I FAMILY PLANNING ^273 ^292 ^337 ^381
The United States has the highest rate of unintended pregnancy in the developed world; approximately one half of all pregnancies are unintended. Although the percentage of unintended pregnancies is highest in adolescents and women older than 40 years, approximately one third of pregnancies in the middle reproductive years also are unintended.
Couples using no contraceptive method account for approximately one half of unintended pregnancies, and the other half are the result of contraceptive failures.Methods of contraception that require the couple to take little or no action after the placement or procedure, “non-user-dependent methods,” are the most effective methods of contraception. These include implants and intrauterine devices. Methods that require contraception linked to the coital act are among the less effective methods of contraception (see Table 3-8). Because one half of unintended pregnancies occur as the result of contraceptive failures, encouraging appropriate couples to consider using methods that are more effective has the potential to decrease unintended pregnancies.
Unintended pregnancies result in tremendous individual and societal consequences, which include family upheaval, nonattainment of educational goals, and financial burdens. Two thirds of American women of reproductive age wish to avoid or postpone pregnancy. When discussing contraception with these women, clinicians should tailor counseling to the individual patient’s lifestyle and needs, in addition to outlining the benefits and risks of different types of contraceptive methods. Counseling also should focus on information that may help decrease contraceptive failures for the method the patient chooses.
Initial Evaluation
The initial visit for family planning, which can be combined with a general preventive care visit, provides an opportunity to assess the health status of
Table 3-8.
Percentage of U.S. Women Who Experience an Unintended Pregnancy During the First Year of Typical Use and the First Year of Perfect Use of Contraception and the Percentage of Women Who Continue Use at the End of 1 Year ^| Method | % of Women Who Experience an Unintended Pregnancy Within the First Year of Use | % of Women Who Continue Use at 1 Year* | |
| Typical Use1 | Perfect Use1 | ||
| No method5 | 85 | 85 | |
| Spermicides∣∣ | 28 | 18 | 42 |
| Fertility awareness-based methods | 24 | 47 | |
| Standard Days method1 | 5 | ||
| TwoDay method1 | 4 | ||
| Ovulation method1 | 3 | ||
| Symptothermal method1 | 0.4 | ||
| Withdrawal | 22 | 4 | 46 |
| Sponge | 36 | ||
| Parous women | 24 | 20 | |
| Nulliparous women Condom# | 12 | 9 | |
| Female | 21 | 5 | 41 |
| Male | 18 | 2 | 43 |
| Diaphragm** | bgcolor=white>126 | 57 | |
| Combined pill and progestin-only pill11 | 9 | 0.3 | 67 |
| Patch | 9 | 0.3 | 67 |
| Ring | 9 | 0.3 | 67 |
| Medroxyprogesterone | 6 | 0.2 | 56 |
| Intrauterine contraceptive devices | |||
| Copper | 0.8 | 0.6 | 78 |
| Levonorgestrel | 0.2 | 0.2 | 80 |
| Etonogestrel | 0.05 | 0.05 | 84 |
| Female sterilization | 0.5 | 0.5 | 100 |
| Male sterilization | 0.15 | 0.10 | |
(continued)
Table 3-8.
Percentage of U.S. Women Who Experience an Unintended Pregnancy During the First Year of Typical Use and the First Year of Perfect Use of Contraception and the Percentage of Women Who Continue Use at the End of 1 Year (continued)*Among typical couples who initiate use of a method (not necessarily for the first time), the percentage who experience an accidental pregnancy during the first year if they do not stop use for any reason other than pregnancy. Estimates of the probability of pregnancy during the first year of typical use for spermicides and the diaphragm are taken from the 1995 National Survey of Family Growth corrected for underreporting of abortion; estimates for fertility awareness-based methods, withdrawal, the male condom, the pill, and medroxyprogesterone are taken from the 1995 and 2002 National Survey of Family Growth corrected for underreporting of abortion.
!Among couples who initiate use of a method (not necessarily for the first time) and who use it perfectly (ie, consistently and correctly), the percentage who experience an accidental pregnancy during the first year if they do not stop use for any other reason.
tAmong couples attempting to avoid pregnancy, the percentage who continue to use a method for 1 year.
§The percentage of women who become pregnant in the typical use and perfect use columns are based on data from populations where contraception is not used and from women who cease using contraception in order to become pregnant. Among such populations, approximately 89% become pregnant within 1 year. This estimate was lowered slightly (to 85%) to represent the percentage who would become pregnant within 1 year among women now relying on reversible methods of contraception if they abandoned contraception altogether.
∣∣Foams, creams, gels, vaginal suppositories, and vaginal film.
^The Ovulation and TwoDay methods are based on evaluation of cervical mucus. The Standard Days method avoids intercourse on cycle days 8 through 19.
The Symptothermal method is a double-check method based on evaluation of cervical mucus to determine the first fertile day and evaluation of cervical mucus and temperature to determine the last fertile day. flWithout spermicides.**With spermicidal cream or jelly.
!!These are weighted averages of estimates derived from the 1995 and 2002 National Surveys of Family Growth. The National Survey of Family Growth does not ask for brand of pill; thus, combined and progestin-only pills cannot be distinguished. However, because use of the combined pill is far more common than use of the progestin-only pill, the results from the National Survey of Family Growth overwhelmingly reflect typical use of combined pills. The efficacy of progestin-only pills may be lower than that for combined pills because progestin-only pills are probably less forgiving of nonadherence to the dosing schedule. Whether the progestin-only pill also is less effective during perfect use is unknown.
Modified with permission from Trussell J. Contraceptive efficacy. In: Hatcher RA, Trussell J, Nelson AL, Cates WJ, Kowal D,Policar MS, editors. Contraceptive technology. 20th revised ed. New York (NY): Ardent Media; 2011. p. 779-863.
the woman and to enlist her involvement in overall health maintenance. Clinicians should encourage women to formulate a reproductive health plan and should discuss it in a nondirective way at each subsequent visit. Such a plan would address the individual’s or couple’s desire for a child or children (or desire not to have children); the optimal number, spacing, and timing of children in the family; and age-related changes in fertility. Because a patient’s plans may change over time, creating a reproductive health plan requires an ongoing, conscientious assessment of the desirability of a future pregnancy; determination of steps that need to be taken either to prevent or to plan for and optimize a pregnancy; and evaluation of current health status.
Contraceptive and Sexual History
For all women of reproductive age, a contraceptive and sexual history should be obtained to assess the need for contraceptive services.
The clinician should obtain a general medical and gynecologic history for women who request contraception. The Centers for Disease Control and Prevention (CDC) have published the U.S. Medical Eligibility Criteria for Contraceptive Use, 2010 (U.S. MEC), which is extremely helpful in identifying contraindications to various methods. The full recommendations are available at www.cdc.gov/mmwr/pdf/rr/rr5904.pdf, and a summary chart can be accessed at www.cdc.gov/reproductivehealth/ UnintendedPregnancy/Docs/USMEC-Color-62012.docx. Updates and supporting information for clinicians are available at www.cdc.gov/reproduc tivehealth/UnintendedPregnancy/USMEC.htm.Screening for Reproductive and Sexual Coercion and Intimate Partner Violence
Reproductive coercion involves behavior that interferes with contraceptive use or pregnancy. The most common forms of reproductive coercion include sabotage of contraceptive methods, pregnancy coercion, and pregnancy pressure. Sexual coercion includes a range of behavior that a partner may use to pressure or coerce a person to have sex without using physical force. Examples include repeatedly pressuring a partner to have sex, threatening to end a relationship if the person does not have sex, forcing sex without a condom or not allowing other prophylaxis use, intentionally exposing a partner to a sexually transmitted infection (STI), including human immunodeficiency virus (HIV), or threatening retaliation if notified of a positive STI test result.
Because of the known link between reproductive health and violence, women’s health care providers should screen women and adolescent girls for intimate partner violence and reproductive and sexual coercion at periodic intervals and include reproductive and sexual coercion and intimate partner violence as part of the differential diagnosis when patients are seen for pregnancy or STI testing, emergency contraception, or with unintended pregnancies. Some examples of screening questions include the following:
• Has your partner ever forced you to do something sexually that you did not want to do or refused your request to use condoms?
• Has your partner ever tried to get you pregnant when you did not want to be pregnant?
• Are you worried your partner will hurt you if you do not do what he wants with the pregnancy?
If a patient responds affirmatively to screening questions, the health care provider should validate her experience and commend her for discussing and evaluating her health and relationships.
