Hypertensive Disorders of Pregnancy: Preeclampsia/ Eclampsia
Luis Sanchez-Ramos
Hypertensive disorders of pregnancy, including preeclampsia and eclampsia, are the second leading cause of maternal mortality in the United States. Preeclampsia is a disorder that affects women exclusively during pregnancy.
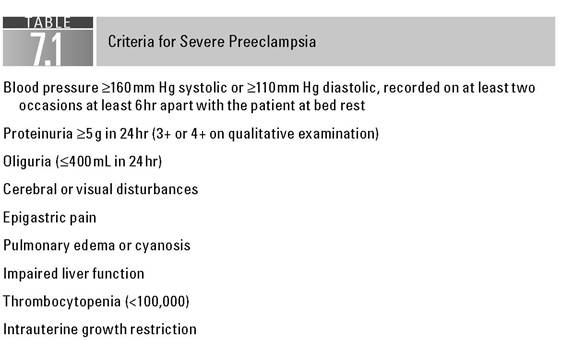
It is a disease of unknown etiology that presents in pregnant women at both extremes of reproductive age. Reported incidences range from 2% to 30%, depending on the diagnostic criteria used and the population studied (1). Conditions associated with an increased incidence include previous preeclampsia, multifetal pregnancy, molar pregnancy, and triploidy. It is a clinical condition that comprises a wide spectrum of signs and symptoms that have been observed to develop alone or in combination. Complications resulting from preeclampsia are also a leading cause of perinatal morbidity and mortality.The diagnosis of the disease is based on the presence of hypertension in association with significant proteinuria. Preeclampsia is usually classified clinically as mild or severe (2). However, even in a seemingly stable patient with minimal signs and symptoms, this disease can rapidly progress to life-threatening eclampsia, with seizures and complications that may include pulmonary edema, intracerebral hemorrhage, acute renal failure, disseminated intravascular coagulation, and abruptio placentae. The criteria for severe preeclampsia are summarized in Table 7.1.
There appears to be an increased incidence of preeclampsia in patients with minimal or no prenatal care and in those of low socioeconomic status (3). All these types of patients are frequently seen for the first time by physicians in the emergency department. Consequently, it is not unusual for such physicians to be the first to make the diagnosis and initiate appropriate management.
PATHOPHYSIOLOGY
The basic disorder underlying preeclampsia is vasospasm.
Constriction of the arterioles causes resistance to blood flow and subsequent arterial hypertension. Vasospasm and damage to the vascular endothelium in combination with local hypoxia presumably lead to hemorrhage, necrosis, and other end-organ disturbances of severe preeclampsia.Vascular reactivity to infused angiotensin II and other vasopressors is decreased in normotensive pregnancy (4,5). The refractoriness to angiotensin II may be mediated by vascular endothelium synthesis of vasodilatory prostaglandins such as prostacyclin. There are data to suggest that preeclampsia may be associated with inappropriately increased production of prostaglandins with vasoconstrictor properties such as thromboxane. Several authors have shown increased vascular reactivity to pressor hormones in patients with early preeclampsia. The increased reactivity to vasopressors may be due to altered ratios of thromboxane and prostacyclin (6).
Pregnancy normally increases blood volume by as much as 40%, but the expansion may not occur in a woman destined to develop preeclampsia. Vasospasm contracts the intravascular space and leaves her highly sensitive
to fluid therapy or blood loss at delivery. The vascular contraction impairs uteroplacental blood flow, contributes to intrauterine growth restriction, and may lead to intrauterine fetal demise. Circulatory impairment reduces renal perfusion and glomerular filtration, and swelling of intracapillary glomerular cells and glomerular endotheliosis may result. Edema probably occurs because of maldistribution of extracellular fluid, since plasma fluid is not increased.
