ASPIRATION AND BIOPSY PROCEDURES
This sub-chapter deals with some common diagnostic or therapeutic aspiration/biopsy procedures in children.
Lumbar puncture (LP) is a common procedure for the diagnosis and treatment of various neurological disorders.
Indications:
• Diagnostic CSF examination for:
- Meningitis, encephalitis, subarachnoid hemorrhage
- D/d acute poliomyelitis vs. Guillain-Barre syndrome
- CNS involvement in septicemia, leukemia, etc.
• Therapeutic CSF drainage in raised ICP,
• Intrathecal drug administrations, e.g. methotrexate, tetanus immunoglobulins, etc.,
Fig. 32.20: Lumbar puncture.
• Intrathecal contrast injections during myelography, CT scan, etc.
• Spinal anesthesia.
Contraindications:
• Raised ICP with papilledema*, due to risk of sudden brain coning/herniation,
• Local skin infection over the LP site, and
• Abnormal coagulation profile or thrombocytopenia lt;20,000/mm3.
*If unavoidable, a guarded LP with attached manometer may be performed after mannitol infusion in these cases.
Prerequisites: (a) informed written consent, (b) fundus examination, to exclude papilledema.
Instrument (LP needle): LP needle is a stainless steel needle with two major parts: (a) main hollow needle with beveled end, relatively malleable body and thick grooved/notched base, and (b) inner stiletto with a small knob that fits into groove of main needle (Fig. 32.20). Although available in various sizes (No. 18-24), only no. 23 and 24 LP needles are used in children. A disposable IV needle (G 20-21) may also be used in children instead of specific LP needles, if required.
Uses: (a) lumbar puncture, (b) ventricular or cisternal puncture, (c) pericardial, pleural or peritoneal tapping, (e) fine needle aspiration cytology (FNAC).
Sterilization: Autoclaving, though disposable LP needles are also available.
LP Site: Inter-vertebral space between L 4-5 or 3-4, in midline.
Procedure: Lateral decubitus position with maximally flexed spine is preferred, though sitting position may be used in some cases. Important steps include:
Restrain and position the child gt; clean the site with an antiseptic gt; drape the surrounding area gt; palpate the desired space, gt; insert the needle (with stylet, if LP needle is used) slowly, in midline directed 10-15 cephalad, till sudden loss of dural resistance gt; look for CSF outflow after removing the stylet gt; collect 2 ml of CSF gt; withdraw the needle gt; seal with tincture benzoin. Patient should be kept in head-low position for few hours.
Complications are rare after LP except:
• Post-procedure headache for 6-8 hours
• Sudden death due to coning of brain-stem in cases with raised ICP,
• Iatrogenic meningitis (exogenous infection), and
• Local inclusion dermoid after many years.
Note that:
• A dry tap indicates faulty technique or subarachnoid block. In such case, procedure should be repeated in a higher intervertebral space.
• A hemorrhagic tap may be due to local trauma or sub-arachnoid hemorrhage. Traumatic CSF is more bloody in the beginning and clears gradually (Three- test tube test).
Subdural tap is indicated for etiological diagnosis or therapeutic drainage in subdural effusions, empyema or hematoma in children with open anterior fontanel.
Procedure: A disposable 21 G IV needle or LP needle is used for this purpose, with following steps:
Shave the scalp gt; restrain the child gt; clean the scalp with antiseptic and drape it gt; palpate anterior fontanel and mark its lateral angles gt; slowly introduce the needle at one of the lateral most angle perpendicular to the scalp (Fig. 32.21), till a feel of give-away is obtained as dura is pierced and subdural fluid starts flowing gt; collect the sample without aspiration by a syringe gt; withdraw the needle gt; apply firm pressure over the site for 2-3 minutes and seal the site gt; repeat the procedure on other side with a separate needle, even if first tap is dry.
Complications: (a) transient CSF leak, (b) hemorrhage,
(c) infection, and (d) porencephaly, if brain tissue was punctured.
Fig. 32.21: Site for subdural or ventricular tap.
Ventricular tap is usually indicated to collect CSF sample for diagnosis/exclusion of ventriculitis in:
(a) non-resolving meningitis, (b) before VP shunt in hydrocephalus. Shunt block is likely in presence of ventriculitis with high CSF protein/cell content.
Procedure is similar to subdural tapping, except that—(a) longer needle is used due to greater depth of ventricles, and (b) needle is directed towards the inner canthus of ipsilateral eye rather than at 90°.
Bone marrow aspiration is commonly used to obtain marrow sample for diagnostic/therapeutic purpose. An alternative method - Trephine biopsy may be required in cases with dry bone marrow aspiration.
Indications: Diagnostic bone marrow aspiration is indicated in suspected:
• Aplastic anemia.
• Leukemia or other malignancies (for staging).
• Chronic refractory anemia, e.g. megaloblastic anemia.
• Hemo-parasitic infestations, e.g. malaria/kala-azar.
• Chronic immune thrombocytopenic purpura.
• Primary marrow disease, e.g. myelofibrosis.
