needs to be explored by the appropriate physician in addition to help with the sexual problem (for instance diabetes or galactorrhoea and lack of libido with hyperprolactinaemia). Indications of generalized conditions reflected in genital complaints such as lichen planus or psoriasis may be missed if the search for both organic and psychological causes is cursory. One of the most common conditions causing sexual problems in postmenopausal women is atrophic vaginitis, even in those women using systemic hormone replacement therapy (HRT). It is simple to treat with topical oestrogens (now with an indefinite license in the UK) or non-hormonal remoisturizers.
Hormone tests may be useful in some women if there is a potential role for hormone replacement, e.g. if an individual is considering HRT or monitoring treatment to which there is no response (Table 12.35.2). It is important to remember that other medications may also modify mood and therefore libido. Synthetic progestogens can have a profound effect in susceptible individuals, whether in hormonal contraception, HRT or for management of other gynaecological conditions.
The most useful androgen measurement is the free androgen index, as this gives an indication of free, biologically active androgen. Only 1–2% of testosterone is free in the circulation: 66% is bound to sex hormone binding globulin (SHBG), 31% to albumin (which is also bioavailable. SHBG levels varies enormously in women and may contribute to poor sexual drive and arousal. In women who are using the combined contraceptive pill or oral HRT, the rise in SHBG (and therefore lowering of free testosterone) may account for a change in reported sexual activity when all other factors are stable. However, overall, population studies have not documented correlation of hormone levels with sexual function.
The free androgen index is calculated from total testosterone and SHBG (normal range 0.4–0.8 ng/L):
FAI = TT (in nmol/L)/SHBG (in nmol/L) ? 100 (ng/L) Differing patient groups may be approached with varying techniques (Table 12.35.3). Correcting any physical problem can help but not necessarily cure FSD, as ingrained behaviours need to be addressed (e.g. avoidance/poor arousal/vaginismus). Vulval pain disorders can respond to topical treatments and systemic management of pain in addition to psychotherapeutic input. Women postpartum may need correction of atrophic vaginitis, perineal anaesthetic, and steroid injection in conjunction with debriefing and analysis of their sexual feelings (or lack thereof).
Table 12.35.2 Sex hormone levels in different age groups

Psychosexual medicine
Sexual function is a ‘mind–body’ activity and therefore any sexual difficulty can have a psychological effect irrespective of its aetiology. The main tenets of psychosexual medicine use the consultation skills (see below) within the doctor–patient relationship to explore the dynamics of the sexual feelings and relationships of the patient (Table 12.35.4). The genital examination can be used as a ‘moment of truth’ when the underlying vulnerabilities and patterns of thinking about sexual parts are explored. Gynaecologists have privileged access to intimate examinations that can be used as more than elicitation of physical signs only. Understanding the psychological examination of the pelvis can help diagnose and provide resolution to many psychosomatic gynaecological complaints in addition to understanding the psychological impact of a physical illness.
• Listen
• Observe
• Feel
• Think
• Interpret
Table 12.35.3 Physical conditions and treatments that may impact on male and female sexuality
Table 12.35.4 Psychosexual, pharmacological and physical management strategies for sexual dysfunction

The patient is central to the process: she is the ‘expert’. The doctor should aim to establish the causative and maintaining factors, understanding then facilitating change and hopefully improvement. The empathic consultation may enable the exposure of subconscious feelings and fantasies, as a reflection of the physical symptoms and sexual problems. The defences and fantasies of the patient (and doctor) should be explored rather than dismissed, as their origins are important to understand. This will be part of the therapeutic pathway. Although some sex therapists follow certain theoretical disciplines, for the gynaecologist offering pragmatic care or providing treatment acceptable to the patient, a practical approach to management and referral using a combination of approaches is likely to be helpful. Understanding what other services are available locally is important to every gynaecology unit. The Internet resources section provides websites that may be able to provide this information. Partners
Women may or may not present with their partners in gynaecological settings. Most often at the first visit, the woman will present alone. This allows her to be more open in her discussion of the sexual difficulties within her current relationship and her previous perception of her sexuality than may occur if she presents with her partner. Women are frequently protective of their partner’s sexual difficulties, with development of their own secondary problems if their male partners develop erectile or ejaculatory disorders, particularly in the older age group. Yet the effectiveness of phosphodiesterase inhibitors in improving male sexual dysfunction has increased the expectations of some who may have abandoned all hope previously.
The most common male sexual problem is erectile dys-function (ED) but desire and ejaculatory problems are frequently reported. It is important that the patient’s description of impotence is clarified as it can be a general term and non-specific to laymen. ED increases with age and a careful medical and sexual history may elicit a predominantly organic problem. Although difficult to elicit, a situational ED is different from a partner who has lost his early-morning erections: the latter much more likely to indicate organic disease. New-onset erectile difficulty may pre-date the onset of cardiovascular disease. Therefore, the evaluation of men with sexual dysfunction requires blood pressure, pulse, weight, genital, and prostate examination with serum glucose, lipids, and early-morning testosterone. Although ED and, to a certain extent premature ejaculation, are compatible with pharmacological treatment, it is important to assess the psychosexual aspects of these difficulties for the couple. Treatment options for men with sexual problems are outlined below (Table 12.35.5). Life events
Adolescence
Adolescence is a time of massive hormonal upheaval, peer group pressure, and evolving self-realization. Prior education with respect to genital function, menstrual cycles, sexual behaviour, contraception, and functional relationships are significant throughout this period as well as exposure to family attitudes. Events during this time can have a profound effect on future sexual fulfilment.
