I CHRONIC GYNECOLOGIC PAIN ^629
Many women experience vulvar or pelvic pain and discomfort that affect the quality of their lives. Vulvodynia, vaginismus, and chronic pelvic pain are common gynecologic pain disorders routinely encountered by obstetrician-gynecologists in their clinical practices.
Vulvodynia and Vaginismus
Vulvodynia is described by most patients as burning, stinging, irritation, or rawness of the vulva. It is a condition in which pain is present with a normal appearance of the vulva (other than erythema). Vaginismus is an involuntary spasm of the muscles surrounding the vagina; it sometimes coexists with vulvodynia, which compounds the problem. Symptoms of vulvovaginal disorders are common, often chronic, and can significantly interfere with women’s sexual function and sense of well-being (see also the “Vulvar Skin Disorders” section later in Part 4).
Classification and Etiology
The most recent terminology and classification of vulvar pain by the International Society for the Study of Vulvovaginal Disease defines vul- vodynia as “vulvar discomfort, most often described as burning pain, occurring in the absence of relevant visible findings or a specific, clinically identifiable, neurologic disorder.” Vulvodynia is not caused by infection (eg, candidiasis, human papillomavirus infection, or herpes), inflammation (caused by, for example, lichen planus or immunobullous disorder), neoplasia (eg, Paget disease or squamous cell carcinoma), or a neurologic disorder (eg, herpes neuralgia or spinal nerve compression). The classification of vulvodynia is based on the site of the pain, whether it is generalized or localized, and whether it is provoked, unprovoked, or mixed.
Several causes have been proposed for vulvodynia, including embryologic abnormalities, increased urinary oxalate levels, genetic or autoimmune
factors, hormonal factors, inflammation, infection, and neuropathic changes.
Most likely, there is no single cause. Because the etiology of vulvodynia is unknown, it is difficult to say whether localized vulvo- dynia (previously referred to as vestibulitis) and generalized vulvodynia are different manifestations of the same disease process. Distinguishing localized disease from generalized disease is fairly straightforward and is done by examination with a cotton swab, as described in “Evaluation and Diagnosis” in this section. Early classification to localized or generalized vulvodynia can facilitate more timely and appropriate treatment.In vaginismus, the involuntary muscle spasm of the muscles surrounding the vagina may function to tighten the vaginal opening, making vaginal intercourse more difficult. Causes include past sexual trauma or abuse, psychologic factors, or a history of discomfort with sexual intercourse. Sometimes no cause can be found. The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, defines genito-pelvic pain/penetration disorder as the persistent or recurrent presence of one or more of the following four symptoms for a minimum of 6 months, which causes significant distress in the individual: 1) difficulty having intercourse, 2) marked vulvovaginal or pelvic pain during intercourse or penetration attempts, 3) marked fear or anxiety about vulvovaginal or pelvic pain anticipating, during, or resulting from vaginal penetration, and 4) marked tensing or tightening of the pelvic floor muscles during attempted vaginal penetration (see also the “Sexual Function and Dysfunction” section later in Part 4).
Evaluation and Diagnosis
Vulvodynia is a diagnosis of exclusion—a pain syndrome with no other identified cause. A thorough history identifies the patient’s duration of pain, prior treatments, allergies, medical and surgical history, and sexual history. Cotton swab testing (see Fig.4-3) is used to identify areas of localized pain and to classify the severity of the pain. A diagram of pain locations and rankings of pain severity may be helpful in assessing the pain over time and response to treatment.
The vagina should be examined, and tests, including wet preparation, vaginal pH testing, and fungal culture, should be performed as indicated. Fungal culture may identify resistant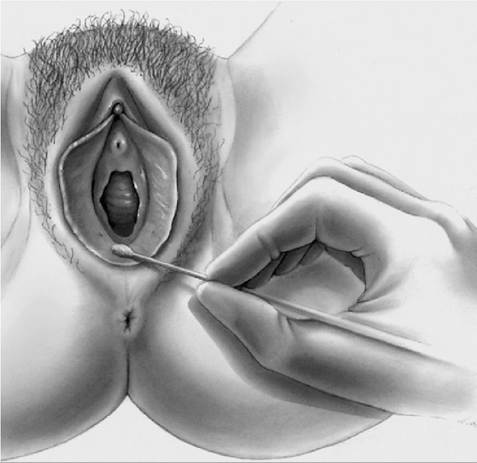
Fig. 4-3. Cotton swab testing. A cotton swab is used to test the vestibule for pain in diagnosing vestibulodynia. The vestibule is tested at the 2-, 4-, 6-, 8-, and 10-o’clock positions. When pain is present, the patient is asked to quantify it as mild, moderate, or severe. (Reprinted with permission from Haefner HK. Critique of new gynecologic surgical procedures: surgery for vulvar vestibulitis. Clin Obstet Gynecol 2000;43: 689-700.) ^
strains, but sensitivity testing generally is not required. Testing for human papillomavirus is unnecessary.
There are no definitive medical tests to diagnose vaginismus. As with vulvodynia, the diagnosis of vaginismus is made by exclusion of other causes. A thorough medical, social, and sexual history with complete physical examination, including a pelvic examination, are important to look for other causes of pain with sexual intercourse, such as dyspareunia.