DIAGNOSIS
The diagnosis of preeclampsia is usually straightforward: the blood pressure is at least 140/90 mm Hg on at least two occasions 6 or more hours apart. In the past, it was recommended that an increase of 30 mm Hg in systolic or 15 mm Hg in diastolic blood pressure be used as a diagnostic criterion, even when absolute values remained lower than 140/90 mm Hg.
During the last decade, the former definition has been accepted by the Working Group on High Blood Pressure in Pregnancy, because the only available evidence shows that women with blood pressures meeting the old criterion are not likely to have adverse outcomes (7,8).In addition to hypertension, the patient often presents with significant proteinuria, defined as the presence of at least 300 mg of protein in a 24-hour urine collection or a reading of 1+ or higher on random dipstick samples. The degree of proteinuria often fluctuates widely over a 24-hour period. Therefore, a single random sample may fail to detect significant proteinuria.
Although in the past, edema was an accepted criterion for the diagnosis of preeclampsia, it is such a common finding in pregnant women that its presence should not validate the existence of preeclampsia any more than its absence should rule out the diagnosis. However, significant edema of the hands and face associated with a sudden increase in weight may be a valuable warning sign (Fig. 7.1).
In addition to the classic findings of hypertension and proteinuria, other laboratory clues may be helpful in the diagnosis of preeclampsia. Thrombocytopenia may at times be an early warning in patients who subsequently will develop hypertensive disorders of pregnancy. Increased serum levels of uric acid may be of both prognostic and diagnostic values. Patients with preeclampsia have markedly decreased urinary excretion of calcium; in fact, hypocalciuria can be detected prior to the appearance of clinical signs and symptoms (9).

FIGURE 7.1 Preeclampsia: edema of face, hand, and foot.
Hypertension and proteinuria, the two most important signs of preeclampsia, are often not obvious. By the time the patient has developed symptoms, such as epigastric pain and severe headache, the disorder may be far advanced. For this reason, prenatal care for early detection of this disorder is imperative (Fig.
7.2).One of the earliest signs of preeclampsia may be a sudden increase in weight. Whenever weight gain exceeds 0.91 kg in any given week, or 2.73kg in a month, early preeclampsia should be considered. Sudden and excessive weight gain may be attributed to abnormal retention of fluid and is demonstrable before significant edema of the face or upper extremities.
The most dependable warning sign of preeclampsia is hypertension. The diastolic blood pressure is a more reliable prognostic sign than the systolic, and a persisting diastolic pressure of ≥90mm Hg is abnormal. Proteinuria varies greatly from case to case and, in the same patient, from hour to hour. This variability is likely due to intermittent renal vasospasm. Frequent urinary dipstick readings or a 24-hour urinary collection is often necessary to diagnose proteinuria.
Other signs and symptoms of preeclampsia, such as severe headache, epigastric pain, blurry vision, shortness of breath, and decreased urinary output, usually appear late and in severe cases (see Table 7.1). However, hemolysis, elevated liver enzymes, and low platelets (HELLP syndrome) may be an early portent of severe preeclampsia (10-12).
