SEXUAL FUNCTION AND DYSFUNCTION ^xv ^221 ^501 ^527
Sexuality involves a broad range of expressions of intimacy and is fundamental to self-identification, with strong cultural, biologic, and psychologic components. There is a range of sexual practices that are normal, and different cultures have their own definitions of normal.
It is necessary for clinicians to understand the sexual response pattern and the variations of these responses to assist in the identification and treatment of patients with sexual dysfunction.Sexual Function
Most clinicians are familiar with the traditional human sexual response cycle of Masters, Johnson, and Kaplan. This model depicts a linear sequence of discrete events: desire, arousal, plateau, orgasm, and resolution (see Fig. 4-4). However, the usefulness of this model for depicting women’s sexuality is limited. Sexual response in women is complex, and events do
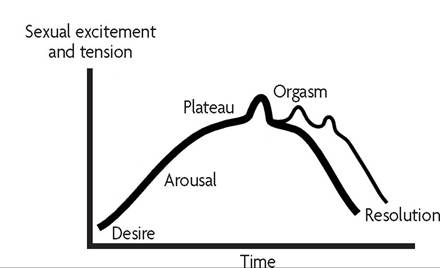
Fig. 4-4. Traditional sexual response cycle of Masters, Johnson, and Kaplan. (Reprinted from Basson R. Female sexual response: the role of drugs in the management of sexual dysfunction [published erratum appears in Obstet Gynecol 2001;98:522]. Obstet Gynecol 2001;98:350-3.)
not always occur in a predictable sequence, as they usually do in men. A woman’s sexuality is influenced by her health and emotional well-being; likewise, healthy sexual functioning promotes physical and emotional well-being. An alternate model of women’s sexual response (see Fig. 4-5) depicts the many sexual motivations, sexual stimuli, and psychologic and biologic factors that govern the processing of those stimuli, thus determining the woman’s arousability.
Studies suggest that fewer than one half of patients’ sexual concerns are recognized by their physicians. The obstetrician-gynecologist has an important role in assessing sexual function because many women view their sexuality as an important quality-of-life issue that frequently is affected by reproductive events.
Clinicians should not make assumptions or judgments about the woman’s behavior and, when counseling patients, should keep in mind the possibility of cultural and personal variation in sexual practices.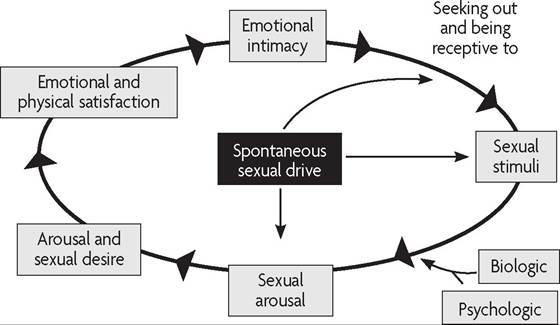
Fig. 4-5. Nonlinear model of female sexual response developed by Basson. Basson's nonlinear model acknowledges how emotional intimacy, sexual stimuli, and relationship satisfaction affect female sexual response. (Modified from Basson R. Female sexual response: the role of drugs in the management of sexual dysfunction [published erratum appears in Obstet Gynecol 2001;98:522]. Obstet Gynecol 2001;98:350-3.)
Sexual Dysfunction
Female sexual dysfunction encompasses a number of conditions that cause disturbance in a woman’s sexual response. The adverse effect of female sexual dysfunction on the quality of life of affected women can extend into interpersonal relationships and the workplace. Sexual dysfunction of one type or another is common and experienced by most women at some time in their lives. Although female sexual dysfunction is prevalent, it often is neglected in the health care setting because women are unlikely to discuss it with their health care providers unless asked. Health care providers can convey to patients that it is appropriate to discuss sexual concerns by integrating the topic of sexual dysfunction into office visits.
Etiology
Sexual dysfunction may be related to emotional issues (eg, relationship difficulties, past sexual abuse), psychologic problems (eg, depression, anxiety, poor body image), physical impairment or illness, medications, alcohol or drug use, or biologic factors (eg, fatigue). The subtypes lifelong or acquired and generalized or situational are used in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), to designate the development and course of symptoms.
Numerous medications (both prescription and over-the-counter) and substances (such as illicit drugs and alcohol) have been associated with sexual dysfunction.