She should be reassured that the situation is not her fault and further assessment of her safety should be elicited and discreet contraceptive options reviewed. Interventions include education on the effect of reproductive and sexual coercion and intimate partner violence on patients’ health and choices, counseling on harm-reduction strategies, and prevention of unintended pregnancies by providing discreet and confidential methods of contraception, such as intrauterine devices (IUDs), emergency contraception, depot medroxyprogesterone acetate injections, and etonogestrel implants. For additional support, patients may be offered hotline numbers, use of the office phone to access suggested care, and referral to a domestic violence advocate for additional resources (see also the “Abuse” section later in Part 3).Physical Examination and Laboratory Tests
As a companion document to the U.S. MEC, the CDC has published the U.S. Selected Practice Recommendations for Contraceptive Use, 2013 (U.S. SPR). According to the U.S. SPR, with few exceptions, examinations and tests are not needed before initiating contraceptive methods in women who are presumed to be healthy because these assessments do not contribute substantially to safe and effective use of contraceptive methods. Examinations or tests that are not deemed necessary for safe and effective contraceptive use might be appropriate for good preventive health care or for diagnosing or assessing suspected medical conditions. For example, weight measurement or body mass index calculations are not needed to determine medical eligibility for any methods of contraception. Measuring weight and calculating body mass index at baseline might be helpful, however, for monitoring any changes and counseling women using hormonal methods or IUDs who might be concerned about weight change perceived to be associated with their contraceptive method. See “Methods” later in this section for specific examinations or tests that are recommended before initiating certain types of contraception.
Counseling on Methods
In the absence of contraindications, patient choice should be the principal factor in prescribing one method of contraception over another. To help the patient make this choice, the health care provider should do the following:
• Fully explain potential adverse effects and risks for all methods; in a healthy woman, death rates from pregnancy are higher than from any contraceptive method.
• Discuss efficacy and failure rates (see Table 3-8). Couples deciding among methods should be encouraged to choose a method they are likely to use effectively. Methods that are less user-dependent often fit this description.
• Describe ease of use and noncontraceptive benefits.
• Explain the use of barrier methods to reduce the risk of STI transmission when nonbarrier contraceptive methods are used (see also the “Sexually Transmitted Infections” section later in Part 3).
A special warning regarding the use of condoms and diaphragms should be given to patients with latex sensitivity. Women, especially, are at high risk of reaction because of mucous membrane contact with these devices.
Nonlatex male condoms and diaphragms are available. The second- generation female condom is nonlatex, being made of nitrile; this condom has the same instructions and has shown similar safety and efficacy to previously marketed polyurethane products. Provide information on when and how to use emergency contraception. To maximize the effectiveness of treatment, women should be able to obtain emergency contraception quickly when the need arises (see also “Emergency Contraception” later in this section).
Periodic Reassessment ^354
The U.S. SPR recommendations address when routine follow-up is recommended for safe and effective continued use of contraception for healthy women. The recommendations refer to general situations and might vary for different users and different situations. Specific populations that might benefit from more frequent follow-up visits include adolescents, those with certain medical conditions or characteristics, and those with multiple medical conditions.
With the exception of hysteroscopic sterilization and vasectomy, routine follow-up visits are not needed for any contraceptive method. Clinicians should advise a woman to return at any time to discuss side effects or other problems, if she wants to change the method being used, and when it is time to remove or replace the method. At other routine visits, health care providers who see contraceptive users should assess the woman’s satisfaction with her contraceptive method and whether she has any concerns about method use. The health care provider should assess any changes in health status, including medications that would change the appropriateness of the method for safe and effective use on the basis of the U.S. MEC (eg, category 3 and 4 conditions and characteristics). Specific recommendations for users of IUDs and combined hormonal contraceptives are included later in this section.
Rates of pregnancy and discontinuation are highest in the first few months after the initiation of a contraceptive method. A visit in the first few months to troubleshoot problems can be considered to help avoid discontinuation or facilitate transfer to another method. Similarly, a phone call from an office nurse after contraception initiation also may be appropriate. High rates of discontinuation may be reduced with good follow-up and the provision of a convenient opportunity to have the patient’s questions about the contraceptive method answered. Once the patient has become comfortable with her method of contraception, annual follow-up examinations should be conducted in accordance with age-specific recommendations for asymptomatic women.
Special Populations
Older Contraceptive Users
Prevention of unintended pregnancy assumes increasing importance for many women during the perimenopausal years. Pregnancies in women over 40 years of age are often unintended. It may be difficult to know when it is safe to change from hormonal contraception to postmenopausal hormone treatment. Assessment of follicle-stimulating hormone levels to determine when older contraceptive users have become menopausal is expensive and may be misleading. Until a well-validated tool to confirm menopause is available, it is appropriate for healthy, nonsmoking women doing well on a combined hormonal contraceptive to continue contraceptive use until age 50-55 years. The likelihood that a woman has reached menopausal status by age 55 years is 85%.
Women With Coexisting Medical Conditions
Clinicians must balance benefits and risks when contemplating appropriate contraception in women with coexisting medical conditions. Avoidance of unintended pregnancy is particularly important, given the risks of pregnancy to the woman and her fetus, for some medical conditions. Some conditions or medications may alter contraceptive effectiveness. The U.S. MEC (www.cdc.gov/reproductivehealth/unintendedpregnancy/usmec. htm) is an excellent resource that can help guide practitioners in regard to contraception for patients with coexisting medical conditions. The U.S. MEC uses four categories to aid clinicians in their decisions regarding the use of each contraceptive method for a patient with a given characteristic or medical condition (see Box 3-15).
Box 3-15. Categories of Medical Eligibility Criteria for Contraceptive Use ^
1 = A condition for which there is no restriction for the use of the contracep
tive method.
2 = A condition for which the advantages of using the method generally out
weigh the theoretical or proven risks.
3 = A condition for which the theoretical or proven risks usually outweigh the
advantages of using the method.
4 = A condition that represents an unacceptable health risk if the contraceptive
method is used.
Reprinted from U.S. Medical Eligibility Criteria for Contraceptive Use, 2010. Centers for Disease Control and Prevention. MMWR Recomm Rep 2010;59(RR-4):1-86: adapted from the World Health Organization. Medical eligibility criteria for contraceptive use. 4th ed. Geneva: WHO; 2009. Available at: http://whqlibdoc.who.int/publica- tions/2010/9789241563888_eng.pdf. Retrieved June 7, 2013.
Methods ^348
Sterilization
A woman who feels that her family is complete should be informed about male and female sterilization options as well as IUDs and contraceptive implants. Intrauterine devices should be strongly considered because their efficacy is similar to that of surgical sterilization with substantially lower risks associated with insertion as compared with surgery for sterilization. The advantages of vasectomy include the fact that it is a less invasive and less expensive procedure than tubal sterilization. Vasectomy also can be performed with local anesthesia.
Female sterilization can be performed at any time when a woman is not pregnant (interval sterilization) or after pregnancy (postpartum sterilization). The choice and timing of sterilization are affected by individual patient preference, medical assessment of acute risk, access to services, and insurance coverage. The timing of the procedure influences the surgical approach and the method of tubal occlusion or ligation. Hysteroscopic techniques are not indicated for postpartum sterilization or sterilization after an abortion.
The laparoscopic approach is used for interval and postabortal tubal ligation procedures. In the United States, minilaparotomy generally is reserved for postpartum procedures and rarely considered for patients at high risk of complications associated with laparoscopic procedures.
If a patient is considering surgical sterilization, she should be told that the procedure is intended to be permanent, that there is a small chance of failure, and that the success of any subsequent attempts at surgical restoration of fertility is uncertain. Although most women do not regret their decision to have tubal sterilization, women aged 30 years or younger at the time of sterilization and those who have had a break-up or divorce are more likely to express sterilization regret. Patients who undergo hys- teroscopic sterilization should have hysterosalpingography performed at 3 months to ensure tubal occlusion. They should be instructed to use another method of contraception until hysterosalpingography confirms bilateral tubal occlusion. Similarly, men who undergo vasectomy need to return for a semen analysis 8-16 weeks after the procedure to ensure it was successful. Men (and their female partners) should be advised to use additional contraceptive protection or abstain from intercourse until after the postvasectomy semen analysis confirms the success of the procedure.
Physicians need to be aware of applicable federal and state requirements that relate to consent, age restrictions, and reimbursement for surgical sterilization (see also the “Ethical Issues” section in Part 1). If the physician has any question about the patient’s capacity to authorize the procedure, he or she should seek consultation to ensure that legal requirements are met.
Intrauterine Devices
Intrauterine devices are used at lower rates by U.S. women compared with women in other nations. The National Center for Health Statistics reports that from 2006 to 2010, only 5.6% of U.S. women used an IUD as contraception. The effectiveness of IUDs is similar to that of female sterilization.
