Emotional and Mental Well-Being in Multiple Pregnancy
Lala Langtry White
Introduction
Pregnancy and parenting in any form continuously challenge and influence parents' mental and emotional well-being - as a collective family unit and as individuals - in a way few other life events do.
The benefits of a parent-centred, holistic approach to healthcare in supporting the mind-body duality are no longer in question. Integrated care is crucial to support both aspects of an individual's well-being.The additional mental and emotional considerations for families pregnant with or parenting multiples may be as unique as the person themselves, but, in my experience as a parent of twins and a parent of multiples (PoMs) support specialist, there are considerable commonalities that are rarely fully understood outside the multiple birth community. Families face significant and specific challenges during pregnancy and the first years of their babies' lives. A lack of quantitative research and feedback within this context contributes to a continued lack of sufficient appreciation, empathy and support. Using primarily an empirical and anecdotal approach, this chapter aims to highlight common concerns, observations and perspectives and provides considerations for healthcare professionals to better support the mental and emotional well-being of the mother and family - from pregnancy to parenting - following these fundamental steps: recognise, empathise, signpost and reflect.
Antenatal Considerations
Recognise and Empathise
As a healthcare provider, your first interaction with PoMs is likely to be discovery of multiples during a scan. Whether you are supporting a family with a genetic predisposition towards multiples, a pregnancy resulting from assisted reproductive techniques (ART) or a spontaneous planned or unplanned pregnancy, it is very likely discovering twins, triplets or more elicits a range of emotions that battle to be recognised simultaneously.
If the information is first imparted within an empathic space allowing parents to process and validate new and possibly unexpected feelings and reactions, this paves a positive pathway for future emotional well-being, shaping the mental health support offered by healthcare professionals. Whoever gives this news sets the tone of all subsequent interactions.Historically, societal reactions have varied greatly, from seeing multiples as symbols of luck to a fascination that has seen them subjected to anything from questionable exposure to a type of reverence. More common in modern, Western society is the culture of negatively cliched statements such as ‘double trouble'. Rarely amusing or helpful, these statements reiterate the ‘rather you than me' ostracism parents of multiples (PoMs) often feel. Equally, if parents struggle with accepting the news, overly enthusiastic statements may also be inappropriate. Instead, allowing parents to form their own reactions, addressing their concerns and providing unbiased support and links to peers who may better understand or have shared a similar reaction, sets up a supportive approach from the outset.
Signpost
Being proactive in referring families to local, national and international organisations and support groups is essential (see Chapter 30). In addition, linking PoMs to well-established online social media groups provides an instant connection to other PoMs. This becomes more pertinent the rarer the subset: higher-order multiples, loss within a multiple pregnancy, twin-twin transfusion syndrome (TTTS), twin anaemia-polycythaemia sequence (TAPS) or parenting children with special needs. The possibilities are multiple. Finding others who share a similar experience can be an essential part of coping with the psychological component. While PoMs undoubtedly face a surfeit of challenges, there is also an unquestionable joy in parenting multiples. While this chapter may focus on mitigating the more challenging physical and psychological tolls of parenting two or more babies simultaneously, it is important to connect parents to the joys too.
As a mother of two singletons as well as twins, I have observed a unique kinship between PoMs that simultaneously normalises, sometimes bemoans, but revels in the privilege of parenting multiples.I could reach out online, day or night, and without fail find someone, somewhere, instantly combatting my feelings of isolation who shared similar feelings of being overwhelmed. That non-judgemental understanding was (and continues to be) a lifeline for my mental health at some really challenging times. Though I never met the majority of parents in person, some were even on opposite sides of the world, we have bonded and followed one another through the challenges and the mini triumphs that may seem insignificant to other parents. We have supported and celebrated each other in a way I don't share with my friends who don't have multiples.
Many questions are likely to arise, for multiple pregnancy brings multiple scenarios of placentation, gender and fetal and maternal health alongside varied financial and familial dynamics. Many parents may be unaware of these differences and the implications for their healthcare requirements during pregnancy. The disproved theory that all monozygotic twins share a placenta still prevails, even within the obstetric and medical communities. Zygosity is important to know in terms of the medical and genetic implications, but also as part of the psychology of being or parenting multiples. Yet zygosity testing is not routinely offered to parents or comes at considerable cost, illustrating a lack of awareness of the effects on both child and parent. It is a belief of the International Council of Multiple Birth Organisations (ICOMBO) that same-sex multiples with undetermined zygosity have a human right to establish zygosity.1
While the potential obstetric risks of a multiple pregnancy are well documented and care plans are in place, the risks to parental well-being in relation to isolation, perinatal anxiety and depression are often overlooked.
Although specific studies are lacking, the majority of evidence gathered to date suggests parents of twins or more are at increased risk.A published study showed a large, unmet need for mental health treatment in parents of multiples during the perinatal period, especially the early post-partum months.2 Two hundred and forty-one parents of multiples completed survey questionnaires: 197 were the mother and 44 were spouses/partners. The survey identified the first three months as the hardest, with few participants receiving any form of mental health support. The most common barrier to care was a lack of time. Forty-eight per cent would have been interested in some type of mental health treatment during pregnancy or the first year after birth. Participants reported a wide range of concerns, including elevated symptoms of depression/anxiety and stress levels, relationship issues and ‘managing having multiples’. The lead author, a mother of twins, identified that ‘eHealth strategies seem particularly feasible and acceptable in this population and may help circumvent common barriers to care’. A further small qualitative study in 2020 by the same lead author reiterated these findings, identifying ‘experiences that were unexpected and unique to parenting multiples and indicated numerous desired aspects of mental health treatment. Interest in internet-delivered care was especially high.’3
Patient Psychosocial Considerations
From the outset, the path to parenting multiples may come with an increased incidence of emotionally challenging factors that may complicate parental well-being. The parental unit may not be limited to the mother. Establishing a psychosocial history whereby parents can choose the disclosures they wish to share with their medical care team would benefit all concerned. This would be achieved through a form with options to provide information such as:
• Language barriers, disability or learning support needs.
• Any influencing or additional factors the mother and supporting family dynamic would prefer healthcare providers were aware of.
These may include ART, surrogacy, previous loss, trauma or abuse, female genital mutilation, financial disadvantage, familial and/or housing and living circumstances, insurance issues, cultural beliefs or practices relating to pregnancy and birth or LGBTQI+ parenting.• How they would like to be referred to, encouraging inclusivity.
• Who will be part of the decision-making process relating to pregnancy, birth and care of the babies.