Psychotropic medications, antihypertensives, histamine blockers, and hormonal contraceptives also have been implicated. The most common medications linked to sexual dysfunction are the selective serotonin reuptake inhibitors. The most frequently reported problems are orgasmic dysfunction, decreased sexual desire, and decreased arousal.Emotional issues can be the basis for sexual dysfunction. The physician should attempt to identify any factors that could affect sexual function and provide education and counseling about them. Events from the past, such as childhood inhibitions or sexual abuse, can affect sexual function. Patients with complex sexual problems of a psychologic nature may benefit from referral to a mental health professional. When emotional problems clearly are limited to unsatisfactory sexual experiences, referral to a qualified sex therapist is appropriate. If the difficulty involves issues other than sexuality, referral to a counselor skilled in marital and other relationship problems may be preferable. Individuals with sexual dysfunction that results from a history of sexual victimization should be referred to mental health professionals with an expertise in abuse-related problems.
Male factors include low desire and erectile dysfunction, which may be based on organic or psychologic factors. Acknowledgment and support from the woman’s physician may assist the patient in helping her partner seek counseling and treatment.
Evaluation
The initial approach to the evaluation of a patient who presents with a possible sexual dysfunction disorder begins with obtaining a sexual history during the review of symptoms. Taking a thorough sexual history includes recording the patient’s medical, surgical, social, and psychiatric history. Information about the use of prescription and over-the-counter medications and other substances should be elicited. If an examination is performed, the patient should be informed of what it will entail. The presence of a chaperone is recommended during examination, regardless of the gender of the health care provider, but privacy during history-taking may elicit more thorough responses.
The clinician should be prepared to discuss patients’ concerns about sexual function in a setting of mutual respect and trust. A nonjudgmen- tal and respectful approach by the clinician, as well as awareness by the clinician of his or her own biases—and the active attempt to counteract them—is essential for effective care. Patients are more likely to develop trusting relationships with their health care providers when the issue of confidentiality has been addressed directly. A confidential relationship, in turn, can facilitate the open disclosure of health histories and behaviors. The clinician should not make assumptions about the gender of the woman’s partner. Although most women report that their sexual partners are men, some women have sex only with other women, and others may have partners of both sexes. The use of terms such as partner instead of husband and sexual activity instead of sexual intercourse and an understanding of nonheterosexual sexuality will assist in open communication and assessment of any difficulties (see also the “Lesbians and Bisexual Women” section in Part 3).
The use of broad, open-ended questions in a routine history gathering can help disclose problems that require further exploration. The following are examples of basic questions, posed in a gender-neutral fashion:
• “Are you sexually active?”
• “Are you sexually satisfied?”
• “Do you have questions or concerns about sexual functioning?”
• “Do you think your partner is satisfied?”
Inquiry about the partner’s sexual function and level of satisfaction may elicit more specific information and give an indication of the couple’s level of communication. Deliberate inquiries should be made to assess the quality of the interpersonal relationship between the patient and her partner, including mutual satisfaction with their sexual relationship. After asking general questions, it may be helpful to ask additional pointed questions, such as the following:
• “Do you have orgasms?”
• “Are you satisfied with the frequency of sexual activity?”
• “Does your vagina lubricate enough?”
This will delineate better the exact nature of a patient’s dysfunction.
Difficulties with prior sexual experience, insufficient foreplay, and attitudes about sexual pleasure can be elicited with careful history taking. For example, difficulties reaching orgasm or markedly reduced intensity of orgasmic sensations may not be a problem unless the patient or partner perceives it to be.Classification and Diagnosis
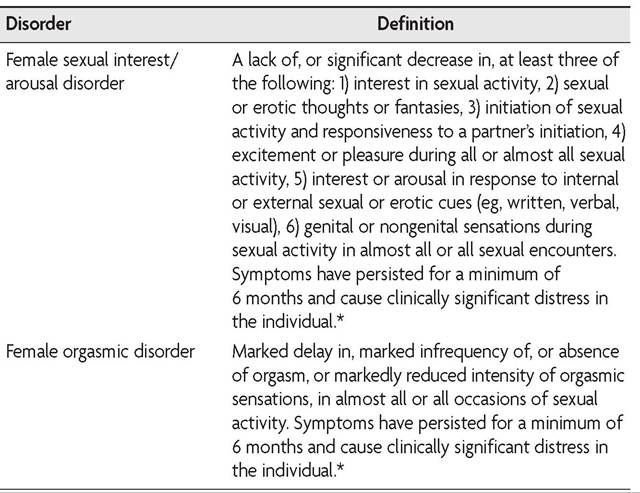
The DSM-5 identifies four specific types of female sexual dysfunction: 1) female sexual interest/arousal disorder, 2) female orgasmic disorder, 3) genito-pelvic pain/penetration disorder (a new classification that merges and expands on the DSM-IV-defined disorders of vaginismus and dyspareunia), and 4) substance/medication-induced sexual dysfunction (Table 4-5). In addition, the DSM-5 also classifies disorders as other specified sexual dysfunction and unspecified sexual dysfunction, and the authors of the DSM-5 note that other factors, such as inadequate sexual stimulation or nonsexual mental or physical disorders, may explain sexual dysfunction as well. For example, atrophic vaginitis after spontaneous menopause or oophorectomy may cause pain with vaginal penetration and difficulties in lubrication that impair sexual arousal. Women often experience more than one type of sexual function disorder.
