I OSTEOPOROSIS ^470 ^485 ^508 ^571
Osteoporosis is a skeletal disorder characterized by loss of bone mass, deterioration of microarchitecture, and a decline in bone quality, all of which lead to an increased vulnerability to fracture.
The time of most rapid bone loss in women coincides with the marked decline in estrogen levels associated with menopause. Approximately 9% of U.S. women aged 50 years and older have osteoporosis at the femur neck or lumbar spine, and another 49% of women older than 50 years have low bone mass at the femur neck or lumbar spine, according to the most recent data from the National Health and Nutrition Examination Survey (2005-2008).Bone mass decreases with age, and bone fragility increases with age. At any bone density, the likelihood of fracture is greater in older women (and men) because of the increase in bone fragility. Although there are many factors that contribute to the likelihood of a fracture, low bone mass is a key determinant and one that is potentially modifiable. Although morbidity and mortality are especially high with hip fractures, the more common thoracic compression spine fracture also is a source of marked morbidity, including pain, deformity, loss of independence, and reduced cardiovascular, respiratory, and even digestive function.
The risk of postmenopausal osteoporosis is a function of the peak bone mass acquired during adolescent growth and the rate of bone loss in adulthood. A decline in adult estrogen levels has been associated with the loss of bone mineral density (BMD) in a number of conditions: anorexia nervosa, lactation, menopause, hypogonadism, and prolonged use of medications such as progestin-only contraceptives (eg, depot medroxyprogesterone acetate [DMPA]), gonadotropin-releasing hormone agonists, and aromatase inhibitors. Certain other drugs and certain diseases or medical conditions also are known to be associated with bone loss (see Box 3-10).
Osteoporosis is a treatable complication of aging. Preventive measures, screening strategies, and pharmacologic interventions for women at high
Box 3-10. Conditions, Diseases, and Medications That Cause or Contribute to Osteoporosis and Fractures ^
• Lifestyle factors: low calcium intake, vitamin D insufficiency, excess vitamin A, high caffeine intake, high salt intake, aluminum intake (in antacids), alcohol intake (three or more drinks per day), inadequate physical activity, immobilization, smoking (active or passive), falling, thinness
• Genetic factors: cystic fibrosis, homocystinuria, osteogenesis imperfecta, Ehlers-Danlos syndrome, hypophosphatasia, parental history of hip fracture, Gaucher disease, idiopathic hypercalciuria, porphyria, glycogen storage diseases, Marfan syndrome, Riley-Day syndrome, hemochromatosis, Menkes (steely hair) syndrome
• Hypogonadal states: androgen insensitivity, hyperprolactinemia, Turner and Klinefelter syndromes, anorexia nervosa and bulimia, panhypopituitarism, athletic amenorrhea, premature ovarian failure
• Endocrine disorders: adrenal insufficiency, diabetes mellitus, thyrotoxicosis, Cushing's syndrome, hyperparathyroidism
• Gastrointestinal disorders: celiac disease, inflammatory bowel disease, primary biliary cirrhosis, gastric bypass, malabsorption, gastrointestinal surgery, pancreatic disease
• Hematologic disorders: hemophilia, multiple myeloma, systemic mastocytosis, leukemia and lymphomas, sickle cell disease, thalassemia
• Rheumatic and autoimmune diseases: ankylosing spondylitis, lupus, rheumatoid arthritis
• Miscellaneous conditions and diseases: alcoholism, emphysema, muscular dystrophy, amyloidosis, end-stage renal disease, parenteral nutrition, chronic metabolic acidosis, epilepsy, posttransplant bone disease, congestive heart failure, idiopathic scoliosis, prior fracture as an adult, depression, multiple sclerosis, sarcoidosis
• Medications: anticoagulants (heparin), cancer chemotherapeutic drugs, gonadotropin-releasing hormone agonists, anticonvulsants, cyclosporine A and tacrolimus, lithium, aromatase inhibitors, depot medroxyprogesterone, barbiturates, corticosteroids (5 or more mg/d of prednisone or equivalent for 3 or more months)
Reprinted with permission from Clinician's Guide to Prevention and Treatment of Osteoporosis, pages 6-8, 2010 National Osteoporosis Foundation Washington, DC 20037.
All rights reserved. Modified from Bone health and osteoporosis: a report of the Surgeon General. Rockville (MD): Department of Health and Human Services Public Health Service, Office of the Surgeon General; 2004. Available at: http://www.ncbi.nlm.nih.gov/books/NBK45513/pdf/TOC.pdf. Retrieved March 28, 2014. All rights reserved.risk are available to reduce the risk of osteoporosis and reduce the incidence of fracture.