• Any areas in which they would like further support or signposting to additional services such as mental health support, breastfeeding education, antenatal classes for multiples, peer support groups and so forth.
This is simple, cost-effective and unanimously applicable. It provides an opportunity for healthcare professionals to take proactive, sensitive steps towards individualised emotional support in tandem with physiological care. Failure to recognise and address these areas can mar pregnancy and the parenting experience from the start with long-reaching and potentially devastating consequences continuing throughout the post-partum period.
This measure could be further evolved into identifiable visual prompts on paper or electronic health records so that parents need to provide this information only once. This can be applied to many of the aforementioned scenarios such as parenting after infertility, loss and surrogacy.
For example, in the case of families who wish their care team to be aware they are parenting after loss, UK-based organisations such as Dear Orla and SANDS offer identifiable, downloadable stickers to place on or within patient records to notify professionals that the parents in their care may require additional understanding and sensitivity. This is especially pertinent for parents who have lost one or more babies during multiple pregnancy, either spontaneously or through fetal reduction, and who may have to continue the pregnancy and give birth to both living and deceased babies. A unique potential dynamic in multiple parents is managing grieving for one or more babies while caring for one or more surviving babies.
Giving emotional space to parents who experience loss at any stage and validating their experience and feelings along with offering signposting to specialised professional and peer support is essential.The same sensitive acknowledgement could easily be applied to any influencing scenarios. Another area of awareness within multiple pregnancy is the lasting emotional impacts of infertility (see Vignette 1).
Vignette 1

After undergoing a prolonged Infertilityjourneythere may be continued mental health issues to be considered, especially in the case of a multiple pregnancy. Issues of anxiety will tend to be amplified in these cases. Often there are medical issues which have prevented spontaneous conception resulting in the birthing person feeling like they have already failed as a parent. When pregnancy is finally achieved these feelings of inadequacy do not simply disappear. The person may well be more concerned than someone who has not had ARTforthe health of herself and her pregnancy. She may have over informed herself on potential risks of a multiple pregnancy and have many concerns and questions. Thoughtful, attentive listening, giving parents a sense that all their questions and concerns are valid and welcomed, being empathic and reassuring whenever possible is key in enabling the birthing person to relax into their pregnancy experience. IVF and other methods of assisted reproduction can bean incredibly stressful experience. The pregnancies that result from them are often beginning from a place of anxiety and stress which may continue through pregnancy and into parenthood. An understanding of that situation is important to families who are navigating their multiple pregnancy. This may be particularly challenging to identify within parents who have travelled overseas for fertility treatment due to restrictions within their own country and may feel unable to freely express how they're feeling.
Cassie Destino, mother of twins and founder of IVF Support UAE
Psychological Impact of the High-Risk Label: When Does Awareness Become Anxiety?
Though not specific to families of multiples, Wright et al examined the effects of high-risk pregnancy on the parental adaptation process.4 The families included all had full-term, healthy infants, yet the appearance of high obstetrical risks appeared to negatively influence the perception of parental competence beyond pregnancy and into parenting. Further studies, articles and observations support this theory.
Most multiple pregnancies are automatically categorised as high risk. Attached from the outset, this label can provoke a range of reactions. Not all parents expressed a negative connotation: some embraced the feeling of uniqueness and heightened medical vigilance while others were ambivalent. Others reported feelings of increased vulnerability, hypervigilance, anxiety, resentment or disempowerment due to the change in expectations of pregnancy and birth. We know increased anxiety can result in detrimental physiological responses such as increased blood pressure, shortness of breath, increased cortisol levels and generally lower levels of physical comfort and mental clarity. This association extends to feelings of guilt, responsibility, helplessness and anxiety reported from birth partners.
An article by the Association for Improvements in the Maternity Services (AIMS) reflected that ‘with the “high risk” label comes an additional reliance on care providers for information and guidance. The content and emotional tenor of this advice will be heavily influenced by the clinicians’ background and experience. ‘I saw two consultant obstetricians at two different Trusts and they were each concerned about entirely different aspects of my twin pregnancy! Nevertheless, the experience of talking to them was positive and I felt that they respected my right to make “unusual choices”. I know this is not the experience many women have of maternity services.’5
Supporting parents psychologically so they can make an informed choice is especially important when considering the profound long-term consequences of fetal reduction. It is essential that healthcare professionals are knowledgeable about the potential for complications and it is equally important that they can inform and offer non-directive counsel to parents clearly, sensitively and without exerting personal bias (see Vignette 2).
The potential implications of this were raised in an article by Zager:6
Vignette 2

We were under the care of a respected fertility doctor when we became pregnant with our triplets following IUI. Our doctor strongly recommended fetal reduction to improve our chance of a pregnancy without complications. After considering our own circumstances [and] feelings and speaking to other triplets mothers, we declined fetal reduction and made this clear to our doctor. However, I was continually reminded of the hypothetical risks at each appointment, and felt stressed by the pressure exerted to reconsider; I was made to feel I was making a poor choice in continuing with expectant management in place of reduction. Although I am eternally grateful to our doctor for our treatment and resulting pregnancy, I would like to see a more individual, unbiased and respectful approach to counselling families on their options and supporting their subsequent choices.
Suman Manning, mother of triplets and founder of Twins Plus Arabia Forthe woman pregnant with two or more fetuses, issues of termination for one or more of them produce anxiety, guilt, and the need to cope with decisions well beyond those of a usual pregnancy, particularly when they have resulted from infertility or similar treatments. The decision to terminate selectively certain of the fetus(es) so that one (or more) can be carried more viably to term represents a significant stress. The woman may continue the pregnancy with the remaining fetus(es), but she probably will be assailed with feelings of responsibility for the death(s) of the other fetus(es);feelings of sadness, guilt, grief, and mourning for them must co-exist with the more expected and positive anticipatory ones in the usual, wanted pregnancy. She will also be beset with increasing anxiety over the fate of the remaining fetus(es).
Studies within pregnancies deemed high risk (not specific to multiples) consistently report increased maternal depression and anxiety. It is therefore reasonable to assume that the high-risk label may influence perinatal psychological well-being and contribute to a lack of confidence emotionally and physically to trust in the body's ability to grow two or more babies without complication or intervention. In turn, this and the need for specialised medical support may cultivate a passivity in decision-making surrounding care choices for pregnancy and birth and unintentionally undermine parental instincts from the outset, potentially leading to a negative or disconnected birth or parenting experience.