• Metabolic storage disorders, e.g. Gaucher disease.
Repeated aspiration is necessary in many cases to assess the therapeutic response.
Contraindications: (a) severe bleeding tendency,
(b) local infection, e.g. osteomyelitis (use other sites).
Instrument (bone marrow aspiration needle): Bone marrow aspiration needle is a short (4-6 cm), thick, stout, non-flexible, stainless steel needle with three important parts: (a) main needle, (b) trochar with a knob on external end, and (c) adjustable guard (Fig. 32.22). The guard prevents accidental excess penetration of the bone and deeper tissue injuries during insertion.
Bdim r#8719;j3rr?#8539;, aspiration n#960;crl#953;, Fig.
32.22: Bone marrow aspiration.Uses: (a) diagnostic marrow aspiration, (b) intraosseous cannulation for emergency fluid/drug therapy, and
(c) bone marrow transplant.
Pre-requisites: (a) informed consent, (b) normal coagulation profile and platelet count.
Sites: The choice of bone marrow aspiration site depends on the patient's age as follows:
a. Tibial tuberosity in children lt;2 years,
b. Anterior superior iliac spine or iliac crest in older children and
c. Mid-manubrium sternii (sternal puncture), if other two options are not possible.
Procedure for marrow aspiration include:
Clean the selected site with antiseptic gt; drape the surrounding area gt; local anesthesia with 2% xylocaine, though not necessary in very young children, gt; adjust the guard at nearly 1.5 cm from the tip, gt; palpate the precise site gt; insert the needle (with stylet) with boring action, till resistance is felt gt; remove the stylet gt; connect a syringe and aspirate 0.5-1.0 ml of bone marrow
gt; withdraw the needle gt; seal the site with Tinc. benzoin
gt; prepare smears.
Complications: While local pain and tenderness is inevitable for 24-48 hours, important complications include: (a) local bleeding and hematoma, (b) trauma to deeper structures, and (c) infection, e.g. osteomyelitis.
Dry tap indicates: (a) faulty technique, (b) severely aplastic bone marrow, (c) primary marrow disease, e.g. myelofibrosis or myelosclerosis, or (d) severe marrow infiltration, e.g. in malignancies. Trephine biopsy, using Jamshidi-Swain needle is indicated in these cases.
Liver biopsy is commonly used for histological diagnosis and/ or follow-up of primary or secondary liver disorders.
Indications: Diagnostic liver biopsy is indicated in:
• Chronic liver disease or cirrhosis.
• Metabolic, storage or infiltrative liver disorders.
• Unexplained persistent icterus or abnormal liver function tests.
• Suspected primary or secondary malignancy.
Serial biopsies are indicated for evaluation of therapeutic response in chronic liver diseases.
Contraindications include:
• Acute liver failure.
• Bleeding disorders.
• Tense ascites or peritonitis.
• Local infection, e.g. subphrenic abscess.
• Congestive hepatomegaly.
• Suspected vascular malformations* of liver
• Suspected hydatid disease*
(*absolute contraindications)
Pre-requisites: (a) informed consent, (b) coagulation profile*, (c) pre-procedure sedation and vagolytic agents,
Fig. 32.23: Liver biopsy.
(d) pre-procedure ascetic tapping, if present, (d) blood grouping and cross-matching.
*Normal prothrombin time is an essential prerequisite for liver biopsy and all cases with abnormal PTT should receive three doses of IM Vitamin K (5 mg/dose) for normalization of coagulation profile with/without fresh frozen plasma just before biopsy.
Pre-procedure vagolytic agent, e.g. IV atropine and sedation, e.g. phenobarbitone or chloral hydrate are indicated ~30 minutes before the procedure to reduce pain, anxiety and risk of vagal shock.
Instruments: Three types of needles are used for liver biopsy: (a) tru-cut needle, (b) vim silverman needle, and (c) menghini's aspiration needle. While Tru-cut needle is least traumatic and preferred choice, Vim Silverman needle is frequently used due to advantage of less failure rate and getting large liver tissue. Menghini's needle is rarely used in pediatric practice. Both needles are autoclavable or disposable. Liver biopsy needles can also be used for kidney and lung biopsy.
• Tru cut needle is a long, non-flexible metallic needle with two parts: (a) outer hollow needle with handle, and (b) inner solid needle with a gutter for biopsy tissue (Fig. 32.23).
• Vim Silverman needle is a long, non-flexible metallic needle with three parts: (a) cannula, i.e. outer hollow needle, (b) trochar, i.e. inner solid needle, and (c) bifid needle for cutting the liver tissue (Fig. 32.23).
Site: 9th-10th intercostal space in mid-axillary line after confirmation of liver dullness is preferred, though subcostal approach is used in select cases under ultrasonographic guidance.