According to the U.S. MEC, the only absolute contraindications (ie, U.S. MEC 4 rating) to IUD use are as follows:
• Distorted uterine cavity
• Persistent or malignant gestational trophoblastic disease
• Current breast cancer (levonorgestrel-releasing intrauterine system [levonorgestrel IUD] only)
• Immediately after septic abortion
• Puerperal sepsis
In addition, whereas continuation of IUD use may be acceptable, IUD use should not be initiated in women with the following:
• Current pelvic inflammatory disease
• Current purulent cervicitis, chlamydial infection, or gonorrhea
• Pelvic tuberculosis
• Cervical or endometrial cancer awaiting treatment
Nulliparous and multiparous women who desire long-term reversible contraception are good candidates for IUD use. The first levonorgestrel IUD that was approved by the U.S. Food and Drug Administration is recommended for women who have had at least one child and should be replaced in 5 years. Although the 5-year levonorgestrel IUD is not approved for nulliparous women, it has a U.S. MEC 2 rating in nulliparous women because the advantages generally outweigh the risks. The recently approved 3-year levonorgestrel IUD, which postdates the publication of the U.S. MEC, is not restricted to use in parous women. The copper IUD is labeled for 10 years of use. Data support the safety of IUD use in adolescents.
Previous ectopic pregnancy is not a contraindication to IUD use. Pelvic inflammatory disease (PID) complicating IUD insertion is uncommon, and the risk of PID decreases to the baseline risk after the first 20 days following insertion. Progestin-containing IUDs have noncontraceptive benefits, including decreased menstrual flow. However, only the 5-year levonorgestrel IUD is labeled as an appropriate treatment for heavy menstrual bleeding in women who choose an IUD for contraception.
According to the U.S. SPR, few examinations or tests are needed before initiation of an IUD by healthy women. Bimanual examination and cervical inspection are necessary before IUD insertion. Recommendations should be followed for routine screening for chlamydial infection and gonorrhea (see also the “Sexually Transmitted Infections” section later in Part 3). Women who have not received indicated screening can be screened at the time of IUD insertion; the insertion should not be delayed while awaiting results. Women who have a very high likelihood of STI exposure (eg, those with a currently infected partner) generally should not undergo IUD insertion until appropriate testing and treatment occur.
For new contraceptive users and those switching from another method, either the copper IUD or levonorgestrel IUD can be inserted at any time if it is reasonably certain that the woman is not pregnant (see Box 3-16). Waiting for the next menstrual period is unnecessary. A back-up method of contraception is not needed if the levonorgestrel IUD is inserted within the first 7 days of the start of menstrual bleeding or at the time of a surgical abortion. Otherwise, the patient needs to abstain from sexual intercourse or use additional contraceptive protection for the next 7 days. Guidance on switching from the copper IUD to the levonorgestrel IUD is available in the U.S. SPR (see Bibliography). No additional contraceptive protection is needed after insertion of the copper IUD.
The copper IUD may be inserted immediately (up to 7 days) after a first-trimester or second-trimester spontaneous abortion or induced abortion. Labeling states that the 5-year and 3-year levonorgestrel IUDs may be inserted immediately after a first-trimester abortion, but insertion after a second-trimester abortion should be delayed until uterine involution is complete (for the 5-year IUD) or for a minimum of 6 weeks or until the uterus is fully involuted (for the 3-year IUD). Immediate insertion of the 5-year levonorgestrel IUD is classified as U.S. MEC 1 after a first-trimester abortion and as U.S. MEC 2 after a second-trimester abortion because of a higher risk of expulsion after a second-trimester abortion. Although there may be a higher risk of expulsions with postabortion IUD placements, studies have shown that many patients do not return for IUD placement at later times.
The U.S. SPR indicates that no routine follow-up visit is required after IUD insertion. General considerations for ongoing contraceptive management are addressed earlier in this section (see “Periodic Reassessment”). At other routine visits, health care providers who treat IUD users should consider performing an examination to check for the presence of the IUD strings. Management of common problems that may occur with IUD use (eg, bleeding irregularities, amenorrhea, PID management in an IUD user) is found in the U.S. SPR (see Bibliography).
Box 3-16. How to Be Reasonably Certain That a Woman Is Not Pregnant ^
A health care provider can be reasonably certain that a woman is not pregnant if she has no symptoms or signs of pregnancy and meets any one of the following criteria:
• Has started her normal menses within the past 7 days
• Has not had sexual intercourse since the start of her last normal menses
• Has been correctly and consistently using a reliable method of contraception
• Has had a spontaneous abortion or induced abortion within the past 7 days
• Has given birth within the past 4 weeks
• Is fully or nearly fully breastfeeding (exclusively breastfeeding or the vast majority [85% or more] of feeds are breastfeeds)[***], amenorrheic, and less than 6 months postpartum
For new contraceptive users and those switching from another method, the contraceptive implant can be inserted at any time if it is reasonably certain that the woman is not pregnant (see Box 3-16). Waiting for the next menstrual period is unnecessary. Contraceptive implant insertion immediately (up to 7 days) after a first-trimester or second-trimester spontaneous abortion or induced abortion is classified as U.S. MEC 1, but this recommendation is based on studies of a levonorgestrel implant system no longer marketed in the United States. If the implant is placed within 5 days of the start of menstrual bleeding or at the time of a surgical abortion, no additional contraceptive protection is needed. Otherwise, the woman needs to abstain from sexual intercourse or use additional contraceptive protection for the next 7 days. Guidance on switching from an IUD to the contraceptive implant is provided in the U.S. SPR (see Bibliography).
The U.S. SPR indicates that no routine follow-up visit is required after contraceptive implant insertion. General considerations for ongoing contraceptive management are addressed earlier in this section (see “Periodic Reassessment”). Management of common problems that may occur with implant use (eg, bleeding irregularities, amenorrhea) is found in the U.S. SPR.
Injectable Contraception
There are two injectable contraceptive formulations currently available in the United States: 1) depot medroxyprogesterone acetate (DMPA) 150 mg/ mL, which is given every 13 weeks intramuscularly and is by far the most common formulation, and 2) DMPA 104 mg/0.65 mL, which is given subcutaneously every 13 weeks. Repeat injections can be given early when necessary. According to the U.S. SPR, repeat injections can be given up to 15 weeks after the last injection without requiring additional contraceptive protection. The typical-use failure rate over 1 year of use is approximately 6%, which is lower than the typical-use failure rate of approximately 9% for combined oral contraceptives, the progestin-only pill, or the contraceptive patch or contraceptive ring (Table 3-8). Because injectable contraception requires minimal patient action, it is often favored by women for whom adherence to other methods is a problem. Injectable contraception use is contraindicated in women with current breast cancer (U.S. MEC 4).
For new contraceptive users and those switching from another method, the first DMPA injection can be given at any time if it is reasonably certain that the woman is not pregnant (see Box 3-16). Waiting for the next menstrual period is unnecessary. The first DMPA injection can be given immediately (up to 7 days) after a spontaneous or induced abortion. If the first DMPA injection is given within 7 days of the start of menstrual bleeding or at the time of a surgical abortion, no additional contraceptive protection is needed. Otherwise, the woman needs to abstain from sexual intercourse or use additional contraceptive protection for the next 7 days. Guidance on switching from an IUD to combined hormonal contraception injection is available in the U.S. SPR (see Bibliography).
The U.S. SPR indicates that no routine follow-up visit is required after DMPA injection. General considerations for ongoing contraceptive management are addressed earlier in this section (see “Periodic Reassessment”). Management of common problems that may occur with the injection (eg, bleeding irregularities, amenorrhea) is found in the U.S. SPR.
The use of contraceptive dosages of DMPA suppresses ovarian production of estradiol. Although DMPA is associated with bone mineral density (BMD) loss during use, current evidence suggests that partial or full recovery occurs after discontinuation of use. Concerns regarding the effect of DMPA on bone mineral density should neither prevent practitioners from prescribing nor cause them to limit its use to 2 consecutive years, despite the “black box” package labeling cautioning against prolonged use. Practitioners should not perform BMD monitoring solely in response to DMPA use, because any observed short-term loss of BMD associated with DMPA use may be recovered and is unlikely to place a woman at risk of fracture either during use or in later years. Caution is advised in the use of DMPA for women with mobility disorders who are not weight bearing.
Weight gain is a problem that may be seen in women using DMPA, although it is critical to note that it is not consistent in all women and may vary by age, ethnicity, and perhaps baseline dietary practices. A systematic review of a limited body of evidence suggests that early weight gain may predict future weight gain. Therefore, measuring weight and calculating body mass index at baseline might be helpful for monitoring any changes and counseling women receiving DMPA injections who might be concerned about weight change perceived to be associated with their contraceptive method. According to the U.S. MEC, obesity is not a contraindication for DMPA use.