If we take a family who has had a fertility-assisted path to conception, a high-risk, medically intense pregnancy who potentially began parenting within the neonatal intensive care unit (NICU), we can see that parental instinct and involvement can be unintentionally undermined by the necessary processes of medical care and a belief that the medical care teams at each stage know best. As a result, often women and parents perceive their role in the pregnancy according to the inverted pyramid model (see Figure 28.1). In this traditional paradigm, parents' personal knowledge, choices and instinct regarding their own and their babies' well-being are perceived as of lower value than those of the experts caring for them (see Vignette 3).
The question to ask as part of this team is: how can we lessen the culture of fear, anxiety and anticipation around the high-risk label in multiple pregnancy, increase the normalcy of
Vignette 3
From the very beginning of my egg-donation twin pregnancy, I felt I lost my ability to make sound decisions. I refused to invest - financially or emotionally - in my impending motherhood and was consumed with fear. I feared pregnancy failure because I believed that my pregnancy was 'against nature'. As a 45-year-old woman in possession of one partial ovary, I had no usable eggs of my own. I believed that I was flaunting nature in being pregnant and that this would have a price. I feared the price might be pregnancy failure;what I see now looking back is that the price was my own ability to accept and enjoy my pregnancy and early motherhood. I felt that I could not have any natural motherly instincts as nothing about my pregnancy was natural. In pregnancy this meant I did not engage in the decision-making process. In early motherhood this meant I felt afraid and barely capable of parenting. In both phases I preferred to wholly trust and leave choices to medical experts believing they knew better than me. I regret not playing more of an active role in my pregnancy and allowing others to do so much of the mother role for me instead of in support alongside me. I am certain that my negative experience of pregnancy and the first year of motherhood was because I did not feel like a mother because I was not able to be a 'real' mother. Five years later, I am still not wholly rid of this belief.
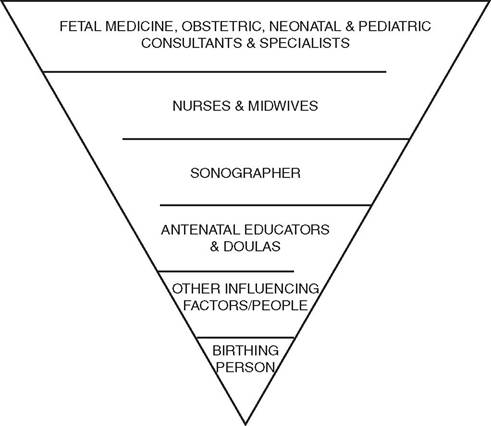
Figure 28.1 Provider
Involvement in patient wellbeing
multiple pregnancy and create a more engaged and empowering experience for parents while maintaining a watchful awareness of potential issues?
Encouraging multiple pregnancy to be viewed as a variation within the norm rather than simply ‘high risk' and ensuring parents understand the potential risks/complications in relation to their individual pregnancy plays an important role in framing parental confidence. We can help families understand that an increased chance of something happening does not mean it will happen and that awareness of potential complications does not equate to a self-fulfilling prophecy. Giving parents confidence to ask questions and feel fully informed rather than fearful creates a culture of trust. This may require providing longer appointment times for PoMs so that their questions and concerns can be addressed without feeling rushed as well as contact details for families to utilise outside of appointments if needed.
Reassurance that every element of the surrounding team is there to support them and their babies' well-being through pregnancy, birth and into parenthood as opposed to waiting to diagnose potential complications is desirable. Encouraging co-decision-making without dissolving the doctor-patient relationship builds confidence and trust in both the medical team and themselves as parents (see Figure 28.2).
Emotional Impact of Contested Interventions
This area continues to raise much debate within both the medical and PoMs communities. The recommendations of contested interventions such as bed rest, cerclage, progesterone treatment, high-protein diets and so forth are routine within certain care environments. While evidence for the physical benefits may be debateable, the emotional implications are varied and complex. Some parents report these interventions gave them a feeling of
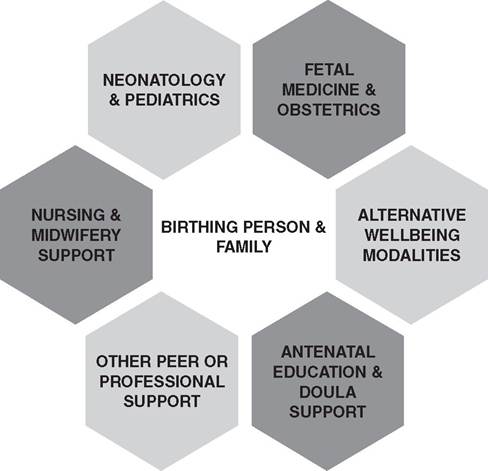
Figure 28.2
regaining control over their well-being. Conversely, others felt undue pressure and responsibility that their immediate actions could harm their babies in some way.
My doctor recommended cerclage, progesterone and strict bed rest from 12 weeks of my IVF triplet pregnancy and I trusted she had our best interests in mind. I felt certain that this, coupled with a high-protein diet, were what got me through to my planned birth at 34 weeks. I felt I was taking every necessary and possible precaution to give my babies the best chance of being born at a good gestation and good birthweight.
Bed rest is notoriously challenging to mental health and often misunderstood by those who haven't experienced it as an ‘opportunity to put your feet up and do nothing'. Individual circumstances may require consideration, but the disparity in blanket recommendations, particularly for triplets and higher-order multiples, from region to region or doctor to doctor raises concerns within the PoMs support networks. Some parents are adamant that it has/will lead to a healthy pregnancy/babies, while others who have not had such recommendations fear they may be jeopardising their babies' well-being by not doing so. For others, it may have ramifications on family life with older siblings, potential loss of earnings or early forced maternity leave diminishing the time allowance once the babies are born.
My doctor recommended a cerclage would be prudent during my spontaneous triplet pregnancy. I did my own research and felt there was not enough evidence to support its use within my individual pregnancy. I presented my research and my doctor was supportive of my decision. I ended up carrying my triplets to week 36 without bed rest, interventions or a deliberate course of action other than listening to my body and not overdoing it.
Further clarity about such interventions would be beneficial for all parties, particularly in relation to the emotional impacts it has both on those to whom they are recommended and on those who worry about the lack of such recommendations.