Reproductive years
Sexual function is inextricably linked with reproductive function despite the ability to control fertility and infection in the modern age.
Table 12.35.5 Treatment options for men with sexual problems

Sexually transmitted infections
Education to prevent sexually transmitted disease and treatment seeks to prevent long-term psychological consequences as well as physical. The circumstances under which an infection is introduced, its consequences and the approach to treatment has a bearing on future sexual behaviour. Management of sexually transmitted infections (STIs) should minimize adverse future behaviour: reduction of high-risk-taking sexual behaviour and normalizing sexuality in general. Advertising strategies for sex education reflect the standards and expectations of the younger age groups but may not target all communities as required.
Infertility
Counsellors, ideally with psychosexual training, are available in fertility clinics as the impact of fertility treatment is profound. It is not uncommon to encounter couples who are not having penetrative intercourse. The demands of performing to specific menstrual cycle dates and maintaining celibacy at other times takes its toll on most couples. Sex becomes goal orientated and the spontaneity may disappear. The financial, physical and psychological impact of fertility alters the relationship between the couple.
Termination of pregnancy
At the other end of the spectrum, control of fertility by termination of pregnancy is repeatedly cited by women recounting their sexual biography. This may be years after the event, often when another precipitating life event brings it to the fore.
Childbirth
Pregnancy and childbirth herald major changes for a couple, as both become different players in society with their first child. Their primary role as partner and lover changes to include mother/parent. For some pregnancy increases orgasmic potential, theoretically via an increase in oxytocin receptors, but changes may be secondary to other psychological and behavioural effects such as bonding and protection. Childbirth itself will alter sexual health. However, it is controversial whether interventions such as Caesarean section and episiotomy alter this. Overall sexual problems are common postpartum: 7–13% of women expressed a need for help, but 25% had not sought it. Advice regarding sexual function should be incorporated into routine postnatal care. Operative intervention should be very cautious in those with dyspareunia, particularly if they plan to have more children and are oestrogen deficient (still breast-feeding and no menstrual cycle). Topical oestrogen cream can safely be used in breastfeeding women.
Colposcopy
Many procedures are experienced very differently by patients when compared with healthcare professionals’ perceptions. These include smear taking, speculum examination, and colposcopy. These intimate examinations may allow the patient to reveal their difficulties but clinicians can miss the opportunity to discuss them in their haste to ‘console’ the patient. Care must be taken to make these procedures as minimally traumatic as possible as the potential to impact on sexual functioning is marked. The potential of a diagnosis of human papillomavirus (HPV) to cause distress due to its STI nature must be recognized. Careful explanation of all aspects of colposcopy care and screening are paramount to circumvent future adverse effects.
Menopause and ageing
A number of studies have explored sexual activity and dys-function in perimenopausal and ageing women. Overall there is a reduction in activity with age but this correlates with partner status and there is some evidence that cessation of activity is more likely to be linked to the male partner. The prevalence of desire disorders stays relatively constant through life as the younger woman is more distressed by this than the older woman. Some studies seem to indicate that sexual responsivity is related to ageing, but libido, frequency of intercourse, and dyspareunia are associated with oestrogen deficiency. Simple measures can improve the physical sequelae of hormone deficiency and tissue ageing such as topical oestrogen, non-hormonal vaginal remoisturizers and lubricants. In addition, consideration of surgery for those with medical problems such as symptomatic prolapse and stress incontinence should be complemented by a psychosexual approach.
Cancer
Aside from the physical effects of surgery, chemotherapy, and radiation the impact of a cancer diagnosis on the patient is enormous. In addition, the role of a partner as carer and provider of comfort is not always complementary to that of a sexual partner. Understanding individual feelings as experienced by the patient and their partner is key. Discussing possible problems at diagnosis and during treatment reinforces the normality of these anxieties. Training of oncology multidisciplinary teams to discuss physical interventions such as vaginal trainer use encourages continuity of care.
Sexual abuse
The possibility of sexual abuse or unwanted sexual experiences should be explored delicately. The lifetime risk of sexual assault for women worldwide is 1 in 4–6 and (in the UK 1 in 20) with a worldwide risk for men of 1 in 10. Only one in five adult rapes are reported to the police with a much lower number being pursued through the legal system. In children, it is estimated at most 1 in 20–50 are known to supervising authorities and therefore most present ‘historically’. What constitutes sexual trauma will be individual and dependant on circumstance and support systems, such as the reaction of a family aware of child sexual abuse, or within the context of physical abuse. In others, over exposure to nudity and sexuality in some may constitute abuse. The British Sexual Offences Act of 2003 has responded to the change in accessibility of children and vulnerable adults via the Internet and deems them prosecutable sexual offences. It now acknowledges any penile penetration of vagina, anus, or mouth as rape, rather than sexual assault. Conclusion
Recognition of sexual problems by the gynaecologist is mandatory. All professionals involved in women’s health should have basic training and some understanding of these issues. Routine questioning regarding sexual health will determine those who need referral, but many who attend gynaecology clinics can be treated by an empathic doctor who understands the presentation of these symptoms. First-line interventions can be initiated if appropriate, including hormone therapy. Psychosexual medicine, as a branch of psychosomatic medicine pertaining to sexual problems, should be a major part of the work of gynaecologists and obstetricians, and training should focus on this area. Further reading
American Psychiatric Association (APA). Diagnostic and statistical manual of mental disorders, 4th edn. Washington DC: American Psychiatric Association 2000.