Prepartum management
The goal of therapy is to prevent eclampsia, as well as other severe complications of preeclampsia. The only definitive therapy for preeclampsia/eclampsia is delivery. Once this has been achieved in a form that assures maximum safety for both the mother and the newborn, the patient is usually on her way to full recovery. This decision is fairly simple in patients with mild preeclampsia at term or with severe preeclampsia at any time during gestation. However, the management of patients with mild preeclampsia far from term is very controversial (13). Some of the areas of controversy include the need for hospitalization, the use of antihypertensive agents, and the use of sedatives and anticonvulsants. Most obstetricians in this country usually advise bed rest in the hospital for the
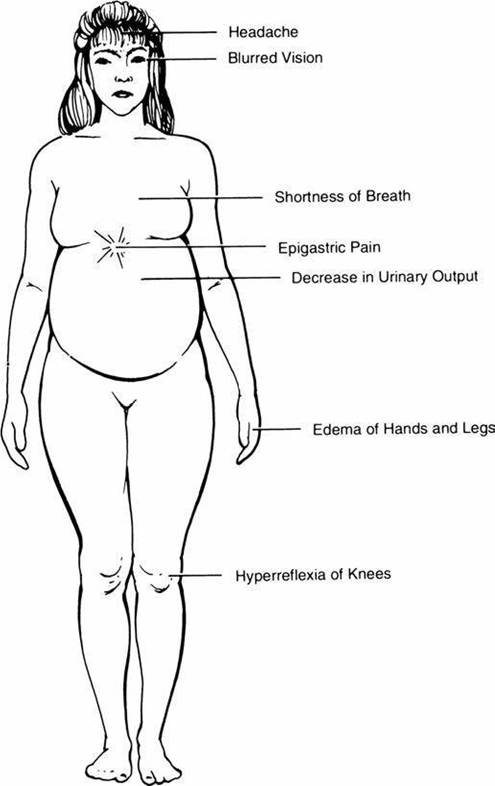
FIGURE 7.2 Signs and symptoms of preeclampsia.
duration of the pregnancy. Ambulatory treatment may be appropriate for a minority of compliant private patients with very mild preeclampsia.
Preterm patients with mild preeclampsia are admitted to the hospital and placed on bed rest. Although this seems a reasonable form of therapy, its efficacy is not clearly established. Strict sodium restriction or diuretic therapy has no role in the prevention or treatment of preeclampsia. Patients are usually placed on a regular diet, although some authorities recommend a high-protein diet. Close monitoring of both the mother and the fetus is initiated. Daily monitoring should include hematocrit and platelet count, frequent blood pressure checks, maternal weight estimation, and search for clinical evidence of severe disease. Important clinical signs and symptoms of severe disease include headache, epigastric pain, blurred vision, and shortness of breath.
If deterioration is progressive, as determined by laboratory findings, symptoms, and clinical signs, the decision to continue the pregnancy must be reevaluated daily. Important clinical signs that need to be monitored include blood pressure, urinary output, and fluid retention as evidenced by daily weight increase. Laboratory studies (24-hour urinary collection for total protein and creatinine clearance, complete blood count, serum uric acid, blood urea nitrogen, and creatinine) should be performed at intervals of no more than 48 hours. Once it has been determined that the patient has developed severe preeclampsia, steps should be taken for prompt delivery.
Fetal size, determined by ultrasonic biometry, is an accurate guide to the functional status of the fetus. Lack of growth suggests insufficient blood flow, which places the fetus in danger because of lack of placental reserve. Another indirect measure of altered maternal circulation is uterine artery Doppler velocimetry, which may serve as an early marker for preeclampsia.
Every effort should be made to deliver the baby as close to term as possible.
Regardless of fetal maturity, however, delivery is indicated whenever the fetoplacental unit is shown to be failing, as documented by a lack of fetal growth or of reassuring tests of fetal well-being. In severe preeclampsia, neonatal survival reportedly ranges from 10% to 37%, depending on gestational age at delivery and birth weight.The most important test of maturity is the lecithin/sphingomyelin ratio, which can be used to determine the risk of severe respiratory distress syndrome. The risk is high when the ratio is and good nutrition are still the most effective means of decreasing the incidence and severity of this disease.
References
1. MacGillivray I. Some observations on the incidence of preeclampsia. J Obstet Gynaecol Br Empire. 1958;65:536.
2. Hughes EC, ed. Obstetric-Gynecologic Terminology. Philadelphia, PA: Davis; 1972:422.
3. Gant NF, Daley GL, Chand S, Whalley PJ, MacDonald PC. A study of angiotensin II pressor response throughout primigravida pregnancy. J Clin Invest. 1973;52:2682.