Emotional Consequences of Physical Challenges
While it is important to recognise that many enjoy a comfortable and uncomplicated pregnancy, multiple pregnancy often increases the incidence and the severity of ‘normal’ physical pregnancy symptoms such as nausea, vomiting, muscle cramps, fatigue, haemorrhoids, pelvic and back pain, constipation, heartburn and varicose veins. Without generalising the distress these can cause, we must acknowledge that these physical tolls can enormously impact emotional well-being. Feedback from mothers showed many felt their challenges in this area were dismissed or downplayed; there was a ‘just get on with it’ attitude which significantly marred their enjoyment of and emotional well-being within pregnancy. It was especially highlighted by those who had experienced a singleton pregnancy and were taken aback by the difference in carrying twins or more. Listening with empathy, normalising without being dismissive and discussing ways to alleviate symptoms is desirable. Equally, be aware of perinatal specialists in alternative modalities such as chiropractic, osteopathy, acupuncture, reflexology and so forth that may help physically and provide an additional layer of emotional support.
Here too peer support can be of enormous, cost-free value and offer a perspective from others who have shared similar struggles. As mentioned previously, being informed of online and in-person support groups and, where possible, offering a space for regular meet-ups within your facilities is a responsible and proactive move towards ensuring greater social support for PoMs. Various evidence, as summarised by a Cochrane review, confirms that for ‘women at low risk of complications and some at increased risk, but not currently experiencing problems’, the midwifery-led model of care increased positive parent experiences.7 It also led to fewer preterm births and fetal and NICU deaths. In multiple pregnancy, while specialist obstetric care may be essential, where possible, a multidisciplinary care model involving a midwife may offer additional support and serve to normalise pregnancy and postnatal experiences. Parents can raise questions they may feel more comfortable addressing with a midwife, meet other PoMs and benefit from group discussions and signposting to further mental health support services.
Antenatal Education
Antenatal education classes, whether in person or through eLearning, can be important for parents to develop well-being strategies. They can also provide information about local parenting networks and events which, for some families, are the beginning of their parent peer support community. Parents of multiples often report that while generalised antenatal classes are helpful to a point, segregation from singleton parents can exist and multiple parenting was an insufficiently covered addendum or an exception to ‘the norm’.
During pregnancy is when PoMs generally have greater ability to take classes that are applicable to all modalities of parenting and classes that are more pertinent within the context of parenting multiples. For example, while statistically one in nine babies are born prematurely, NICU parenting is unlikely to be covered in depth within routine antenatal classes whereas around 40% of multiples require NICU or special care support after birth. Understanding factors regarding timing and mode of birth can encourage PoMs to find confidence in their decision-making. Likewise, mothers of multiples need breastfeeding education specific to multiples.
Multiple-specific antenatal education may manage parental expectations, emphasise mental well-being, raise awareness of symptoms for parents to be aware of and provide pre-emptive signposting to mental health support, as well as encourage selfconfidence, self-reliance and inclusion. Incorporating classes within your practice or knowing where to refer to externally or online would be a proactive and positive approach.
Not Just One Day in Your Life: Making Birth More Parent Centred
Mode of Birth
Birth is unique and transformational for all parents, no matter whether they are parents to a single baby or to multiples. How a mother is engaged with, supported and cared for will have a lasting impact long beyond the day of birth. Within the context of twin births, we know there are many influencing factors when it comes to deciding the optimal timing and mode of birth. Ensuring these factors are fully understood by a family and framing the conversation so that they can take an active role in the decision-making process is important. An informed, competent parent should be the appropriate decision maker about what is best for their birth, with the support, expertise and guidance of their care team. Empowering parents in the decision-making process is essential in starting the parenting journey engaged and with confidence.
It is important that as guidelines are updated they are represented in the options given to families. Evidence shows caesarean birth is not the safest mode of birth as a blanket rule, but it remains the preferred mode of birth in many healthcare settings. As we continue to see high rates of caesarean birth for twin births, where all influencing factors are optimal, we need to question whether further professional development is required to improve confidence levels in changing practice. No parent wants to ask their care team to support them in a choice they don't feel competent or confident in, or to knowingly jeopardise the well-being of their babies, but we routinely see bias exerted and parents pressured to make decisions based on outdated practice, scaremongering or convenience. Parents who have gone through an ART journey often hear the phrase ‘precious babies' used to influence a decision. While it stands to reason that no one would be any more cavalier with care for babies conceived spontaneously, once that hint of doubt or fear creeps in it is hard to make a choice based upon evidence and parental preference. This is another scenario where care shared between a multidisciplinary team of fetal medicine and obstetric consultants, together with midwives, may be beneficial not only psychologically but also physically (see Vignette 4).
Vignette 4
During the course of my MCDAtwin pregnancy, I moved between two countries, experiencing a multidisciplinary midwifery/obstetric care model and then a purely obstetric-led system. Although a language of risk and a strong bias towards caesarean birth prevailed under both systems, my maternal wishes for vaginal birth felt more understood by midwives, who recognised and prioritised my informed birth choices as integral to my birth experience and birth outcome. I was fortunate that my pregnancy was uncomplicated and my first baby presented head down so that circumstance and perseverance together led me to a vaginal birth by induction, with an intervention- and trauma-free second-stage labour at 35 weeks. This enabled me to immediately follow my babies into the NICU, initiate breastfeeding without disruption and recover in good time to meet the physical, mental and emotional demands of caring for two premature newborns. My gratitude for my labour extends far beyond the birth experience; it served me and my babies in the immediate aftermath of my birth and set a foundation for the strongest possible start from which two lives could flourish. Having benefitted from the best of both, I would confidently advocate for an integrated care system which balances the obstetric expertise of intricate twin pregnancies with the parent-centred approach for which midwives are deservedly recognised. For, alongside medical aptitude, women-centred care that recognises each woman's social, emotional, physical, spiritual and cultural needs is vital for mothers faced with the unique risks, challenges and promise of birthing and raising multiples.
Brit Williams, perinatal fitness author and mother of twins To be accompanied by Figure 28.3

Changing the Language around Birth
Babies are not pizzas; they are born not delivered.
Rebecca Dekker, PhD, RN, founder of Evidence Based Birth
Small differences in language can have a big impact on how engaged and empowered a parent feels in the birth experience. Parents need to be supported with appropriate expertise rather than ‘managed’. You may support a person's birth, but no matter how that baby is born, framing it as their birth rather than your delivery changes the onus enormously back to it being the parents’ active experience than something in which they played a passive, secondary role.
Birth Support
Within the context of birth of multiples, other small differences can have a great impact on creating a parent-centred experience. An additional support person, whether family, friend or doula, in a multiple birth scenario may result in more positive birth experiences for PoMs.