Basson R, Berman J, Burnett A, et al. Report of the international consensus development conference on female sexual dysfunction: definitions and classifications. Urology 2000;163:888–93.
Basson R. Women’s sexual dysfunction: revised and expanded definition. CMAJ 2005;172:1327–33.
Cockburn J, Pawson M (eds). Psychological challenges in obstetrics and gynaecology. London: Springer-Verlag 2007.
Glazener CM. Sexual function after childbirth: women’s experiences, persistent morbidity and lack of professional recognition. Br J Obstet Gynaecol 1997;104:330–5.
Hayes RD, Bennett CM, Fairley CK, Dennerstein L. What can prevalence studies tell us about female sexual difficulty and dysfunction? J Sex Med 2006: 3; 589–95.
Laumann E, Paik A, Rosen R. Sexual dysfunction in the United States: prevalence and predictors JAMA 1999;281:537–44.
Masters WH, Johnson VE. Human sexual response. Boston: Little Brown 1966.
Montford H, Skrine R (eds). Psychosexual medicine: an introduction. London: Hodder Arnold 2001.
Rees M, Mander T (eds). Sexual health and the menopause. London: Royal Society of Medicine Press 2005.
Trigwell P. Helping people with sexual problems: a practical approach for clinicians. Mosby Elsevier 2005. Internet resources
www.ipm.org.uk Institute of Psychosexual Medicine
www.basrt.org.uk British Association of Sexual and Relationship Therapy
www.fsrh.org.uk Faculty of Sexual and Reproductive Health
www.sda.uk.net Sexual Dysfunction Association Questionnaires
Female sexual function index (FSFI): general population (19 items)
Profile Female Sexual Function: HSDD diagnosis in postmenopausal women (37 items)
Brief Profile Female Sexual Function: screening for HSDD (7 items)
Golombok Rust Inventory Sexual Satisfaction (GRISS): sexual relationships (28 items)
Changes in Sexual Functioning Questionnaire (CSFQ): intervention related change (14/35 items)
Prolapse and Incontinence Sexual Function questionnaire (PISQ): women with pelvic floor disorders (9/12/31 items)
Macoy Sexual Function Questionnaire (MSFQ): women with hormonal factors (19 items)
Recurrent miscarriage Definition
Recurrent miscarriage (RM) has traditionally been defined as the loss of three or more consecutive pregnancies under 24 completed weeks’ gestation. However, a recent analysis of a Scottish population-based database has suggested that after adjusting for age and smoking, the risk of a further miscarriage increased sequentially in women who had one and two miscarriages and that three miscarriages did not increase the odds any further. In the face of declining birth rates, an increasing number of clinicians now define RM as two or more consecutive pregnancy losses.
Primary RM refers to consecutive pregnancy losses with no prior successful pregnancy.
Secondary RM refers to consecutive pregnancy losses following a live birth. Epidemiology
The statistical prediction for three consecutive miscarriages is 0.34%. However, the condition is seen to affect 1% of women. If defined as two consecutive miscarriages, the incidence is 5%. Pathology
RM is a heterogeneous condition that has many possible causes. The pathology is therefore varied. Aetiology
• Unexplained: the cause remains unknown in 50% of the cases.
• Maternal age and previous reproductive outcome: these are two independent risk factors for a further miscarriage. The risk of fetal loss increases steeply after the age of 35 years, rising to 75% at 45 years. Similarly, the risk of a further miscarriage increases after each consecutive miscarriage, reaching 45% after three consecutive miscarriages (RCOG 2003).
• Chromosomal and single gene disorders: 4–5% of couples with RM show changes in the karyotypes compared with 0.2% in the general population. These include balanced reciprocal translocations, Robertsonian translocations, gonosomal check with Rohan mosaic, and inversions.
Anatomical factors
• Congenital uterine malformations: 1.8%–37.6% of patients with RM have congenital uterine malformations such as septate, bicornuate, and didelphic uteri. However, the ‘true impact’ of these malformations on RM is questionable.
• Uterine fibroids: in addition to a mechanical effect of uterine fibroids that impedes embryonic implantation, uteri with fibroids have now been shown to have a lower expression of HOX10, a gene involved in implantation. The effect of uterine fibroids on reproductive outcome however, remains controversial.
• Acquired anatomical problems: Asherman’s syndrome and cervical abnormalities resulting from trauma or surgical treatment are associated with RM.
Immunological factors
• Antiphospholipid antibody syndrome (APS): this has been reported in 15% of RM patients and in untreated pregnancies, a miscarriage rate of 90% has been reported.
• Alloimmune factors: it has been suggested that defects in the immunosuppressive factors, cytokines, and growth factors at the local maternofetal interface may be implicated in the pathogenesis of implantation failure and RM, but there is still no clear evidence to support the hypothesis that HLA incompatibility between couples, the absence of maternal leucocytotoxic antibodies or the absence of maternal blocking antibodies are related to RM.
• Natural killer (NK) cells: women with RM have higher levels of NK cells in the uterine mucosa than controls and those with the highest levels have a correspondingly high rate of miscarriage in subsequent pregnancies without treatment.