4. Talledo OE, Chesley LC, Zuspan FP. Renin-angiotensin system in normal and toxemic pregnancies. III. Differential sensitivity to angiotensin II and norepinephrine in toxemia of pregnancy. Am J Obstet Gynecol. 1968;100:218.
5. Sibai BM. The HELLP syndrome (hemolysis, elevated liver enzymes, and low platelets): much ado about nothing? Am J Obstet Gynecol. 1990;162:311.
6. Sibai BM, Taslimi MM, El-Nazer A, et al. Maternal perinatal outcome associated with the syndrome of hemolysis, elevated liver enzymes, and low platelets in severe preeclampsia-eclampsia. Am J Obstet Gynecol. 1986;155:501.
7. North RA, Taylor RS, Schellenberg JC. Evaluation of a definition of pre-eclampsia. Br J Obstet Gynaecol. 1999;106:767-773.
8. Levine RJ. Should the definition of preeclampsia include a rise in diastolic blood pressure ≥15 mm Hg? Am J Obstet Gynecol 2000;182:225.
9. Sanchez-Ramos L, Jones DC, Cullen MT. Urinary calcium as an early marker for preeclampsia. Obstet Gynecol. 1991;77:685.
10. Cunningham FG, Leveno KJ. Management of pregnancy-induced hypertension. In: Rubin PC, ed. Handbook of Hypertension, Vol 10. Hypertension in Pregnancy. Amsterdam, the Netherlands: Elsevier; 1988:290.
11. Sibai BM, McCubbin JH, Anderson GD, et al. Eclampsia. I. Observations from sixtyseven recent cases. Obstet Gynecol. 1981;58:609.
12. Adams EM, MacGillivray I. Long-term effect of preeclampsia on blood pressure. Lancet. 1961;2:1373.
13. Fisher KA, Luger A, Spargo BH, Lindheimer MD. Hypertension in pregnancy: clinical-pathologic correlations and remote prognosis. Medicine. 1981;60:267.
14. Aarnoudse JG, Houthoff HJ, Weits J, Vellenga E, Huisjes HJ. A syndrome of liver damage and intravascular coagulation in the last trimester of normotensive pregnancy: a clinical and histopathological study. Br J Obstet Gynaecol. 1986;93:145.
15. Hinselmann H. Allgemeine Krankheitslehre. In: Hinselmann H, ed. Die Eklampsie. Bonn, Germany: Cohen; 1924:1.
16. Beaufils M, Uzan S, Donsimoni R, Colau JC. Prevention of pre-eclampsia by early antiplatelet therapy. Lancet. 1985;1:840.
17. Wallenburg HC, Dekker GA, Makovitz JW, Rotmans P. Low-dose aspirin prevents pregnancy-induced hypertension and pre-eclampsia in angiotensin-sensitive primigravidae. Lancet. 1986;1:1.
18. Schiff E, Peleg E, Goldenberg M, et al. The use of aspirin to prevent pregnancy- induced hypertension and lower the ration of thromboxane A2 to prostacyclin in relatively high-risk pregnancies. N Engl J Med. 1989;321:351.
19. Benigni A, Gregorini G, Frusca T, et al. Effect of low dose aspirin on fetal and maternal generation of thromboxane by platelets in women at risk for pregnancy-induced hypertension. N Engl JMed. 1989;321:357.
20. Knight M, Duley L, Henderson-Smart D, King JF. Antiplatelet agents for preventing and treating pre-eclampsia. Cochrane Pregnancy and Childbirth Group. Cochrane Database Syst Rev. 2009;1.
21. Bucher HC, Guyatt GH, Cook RJ, et al. Effect of calcium supplementation on pregnancy-induced hypertension and preeclampsia: a meta-analysis of randomized controlled trials. JAMA. 1996;275:1113.
22 Melnikow JA. Calcium supplementation during pregnancy. J Fam Pract. 1996;43:115.
23. Lewis R, Sibai B. Recent advances in the management of preeclampsia. JMatern Fetal Med. 1997;6:6.