Due to circumstances in my pregnancy, my partner and I understood it was likely our babies would be born prematurely and would need to go to [the] NICU. It was my partner's preference that I went with the babies straight after birth and remained with them initially. My concern at that point was primarily for my partner's well-being and I felt hesitant at the thought of leaving her side. We chose to employ the support of a doula who was experienced in supporting multiples, who would remain beside my partner in theatre and into recovery, while I stayed with the babies. This was invaluable in making the day of our children's birth a fully supported experience of excellent medical and emotional care. I found great comfort and confidence knowing there was someone there to support us both, who understood what that day might look like for us from an emotional perspective and whose focus was solely on our emotional well-being. She was able to help my wife establish early expressing of colostrum and act as a liaison between me in [the] NICU and my wife in recovery.
Father of twins
Allowing parents to create their own support framework, within logistical reason, enables them to continue to have choices, even when they may have felt restricted by the circumstances of their multiple pregnancy. For parents from the LGBTQI+ community, parents of colour, parents from indigenous or minority ethnic groups, parents with particular religious or cultural influences or parents birthing via surrogacy or from other minority demographics, allowing greater choice in framing the support system may be an important step in recognising individuality and fostering early parenting confidence without compromising the work and expertise of the medical team.
Birth Environment
Encouraging parental input and choice wherever possible can have a significant impact on how engaged parents feel, especially where parents may not have been able to choose the mode of birth they would have liked due to maternal or fetal factors. For example, they can choose who is there to support them, opt to make the environment and lighting more sympathetic and less clinical, make informed choices about pain relief and, crucially, provide informed consent at every stage of labour and/or birth.
Being able to choose the song that each of our babies was born to was a small detail that made a big impact on reclaiming some individuality and choice in an otherwise, highly medicalised, caesarean birth experience for us as parents. Cutting the umbilical cord was something I'd always imagined doing as a father. Our doctor respected our wish for delayed cord clamping of two minutes and then cut the cords to be long so that I could cut them shorter up on the warmer which meant a lot to me and helped normalise and personalise our birth experience.
Navigating the Emotional Roller Coaster of the NICU and Special Care
Mental Health Support
A 2018 survey by UK-based charity BLISS revealed that 80% of parents whose babies were admitted into neonatal care think that their mental health suffered after their experience.8 Some were formally diagnosed with PTSD and postnatal depression while many felt they had developed a mental health condition but were not formally diagnosed. The vast majority of families did not have access to formal psychological support during their time in the unit or once discharged home. With twins 10 times and triplets 30 times more likely to be born preterm, it is logical to take a pre-emptive approach towards addressing the psychological strain of parenting in the NICU. This preparative approach could be incorporated in the aforementioned antenatal classes specifically for PoMs, healthcare-facilitated group support meetings and peer support systems. Further research is needed to understand the unique dynamic that parenting multiples in the NICU presents.
Issues repeatedly raised by families of multiples with one or more babies in the NICU include but are not limited to:
• Feeling disempowered and helpless as parents.
• The emotional implications of having babies separated, be it to different beds, rooms or units within a hospital, or to a different hospital entirely.
• The additional financial strain and time constraints for both parents.
• The challenges of balancing older siblings alongside one or more babies in the NICU.
• Staggered discharge and the effects on parental ability to spend adequate time with either baby once one or more of a set of multiples is home when one or more remains within special care.
• The challenge of expressing for two or more babies.
• Establishing breastfeeding, especially when rooming in or parent accommodation is not available.
Starting any parenting journey within the NICU or special care is emotionally challenging. It may mean parents are separated from their baby having barely seen them, and this may continue for some hours or days depending on the health of the mother. Even parents who felt they had prepared for a NICU journey report being overwhelmed by the actual experience.
Even though we had older children and we had met the neonatology team and discussed what those first few days might look like, I was emotionally floored by the difference in experience from my previous births. Recovering from a caesarean birth, being separated from my babies, being placed in a busy ward with other mothers who had their babies with them, trying to express precious colostrum... the whole experience was incredibly traumatic and, I felt, the catalyst for my poor mental health in those early months.
It is essential that psychological support for the whole family be made a priority alongside the physical care of the babies in NICU. Where professional support within a unit is not possible, partnering with local or national psychological support centres and systems should be investigated and encouraged (see the list of support organisations at the end of this chapter). In addition to multiple-specific support communities, NICU support organisations provide another avenue for peer-to-peer support.
Family-Integrated Care
We know the evidence to support kangaroo care as a means of therapeutic and bonding practice for both parents and neonates is overwhelming (see Figure 28.4). However, parents consistently report feelings of anxiety or a lack of support in carrying out this practice. One reason seems to be the lack of clarity surrounding the stability criteria for babies before carrying out kangaroo care. Further research and clearer guidelines would benefit both staff and parents. It is also an area that parents who experience the death of one or more of their multiples during or after birth, particularly in relation to infection, may struggle with when caring for surviving multiples, and awareness of this and specialised support within units is essential. Understanding the benefits and risks of tandem or more kangaroo care with multiples needs to be similarly explored.
Involving parents in other aspects of their babies' routine care is also shown to have benefits both within NICU and longer term, post discharge. Most parents are not aware of

how they can care for their baby when they first enter the ward; typically they express feelings Ofhelplessness and being overwhelmed. Having supportive and encouraging staff to guide their involvement as early as possible is an essential way to care for both parents' and babies' emotional well-being. Taking time to show parents how to care for, feed, clean and hold their baby fosters parental confidence. It is also important to recognise that parents may feel they have surrendered much of their hopes of parenting and that important firsts such as first feed, first bath or first cuddle are momentous and must be respected and celebrated appropriately.
Although I was rooming in at the hospital, I was shocked to come up to the NICU one night to feed my babies only to have a nurse share with delight that my babies had just enjoyed their first bath. To say I was devastated is an understatement, and I was so angry that my consent had not been sought, nor my desire to be involved even considered! I don't doubt she had my babies' best interests in mind, but I felt it was at the expense or ignorance of my well-being and [I was] robbed of another 'first' for my babies that should have been with me.