• Other immunological conditions: there might be a correlation between coeliac disease and RM but not between the presence of circulating thyroid antibodies and pregnancy outcome in euthyroid women.
• Inherited thrombophilic defects: hereditary thrombophilias due to mutations in factor V and prothrombin gene as well as deficiencies of protein C, protein S, and antithrombin are established causes of systemic thrombosis and are more prevalent in patients with disturbed pregnancy (RM, pre-eclampsia, and late fetal loss) than in patients with normal pregnancy.
Infectious causes
• Bacterial vaginosis (BV): although the association of BV with first trimester miscarriage is inconsistent, the presence of BV in the first trimester is associated with an increased risk of second trimester miscarriage and pre-term delivery.
• TORCH infections: although a recognized cause of sporadic miscarriages, the role of these agents in RM is unclear and screening is not advocated.
• Endocrinological factors: RM is associated with thyroid dysfunction, polycystic ovarian syndrome (PCOS), diabetes mellitus especially type I and hyperprolactinaemia.
• Enzyme deficiencies: Some cases of RM are associated with deficiencies in either glucose-6-phosphate dehydrogenase or nitric oxide synthase which are enzymes involved in the metabolism of reactive oxygen species.
• Psychological factors: RM is associated with early pregnancy-related fear and baseline depressive symptoms
Recently identified risk factors
• Circulating microparticles: fibrin deposits have been found in the placental intervillous space of women with RM, suggesting a ‘permanent, acquired procoagulatory state’. In some of these patients, there is an increased concentration of microparticles from circulating blood cells. They are believed to induce coagulation that becomes clinically manifest during pregnancy.
• Glycoproteins: the glycoprotein glycodelin, secreted in high amounts by the trophoblast seems to be downregulated in RM patients. Reduced glycodelin expression in miscarriage could lead to increased activation of the maternal immune system, thus causing rejection of the developing fetus.
• Nuclear hormone receptors and leptin: the nuclear hormonal receptor peroxisome proliferator-activated receptor (PPAR) γ seems to play a major role in facilitating the invasion of the placental trophoblast. Leptin is connected to PPAR γ by a negative feedback loop and decreased leptin levels seem to be associated with miscarriage. Clinical approach
Investigations
Investigations for genetic factors
• Peripheral blood karyotyping of both parents has been recommended for all couples with a history of RM as the incidence of an abnormal karyotype can be as high as 3–5% in this group.
• Cytogenetic analysis of the products of conception, although an expensive tool, provides useful information for counselling and future management. If the karyotype of the miscarried pregnancy is abnormal, there is a better prognosis in the next pregnancy.
Investigations for uterine anatomical defects
• Routine two-dimensional pelvic ultrasound with or without sonohysterography is at least as sensitive in detecting uterine anomalies than the more invasive and uncomfortable procedure of hysterosalpingography and is currently recommended in all patients with RM.
• Three-dimensional ultrasound offers both diagnosis and classification of uterine malformation and its use may obviate the need for diagnostic hysteroscopy and laparoscopy in the future.
• There is currently no satisfactory objective test that can identify women with cervical weakness in the non-pregnant state.
Investigations for immunological factors
• Antiphospholipid antibody syndrome: diagnosis requires fulfilment of the criteria outlined in the updated international consensus statement. This includes the presence of at least one clinical and one laboratory-based criterion detected on two separate occasions at least 12 weeks apart.
• Alloimmune factors: testing for alloimmune factors is currently not recommended outside a research setting.
• NK cells in peripheral blood: there is poor correlation between levels of NK cells in uterine mucosa and peripheral blood and levels in peripheral blood are not representative of an individual’s risk of RM. Testing is therefore not warranted.
• Testing for thyroid antibodies in women with RM is not recommended.
Investigations for inherited thrombophilias
In the absence of a randomized trial, the poor pregnancy outcome associated with inherited thrombophilias, coupled with the maternal risks during pregnancy, may justify routine screening for these conditions and offering thromboprophylaxis to those affected.
Investigations for infective causes
• Screening for bacterial vaginosis: screening low-risk women for bacterial vaginosis during the first trimester of pregnancy and treating them with oral clindamycin may reduce the risk of late miscarriage and preterm birth.
• Screening for TORCH infections is currently not recommended.
Investigations for endocrinological factors
• Hyperprolactinaemia: treatment with bromocriptine significantly reduces the rate of miscarriage.
• Other endocrinological factors: routine screening for occult diabetes and thyroid disease with oral glucose tolerance and thyroid function tests in asymptomatic women presenting with RM is uninformative. Ovarian morphology in PCOS is not predictive of pregnancy outcome. These tests are therefore not recommended. Management
Counselling and adjuvant therapy
• Genetic counselling: the finding of an abnormal parental karyotype should prompt referral to a clinical geneticist. Genetic counselling offers the couple prognosis for future pregnancy, familial chromosomal studies and appropriate prenatal diagnosis in future pregnancies.
• General counselling: RM patients may profit not only from general supportive counselling but also from interventions like psychotherapy.
Medical management
• Progesterone: progesterone induces secretory changes in the endometrium that are essential for implantation of the embryo. Its use in the first trimester might be of benefit to women with RM.
• Metformin: the use of insulin-sensitizing agents such as metformin is associated with a reduction in miscarriage rate in women with PCOS.