Combined Hormonal Contraceptives: Oral, Patches, and Rings Combined hormonal contraceptives that contain an estrogen and a progestin are available in oral contraceptive pills, the contraceptive patch, and the contraceptive ring. Because all have an estrogen component, a contraindication to estrogen use precludes the use of any of these methods. Combined hormonal contraceptives should be prescribed with caution, if ever, to women who are older than 35 years and are smokers (ie, U.S. MEC
3 rating for those who smoke fewer than 15 cigarettes a day and a U.S. MEC
4 rating for those who smoke more than 15 cigarettes a day).
According to the U.S. SPR, few examinations or tests are needed before initiation of combined hormonal contraceptives by healthy women. Blood pressure should be measured before initiation of combined hormonal contraceptives. In cases in which access to health care might be limited, the blood pressure measurement can be obtained by the woman in a nonclini- cal setting (eg, pharmacy or fire station) and self-reported to the clinician.
According to the U.S. SPR, for new contraceptive users and those switching from another method, combination hormonal contraceptives (pills, patch, and ring) can be initiated at any time if it is reasonably certain that a woman is not pregnant (see Box 3-16). Waiting for the next menstrual period is unnecessary. Combined hormonal contraceptives can be started immediately (up to 7 days) after a first-trimester or second-trimester spontaneous abortion or induced abortion. If combined hormonal contraceptives are started within 5 days of the start of menstrual bleeding or at the time of a surgical abortion, no additional contraceptive protection is needed. Otherwise, the woman needs to abstain from sexual intercourse or use additional contraceptive protection for the next 7 days. Guidance on switching from an IUD to combined hormonal contraception is provided in the U.S. SPR (see Bibliography).
The U.S. SPR indicates that no routine follow-up visit is required after initiation of combined hormonal contraception. General considerations for ongoing contraceptive management are addressed earlier in this section (see “Periodic Reassessment”). At other routine visits, health care providers who treat users of combined hormonal contraception should assess blood pressure or, if access to health care is limited, request self-reports of blood pressure readings from patients. Management recommendations for common problems that may occur with use of combined hormonal contraceptives (eg, unscheduled bleeding, vomiting, or severe diarrhea while using the method) are found in the U.S. SPR (see Bibliography).
Oral Contraceptives
The U.S. Food and Drug Administration considers generic and brand name oral contraceptive products to be clinically equivalent and interchangeable. The College supports patient or clinician requests for branded oral contraceptives or continuation of the same generic or branded oral contraceptives if the request is based on clinical experience or concerns regarding packaging or adherence, or if the branded product is considered a better choice for that individual patient.
Although some data have suggested that use of drospirenone-containing pills has a higher risk of venous thromboembolism, this risk is still very low and is much lower than the risk of venous thromboembolism during pregnancy and the immediate postpartum period. Decisions regarding choice of oral contraceptive should be left to clinicians and their patients, taking into account the possible minimally increased risk of venous thromboembolism, patient preference, and the available alternatives. When prescribing any oral contraceptive, clinicians should consider a woman’s risk factors for venous thromboembolism and refer to the U.S. MEC.
Product labeling and protocols developed by various organizations may differ in the information they provide on how to handle a missed dose of a contraceptive pill. Often, patients missing several doses will have unscheduled or breakthrough bleeding, which may serve as an adherence reminder and an opportunity to reevaluate contraceptive method choice. The protocol for missed or late pills developed for the U.S. SPR is detailed in Box 3-17. Package labeling also makes recommendations depending on the package week and number of doses missed.
Missed doses are very common for any prescription product. Practitioners can help patients with daily adherence by linking the taking of
Box 3-17. Recommended Actions After Late or Missed Combined Oral Contraceptives ^
If one hormonal pill is taken late (less than 24 hours since a pill should have been taken) or missed (24 hours to less than 48 hours since a piil should have been taken):
• Take the late or missed pill as soon as possible.
• Continue taking the remaining pills at the usual time (even if it means taking two pills on the same day).
• No additional contraceptive protection is needed.
• Emergency contraception is not usually needed but can be considered if hormonal pills were missed earlier in the cycle or in the last week of the previous cycle.
If two or more consecutive hormonal pills have been missed (48 hours or longer since a pill should have been taken):
• Take the most recent missed pill as soon as possible. (Any other missed pills should be discarded.)
• Continue taking the remaining pills at the usual time (even if it means taking two pills on the same day).
• Use back-up contraception (eg, condoms) or avoid sexual intercourse until hormonal pills have been taken for 7 consecutive days.
• If the pills were missed in the last week of hormonal pills (eg, days 15-21 for 28-day pill packs):
— Omit the hormone-free interval by finishing the hormonal pills in the current pack and starting a new pack the next day.
— If unable to start a new pack immediately, use back-up contraception (eg, condoms) or avoid sexual intercourse until hormonal pills from a new pack have been taken for 7 consecutive days.
• Emergency contraception should be considered if hormonal pills were missed during the first week and unprotected sexual intercourse occurred in the previous 5 days.
• Emergency contraception may also be considered at other times as appropriate.
Reprinted from U.S. Selected Practice Recommendations for Contraceptive Use, 2013: adapted from the World Health Organization selected practice recommendations for contraceptive use, 2nd edition. Division of Reproductive Health, National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention. MMWR Recomm Rep 2013;62:1-60. the product to a daily activity, such as tooth brushing or the morning cup of coffee, and the pills can be stored next to the toothbrush or coffee products as a memory cue. Similar lifestyle reminders can be used for weekly products, for example, setting a weekly confidential reminder on a cellphone to remind oneself that the contraceptive patch needs to be changed. Programs are available that allow patients to set various computer-generated reminders including e-mails, text messages, phone applications, and pop-up cues.
Access and cost issues are common reasons why women either do not use contraception or have gaps in use. Although oral contraceptives are the most widely used reversible method of family planning in the United States, oral contraceptive use is subject to problems with adherence and continuation, often because of logistics or practical issues. The American College of Obstetricians and Gynecologists supports over-the-counter access to oral contraceptives and access to multiple pill packs at one time as potential ways to improve contraceptive access and use and possibly decrease the unintended pregnancy rate. The U.S. SPR recommends that up to a 1-year supply of combined hormonal contraception be prescribed or provided at initial and return visits. The more pill packs given up to 13 cycles, the higher the continuation rates.
Contraceptive Patch and Ring
The contraceptive patch is changed weekly for 3 weeks, followed by 1 week without the patch. It is less effective in women who weigh more than 198 lb. The vaginal contraceptive ring is initially inserted on a day between cycle days 1 and 5 and left in place for 3 weeks, followed by 1 week of no ring use. Management of delayed application or detached contraceptive patches and delayed insertion or reinsertion of the vaginal ring is addressed in Box 3-18.
Currently, only one brand of contraceptive patch and one brand of vaginal contraceptive ring are available in the United States. Both products have informational web sites sponsored by the pharmaceutical makers, which provide patients and clinicians with answers to frequently asked questions. Various scenarios, such as detached patches and what to do if the ring falls out, also are addressed in the patient package insert.
Box 3-18. Recommended Actions After Delayed Application of a Combined Hormonal Patch or Insertion of a Combined Vaginal Ring ^
Box 3-18. Recommended Actions After Delayed Application of a Combined Hormonal Patch or Insertion of a Combined Vaginal Ring (continued)
— emergency contraception also may be considered at other times as appropriate.
contraceptive protection for the next 2 days. Guidance on switching from an IUD to progestin-only pills is provided in the U.S. SPR (see Bibliography).
The U.S. SPR indicates that no routine follow-up visit is required after initiation of progestin-only pills. General considerations for ongoing contraceptive management are addressed earlier in this section (see “Periodic Reassessment”). Progestin-only pills require careful attention to consistent pill-taking at the same time of day (within a 3-hour window) to help ensure contraceptive efficacy. If a pill is taken more than 3 hours late, the pill should be taken as soon as possible, and pills should be taken daily, one each day at the same time each day, even if it means taking two pills on the same day. Back-up contraception or avoidance of sexual intercourse is recommended until pills have been taken correctly, on time, for 2 consecutive days. Emergency contraception should be considered if the woman has had unprotected sexual intercourse. Vomiting and severe diarrhea that occur within 3 hours of taking a progestin-only pill is managed similarly to late pills. Irregular bleeding is seen significantly more in progestin-only pill users than in women who take combined oral contraceptives and is the major reason for discontinuation.
Over-the-Counter Products, Barrier Methods, and Rarely Used Prescription Products
Although over-the-counter methods are less effective than prescription methods, they may be preferred by many couples (see Table 3-8). Contraceptive sponges and spermicides are available without prescription. It is important that the patient understands that the sponge does not protect against STIs. The sponge is effective for contraception immediately after insertion for up to 24 hours after coitus. The sponge must be left in the vagina for at least 6 hours after coitus and must not be left for longer than 30 hours.