Parents who are encouraged to spend time observing their baby are more intuitive and often the first to notice if their baby is ‘out of sorts', potentially enabling earlier medical intervention where needed. Offering signposting/access to specialised mental health support and allied healthcare professionals would be beneficial. Early lactation support for expressing and guidance in initiating non-nutritive sucking and then breastfeeding is especially valuable at this early stage. Acknowledging the mother's wish to work towards exclusive breastfeeding is imperative to ensure that her goals are aligned with those of the babies' weight gain and well-being. Many mothers report feeling that the goal within the NICU was to grow the babies to a healthy discharge weight and that this sometimes came at the expense of establishing breastfeeding. Creating a plan with the mother and care team to support both goals benefits babies' and mothers' well-being. Helping parents to understand the roles of allied professionals such as physiotherapists, dieticians and occupational and speech therapists creates a clear support structure for parents with babies who may have longer-term support needs from birth. It also offers a chance for parents to avail of additional emotional support within one place and before the time constraints of fulltime care of multiples makes this more challenging.
Acknowledging Twinship While Cultivating Individuality
Parents of multiples describe feeling that their babies draw comfort from one another after birth and often find it distressing to see their babies separated, especially when this may mean hours of distance between them. While this may be unavoidable, reuniting parents and babies within a single unit must be a priority. The evidence to support co-bedding of twins or more in relation to co-regulation or therapeutic benefits is conflicting and in short supply. A Cochrane review raises the issues of infection, medication errors and caregiver satisfaction.9 On the basis of the available evidence, the authors could not make recommendations for or against co-bedding and recommended further research. Parental feelings should be considered as the majority of parents embrace the concept of their babies cobedding in the NICU, as long as it poses no risk to the babies' well-being. Where parents cannot be with their babies full-time, comfort may be drawn from the fact the babies have physical contact with one another, a unique advantage to parenting multiples.
While PoMs may be keen to keep their babies together, having them recognised as individuals within the NICU and during their follow-up healthcare is often felt to be in stark contrast to single babies. It would be surprising for a single baby to be referred to generically as ‘baby’ for an extended duration after birth rather than by name; however, multiples are often referred to as twin 1 or 2 for days, weeks or months after birth. While identifying multiples can be challenging and a clear difference in identification is undoubtedly needed for clinical care purposes, individualised care has a big emotional impact for parents. Having a simple white board or sticker system for each incubator or cot that identifies the baby’s name, parents’ names and multiple siblings’ names where appropriate is a simple way to make an alien environment feel more personal and a way for parents to communicate with healthcare professionals when not with their baby.
Bereavement
Small differences in personalising care make a big emotional impact on parents. This is never more crucial than when supporting parents through the loss of one or more of their babies. The Purple Butterfly Project in the UK is one organisation concentrating on increasing bereavement support for families who lose one or more of their twins, and their awareness videos are an essential watch for anyone caring for multiples in an NICU setting.
One of their simple suggestions is offering a card or sticker with, for example, a purple butterfly to be placed on or within the cot of a surviving twin to acknowledge their bereavement and the twinship of the surviving baby/ies. Specialised bereavement support services that recognise the unique dynamic of caring for one or more babies when one or more babies has died are essential. Many hospitals offer memory boxes or memory making for bereavement and it is important where possible to take photos alongside their twin as this holds enormous value not just for parents, but also for surviving multiples. Parents often struggle to comprehend memory making at the time but almost always later report that it brings enormous comfort. Explaining this in a sensitive, unhurried manner and repeating, if necessary, so that parents understand all options available to them, is essential.
It is also a crucial role of the medical team caring for the surviving baby that they feel confident to engage with the parents who may want to talk about the baby they have lost, helping them to care for their grief within their unique context as PoMs. Where possible, providing privacy for families within the ward environment is beneficial. Be mindful that parents may have to return to the ward where they have lost a baby, or to see another baby in the cot or space where their baby had been while visiting their surviving twin, and this may be extremely traumatic. Empathy, validation and continued support are critical, especially when many families report having to ‘keep it together’ for the sake of their surviving baby and may seem to be coping on the surface. An instantly identifiable visual reminder such as the aforementioned purple butterfly helps staff to identify where additional sensitivity is required.
Acknowledging External Strains and Stressors
Additional time and financial pressures exaggerated by having two or more babies in the NICU are significant contributing risk factors to parental well-being. Alleviating stressors on parents at a basic level such as reduced parking costs and longer or more flexible appointment times should be considered wherever possible. Advocacy or lobbying for

Figure 28.5 Sibling with twins in cot
better parental leave - both within individual scenarios through proof of medical care letters for employers and on a governmental policy level for parents of preterm babies and multiples - as well as for more comprehensive insurance coverage, where applicable, may shift the landscape of early parental support and well-being within the context of parenting multiples in the NICU. Family dynamics such as older siblings should be equally taken into consideration and helpful childcare strategies established, as well as ways to include them, focusing on the well-being of the family as a whole as they navigate the NICU together (see Figure 28.5).
Our time spent in the NICU was a really emotional journey for our whole family. Our older children had limited access to us as parents and they were not allowed into the NICU to meet their siblings due to infection control policies. They had to be content with photos of the babies and a team effort of extended family and friends to keep their day-to-day routines running while we drove back and forth from hospital. Taking small steps to include them such as having them draw pictures and print photos of themselves that we could laminate and stick on the incubators, and in turn taking photos back to them, telling them how much their baby siblings loved them, went some small way to helping them feel included in caring for babies they had never even met.
This challenge only continues when one baby is discharged ahead of its multiple sibling(s); hospital policies vary enormously on the protocol for visiting the NICU with a discharged baby. Where there is no provision for support or care for the discharged twin, it creates additional emotional pressures and stress on parents, particularly in the context of older siblings and/or single parenting or where one parent has had to return to work. Offering options for rooming in or parent accommodation may not be feasible or practical in all scenarios, but it would be an important consideration for supporting physical and emotional recovery and the transition to parenting should parents desire this option.
Post-partum Well-Being
Post-partum Recovery and Adjusting to Parenting
A published study concluded that PoMs had 43% greater odds of moderate to severe postpartum depressive symptoms at nine months compared with mothers of singletons and that greater attention is needed in paediatric settings to address maternal mental and emotional well-being in families with multiples.10
Parenting rarely has a gentle introductory period, and this is never more so than with multiples. For a significant majority of mothers, it may also include the discomfort, restrictions and physical recovery period associated with caesarean or assisted birth. It is important that when discussing mode of birth prenatally, families understand these considerations as far as possible and the implications they can have for caring for two or more newborn babies as well as for their own sleep, physical comfort and emotional well-being. Though research regarding mode of birth as a risk factor for post-partum depression is varied, some empirical studies report that mothers who give birth by caesarean section are more likely to experience a negative self-image and anxiety. No matter the mode of birth, it is important that every mother be made aware of what the short- and longer-term birth recovery period may look like from both a physical and an emotional standpoint. Parents need to understand the role adjusting hormones play in emotional well-being - particularly over the first fortnight - how to recognise the ‘baby blues' and how to differentiate between them and post-partum depression or anxiety. Although it is important not to generalise distress or expectations of the post-partum period, parents need to understand what those early weeks may look like, what is ‘normal', how to cope with the extremes of exhaustion associated with caring for multiple newborns and when and how to seek professional support. Involving birth partners and those who will be closely involved in supporting the parents in the early days in this awareness is important for whole family's well-being and encourages active involvement and self-confidence in co-parenting.