• Antithrombotic treatment
• For antiphospholipid syndrome (APS): aspirin combined with low molecular weight heparin (LMWH) significantly increases live birth rate in RM patients with APS.
• For inherited thrombophilias: although several trials emphasize the benefit of LMWH in treatment of patients with known hereditary thrombophilia, the heparin/aspirin (HepASA) trial in Canada showed that 80% of RM patients had a successful pregnancy regardless of treatment given (heparin + aspirin versus aspirin alone) raising questions on the efficacy of LMWH treatment in this cohort of patients. However, as there is some evidence for benefit, and since the potential for harm is so small, LMWH is still considered acceptable for use in cases of inherited thrombophilia.
• For unexplained RM: neither aspirin alone nor aspirin combined with LMWH is shown to be of any benefit in women with unexplained RM. The Scottish Pregnancy Intervention Trial has shown no reduction in pregnancy loss rate with antithrombotic agents in women with ≥2 consecutive previous pregnancy losses.
• Immunotherapy: this is of two types
• active immunotherapy: an injection of paternal leucocytes is used to boost the subsequent maternal immune recognition of the developing conceptus. Whereas meta-analysis showed no significant benefit on pregnancy outcome in RM patients when compared with placebo, paternal immunization has recently been shown to be associated with significantly lower levels of tumour necrosis factor (TNF)-α and interferon (IFN)-γ; higher levels of CD4+ CD25+ (bright) T cells and significantly higher successful pregnancy rates in cases of unexplained RM
• passive immunotherapy: an intravenous infusion of immunoglobulins is used in the hope of neutralizing circulating maternal autoantiboidies, inhibiting complement-mediated cytotoxicity and modulating cytokine release. It may be beneficial in a subpopulation of RM patients >37 years with ≥4 miscarriages or secondary RM and in patients with high numbers of CD56 + CD3 + NK cells; this expensive treatment is not without side-effects and should only be used under controlled study conditions.
• Newer treatments
• TNF-α inhibitors and granulocyte colony-stimulating factor (G-CSF) are promising new drugs and their use in recent studies has shown increased live birth rates when compared with placebos. They still are not recommended outside a research setting.
• PPAR and leptin are potential targets for new treatment strategies concerning miscarriage.
• RM patients with coeliac disease might benefit from a gluten-free diet.
Surgical management
• Surgery for anatomical factors
• Congenital uterine anomalies: there is a suggestion that RM patients with septate uteri may profit from hysteroscopic metroplasty, but no randomized trial has assessed the benefits of this procedure on pregnancy outcome. Open uterine surgery is not recommended as it is associated with postoperative infertility and carries a significant risk of uterine scar rupture during pregnancy.
• Fibroids: surgical treatment of uterine fibroids is controversial and depends on their size and location.
• Cervical cerclage: a Cochrane review identified no conclusive evidence that prophylactic cervical cerclage reduces the risk of recurrent midtrimester miscarriage and the insertion of a rescue cerclage for cervical shortening identified on serial ultrasound scans is questionable. Abdominal cerclage has been advocated for selected women with known cervical incompetence and failed vaginal cerclage. Although this might reduce perinatal death, it is associated with a higher risk of serious operative morbidity.
• Preimplantation genetic diagnosis and in vitro fertilization: this is a treatment option being explored for translocation carriers, but is a technically demanding procedure and the experience is still limited. Complications/side-effects/sequelae
Recurrent miscarriage is being increasingly recognized as part of a spectrum of disorders resulting from faulty placentation and is found to be associated with late pregnancy complications, including intrauterine growth restriction, preterm labour, and pre-eclampsia. Prognosis/follow-up/recurrence/future pregnancy planning
Despite a thorough evaluation, a significant proportion of cases of RM remain unexplained. The prognosis for successful future pregnancy in these cases, with supportive care alone is in the region of 75%. Attendance at a dedicated early pregnancy clinic has been shown to have a beneficial effect, although the mechanism remains unclear. Further reading
Greer IA. Antithrombotic therapy for recurrent miscarriage? N Engl J Med 2010;362:1630–1
Rai R, Regan L. Recurrent miscarriage. Lancet 2006;368:601–611
RCOG The investigation and treatment of couples with recurrent miscarriage. Greentop guideline no. 17. London: RCOG 2003. www.rcog.org.uk
Toth B, Jeschke U, Rogenhofer N, et al. Recurrent miscarriage: current concepts in diagnosis and treatment. J Reproduct Immunol 2010;85:25–32 Patient resources
Couples with recurrent miscarriage: what the RCOG guideline means for you? www.rcog.org.uk/womens-health/clinical-guidance/couples-recurrent-miscarriage-what-rcog-guideline-means-you
The Miscarriage Association, Clayton Hospital, Northgate, Wakefield WF1 3JS: www.miscarriageassociation.org.uk
Women’s Health, 52 Featherstone Street, London EC1Y 8RT: www.womenshealthlondon.org.uk
Termination of pregnancy Introduction
Termination of pregnancy (TOP) is one of the most commonly performed gynaecological procedures in Great Britain. At least one-third of British women will have had an abortion by the time they reach the age of 45 years, with approximately 192 000 pregnancy terminations being performed each year. The UK also has the highest TOP rates among 15–19-year-old girls in Western Europe.