Condoms are an excellent choice as a barrier method because they prevent STIs and pregnancy. No examinations or tests are needed before initiating use of condoms or spermicides. However, patients should be aware that although condoms offer the best protection against STIs, they are not the most effective contraceptive method. Diaphragms are similar to condoms in contraceptive effectiveness and have the advantage of being female controlled but the disadvantages of not providing STI protection and requiring a health care provider visit with bimanual examination and a prescription.
Less commonly used nonhormonal prescription methods include a reusable one-size shield that is held by the vaginal wall and a cervical cap that is available in several sizes to allow for coverage of the cervix. Both devices are labeled for use with a spermicide. A bimanual examination and cervical inspection are needed for cervical cap fitting.
Fertility Awareness-Based Methods and Withdrawal
Fertility awareness-based methods of family planning help women to either plan or prevent pregnancy by helping them identify the days when pregnancy is likely. Identifying the fertile days involves tracking the menstrual cycle or monitoring a woman’s fertility signs. The woman prevents pregnancy by avoiding unprotected intercourse on fertile days. Fertility awareness-based methods provide options for women who want to use a natural method for medical or personal reasons. They are used by approximately 1.3% of U.S. women at risk of pregnancy. The “TwoDay method” and the “Ovulation method” use cervical mucus as a marker of ovulation. In the “Standard days method,” unprotected intercourse is avoided from cycle days 8 through 19. Approximately 47% of women using fertility awareness-based methods discontinue the method at 1 year, with typical use failure rates similar to those of the withdrawal method. Perfect-use failure rates with fertility awareness methods are in the 3-5% range for most methods, with the symptothermal method—which provides a crosscheck—much lower at 0.4% (Table 3-8).
Withdrawal is a method that has been practiced by more than one half of all U.S. couples during their lifetimes and is widely practiced in the adolescent population. Although its typical use failure rate of 22% places it in the next-to-lowest tier of contraceptive effectiveness, withdrawal still is much more effective than use of no contraceptive method. Sperm are present in the preejaculatory fluid of some men, which is one cause of withdrawal method failure. The withdrawal method does not eliminate the transmission of STIs. Preejaculatory fluid, for example, can contain cells infected with HIV.
Emergency Contraception ^349
Emergency contraception may be used to prevent pregnancy after an unprotected or inadequately protected act of sexual intercourse. Emergency contraception should be taken as soon as possible within 5 days of unprotected sexual intercourse. It is most effective if used within the first 24 hours. The most common emergency contraceptive method is oral progestin-only pills (levonorgestrel), but other effective methods include antiprogestin ulipristal acetate and combined regimens (high doses of ethinyl estradiol and a progestin). A copper IUD is the most effective form of emergency contraception for medically eligible women, may prevent pregnancy if inserted within 5 days of unprotected intercourse, and has the additional benefit of providing long-term, effective contraception.
Progestin-only emergency contraception is better tolerated and more efficacious than the combined regimen. In the United States, the two levonorgestrel-only regimens include a single-dose regimen (1.5 mg levonorgestrel) and a two-dose regimen (two tablets of 0.75 mg of levonorgestrel taken 12 hours apart).
The antiprogestin ulipristal acetate is at least as effective as levonorgestrel in preventing pregnancy up to 72 hours after unprotected intercourse and appears to be more effective than levonorgestrel in preventing pregnancy when used between 72 hours and 120 hours after unprotected intercourse. Ulipristal acetate may reduce the efficacy of combined hormonal contraceptive methods, such as oral contraceptives, patches, and rings. According to the U.S. SPR, any regular contraceptive method may be started immediately after using ulipristal acetate, but it is recommended that the woman abstain or use barrier contraception for 14 days or until her next menses and that she have a pregnancy test if she does not have a withdrawal bleed within 3 weeks. Guidance for the use of emergency contraception that contains levonorgestrel or combined hormonal contraceptives is similar except that abstinence or back-up methods are needed for only 7 days.
Emergency contraception should be offered or made available to women who experience unprotected or inadequately protected sexual intercourse and who do not desire pregnancy. Treatment with emergency contraception should be initiated as soon as possible to maximize efficacy, and it should be made available to patients who request it up to 120 hours after unprotected intercourse. No clinical examination or pregnancy testing is necessary before the provision or prescription of emergency contraception. Prescription or provision of emergency contraception in advance of need, particularly for adolescents younger than 17 years, can increase availability and may increase use. In 2013, the Plan B One-Step (Teva Women’s Health, Inc.) single-dose levonorgestrel regimen was made available over- the-counter without age restriction. The other levonorgestrel-only regimens also are available without a prescription but only to women aged 17 years or older with government-issued photo identification. A 30-mg tablet of ulipristal acetate requires a prescription.
Access to emergency contraception can be limited by pharmacist refusal and pharmacy stocking issues. Not all pharmacies stock these dedicated products, and pharmacist refusal may occur. Access to emergency contraception remains difficult for some populations, including adolescents, immigrants, non-English speaking women, survivors of sexual assault, those living in areas with few pharmacy choices, and poor women.
Some patients may have oral contraceptives in their household that can be used for emergency contraception. Table 3-9 describes appropriate formulations from a variety of combined oral contraceptives available in the United States. To reduce the chances of nausea with the combination estrogen-progestin regimen, an antiemetic agent (such as dimenhydrinate) is recommended and may be taken 1 hour before the first emergency contraception dose.
Emergency contraception is effective only before a pregnancy is established. The major, if not sole, mechanism of emergency contraception appears to be inhibition or delay of ovulation. Emergency contraception does not disrupt a pregnancy after nidation, or implantation, has occurred. No studies have specifically investigated adverse effects of exposure to emergency contraception during early pregnancy. However, numerous studies of the teratogenic risk of conception during daily use of oral contraceptives (including older, higher-dose preparations) have found no increase in risk to either the pregnant woman or the developing fetus.
Emergency contraception may be used even if the woman has used it before, even within the same menstrual cycle. The U.S. MEC includes no conditions in which the risks of emergency contraception outweigh the
Table 3-9. Oral Contraceptives That Can Be Used for Emergency Contraception in the United States* ^
| Brand | Company | First Doseτ | Second Ulipristal Doseτ Acetate (12 hours per later) Dose (mg) (ι | Ethinyl Estradiol per Dose microgram) | Levonorgestrel per Dose (mg)t |
| Ulipristal acetate pills | |||||
| ella | Watson | 1 white pill | Noneτ 30 | - | - |
| Progestin-only pills | |||||
| Plan B | Teva | 1 white pill | None - | - | 1.5 |
| One-Step | |||||
| Next Choice | Watson | 1 peach pill | None - | - | 1.5 |
| One Dose | |||||
| My Way | Gavis | 1 white pill | None - | - | 1.5 |
| Levon- | Perrigo | 2 white pills | Noneτ - | - | 1.5 |
| orgestrel | |||||
| Tablets | |||||
| Combined progestin and estrogen pills | |||||
| Altavera | Sandoz | 4 peach | 4 peach - | 120 | 0.60 |
| pills | pills | ||||
| Amethia | Watson | 4 white | 4 white - | 120 | 0.60 |
| pills | pills | ||||
| Amethia Lo | Watson | 5 white | 5 white - | 100 | 0.50 |
| pills | pills | ||||
| Amethyst | Watson | 6 white | 6 white - | 120 | 0.54 |
| pills | pills | ||||
| Aviane | Teva | 5 orange | 5 orange - | 100 | 0.50 |
| pills | pills | ||||
| Camrese | Teva | 4 light blue- | 4 light blue- - | 120 | 0.60 |
| green pills | green pills | ||||
| CamreseLo | Teva | 5 orange | 5 orange - | 100 | 0.50 |
| pills | pills | ||||
| Cryselle | Teva | 4 white | 4 white - | 120 | 0.60 |
| pills | pills | ||||
Table 3-9. Oral Contraceptives That Can Be Used for Emergency Contraception
| in the United States* (continued) | |||||
| Second | Ulipristal | Ethinyl | Levon- | ||
| Doseτ | Acetate | Estradiol | orgestrel | ||
| First | (12 hours | per | per Dose | per | |