Demographics vary greatly from family to family and region to region, and the expectation of involvement and support from the wider family and surrounding community can have a big impact on the availability of support in the early days. It would be beneficial to encourage parents to consider in advance where they may be able to afford to hire help or draw support from willing helpers, whether that's practical support with the babies, meals for parents, housework and laundry or care of pets or older children.
Whether or not parents have invested time and money in gathering knowledge, researching and preparing for parenthood, once their babies are born and discharged from hospital the abstract and theoretical very quickly become reality. While all parents may feel overwhelmed as they adjust to life at home with a new baby, PoMs have an even greater adjustment to life as a family. While most parents will undoubtedly be happy and relieved to be at home with healthy babies, they may carry trauma from the experience of their path to conception, pregnancy and birth. Parents may have experienced the neonatal loss of one or more babies or be parenting a baby with special or high-dependency needs.
I found it really hard to say out loud that I was finding caring for my baby challenging as it immediately raised feelings of guilt. I should have been caring for two babies and would have given anything for my other twin to have survived and things to feel even more overwhelming. I felt by voicing my struggles it might mean or be perceived that I didn't wish every second that he was there too. It was extremely confusing and I found very few people I felt brave enough to confide my feelings in. It accounted for a very difficult time for me emotionally.
The intense early weeks of caring for a newborn, or for two or more, may allow little time to process those emotions or in the case of loss, may serve as a constant reminder of what parents are missing. Parents of multiples are more likely to report low confidence and feeling overwhelmed.
Breastfeeding Two or More Babies
One of the most intense and emotive areas postnatally surrounds breastfeeding. Women need proper information about the value of breastfeeding twins or more, for both mother and babies, and about the risks of choosing not to breastfeed, in order to make an informed choice. Too often the perception or the societal bias is that breastfeeding multiples is not possible or is unrealistic, which undermines maternal confidence. In reality, breastfeeding multiples can be enormously challenging. A mother of newborn twins is likely to offer 16-24 feeds every 24 hours, and that number increases with each additional baby. Success is often let down by unrealistic expectations coupled with a lack of effective education and support.
Access to prenatal and early postnatal specialised support from a lactation consultant or breastfeeding counsellor (clinical background or peer based) confident in supporting mothers of multiples is a crucial provision for all families wishing to breastfeed their multiples. Parents of multiples are more likely to have preterm and/or low-birthweight babies, which can have significant impact on feeding efficacy and the early success of exclusive breastfeeding. Effective education and support in hand expressing, providing access to and explaining how and when to use a breast pump, giving practical help in tandem or individually positioning babies at the breast, explaining how to safely store milk and how to offer supplementary feeds where necessary, without potentially compromising breastfeeding goals, and mixed feeding all play an enormous role in success rates and maternal confidence. This in turn has enormous influence on emotional well-being in mothers wishing to breastfeed their babies. Lack of confidence, concern around adequate infant weight gain, worrying about milk supply and the challenge of transitioning from bottle to breast are standout challenges to maternal mental health for breastfeeding mothers of multiples in the early postnatal period. Acknowledging maternal feelings and goals and offering unbiased support, reassurance and encouragement are highly valued by mothers.
A published study11 reported that women commented more positively on support from breastfeeding counsellors than on support from healthcare professionals, and they showed an appreciation of the counsellors’ knowledge, experience, reassurance, non-judgemental approach and preparation to listen; another study found higher levels of breastfeeding knowledge and positive attitudes in peer supporters compared to student midwives.12 This may be attributed to the fact that many peer counselling training programmes have a requirement that counsellors have personal experience of breastfeeding. Expanding peer counselling training within multiple birth support initiatives and improving accessibility to peer counsellors both in and out of clinical settings would benefit parents and alleviate pressures on healthcare services. We also know that breastfeeding success is greater when co-parents are supportive, so including them within the education and support framework is important (see Vignette 5).
Parents who choose not to breastfeed their babies also require support and clarity around safely preparing and offering feeds. Since the introduction of formula preparation machines and hands-free feeding pillows and aids a lack remains of clear knowledge and guidance on safe preparation and feeding practices. Parents are naturally inclined towards streamlining and efficiency when parenting multiples given the additional demands on their time. Understanding parental choices without exerting judgement while supporting safe practice is important in not undermining parental confidence while ensuring the well-being of their babies.
Vignette 5
This is more than a beautiful photo capturing a precious moment with my babies. It embodies everything I wanted motherhood to be and everything I worked hard to achieve as a single parent: the ability to give life to new humans, to feed them with my own body and to watch them grow and thrive. But this moment would never have happened without the help of an amazing breastfeeding counsellor and doula. She knew I didn't get the support I needed post partum from the hospital, their lactation team or our paediatrician. She understood that I was heartbroken, frustrated and lost. She helped me to latch and position my twins for the first time and then captured the moment in an image that will be a part of my heart forever. The care and attention I received when pregnant with my twins was intense. The number of doctors' visits and scans makes you feel deeply cared for and paid attention to. But the instant I gave birth I felt this virtually vanished. Post-partum care is very little about you anymore, other than the physical basics, and all about the babies, but as a new mother you still need care too. I felt tired, often lost, overwhelmed and sleep deprived. I felt I, like many multiples mothers I have spoken to, was left to slip through the cracks by the professionals and discouraged from breastfeeding as 'too hard'. This peer supporter and this moment shows that with time, patience and the right support everything is possible
To be accompanied by Figure 28.7.

Figure 28.7 Simultaneous
Breast Feeding
Safe Sleep with Multiples
Not many families have the luxury of space to easily accommodate two, three or more cots within their bedroom for the recommended six months of rooming in. The Lullaby Trust has one of the most comprehensive guides for parents of multiples and acknowledges the challenges associated with adhering strictly to all recommended guidelines; however, the guidelines are still very much directed towards singletons.13 The realities of parenting newborn multiples mean co-sleeping is often key to precious additional sleep. However, the majority of multiples fall into the low birthweight and/or preterm category, for whom it is contraindicated, and there is a demographic of parents more likely to have anxiety relating to their babies' well-being or vulnerable child syndrome. Research into safe sleeping practices that accommodate the realities of multiple parenting is important both from a safety aspect and to better support parent post-partum adjustment, confidence and well-being.