In 2008, for women resident in England and Wales
• the total number of abortions was 195 296, compared with 198 499 in 2007, a fall of 1.6%
• the age-standardized abortion rate was 18.2 per 1000 resident women aged 15–44, compared with 18.6 in 2007
• the abortion rate was highest at 36 per 1000, for women age 19, the same as in 2007
• the under-16 abortion rate was 4.2 and the under-18 rate was 18.9 per 1000 women, both lower than in 2007
• 90% of abortions were carried out at under 13 weeks’ gestation; 73% were at under 10 weeks
• medical abortions accounted for 38% of the total
• 91% of abortions were funded by the NHS; of these, just over half (58%) took place in the independent sector under NHS contract.
Induced abortion is a healthcare need. In 1999, the International Federation of Gynaecology and Obstetrics (FIGO) recommended that ‘after appropriate counselling, a woman has the right to have access to medical or surgical induced abortion, and that healthcare services have an obligation to provide such services as safely as possible’.
In 2004, the Royal College of Obstetricians and Gynaecologists (RCOG) published National evidence based guidelines on ‘The Care of Women Requesting Abortion’, which sets quality standards for abortion services
The aim of a termination of pregnancy service is to provide high-quality, efficient, effective, legal and comprehensive care, which respects the dignity, individuality and rights of women to exercise personal choice over their treatment. Ideally, an abortion service should be an integral component of a broader service for reproductive and sexual health, encompassing contraception and management of sexually transmitted infections.
Termination of pregnancy services should be able to offer impartial support and advice to all women with unintended pregnancy who an abortion requests regardless of age, ethnicity, language, religious or personal circumstances. Statutory grounds for TOP
TOP or abortion is legal in Great Britain if two doctors decide in good faith that a particular pregnancy is associated with factors that satisfy one or more of five grounds specified in the Regulations of the Abortion Act and Section 37 of the Human Fertilisation and Embryology Act 1990.
A. The continuance of the pregnancy would involve risk to the life of the pregnant woman greater than if pregnancy were terminated.
B. The termination is necessary to prevent grave permanent injury to the physical or mental health of the pregnant woman.
C. The pregnancy has not exceeded its 24th week and the continuance of pregnancy would involve risk, greater than if pregnancy were terminated, of injury to physical or mental health of the pregnant woman
D. The pregnancy has not exceeded its 24th week and continuance of pregnancy would involve risk, greater than if the pregnancy were terminated, of injury to physical or mental health of the existing child(ren) of the family of pregnant women.
E. There is substantial risk if the child were born it would suffer from such physical or mental abnormality as to be seriously handicapped.
The Regulations also permit abortion to be performed in an emergency on the basis of signature of the doctor performing the procedure, which may be provided up to 24 hours after the termination. The grounds are
F. To save the life of the pregnant woman.
G. To prevent grave permanent injury to the physical or mental health of the pregnant woman at risk.
A pregnancy may only be terminated if two registered medical practitioners are of the opinion, formed in good faith, that TOP is justified within the terms of the Act. The Abortion Act has a conscientious objection clause which permits doctors to decline participating in pregnancy terminations. However, doctors are obliged to provide emergency treatment when a woman’s life is at risk. Most abortions are undertaken on grounds C or D. Access and referral to TOP services
Some 90% of abortions are performed in the NHS, with the majority being referred by GPs. Rapid access to abortion care is important to reduce the distress and complications associated with procedures undertaken at higher gestations. Services should therefore offer arrangements to minimize delay. Appointments for assessment prior to TOP can be made via a common telephone booking service that can be accessed by clients either directly, or via GPs, family planning clinics, young people’s clinic, Brook clinics, and genitourinary medicine clinics. Fast track referral guidelines should also be put in place for GPs and family planning services, and attempts should be made to treat women having abortions separately from other gynaecological patients.
The Government’s sexual health strategy states that no woman should wait longer than 3 weeks from the first appointment with the referring doctor to the procedure, a standard supported by professional guidelines. RCOG recommendations on referral procedure
• All women requesting TOP should ideally be offered an assessment appointment within 5 days of referral.
• As a minimum standard, all women requesting TOP should ideally be offered an assessment appointment within 2 weeks of referral.
• Ideally all women can undergo TOP within 7 days of the procedure being agreed upon.
• As a minimum standard, all women should undergo TOP within 2 weeks of the decision being agreed upon.
• Women with urgent medical reasons requiring TOP should be seen as soon as possible.
• As a minimum standard, no woman should wait for more than 3 weeks from her initial referral to the time of abortion. Management
A TOP service should provide counselling, contraceptive advice, gestational age assessment by ultrasound, a specialist nurse, and a clinician for clinical assessment and management. Counselling
Counselling enables the person concerned to understand the implications of the proposed course of action for themselves and for their family. Counselling also aims at giving emotional support at times of particular stress and helps people with consequences of their decision and to help them resolve problems that may arise as a result. Contraceptive advice following termination
• It is important to ask the patient about previous contraception and to offer contraceptive advice post termination. Before the patient is discharged following abortion, future contraception should have been discussed with each woman and contraceptive supplies should have been offered if required. The chosen method of contraception should be initiated immediately following abortion.
• Intrauterine contraception can be inserted immediately following first or second trimester abortion.
• Sterilization can be safely performed at the time of induced abortion. However, combined procedures are associated with high rates of failure and of regret on the part of the woman Investigations
• A detailed clinical history and thorough examination to determine patient fitness for the procedure.