| Brand | Company Doseτ | later) | Dose (mg) (microgram) Dose (mg)t | ||
Combined progestin and estrogen pills
| Enpresse | Teva | 4 orange pills | 4 orange - pills | 120 | 0.50 |
| Introvale | Sandoz | 4 peach pills | 4 peach - pills | 120 | 0.60 |
| Jolessa | Teva | 4 pink pills | 4 pink pills - | 120 | 0.60 |
| Lessina | Teva | 5 pink pills | 5 pink pills - | 100 | 0.50 |
| Levora | Watson | 4 white pills | 4 white - pills | 120 | 0.60 |
| Lo/Ovral | Akrimax | 4 white pills | 4 white - pills | 120 | 0.60 |
| LoSeasonique | Teva | 5 orange pills | 5 orange - pills | 100 | 0.50 |
| Low-Ogestrel | bgcolor=white>Watson4 white pills | 4 white - pills | 120 | 0.60 | |
| Lutera | Watson | 5 white pills | 5 white - pills | 100 | 0.50 |
| Lybrel | Wyeth | 6 yellow pills | 6 yellow - pills | 120 | 0.54 |
| Nordette | Teva | 4 lightorange pills | 4 light- - orange pills | 120 | 0.60 |
| Ogestrel | Watson | 2 white pills | 2 white - pills | 100 | 0.50 |
| Portia | Teva | 4 pink pills | 4 pink pills - | 120 | 0.60 |
| Quasense | Watson | 4 white pills | 4 white - pills | 120 | 0.60 |
| Seasonale | Teva | 4 pink pills | 4 pink pills - | 120 | 0.60 |
Table 3-9. Oral Contraceptives That Can Be Used for Emergency Contraception
| in the United States* (continued) | |||||
| Second | Ulipristal | Ethinyl | Levon- | ||
| Doseτ | Acetate | Estradiol | orgestrel | ||
| First | (12 hours | per | per Dose | per | |
| Brand | Company Doseτ | later) | Dose (mg) (microgram) Dose (mg)t | ||
Combined progestin and estrogen pills
| Seasonique | Teva | 4 light-blue- green pills | 4 light-blue- - green pills | 120 | 0.60 |
| Sronyx | Watson | 5 white | 5 white - | 100 | 0.50 |
| pills | pills | ||||
| Trivora | Watson | 4 pink pills | 4 pink pills - | 120 | 0.50 |
*ella, Plan B One-Step, Next Choice One Dose, My Way, and Levonorgestrel Tablets are the only dedicated products specifically marketed for emergency contraception. The regular oral contraceptives listed have been declared safe and effective for use as emergency contraceptive pills by the U.S. Food and Drug Administration. Outside the United States, approximately 100 emergency contraceptive products are specifically packaged, labeled, and marketed. Levonorgestrel-only emergency contraceptive pills are available either over-the-counter or from a pharmacist without having to see a clinician in 60 countries. In the United States, Plan B One-Step is available on the shelf with no restrictions. The one-pill generic products Next Choice One Dose and My Way will soon be available on the shelf, but will be available only to those aged 17 or older. The one-pill generic product Levonorgestrel Tablets is available at the pharmacy counter to women and men aged 17 and older, or by prescription to younger individuals. ella is available by prescription only.
τThe label for Levonorgestrel Tablets says to take one pill within 72 hours after unprotected intercourse, and another pill 12 hours later. However, research has found that both pills can be taken at the same time. All of the brands listed here may be effective when used within 120 hours after unprotected sex, but should be taken as soon as possible.
1The progestin in Cryselle, Lo/Ovral, Low-Ogestrel, and Ogestrel is norgestrel, which contains two isomers, only one of which (levonorgestrel) is bioactive; the amount of norgestrel in each tablet is twice the amount of levonorgestrel.
Reprinted with permission from Association of Reproductive Health Professionals, Office of Population Research at Princeton University. Emergency contraception website. Oral contraceptives that can be used for emergency contraception in the United States. Available at: http:// ec.princeton.edu/questions/dose.htmltfdose. Retrieved July 29, 2013.
This information is updated on a regular basis. For the most up to date information, see The Emergency Contraception web site at http://ec.princeton.edu/questions/dose.htmltfdose.
benefits. These criteria note that women with previous ectopic pregnancy, cardiovascular disease, migraines, or liver disease and women who are breastfeeding may use emergency contraception. Therefore, emergency contraception may be made available to women with contraindications to the use of conventional oral contraceptive preparations.
Information regarding effective contraceptive methods should be made available either at the time that emergency contraception is prescribed or at some convenient time thereafter. Use of highly effective long-acting reversible methods should be strongly encouraged. Repetitive use of emergency contraception is not as effective as other contraceptive methods such as IUDs, implants, injections, oral contraceptives, contraceptive rings, and patches. Clinical evaluation is indicated for women who have used emergency contraception if menses are delayed by 1 week or more after the expected time or if abdominal pain or persistent irregular bleeding develops.
Postpartum Contraception
Ovulation returns quickly after delivery, with an average time to ovulation of 45 days, so contraception initiation must occur quickly in women who are not using the lactational amenorrhea method. Because approximately two thirds of couples are sexually active in the first postpartum month and more than three fourths in the second postpartum month, contraception planning during the antenatal period is ideal. If initiation of a prescription-only method is delayed, the use of condoms is an excellent option. Withdrawal also provides some protection if couples choose not to use condoms. Timing of postpartum visits may depend on and affect the method and timing of postpartum contraception.
Breastfeeding and Choice of Contraceptive Method
Breastfeeding has multiple benefits to the mother and infant, including the potential benefit of contraception. The lactational amenorrhea method is an excellent method of contraception as long as three conditions are met: 1) menses have not returned, 2) the mother is fully or nearly fully breastfeeding (exclusively breastfeeding or the vast majority [85% or more] of feeds are breastfeeds), and 3) the infant is 6 months of age or younger. It should especially be noted that pumping milk appears not to have the same antiovulatory effect as suckling from breastfeeding.
Traditionally, combined oral contraceptives have not been recommended as the first choice for breastfeeding women because of concerns that the estrogenic component of combined oral contraceptives can reduce the volume of milk production and the caloric and mineral content of breast milk. However, use of combined oral contraceptives by well- nourished breastfeeding women does not appear to result in infant development problems. A systematic review of randomized controlled trials concluded that existing data are of poor quality, report inconsistent findings, and are insufficient to establish an effect of hormonal contraception on lactation. Use of combined hormonal contraceptives can be considered once milk flow is well established. Overall, progestin-only methods (progestin-only pills, DMPA, levonorgestrel IUD, and etonogestrel single-rod contraceptive implant) appear to have little effect on either breastfeeding success or infant growth and health, and some obstetricians routinely initiate these methods in many women before hospital discharge, including those who choose to breastfeed.
Timing of Initiation
Postpartum women remain in a hypercoagulable state for weeks after childbirth, but ovulation can occur as early as 25 days postpartum in women who are not breastfeeding, making timely initiation of contraception important. Before initiation of contraception, the health care provider should confirm that the woman meets medical eligibility criteria for the chosen method (see U.S. MEC) and be reasonably certain that she is not pregnant (Box 3-16). Timing of initiation varies based on the contraceptive method and whether the mother is breastfeeding (Table 3-10).
Need for Back-up Contraception
A postpartum woman’s need for back-up contraception depends on the method of primary contraception initiated, whether she is breastfeeding, and whether her menstrual cycle has resumed. Women who are using the copper IUD require no additional contraceptive protection, regardless of breastfeeding or menstruation status. For women who are less than 6 months
postpartum, amenorrheic, and fully or nearly fully breastfeeding (exclusively breastfeeding or the vast majority [85% or more] of feeds are breastfeeds), no additional contraceptive protection is needed. Otherwise, a woman who is 21 days or more postpartum and has not experienced return of her menstrual cycle needs to abstain from sexual intercourse or use additional contraceptive protection for the next 7 days (for combined oral contraceptives users) or the next 2 days (for progestin-only pill users). If a woman’s menstrual cycle has resumed and it has been more than 5 days since the start of menstrual bleeding (or more than 7 days in the case of levonorgestrel IUD or DMPA injection users), additional contraceptive protection is needed for the next 7 days (or the next 2 days for progestin-pill users).