Encouraging Postnatal Support Frameworks and Fostering Self-Confidence
It is not always an easy adjustment to go from the intensity and frequency of antenatal healthcare appointments, possibly preceded by a fertility journey and then followed with a NICU journey, and then transition to life at home without the same routine level of contact and reassurance from healthcare experts. Helping parents to understand that it may be a period of adjustment and guiding them on where they can reach out for help is important in mitigating feelings of abandonment, uncertainty, self-doubt and isolation in their new, parent-led dynamic.
Given the significantly increased time and financial constraints of multiple parenting it is not uncommon to see parents place less emphasis on their own well-being and they are unlikely to be motivated or feel able to seek help, particularly during the early months, outside of routine or necessary appointments for their babies. In these settings it would be prudent for healthcare providers who are likely to be in contact with parents during pregnancy, through birth, the NICU and into parenthood to consider additional measures they can put in place to offer tangible support or signposting where necessary.
Where it is not possible to offer individual support sessions to families postnatally, alternative methods of support should be considered such as finding collective group support facilitated by a healthcare professional, encouraging parents to be proactive in getting together and exploring further the efficacy of e-consultations, e-counselling, teletherapy or cyber-counselling for mental well-being, lactation and general parenting support. This is particularly pertinent for families recognised as suffering from or vulnerable to PTSD, anxiety and postnatal mood disorder/depression, especially if those families have self-identified and requested support.
Life with Two or More Babies
Within this same context it is important to normalise with empathy the exhaustion of parents caring for two or more babies who may likely have independent sleep and feeding routines, certainly initially. This is where peer support is of undeniable value as it really is hard to comprehend quite how much more challenging multiple parenting can be in terms of sleep deprivation unless you’ve experienced it first-hand. Understanding subtle differentiations that have a big emotional difference is important. For example, since the majority of multiples are likely to be born before 37 weeks and are at increased risk of developmental delays, it may be months of keeping up with the physical and emotional demands of parenting before you get those heart-warming smiles that punctuate the natural take-take character of a newborn. Families who have parented one or more children previously frequently report being surprised by the big differences in parenting twins or more, but also tend to show a greater resolve to ‘just get on with it’, knowing it will eventually get easier.
I underestimated how much more challenging it would be co-parenting twins. With our first child I willingly helped out ad hoc at nights when my partner needed support but with our twins it was clear we needed to work as a team day and night. The unrelenting exhaustion for both of us put a strain on our relationship, our family and work, but I'm proud that we all got through it and I believe it ultimately made us all a stronger, more bonded family for it.
Effective co-parenting may look different for every family and may not be an option for everyone, but it is prudent to discuss and encourage it wherever possible. In turn, the greater toll on both parents’ mental and emotional well-being is important to recognise. Though parenting multiples often comes with challenges, raising multiples brings many joys. Most parents feel incredibly privileged to parent multiples and to observe the growing interaction between their babies as they discover one another and become playmates. Some parents report assuaged negative emotions at leaving their babies or returning to work because the babies have one another for comfort and company, a point that also raises the understandable resentment PoMs may have at having no different parental leave than parents of a singleton. As with all parenting, the challenges of the early months may lessen as others evolve. Parents of multiples have an increased chance of parenting children with moderate or severe developmental delays or dependency needs. Simple family outings can often result in being treated as or perceiving themselves as a nuisance with larger strollers, greater noise volume, extra pairs of hands to fiddle or children to keep an eye on.
Conclusion
There is no better demographic than PoMs themselves from which to gain first-hand knowledge about the mental and emotional considerations that come with parenting multiples. I would encourage you to take the steps outlined at the beginning of this chapter and adopt them into your care: recognise, empathise, signpost and reflect.
References
1. http://icombo.org/wp-content/uploads/2010/11/Declaration-of-Rights.pdf
2. Wenze SJ, Battle CL. Perinatal mental health treatment needs, preferences, and barriers in parents of multiples. J Psychiatr Pract 2018 May;24(3):158-68. https://doi.org/10.1097/ PRA.0000000000000299. PMID: 30015786
3. Wenze SJ, Miers QA, Battle CL. Postpartum mental health care for mothers of multiples: a qualitative study of new mothers' treatment preferences. J Psychiatr Pract. 2020 May;26(3):201- 14. https://doi.org/10.1097/PRA.0000000000000469. PMID: 32421291
4. Wright J, Belanger C, Delude D. The effects of pregnancy complications on the parental adaptation process. J Reprod Infant Psychol 2000;18(1):5-20. https://doi.org/10.1080/ 02646830050001645
5. Whistler J. Are twins always high risk? AIMS J 2011;23(4).
6. Zager R. Glob. libr. women's med. (ISSN: 1756-2228) 2009. https://doi.org/10.3843/ GLOWM.10155
7. Sandall J, Soltani H, Gates S, Shennan A, Devane D. Midwife-led continuity models versus other models of care for childbearing women. Cochrane Database Syst Rev 2016;(4). Art. No.: CD004667. https://doi.org/10.1002/14651858.CD004667.pub5
8. www.bliss.org.uk/news/bliss-releases-new-research-on-mental-health
9. Lai N, Foong S, Foong W, Tan K. Co-bedding in neonatal nursery for promoting growth and neurodevelopment in stable preterm twins. Cochrane Database Syst Rev 2016;(4). Art. No.: CD008313. https://doi.org/10.1002/14651858.CD008313.pub3
10. Choi Y, Bishai D, Minkovitz CS. Multiple births are a risk factor for postpartum maternal depressive symptoms. Pediatrics 2009;123(4):1147-54. https://doi.org/10.1542/peds.2008-1619
11. Graffy J, Taylor J. What information, advice and support do women want with breastfeeding? Birth 2005;32(3):179-86. https://doi.org/10.1111/j.0730-7659.2005.00367.x
12. Darwent KL, Kempenaar LE. A comparison of breastfeeding women's, peer supporters' and student midwives' breastfeeding knowledge and attitudes. Nurse Educ Pract 2014;14(3):319-25. https://doi.org/10.1016/j.nepr.2014.02.004. Epub 2014 Feb 19.
13. www.lullabytrust.org.uk/safer-sleep-advice/twins