• Screening for chlamydia.
• Screening for HIV, hepatitis B and C is indicated in the light of clinical features, individual risk factors or prevalence.
• Preprocedure blood testing: full blood count, ABO and Rhesus blood groups, screening for red cell antibodies.
• Women who have not had a cervical smear within the recommended interval in their programme can be offered one within the TOP service.
• Ultrasound scanning of all patients prior to TOP is not considered to be an essential prerequisite.
• All services, however, must have access to scanning, as it can be a part of pre-abortion assessment, particularly where gestation is in doubt or where extrauterine pregnancy is suspected. Consent
• Any competent young person, regardless of age, may independently seek medical advice and give valid consent to medical treatment.
• Following the Gillick case, Lord Fraser provided the Fraser Criteria for young girls under 16. Although parental involvement is ideal, girls under 16 may sign consent for TOP if they decline parental involvement and doctors feel they are ‘mature’ (Gillick competent) to comprehend their circumstances. Surgical procedure
• Appropriate at gestations of 7–15 weeks
• If performed at less than 7 weeks’ gestation, it is three times more likely to fail to remove products of conception than that performed at 7–12 weeks
• For first trimester suction termination either electric or manual aspiration devices may be used, as both are effective and acceptable to women and clinicians. In this process, a plastic aspiration cannula is used with a vacuum device to empty the uterus.
• Suction termination is performed as a day case procedure, usually under general anaesthesia.
• Suction termination is safer under local anaesthesia than under general anaesthesia. Consideration should be given to making this option available, particularly at low gestational ages.
• Cervical priming prior to surgical abortion reduces the risks of cervical injury by making the cervix softer and easier to dilate.
• Based on available evidence, misoprostol given in a regimen 400 μg (2 ? 200 μg tablets) administered vaginally, either by the woman or a clinician, 3 hours prior to surgery remains the most widely used prostaglandin for cervical priming although it is unlicensed.
• Gemeprost 1 mg vaginally, 3 hours prior to surgery or mifepristone 600 mg orally 36–48 hours prior to surgery is licensed for use.
• During suction termination, the uterus should be emptied using the suction curette and blunt forceps (if required) only. Sharp curette should not be used.
• An ultrasound-guided procedure should be performed if there is any difficulty encountered during the procedure.
• Suction termination can be done from 12 to 15 weeks’ gestation, varying according to the skills and experience of local clinicians
• For gestations above 15 weeks, surgical abortion by dilatation and evacuation (D&E), preceded by cervical preparation, is safe and effective
• The risk of cervical incompetence is increased as a result of the degree of dilatation necessary and there is a higher risk of major complications, e.g. uterine perforation and visceral damage
• Routine histopathological examination of tissue obtained at TOP is not necessary. Medical procedure
• There has been an increase in the last few years: 30% (2006), 35% (2007), 38% (2008)
• It is a safe and effective alternative to surgery.
• Ninety per cent of women state that they would choose medical treatment for subsequent termination
• There are few contraindications to medical termination; these include:
• ectopic pregnancy
• chronic adrenal failure
• long-term corticosteroid therapy
• haemorrhagic disorders and anticoagulant therapy
• cardiac disease
• porphyria. Early medical TOP
• Gestations up to 9 weeks.
• Medical abortion using Mifepristone plus prostaglandin is the most effective method of abortion at gestations of less than 7 weeks.
• Medical abortion using Mifepristone plus prostaglandin continues to be an appropriate method for women in the 7–9 week gestation band.
• Early medical TOP (up to 49 days), based on the evidence of published, but unlicensed regimes: day 1 Mifepristone 200 mg given orally, followed by 1–3 days later by misoprostol 800 μg vaginally.
• For women between 49 and 63 days, the above regimen is given, followed by a second dose of 400 μg of misoprostol if the first dose has not caused abortion. The route of the second dose of misoprostol depends on the amount of vaginal bleeding and preference.
• The following regime is licensed: mifepristone 600 mg orally followed 36–48 hours later by gemeprost 1 mg vaginally.
• If women are well informed, offered sufficient pain relief, and have a well functioning follow-up programme, this procedure can be done at home
• Early medical TOP service can be run by a nurse-led clinic without compromising on safety and effectiveness.
• The involvement of nurses in medical abortion should be encouraged, if future legislation permits, as recommended in the report from the House of Commons Science and Technology Committee. Late medical TOP
• Gestations from 13–24 weeks.
• Mifepristone followed by prostaglandin is an appropriate method and has been shown to be safe and effective at these gestations.
• Based on the available evidence, mifepristone 600 mg orally, followed 36–48 hours later by gemeprost 1 mg vaginally every 3 hours to a maximum of five pessaries.
• Also based on evidence, but unlicensed regime includes mifepristone 200 mg orally, followed 36–48 hours later by misoprostol 800 μg vaginally, then misoprostol 400 mg orally, 3-hourly, to a maximum of four oral doses. Other methods of TOP Extra-amniotic route medication
• For second trimester abortions.
• A self-retaining catheter is passed through the cervix into the extra-amniotic space and a continuous infusion of PGE2 is given until the cervix is sufficiently dilated to allow catheter balloon to be expelled, followed by oxytocin infusion. Intra-amniotic route medication
• Recommended after 20 weeks.