Prevention Counseling
Physical activity, adequate nutrition, and good health are necessary for bone health. The effect of lifestyle and nutrition on bone health should be considered for girls and women of all ages, and patients should be counseled accordingly as part of the annual gynecologic examination. Counseling should include recommending the following preventive measures:
• Adequate calcium and vitamin D consumption—In its 2011 report, the Institute of Medicine (IOM) recommended a dietary allowance for calcium of 1,000 mg/d for adults aged 19-50 years and 1,200 mg/d for adults aged 51 years and older. The IOM's recommendations for vitamin D are 600 international units/d for most of life and 800 international units/d for individuals older than 70 years. Routine screening for vitamin D levels is not recommended in the absence of risk factors for vitamin D deficiency. Whether to recommend supplementation, as opposed to dietary sources, is uncertain. Health care providers are advised to refer to the U.S. Preventive Services Task Force for up-to-date, evidence-based vitamin D supplementation recommendations.
• A minimum of 30 minutes three times per week of weight-bearing exercise on an ongoing basis is recommended to reduce falls and prevent fractures and help to “pad” the bones and provide protection if there is a fall (see also the “Fitness” section earlier in Part 3).
• Smoking cessation (see also the “Substance Use and Abuse” section later in Part 3)
• Moderation of alcohol intake
• Fall prevention strategies, including removal of throw rugs and use of hip protectors, for women prone to falling
Bone Mineral Density Screening
Bone mineral density screening recommendations from the American College of Obstetricians and Gynecologists are shown in Fig.
3-1. Several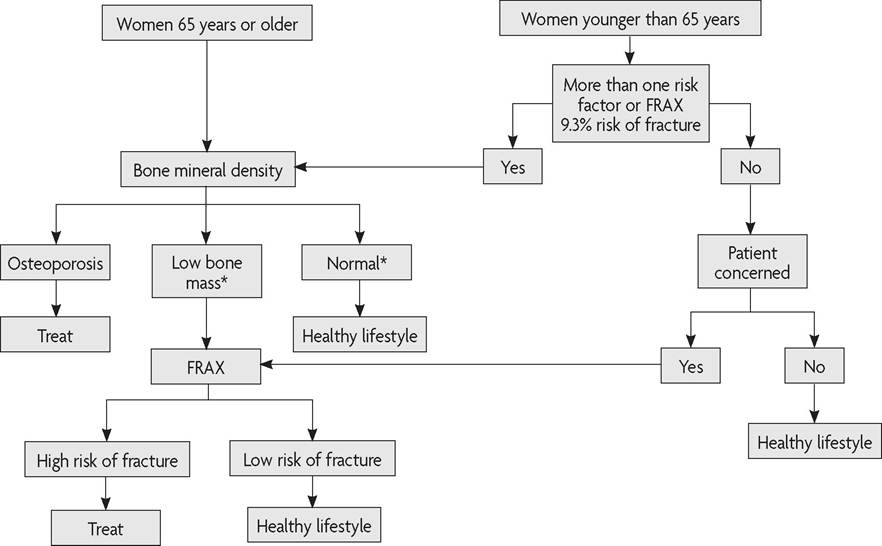
*FragiIity fracture is an indication for treatment despite lack of osteoporosis on DXA.
Fig. 3-1. Screening and treating postmenopausal women for fracture prevention. (Screening and treating premenopausal women is generally restricted to women who have diseases, condition, or medication use known to increase risk of fractures.) Abbreviations: FRAX, fracture risk assessment tool; DXA, dual-energy X-ray absorptiometry. (Reprinted from Osteoporosis. Practice Bulletin No. 129. American College of Obstetricians and Gynecologists. Obstet Gynecol 2012;120:718-34.) (T-score greater than or equal to -1.5), a 5-year screening interval for a T-score from -1.5 to -1.99, and a 1-year screening interval for a T-score between -2.0 and -2.49. The FRAX fracture risk assessment tool, a description of which immediately follows, should continue to be used on an annual basis to monitor the important effect of age on fracture risk.
Fracture Risk Assessment Tool
In 2008, the World Health Organization introduced FRAX to allow clinicians to estimate the 10-year probability of hip and major osteoporotic fractures (forearm, hip, shoulder, or spine) for patients aged 40-90 years
| Table 3-4. Diagnosing Osteoporosis Using Bone Densitometry Criteria Developed by the World Health Organization ^ | |
| Category | T-Score* |
| Normal Low Bone Mass (formerly osteopenia) Osteoporosis | Greater than or equal to -1.0 Less than -1 to greater than -2.5 Less than or equal to -2.5 |
*T-score is the number of standard deviations above or below the mean average bone density value for young adult women.