A diagnosis of one of the DSM-5-classified female sexual dysfunctions is made when symptoms persist for at least 6 months (except in the case of substance/medication-induced sexual dysfunction) and are sufficient to result in significant personal distress. In addition, diagnosis requires that the symptoms are not better explained by a nonsexual mental disorder, a medical condition, severe relationship distress or other significant life stressors, or the effects of a substance or medication (except in the case of substance/medication-induced sexual dysfunction).
Table 4-5. Types of Female Sexual Dysfunction
(continued)
Table 4-5.
Types of Female Sexual Dysfunction (continued)| Disorder | Definition |
| Genito-pelvic pain/ penetration disorder | The persistent or recurrent presence of one or more of the following symptoms: 1) difficulty having intercourse, 2) marked vulvovaginal or pelvic pain during intercourse or penetration attempts, 3) marked fear or anxiety about vulvovaginal or pelvic pain anticipating, during, or resulting from vaginal penetration, and 4) marked tensing or tightening of the pelvic floor muscles during attempted vaginal penetration. Symptoms have persisted for a minimum of 6 months and cause clinically significant distress in the individual.* |
| Substance/medication- induced sexual dysfunction | A disturbance in sexual function that has a temporal relationship with substance/medication initiation, dose increase, or substance/medication discontinuation and causes clinically significant distress in the individual.1 |
*A diagnosis of a sexual dysfunction disorder can be made only if the sexual dysfunction is not better explained by a nonsexual mental disorder or as a consequence of severe relationship distress (eg, partner violence) or other significant stressors and is not due to the effects of a substance or medication or another medical condition.
1The disturbance is not better explained by an independent sexual dysfunction disorder. Evidence that suggests a nonsubstance/medication-induced sexual disorder includes a history of an independent sexual dysfunction disorder, symptoms that precede the onset of substance or medication use, or symptoms that persist for at least 1 month after cessation of acute withdrawal or severe intoxication.
Data from American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-5. 5th ed. Washington, DC: APA; 2013.
Management
Management of sexual dysfunction will vary with the type of dysfunction, although many types of dysfunction are related. In general, sexual dysfunction involves the couple, and therapy should be with both partners. However, even if an individual has a specific problem, it still may be appropriate for the partner to be involved in therapy. Some treatments for sexual dysfunction may be within the scope of the obstetrician-gynecologist. If not, referrals to mental health practitioners, marriage or relationship counselors, or sex therapists are appropriate.
Female Sexual Interest/Arousal Disorder
For women with a reduced or absent sexual interest or arousal, sensate focus exercises can help couples develop verbal and nonverbal means to communicate with each other to improve satisfaction. Studies have found transdermal testosterone to be effective for the short-term treatment of low sexual desire in women, with little evidence to support long-term use (longer than 6 months). However, testosterone is not approved by the U.S. Food and Drug Administration for this treatment.
Female Orgasmic Disorder
Behaviorally oriented, time-limited treatment programs for previously anorgasmic women have been described. Behavioral treatments include masturbation instruction, communication exercises, sensate focus exercises, and systematic desensitization. Psychotherapy and couples counseling and support groups of women with similar problems may be helpful. After counseling, self-stimulation techniques may be beneficial for the patient. Recently, surgical procedures, such as “vaginal rejuvenation” or “G-spot amplification” have been promoted as a means of enhancing sexual satisfaction. Often, the exact procedure performed is not clear because standard medical nomenclature is not used. Such procedures are not medically indicated, and their safety and effectiveness have not been documented (see also the “Ambulatory Gynecologic Surgery” section later in Part 4).
Genito-Pelvic Pain/Penetration Disorder
Effective treatment of fear of pain with vaginal penetration consists of psychotherapy and behavior modification called desensitization, which gradually allows patients to overcome their fear by using sequential vaginal dilators of increasing diameter. Pelvic floor physical therapy can also effectively address pain and tensing or tightening of the pelvic floor muscles associated with vaginal intercourse.
Sexual dysfunction increases as women age, even in the absence of measurable physiologic changes or a specific diagnosis of genito-pelvic pain/penetration disorder. After menopause, women often report a lack of vaginal lubrication that makes intercourse painful. The use of vaginal estrogen and lubricants can ease the problem. Although more common in the elderly, women of any age may experience this problem, particularly women with relatively lower estrogen levels, such as women who lactate or women who use depot medroxyprogesterone acetate for contraception.