Management
Many treatments have been used for patients with vulvodynia, including vulvar care measures (Box 4-5); topical, oral, and injectable medications;
Box 4-5. Vulvar Care Measures to Minimize Vulvar Irritation ^
• Wearing 100% cotton underwear (no underwear at night)
• Avoiding vulvar irritants (perfumes, dyes, shampoos, and detergents) and douching
• Using mild soaps for bathing, with none applied to the vulva
• Cleaning the vulva with water only
• Avoiding the use of hair dryers on the vulvar areas
• Patting the area dry after bathing and applying a preservative-free emollient (such as vegetable oil or plain petrolatum) topically to hold moisture in the skin and improve the barrier function
• Switching to 100% cotton menstrual pads (if regular pads are irritating)
• Using adequate lubrication for intercourse
• Applying cool gel packs to the vulvar area
• Rinsing and patting dry the vulva after urination
Data from Vulvodynia. ACOG Committee Opinion No.
345. American College of Obstetricians and Gynecologists. Obstet Gynecol 2006;108:1049-52.biofeedback training; physical therapy; dietary modifications; cognitive behavioral therapy; sexual counseling; and surgery. Newer treatments include acupuncture, hypnotherapy, immunomodulation, neuromodulation, and botulinum toxin. Treatments for vaginismus include education, sex therapy, and specialized physical therapy (with or without vaginal dilators), in addition to the treatment of vulvodynia, if that also is present.
Vulvodynia and vaginismus can be difficult to treat, and rapid resolution is unusual, even with appropriate therapy. Decreases in pain may take weeks to months and may not be complete. No single treatment is successful in all women, and combinations of vulvar skin care and medical and behavioral therapies often are needed. Expectations for improvement need to be realistically addressed with the patient. Emotional and psychologic support is important for many patients, and sex therapy and counseling may be beneficial (see also the “Sexual Function and Dysfunction” section later in Part 4).
Chronic Pelvic Pain
Chronic pelvic pain is a common disorder of women that often presents a diagnostic dilemma for obstetrician-gynecologists, and requires a multidisciplinary approach to its evaluation, diagnosis, and treatment. There is no generally accepted definition of chronic pelvic pain. One proposed definition is noncyclic pain of 6 or more months’ duration that localizes to the anatomic pelvis, the anterior abdominal wall at or below the umbilicus, the lumbosacral back, or the buttocks and is of sufficient severity to cause functional disability or lead to medical care.
A systematic, multisystem evaluation of potential sources is required, including the bladder, neurologic causes, psychologic causes, pain from birth trauma and pelvic surgery, as well as musculoskeletal and colorectal sources. Abuse is another important potential source to consider in women who present with chronic pelvic pain.
Pelvic pain is highly associated with childhood or adult sexual abuse and intimate partner or domestic violence. Clinicians should screen for abuse and be familiar with any state requirements for reporting occurrences (see also the “Abuse” section in Part 3).Chronic pelvic pain is frequently difficult to cure or manage adequately. A lack of physical examination findings does not negate the significance of a patient’s pain, and normal examination results do not preclude the possibility of an abnormal pelvic condition. If a cause is found, management should be directed at treatment of the underlying condition causing the pain. Referral to an appropriate specialist should be provided if the source of the pain is found to be nongynecologic in nature. If no cause is identified, management should focus on pain relief (see also the “Acute and Chronic Pain Management” section earlier in Part 4).
Bibliography
American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-5. 5th ed. Washington, DC: APA; 2013.
Crowley T, Richardson D, Goldmeier D. Recommendations for the management of vaginismus: BASHH Special Interest Group for Sexual Dysfunction. Int J STD AIDS 2006;17:14-8. [PubMed]
Haefner HK, Collins ME, Davis GD, Edwards L, Foster DC, Hartmann ED, et al. The vulvodynia guideline. J Low Genit Tract Dis 2005;9:40-51. [PubMed] [Full Text] Haefner HK. Critique of new gynecologic surgical procedures: surgery for vulvar vestibulitis. Clin Obstet Gynecol 2000;43:689-700. [PubMed]
Howard FM. Chronic pelvic pain. Obstet Gynecol 2003;101:594-611. [PubMed] [Obstetrics & Gynecology]
Lamont JA. Vaginismus. Am J Obstet Gynecol 1978;131:633-6. [PubMed]
National Library of Medicine. PubMed Health. Vaginismus. Available at: http:// www.ncbi.nlm.nih.gov/pubmedhealth/PMH0002457. Retrieved August 9, 2013.
Nizard J, Raoul S, Nguyen JP, Lefaucheur JP. Invasive stimulation therapies for the treatment of refractory pain. Discov Med 2012;14:237-46.
[PubMed] [Full Text]Vulvodynia. ACOG Committee Opinion No. 345. American College of Obstetricians and Gynecologists. Obstet Gynecol 2006;108:1049-52. [PubMed] [Obstetrics & Gynecology]
Resources
American College of Obstetricians and Gynecologists. Chronic pelvic pain. Patient Education Pamphlet AP099. Washington, DC: American College of Obstetricians and Gynecologists; 2010.
American College of Obstetricians and Gynecologists. Vulvodynia. Patient Education Pamphlet AP127. Washington, DC: ACOG; 2014.
American College of Obstetricians and Gynecologists. When sex is painful. Patient Education Pamphlet AP020. Washington, DC: American College of Obstetricians and Gynecologists; 2010.
American Society for Colposcopy and Cervical Pathology. Vulvodynia: the basics. Frederick (MD): ASCCP; 2010. Available at: http://www.asccp.org/Portals/9/ docs/pdfs/Practice%20Management/Vulvodynia%20Basics.pdf. Retrieved August 9, 2013.
Female sexual dysfunction. Practice Bulletin No. 119. American College of Obstetricians and Gynecologists. Obstet Gynecol 2011;117:996-1007. [PubMed] [Obstetrics & Gynecology]
National Vulvodynia Association. Available at: http://www.nva.org. Retrieved August 9, 2013.