• Amniocentesis is performed,100–200 mL of liquor removed, and replaced with 80–120 g of 20% urea and up to 5 μg of PGE2. This usually causes fetal demise before expulsion. Continuous ultrasound scanning is essential for the procedure, to prevent intravascular injection, leading to coagulopathy, and cardiogenic collapse. Hysterotomy
• Nowadays, rarely performed for TOP.
• May be considered for midtrimester TOP for conjoint twins, where vaginal delivery may not be feasible Complications
Complication rates depend on stage of gestation, method of termination, skill and experience of the operator, and coexisting factors, e.g. uterine malformation. Haemorrhage
Haemorrhage complicates approximately 1.5 per 1000 procedures, under 13 weeks of gestation and 8.5 per 1000 over 20 weeks. Significant haemorrhage is more common in the second trimester, and if not treated promptly, can lead to significant blood loss. Oxytocics are effective in reducing intraoperative blood loss; however, its routine use is not recommended. Uterine perforation
Uterine perforation can occur in 1–4 per 1000 procedures. When suspected at the time of TOP, laparoscopy is indicated to confirm the diagnosis. If the bleeding from the perforation is significant, it needs to be sutured. Visceral perforation may also occur at the time of TOP, the appropriate team must be involved in repair. At times, a perforation can go undiagnosed at the time of TOP and present later with abdominal pain or shock. Continuous traction of the vulsellum during cervical dilatation may be helpful in straightening the angle between the cervix and uterine cavity and reduce the risk of perforation in a markedly anteverted or retroverted uterus. Retained products
Incidence is 1–2%. Sometimes, a repeat evacuation may be required. Ultrasound may reveal blood clots, which makes the diagnosis difficult. Failure to abort
The incidence in surgical TOP is around 2.3 per 1000 procedures, and for medical TOP around 6 per 1000. Cervical trauma
Incidence is 1%. Cervical priming with prostaglandin reduces the risk of cervical trauma. Dilatation above 10 mm may cause cervical incompetence. Infection
Infection, including pelvic inflammatory disease, occurs in up to 10% of cases, although this rate is lower if bacteriological screening is performed and prophylactic antibiotics are given. Long-term sequelae
Only a minority of women experience any long-term psychological sequelae. There are no proven associations with infertility, future pregnancy loss, breast cancer or adverse outcome in subsequent pregnancies such as low birth-weight, preterm labour. Prevention of infection
RCOG recommendations on antibiotic prophylaxis:
• metronidazole 1 g rectally at the time of abortion plus
• doxycycline 100 mg orally twice daily for 7 days, commencing on the day of abortion or
• metronidazole 1 g rectally at the time of abortion plus
• azithromycin 1 g orally on the day of abortion. Compliance is better with Azithromycin as it is a single dose regime. Anti-D prophylaxis
According to the RCOG recommendation May 2002, anti-D immunoglobulin G (250 IU before 20 weeks of gestation and 500 IU thereafter) should be given, by injection into the deltoid muscle, to all not sensitized Rh D-negative women within 72 hours following abortion, whether by surgical or medical methods. Sharing information and patient confidentiality
The GP, referring doctor/nurse, and doctor providing follow-up care should be informed in writing of the date of termination, method used, antibiotic treatment, other medical problems, any complications or referral to other services, and arrangements for contraception and follow-up. The woman’s consent to passing on of information to professional carers should first be obtained, although the importance of the GP being informed in case of emergency should be emphasized to the woman. In order to maintain confidentiality, no information should be sent to the woman’s home address unless the woman expressly wishes this. Further reading
Abortion Act 1967. London: HMSO 1967.
Allsop JR. Termination of pregnancy. Curr Obstet Gynaecol 2004;14:285–90.
Buehler JW, Schulz KF, Grimes DA, Hogue CJ. The risk of serious complications from induced abortion: do personal characteristics make a difference? Am J Obstet Gynecol 1985;153:14–20.
Department of Health. Abortion statistics, England & Wales: 2008. www.dh.gov.uk
Department of Health. The national strategy for sexual health and HIV. Implementation Action Plan. London: DH 2002.
Ferris LE, McMain-Klein M, Colodny N, et al. Factors associated with immediate abortion complication. Can Med Assoc J 1996;154:1677–85.
Lipp A. A review of developments in medical termination of pregnancy. J Clin Nursing 2008;17:1411–18.
Niinimäki M, Pouta A, Bloigu A, et al. Immediate complications after medical compared with surgical termination of pregnancy. Obstet Gynecol 2009;114:795–80.
Peyron R, Aubeny E, Targosz V, et al. Early termination of pregnancy with mifepristone (RU 486) and the orally active prostaglandin misoprostol. N Engl J Med 1993;328:1560–13.
Premila S, Arulkumaran S. Termination of pregnancy. Obstet Gynaecol Reproduct Med 2007;10:301–4.
Royal College of Obstetricians and Gynaecologists (RCOG). Rh prophylaxis, anti-D immunoglobulin. Green Top Guideline No.22. London: RCOG 2002.
Royal College of Obstetricians and Gynaecologists (RCOG). The care of women requesting induced abortion. National Guidance-Based Clinical Guideline No. 7. London: RCOG Press 2004.
Soulat C, Gelly M. Immediate complications of surgical abortion. J Gynecol Obstet Biol Reprod (Paris) 2006;35:157–62. Internet resources
www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAnd Guidance/DH_080925