Substance/Medication-Induced Sexual Dysfunction
When medications result in sexual dysfunction, the medication or dosage may need to be changed or eliminated. Couples should be counseled about the effects of illness or medication on sexuality and be encouraged to experiment with alternative forms of sexual expression to accommodate physical limitations. Female sexual dysfunction that is linked to the use of certain medications (eg, selective serotonin reuptake inhibitors) typically resolves when the medication is adjusted. Consultation with a health care provider with expertise in psychiatric medications who can assist in distinguishing baseline female sexual dysfunction from dysfunction that results from treatment of depression may be helpful. A medication adjustment with longterm follow-up may be important for improved sexual functioning.
Bibliography
American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-5. 5th ed. Washington, DC: APA; 2013.
Basson R. Female sexual response: the role of drugs in the management of sexual dysfunction [published erratum appears in Obstet Gynecol 2001;98:522]. Obstet Gynecol 2001;98:350-3. [PubMed] [Obstetrics & Gynecology]
Basson R. Sexuality and sexual disorders. Clin Update Womens Health Care 2003; II(2):1-94.
Brotto LA, Bitzer J, Laan E, Leiblum S, Luria M. Women's sexual desire and arousal disorders [published erratum appears in J Sex Med 2010;7:856]. J Sex Med 2010; 7:586-614. [PubMed] [Full Text]
Drugs that cause sexual dysfunction: an update. Med Lett Drugs Ther 1992;34:73-8. [PubMed]
Female sexual dysfunction. Practice Bulletin No. 119. American College of Obstetricians and Gynecologists. Obstet Gynecol 2011;117:996-1007. [PubMed] [Obstetrics & Gynecology]
Hayes RD, Bennett CM, Fairley CK, Dennerstein L. What can prevalence studies tell us about female sexual difficulty and dysfunction? J Sex Med 2006;3:589-95. [PubMed]
Kennedy SH, Rizvi S. Sexual dysfunction, depression, and the impact of antidepressants. J Clin Psychopharmacol 2009;29:157-64. [PubMed]
Resources
American Association for Marriage and Family Therapy, 112 South Alfred Street, Alexandria, VA 22314. (703) 838-9808. http://www.aamft.org. Retrieved August 12, 2013.
American Association of Sexuality Educators Counselors and Therapists. Available at: http://www.aasect.org. Retrieved August 12, 2013.
American College of Obstetricians and Gynecologists, District II. Finding solutions for female sexual dysfunction. Albany (NY): American College of Obstetricians and Gynecologists, District II; 2010. Available at: http://mail.ny.acog.org/website/ FSDResourceGuide.pdf. Retrieved September 14, 2013.
American College of Obstetricians and Gynecologists. Your sexual health. Patient Education Pamphlet AP072. Washington, DC: American College of Obstetricians and Gynecologists; 2010.
Association of Reproductive Health Professionals. Clinician competencies for sexual health. Washington, DC: ARHP; 2010. Available at: http://www.arhp.org/upload Docs/SHF_Competencies.pdf. Retrieved August 12, 2013.
Haefner HK, Collins ME, Davis GD, Edwards L, Foster DC, Hartmann ED, et al. The vulvodynia guideline. J Low Genit Tract Dis 2005;9:40-51. [PubMed] [Full Text] Health care for lesbians and bisexual women. Committee Opinion No. 525. American College of Obstetricians and Gynecologists. Obstet Gynecol 2012;119:1077-80. [PubMed] [Obstetrics & Gynecology]
Health care for transgender individuals. Committee Opinion No. 512. American College of Obstetricians and Gynecologists. Obstet Gynecol 2011;118:1454-8. [PubMed] [Obstetrics & Gynecology]
International Society for Sexual Medicine. Available at: http://www.issm.info. Retrieved September 14, 2013.
Kingsberg SA, Iglesia CB, Kellogg S, Krychman ML. Handbook on female sexual health and wellness. Washington, DC: Association of Reproductive Health Professionals; 2011. Available at: http://www.arhp.org/uploadDocs/ARHP_ACOG_ SexualityHandbook.pdf. Retrieved September 19, 2013.
Society for Sex Therapy and Research. Available at: http://www.sstarnet.org. Retrieved September 14, 2013.
Vulvodynia. ACOG Committee Opinion No. 345. American College of Obstetricians and Gynecologists. Obstet Gynecol 2006;108:1049-52. [PubMed] [Obstetrics & Gynecology]