ACUTE OSTEOMYELITIS
Osteomyelitis in children primarily involves long bones of the lower or upper limbs. It is more common in males and ~1/3 cases occur lt;2 years of age.
Etiology: Staph. aureus is the commonest causative organism for acute osteomyelitis, followed by Streptococci, Pneumococci and H.
influenzae. Gram negative or anaerobic osteomyelitis is common in posttraumatic infections. Osteomyelitis in sickle cell anemia is usually due to salmonella and H. influenzae.Pathogenesis: Infection is usually acquired via hematogenous route following septicemia from a distant focus, or direct inoculation after neighboring injuries/surgeries.
Metaphyses of long bones are commonest sites for localization of blood-borne infection, due to typical vascular anatomy, i.e. sinusoidal network with sluggish blood flow. From here, infection may spread to diaphysis and subperiosteal space through Haversian system and Volkmann canals. Although epiphyseal plate limit extension of infection into joint space, co-arthritis is common in infants due to criss-crossing capillaries.
Chronic osteomyelitis is pathologically characterized by formation of abscess (Brodie's abscess), sequestrum (dead bone tissue), sub-periosteal involucrum (reparative bone tissue) and occasionally, sinus tracts to discharge the pus on skin surface. Weakened bone at the site of these changes is susceptible for pathological fractures.
Clinically, early osteomyelitis may be asymptomatic till the infection extends beyond metaphysis, while an established case presents with: (a) local inflammation, e.g. pain, tenderness, swelling and restricted movements of affected site, and (b) constitutional features, e.g. fever.
Constitutional signs are minimal in chronic osteomyelitis, which usually presents with chronic discharging sinuses and pathological fractures at the site of lesion. Diagnosis: Radio nucleotide bone scan (99mTc) or MRI of the suspected site is the best investigation for diagnosis of early osteomyelitis, as X-ray changes appear only after 7-10 days.
On X-rays, periosteal elevation over metaphysis is the earliest sign, followed by irregularity of cortex, abnormal diaphyseal densities (sequestrum), subperiosteal bone formation (involucrum) with sequestrum formation in more chronic cases (Fig.
23.10).Ultrasonography to exclude co-existing arthritis and Blood/pus cultures for specific antibacterial therapy are indicated in all cases, though ~1/3rd cases are sterile at the time of diagnosis.
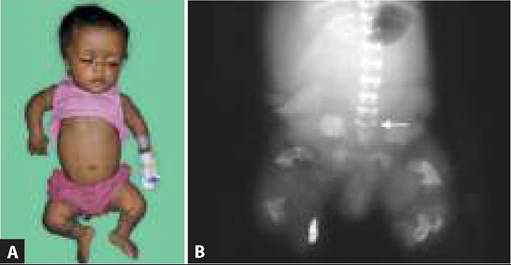
Fig. 23.10: Osteomyelitis: Arrows indicate sequestrum.
Treatment of osteomyelitis includes:
a. Antibiotics: Vancomycin (or Cloxacillin) with a third generation cephalosporin is the drug of choice for empirical therapy till culture reports. Vancomycin is preferred in settings with high MRSA resistance. Clindamycin may be used in cases allergic to betalactam drugs. It is also effective against anaerobic infections common after penetrating injuries or compound fractures. Initial therapy is essentially intravenous, which may be switched to oral antibiotics after 7-10 days in good responders and continued for minimum 14-21 days or till resolution.
b. Surgical intervention is indicated in cases with arthritis (pus drainage) or chronic osteomyelitis (curettage and removal of sequestrum).
c. Limb immobilization (splinting/cast) is useful in select cases to reduce pain and restrict movements, which may facilitate spread of infection or cause pathological fractures. However, passive physiotherapy should begin as soon as pain subsides.
Outcome depends on severity/duration of osteomyelitis and promptness of therapy. Chronic osteomyelitis may lead to pathological fractures, deformities and limb shortening.
23.5.2