Reprinted from Osteoporosis. Practice Bulletin No. 129. American College of Obstetricians and Gynecologists. Obstet Gynecol 2012;120:718-34.
Box 3-11. When to Screen for Bone Density Before Age 65 Years
Bone density should be screened in postmenopausal women younger than 65 years if any of the following risk factors are noted:
• Medical history of a fragility fracture
• Body weight less than 127 lb
• Medical causes of bone loss (medications or diseases)
• Parental medical history of hip fracture
• Current smoker
• Alcoholism
• Rheumatoid arthritis
Reprinted from Osteoporosis. Practice Bulletin No. 129. American College of Obstetricians and Gynecologists. Obstet Gynecol 2012;120:718-34.
based on sex, ethnicity, and region of the world (available at www.shef. ac.uk/FRAX). This tool incorporates BMD and clinical risk factors. The clinical risk factors used in FRAX include, age, sex, body mass index, previous fragility fracture, parental hip fracture, current smoking status, corticosteroid use (greater than or equal to 5 mg prednisolone per day for 3 months), alcohol intake greater than or equal to 3 units per day (approximately three drinks), rheumatoid arthritis, and other secondary causes of osteoporosis.
The National Osteoporosis Foundation recommends FRAX be used in women who are postmenopausal, are not receiving osteoporosis treatment, have a T-score indicating low bone mass, and have no prior hip or vertebral fracture. In the United States, FRAX has been most widely used as an aid in decision making regarding treatment initiation when the patient’s BMD score is in the low bone mass range. The fracture risk assessment tool also can be used in women younger than 65 years to determine which women should have a DXA scan. Those women with a FRAX 10-year risk of major osteoporotic fracture of 9.3% or greater could justifiably be referred for DXA because that is the risk of fracture found in a 65-year-old Caucasian woman with no risk factors.
Pharmacologic Interventions
Medical treatment should be recommended for women who have a BMD T-score of less than or equal to -2.5.
For women with a BMD T-score between -1 and -2.5, the FRAX calculator can be used to make an informed decision about the need for treatment (Fig. 3-1). Women who are found to have a 10-year risk of major osteoporotic fracture greater than or equal to 20% or a risk of hip fracture greater than or equal to 3% using the FRAX calculator are candidates for medical pharmacologic therapy. Women who have had a low-trauma fracture (especially of the vertebra or hip) also are candidates for treatment even in the absence of osteoporosis on the DXA report (Fig. 3-1).There are now several pharmacologic options available for osteoporosis prevention, treatment, or both. All of these agents are antiresorptive (slow bone loss) with the exception of parathyroid hormone, which is an anabolic agent (builds new bone).
• Bisphosphonates—These drugs, which can be used for the prevention and treatment of osteoporosis, inhibit resorption of bone by osteoclasts, ultimately leading to an increase in BMD and a decrease in bone turnover. Products are available that can be taken orally (daily, weekly, monthly) or intravenously (quarterly or yearly).
• Selective estrogen receptor modulators—This class of partial estrogen agonists/antagonists reduces the risk of vertebral fractures and is available in daily oral formulation. Raloxifene is approved for osteoporosis prevention and treatment.
• Hormone therapy—Estrogen therapy and combined estrogen and progestogen therapy are approved for the prevention of osteoporosis in women at an increased risk of osteoporosis and fracture (see also the “Menopause” section later in Part 3).
• Parathyroid hormone - Recombinant human parathyroid hormone is an anabolic bone treatment agent that increases trabecular size and connectivity and is administered by subcutaneous injection daily.
• Calcitonin—A naturally occurring hormone, calcitonin reduces fractures but appears to be less effective than other treatment agents. It can be administered by injection (subcutaneous or intramuscular) or nasal spray. In 2013, a U.S. Food and Drug Administration advisory panel reviewed evidence that indicated a potential risk of cancer may outweigh the benefit of fracture prevention. Updated labeling indicates that calcitonin-salmon treatment should be used only in patients for whom alternative treatments are not suitable, and use should be reevaluated on a periodic basis.
• RANK ligand inhibitor—This human monoclonal antibody to the receptor activator of nuclear factor-κβ ligand decreases bone resorption and increases BMD. This medication is administered subcutaneously every 6 months.
Clinicians should take into account patient symptoms and medical history and should weigh the potential benefits and risks when selecting medication for the prevention or treatment of osteoporosis. Pharmacologic treatment should be used in conjunction with dietary modifications and supplements, weight-bearing exercises, and modification of risk factors for falling (see “Prevention Counseling” earlier in this section).