Table 3-10. U.S. Medical Eligibility Criteria for Postpartum Initiation of Contraception* ^
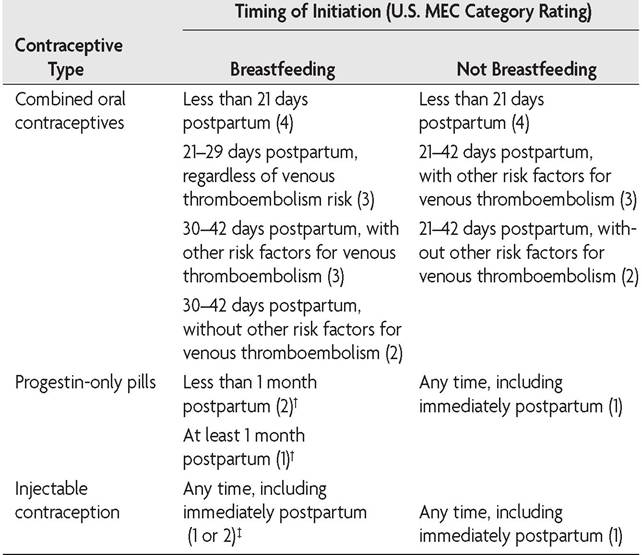
Table 3-10. U.S. Medical Eligibility Criteria for Postpartum Initiation of Contraception* (continued)
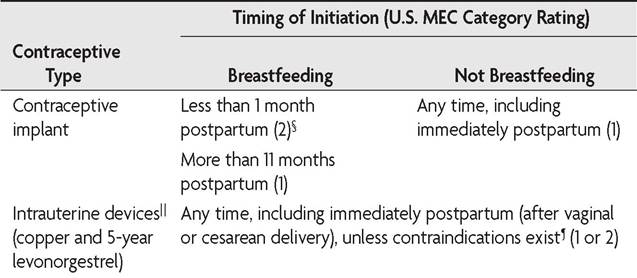
Abbreviations: IUD, intrauterine device; U.S. MEC, U.S. Medical Eligibility Criteria for Contraceptive Use, 2010.
*Before initiation of contraception, the health care provider should confirm that the woman meets medical eligibility criteria for the chosen method (see U.S. Medical Eligibility Criteria for Contraceptive Use) and be reasonably certain that she is not pregnant.
τIn nursing women who use progestin-only oral contraceptives, very small amounts of progestin are passed into the breast milk, and no adverse effects on infant growth have been observed. 1When initiated immediately postpartum, use of depot medroxyprogesterone acetate does not adversely affect lactation or infant development.
§A category 2 rating is given because of theoretical concerns regarding milk production and infant growth and development.
∣∣This does not include the 3-year IUD. For information on prescribing, see Bayer HealthCare Pharmaceuticals Inc. Skyla (levonorgestrel-releasing intrauterine system): highlights of prescribing information. Wayne (NJ): Bayer; 2013. Available at: http://labeling.bayerhealthcare.com/ html/products/pi/Skyla_PI.pdf. Retrieved July 26, 2013.
’Immediate postpartum insertion of an IUD is contraindicated in cases of puerperal sepsis or septic abortion.
Data from U.S. Selected Practice Recommendations for Contraceptive Use, 2013: adapted from the World Health Organization selected practice recommendations for contraceptive use, 2nd edition. Division of Reproductive Health, National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention. MMWR Recomm Rep 2013;62:1-60.
Contraceptive Failure
If a pregnancy occurs while a hormonal method of contraception is being used, the method should be discontinued, although there is no substantive evidence that the use of any method of contraception during early pregnancy is associated with fetal anomalies. If a patient becomes pregnant
while using an IUD, the U.S. SPR recommends an evaluation for ectopic pregnancy, counseling regarding the increased risk of spontaneous abortion (including septic abortion) and preterm delivery if the IUD is left in place, and removal of the IUD as soon as possible if the strings are visible or the device can be removed safely. If the IUD strings are not visible or the IUD cannot be removed safely, consider performing or referring for ultrasound examination to determine the location of the IUD. If ultrasonography is not available or fails to locate the device, advise the woman to seek care promptly if she has heavy bleeding, cramping, pain, abnormal vaginal discharge, or fever.
Bibliography
Access to emergency contraception. Committee Opinion No. 542. American College of Obstetricians and Gynecologists. Obstet Gynecol 2012;120:1250-3. [PubMed] [Obstetrics & Gynecology]
Access to postpartum sterilization. Committee Opinion No. 530. American College of Obstetricians and Gynecologists. Obstet Gynecol 2012;120:212-15. [PubMed] [Obstetrics & Gynecology]
Adolescents and long-acting reversible contraception: implants and intrauterine devices. Committee Opinion No. 539. American College of Obstetricians and Gynecologists. Obstet Gynecol 2012;120:983-8. [PubMed] [Obstetrics & Gynecology] American College of Obstetricians and Gynecologists. Guidelines for adolescent health care [CD-ROM]. 2nd ed. ed. Washington, DC: American College of Obstetricians and Gynecologists; 2011.
American College of Obstetricians and Gynecologists. Reproductive health care for adolescents with disabilities: supplement to Guidelines for adolescent health care. 2nd ed. ed. Washington, DC: American College of Obstetricians and Gynecologists; 2012. Available at: http://www.acog.org/Resources_And_Publications/Guidelines_ for_Adolescent_Health_Care/Reproductive_Health_Care_for_Adolescents_With_ Disabilities. Retrieved July 23, 2013.
Bartz D, Greenberg JA. Sterilization in the United States. Rev Obstet Gynecol 2008; 1:23-32. [PubMed] [Full Text]
Bayer HealthCare Pharmaceuticals Inc. Mirena (levonorgestrel-releasing intrauterine system): highlights of prescribing information. Wayne (NJ): Bayer; 2013. Available at: http://labeling.bayerhealthcare.com/html/products/pi/Mirena_PI.pdf. Retrieved July 26, 2013.
Bayer HealthCare Pharmaceuticals Inc. Skyla (levonorgestrel-releasing intrauterine system): highlights of prescribing information. Wayne (NJ): Bayer; 2013. Available at: http://labeling.bayerhealthcare.com/html/products/pi/Skyla_PI.pdf. Retrieved July 26, 2013.
Benefits and risks of sterilization. Practice Bulletin No. 133. American College of Obstetricians and Gynecologists. Obstet Gynecol 2013;121:392-404. [PubMed] [Obstetrics & Gynecology]
Brand versus generic oral contraceptives. ACOG Committee Opinion No. 375. American College of Obstetricians and Gynecologists. Obstet Gynecol 2007;110: 447-8. [PubMed] [Obstetrics & Gynecology]
Depot medroxyprogesterone acetate and bone effects. Committee Opinion No. 602. American College of Obstetricians and Gynecologists. Obstet Gynecol 2014;123:1398-402. [PubMed] [Obstetrics & Gynecology]
Emergency contraception. Practice Bulletin No. 112. American College of Obstetricians and Gynecologists. Obstet Gynecol 2010;115:1100-9. [PubMed] [Obstetrics & Gynecology]
Hatcher RA, Trussell J, Nelson AL, Cates WJ, Kowal D, Policar MS, editors. Contraceptive technology. 20th revised ed. New York (NY): Ardent Media; 2011.
Increasing use of contraceptive implants and intrauterine devices to reduce unintended pregnancy. ACOG Committee Opinion No. 450. American College of Obstetricians and Gynecologists. Obstet Gynecol 2009;114:1434-8. [PubMed] [Obstetrics & Gynecology]
Institute for Reproductive Health. Fertility awareness. Available at: http://irh.org/ focus-areas/fertility_awareness. Retrieved July 29, 2013.
Janssen Pharmaceuticals Inc. Ortho Evra (norelgestromin/ethinyl estradiol transder- mal system): highlights of prescribing information. Titusville (NJ): Janssen; 2013. Available at: http://www.orthoevra.com/sites/default/files/assets/OrthoEvraPI.pdf. Retrieved July 29, 2013.
Jones J, Mosher W, Daniels K. Current contraceptive use in the United States, 2006-2010, and changes in patterns of use since 1995. Natl Health Stat Report 2012;(60):1-25. [PubMed]
Labbok MH, Perez A, Valdes V, Sevilla F, Wade K, Laukaran VH, et al. The lactational amenorrhea method (LAM): a postpartum introductory family planning method with policy and program implications. Adv Contracept 1994;10:93-109. [PubMed] Long-acting reversible contraception: implants and intrauterine devices. Practice bulletin No. 121. American College of Obstetricians and Gynecologists. Obstet Gynecol 2011;118:184-96. [PubMed] [Obstetrics & Gynecology]
Lyus R, Lohr P, Prager S, Board of the Society of Family Planning. Use of the Mirena LNG-IUS and Paragard CuT380A intrauterine devices in nulliparous women. Contraception 2010;81:367-71. [PubMed]
Merck & Company Inc. NuvaRing® (etonogestrel/ethinyl estradiol vaginal ring). Whitehouse Station (NJ): Merck; 2012. Available at: http://www.merck.com/prod uct/usa/pi_circulars/n/nuvaring/nuvaring_pi.pdf. Retrieved July 29, 2013.
Multifetal pregnancy reduction. Committee Opinion No. 553. American College of Obstetricians and Gynecologists. Obstet Gynecol 2013;121:405-10. [PubMed] [Obstetrics & Gynecology]
Over-the-counter access to oral contraceptives. Committee Opinion No 544. American College of Obstetricians and Gynecologists. Obstet Gynecol 2012;120: 1527-31. [PubMed] [Obstetrics & Gynecology]
Reproductive and sexual coercion. Committee Opinion No. 554. American College of Obstetricians and Gynecologists. Obstet Gynecol 2013;121:411-5. [PubMed] [Obstetrics & Gynecology]
Risk of venous thromboembolism among users of drospirenone-containing oral contraceptive pills. Committee Opinion No. 540. American College of Obstetricians and Gynecologists; Obstet Gynecol 2012;120:1239-42. [PubMed] [Obstetrics & Gynecology]
Steenland MW, Zapata LB, Brahmi D, Marchbanks PA, Curtis KM. Appropriate follow up to detect potential adverse events after initiation of select contraceptive methods: a systematic review. Contraception 2013;87:611-24. [PubMed] [Full Text] Trussell J. Contraceptive efficacy. In: Hatcher RA, Trussell J, Nelson AL, Cates WJ, Kowal D,Policar MS, editors. Contraceptive technology. 20th revised ed. New York (NY): Ardent Media; 2011. p. 779-863.
U.S. Medical Eligibility Criteria for Contraceptive Use, 2010. Centers for Disease Control and Prevention. MMWR Recomm Rep 2010;59(RR-4):1-86. Available at: http://www.cdc.gov/mmwr/pdf/rr/rr5904.pdf. Retrieved September 11, 2013.
U.S. Selected Practice Recommendations for Contraceptive Use, 2013: adapted from the World Health Organization selected practice recommendations for contraceptive use, 2nd edition. Division of Reproductive Health, National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention. MMWR Recomm Rep 2013;62:1-60. [PubMed]
Understanding and using the U.S. Medical Eligibility Criteria For Contraceptive Use, 2010. Committee Opinion No. 505. American College of Obstetricians and Gynecologists. Obstet Gynecol 2011;118:754-60. [PubMed] [Obstetrics & Gynecology]
Understanding and using the U.S. Selected Practice Recommendations for Contraceptive Use, 2013. Committee Opinion No. 577. American College of Obstetricians and Gynecologists. Obstet Gynecol 2013;122:1132-3. [PubMed] [Obstetrics & Gynecology]
Update to CDC's U.S. Medical Eligibility Criteria for Contraceptive Use, 2010: revised recommendations for the use of contraceptive methods during the postpartum period. Centers for Disease Control and Prevention. MMWR Morb Mortal Wkly Rep 2011;60:878-83. [PubMed] [Full Text]
Watson Pharma Inc. ELLA-ulipristal acetate tablet. Parsippany (NJ): Watson; 2012. Available at: http://pi.actavis.com/data_stream.asp?product_group=1699&p =pi&language=E. Retrieved July 29, 2013.
Resources
American College of Obstetricians and Gynecologists. Barrier methods of contraception. Patient Education Pamphlet AP022. Washington, DC: American College of Obstetricians and Gynecologists; 2011.
American College of Obstetricians and Gynecologists. Birth control. Patient Education Booklet AB020. Washington, DC: American College of Obstetricians and Gynecologists; 2011.
American College of Obstetricians and Gynecologists. Combined hormonal birth control methods: pills, patches, and rings. Patient Education Pamphlet AP185. Washington, DC: American College of Obstetricians and Gynecologists; 2014.
American College of Obstetricians and Gynecologists. Emergency contraception. Patient Education Pamphlet AP114. Washington, DC: American College of Obstetricians and Gynecologists; 2013.
American College of Obstetricians and Gynecologists. Long-acting reversible contraception Patient Education Pamphlet AP184. Washington, DC: American College of Obstetricians and Gynecologists; 2014.
American College of Obstetricians and Gynecologists. Natural family planning. Patient Education Pamphlet AP024. Washington, DC: American College of Obstetricians and Gynecologists; 2012.
American College of Obstetricians and Gynecologists. Postpartum sterilization. Patient Education Pamphlet AP052. Washington DC: American College of Obstetricians and Gynecologists; 2013.
American College of Obstetricians and Gynecologists. Progestin-only hormonal birth control methods: pills and injections. Patient Education Pamphlet AP186. Washington, DC: American College of Obstetricians and Gynecologists; 2014.
American College of Obstetricians and Gynecologists. Sterilization by laparoscopy. Patient Education Pamphlet AP035. Washington, DC: American College of Obstetricians and Gynecologists; 2013.
American College of Obstetricians and Gynecologists. Sterilization for women and men. Patient Education Pamphlet AP011. Washington, DC: American College of Obstetricians and Gynecologists; 2014.
American College of Obstetricians and Gynecologists. Long-Acting Reversible Contraception. Available at http://www.acog.org/About_ACOG/ACOG_Depart ments/Long_Acting_Reversible_Contraception. Retrieved July 29, 2013.
Association of Reproductive Health Professionals, Office of Population Research at Princeton University. Emergency contraception hotline. 1-888-NOT-2-LATE.
Association of Reproductive Health Professionals, Office of Population Research at Princeton University. Emergency contraception website. Oral contraceptives that can be used for emergency contraception in the United States. Available at: http:// ec.princeton.edu/questions/dose.html#dose. Retrieved July 29, 2013.
Association of Reproductive Health Professionals. A quick reference guide for clinicians: choosing a birth control method. Washington, DC: ARHP; 2011. Available at: http://wwww.arhp.org/uploadDocs/choosingqrg.pdf. Retrieved July 29, 2013.
Association of Reproductive Health Professionals. Health matters: facts about emergency contraception pills. Washington, DC: ARHP; 2012. Available at: http:// wwww.arhp.org/uploadDocs/EC_healthmatters.pdf. Retrieved July 29, 2013.
Association of Reproductive Health Professionals. Method match. Available at: http://wwww.arhp.org/MethodMatch. Retrieved July 29, 2013.
Bedsider. The National Campaign to Prevent Teen and Unplanned Pregnancy. Available at: http://bedsider.org. Retrieved July 29, 2013.
Cromer BA, Scholes D, Berenson A, Cundy T, Clark MK, Kaunitz AM. Depot medroxyprogesterone acetate and bone mineral density in adolescents—the Black Box Warning: a Position Paper of the Society for Adolescent Medicine. Society for Adolescent Medicine. J Adolesc Health 2006;39:296-301. [PubMed] [Full Text]
Jaccard J. Careful, current, and consistent: tips to improve contraceptive use. Washington, DC: National Campaign to Prevent Teen and Unplanned Pregnancy; 2010. Available at: https://thenationalcampaign.org/sites/default/files/resource- primary-download/carefulcurrentconsistent.pdf. Retrieved March 28, 2014.
Jaccard J. Unlocking the contraception conundrum: reducing unplanned pregnancies in emerging adulthood. Washington, DC: National Campaign to Prevent Teen and Unplanned Pregnancy; 2009. Available at: http://thenationalcampaign. org/sites/default/files/resource-primary-download/unlocking_contraceptive.pdf. Retrieved March 28, 2014.
Johns Hopkins Bloomberg School of Public Health, Center for Communication Programs, Information and Knowledge for Optimal Health (INFO), World Health Organization. Decision-making tool for family planning clients and providers. Baltimore (MD); INFO; Geneva: WHO; 2005. Available at: http://whqlibdoc.who. int/publications/2005/9241593229_eng.pdf. Retrieved July 29, 2013.
Johns Hopkins Bloomberg School of Public Health, United States Agency for International Development, World Health Organization. Family planning: a global handbook for providers. Baltimore (MD): JHBSPH; Washington, DC: USAID; Geneva: WHO; 2011. Available at: http://whqlibdoc.who.int/publica- tions/2011/9780978856373_eng.pdf. Retrieved July 29, 2013.
Kapp N, Curtis KM. Combined oral contraceptive use among breastfeeding women: a systematic review. Contraception 2010;82:10-6. [PubMed] [Full Text]
Planned Parenthood Federation of America. Birth control. Available at: http://www. plannedparenthood.org/health-topics/birth-control-4211.htm. Retrieved July 29, 2013.
Planned Parenthood Federation of America. My method. Available at: http://www. plannedparenthood.org/all-access/my-method-26542.htm. Retrieved July 29, 2013.
Society of Family Planning, Clinical guidelines. Available at: http://societyfp.org/ resources/guidelines.asp. Retrieved September 27, 2013.
Sterilization of women, including those with mental disabilities. ACOG Committee Opinion No. 371. American College of Obstetricians and Gynecologists. Obstet Gynecol 2007;110:217-20. [PubMed] [Obstetrics & Gynecology]
Vasquez P, Schreiber CA. The missing IUD. Contraception 2010;82:126-8. [PubMed] [Full Text]
World Health Organization. Medical eligibility criteria for contraceptive use. 4th ed. Geneva: WHO; 2009. Available at: http://whqlibdoc.who.int/publications/2010/ 9789241563888_eng.pdf. Retrieved June 7, 2013.