Testing with DXA to assess the effect of treatment generally should not be undertaken before 2 years after initiation of treatment because it often takes 18-24 months to document a clinically meaningful change. If the BMD is improved or stable (no significant change), the DXA does not usually need to be repeated in the absence of new risk factors.
Bibliography
Chen WY, Manson JE, Hankinson SE, Rosner B, Holmes MD, Willett WC, et al. Unopposed estrogen therapy and the risk of invasive breast cancer. Arch Intern Med 2006;166:1027-32. [PubMed] [Full Text]
Chlebowski RT, Hendrix SL, Langer RD, Stefanick ML, Gass M, Lane D, et al. Influence of estrogen plus progestin on breast cancer and mammography in healthy postmenopausal women: the Women's Health Initiative Randomized Trial. WHI Investigators. JAMA 2003;289:3243-53. [PubMed] [Full Text]
Depot medroxyprogesterone acetate and bone effects. Committee Opinion No. 602. American College of Obstetricians and Gynecologists. Obstet Gynecol 2014;123:1398-402. [PubMed] [Obstetrics & Gynecology]
Food and Drug Administration. Questions and answers: changes to the indicated population for miacalcin (calcitonin-salmon). Available at: http://www.fda.gov/ Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ ucm388641.htm. Retrieved April 10, 2014.
Gourlay ML, Fine JP, Preisser JS, May RC, Li C, Lui LY, et al. Bone-density testing interval and transition to osteoporosis in older women. N Engl J Med 2012; 366:225-33. [PubMed] [Full Text]
Hormone therapy. American College of Obstetricians and Gynecologists. Obstet Gynecol 2004;104 (suppl):1S-129S.
Kanis JA, Johnell O, Oden A, Johansson H, McCloskey E. FRAX and the assessment of fracture probability in men and women from the UK. Osteoporos Int 2008;19:385-97. [PubMed] [Full Text]
Looker AC, Borrud LG, Dawson-Hughes B, Shepherd JA, Wright NC. Osteoporosis or low bone mass at the femur neck or lumbar spine in older adults: United States, 2005-2008. NCHS Data Brief 2012;(93):1-8. [PubMed]
Management of osteoporosis in postmenopausal women: 2010 position statement of The North American Menopause Society. Menopause 2010;17:25-54; quiz 55-6. [PubMed]
Moyer VA. Prevention of falls in community-dwelling older adults: U.S. Preventive Services Task Force recommendation statement. U.S. Preventive Services Task Force. Ann Intern Med 2012;157:197-204. [PubMed] [Full Text]
Moyer VA. Vitamin D and calcium supplementation to prevent fractures in adults: U.S. Preventive Services Task Force recommendation statement. U.S. Preventive Services Task Force. Ann Intern Med 2013;158:691-6. [PubMed] [Full Text] National Osteoporosis Foundation. Clinician's guide to prevention and treatment of osteoporosis. Washington, DC: NOF; 2013. Available at: http://www.nof.org/ files/nof/public/content/file/2237/upload/878.pdf. Retrieved August 29, 2013.
Osteoporosis prevention, diagnosis, and therapy. NIH Consensus Development Panel on Osteoporosis Prevention, Diagnosis, and Therapy. JAMA 2001;285: 785-95. [PubMed] [Full Text]
Osteoporosis. Practice Bulletin No. 129. American College of Obstetricians and Gynecologists. Obstet Gynecol 2012;120:718-34. [PubMed] [Obstetrics & Gynecology]
Ross AC, Manson JE, Abrams SA, Aloia JF, Brannon PM, Clinton SK, et al. The 2011 report on dietary reference intakes for calcium and vitamin D from the Institute of Medicine: what clinicians need to know. J Clin Endocrinol Metab 2011;96:53-8. [PubMed] [Full Text]
Screening for osteoporosis: U.S. preventive services task force recommendation statement. U.S. Preventive Services Task Force. Ann Intern Med 2011;154:356-64. [PubMed] [Full Text]
The 2012 hormone therapy position statement of the North American Menopause Society. North American Menopause Society. Menopause 2012;19:257-71. [PubMed] [Full Text]
Resources
American College of Obstetricians and Gynecologists. Osteoporosis. Patient Education Pamphlet AP048. Washington, DC: American College of Obstetricians and Gynecologists; 2013.
American College of Obstetricians and Gynecologists. The menopause years. Patient Education Pamphlet AP047. Washington, DC: American College of Obstetricians and Gynecologists; 2013.
World Health Organization Collaborating Centre for Metabolic Bone Diseases. WHO Fracture Risk Assessment Tool (FRAX). Sheffield, United Kingdom: University of Sheffield; 2013. Available at: http://www.shef.ac.uk/FRAX/. Retrieved September 30, 2013.