Procedure: Important steps in liver biopsy by Vim- Silverman needle are as follows:
Restrain and position the patient in supine position on the edge of the bed with arms under head gt; clean the selected site with an antiseptic gt; drape the surrounding area gt; infiltrate 1-2% xylocaine for local anesthesia, gt; palpate the desired space gt; ask the patient to hold
the breath gt; insert the cannula with trochar for ~ 2 cm depth gt; remove the trochar, gt; insert the forked cutting needle through cannula for ~ 5 mm longer depth gt; rotate the bifid needle at 360° to cut the liver tissue gt; advance the cannula over needle gt; withdraw whole assembly
gt; transfer the tissue between two blades of forked needle into preservative, e.g. formalin gt; seal the site with tincture benzoin.
Similar procedure is adopted by tru-cut needle except that - insert outer hollow needle with solid needle inside, till liver is penetrated gt; advance inner needle further into liver tissue for ~1 cm to collect the tissue sample in the gutter gt; advance outer needle to cover the gutter
gt; withdraw whole assembly.
Failed liver biopsy indicates: (a) wrong technique, or (b) tough liver tissue, e.g. cirrhosis.
Complications include:
• Vagal shock during procedure,
• Local hematoma,
• Internal tissue injury or hemorrhage
• Infections, e.g. cholangitis/liver abscess and
• Precipitation of hepatic encephalopathy.
Post-procedure, the child should be observed for at least 24 hours for: (a) vital signs, (b) abdominal distension, (c) local hematoma formation, (d) signs of internal hemorrhage. A mild/anti-inflammatory agent may be given to reduce the pain and local inflammation.
Renal biopsy: Being an invasive procedure, renal biopsy is indicated only in selected cases with unexplained pathology, where precise diagnosis is essential for therapy/prognosis.
Indications include:
• Steroid-resistant nephrotic syndrome,
• Before starting calcineurin inhibitors therapy,
• Unexplained progressive/chronic renal failure,
• Unexplained/persistent hematuria or proteinuria,
• Suspected inherited/metabolic renal disease,
• Follow-up in chronic renal disease or renal transplant.
Contraindications include:
• Solitary functioning or ectopic kidney,
• Bleeding diathesis,
• Severe acute renal failure,
• Severe hypertension.
Procedure: A tru-cut needle or Vim-Silverman needle with Franklin modification is used for renal biopsy. Preprocedure ultrasonographic localization of kidney (~2 cm below and medial to tip of 12th rib), is must before the procedure, as also the vagolytic/sedative medications. Important steps include:
Restrain and position the patient in prone position with head turned on one side and a rolled-up towel under abdomen gt; clean the USG marked site with an antiseptic gt; drape the surrounding area gt; local anesthesia with 1-2% xylocaine, gt; palpate the desired site gt; ask the patient to hold the breath gt; insert a 21 G long Needle (~8 cm) till kidney is pierced and needle moves with respiration (confirms the position) gt; mark the depth on needle and withdraw it gt; insert tru-cut or Vim Silvermann needle from the same track for similar depth gt; biopsy the tissue with procedure similar to that discussed for liver biopsy gt; withdraw whole assembly gt; transfer the collected tissue in proper preservatives* gt; seal the site with tincture benzoin.
*Obtained material should be sent for routine microscopic histology (in formalin), electron microscopy (in glutaraldehyde) and immunofluorescent studies (in saline).
Complications: Although transient microscopic hematuria for next 24-48 hours is inevitable after renal biopsy, other complications include:
• Persistent/gross hematuria
• Perirenal hematoma
• Renal or perinephric infection.
Complete bed rest and BP/output monitoring is essential for first 24 hours, to detect/treat complications. Thoracocentesis is a common diagnostic/therapeutic procedure to obtain pleural fluid in effusions/empyema. Indications: (a) diagnostic aspiration of fluid in suspected pleural effusion/empyema, (b) therapeutic drainage of large pleural collections, (c) rarely, to insert intra peural medications, e.g. antibiotics and steroids. Site: Upper edge of lower rib in 7th or 8th intercostals space in posterior axillary line (Fig. 32.24). Lower edge of the upper rib should be avoided to prevent injury to neighboring intercostal vessels.
Procedure: Restrain and position the child, preferably in sitting position gt; confirm the fluid level by ultrasonography or by percussion, gt; clean the selected site with an antiseptic gt; drape the surrounding area gt; infiltrate 1-2% xylocaine for local anesthesia, gt; palpate
Fig. 32.24: Thoracocentesis.
the desired space gt; ask the patient to hold the breath
gt; insert a 16-18 gz. Needle attached to a syringe, perpendicular to the surface, till a give-away feel of entering pleural space gt; aspirate with gentle negative suction, gt; withdraw the needle and seal the site with tincture bezoin.
Note that:
• For therapeutic drainage of large effusions, a threeway stopcock must be fixed between the syringe and needle, to avoid repeated disengagement of syringe and risk of pneumothorax.
• Total aspirated volume in single sitting should not exceed gt; 5% of body weight.
• In cases of empyema, intercostal tube thoracotomy is necessary for continuous drainage of pus.
Complications include: (a) pneumothorax, (b) infection, and (c) traumatic puncture of liver/spleen or bleeding, and rarely, (d) sinus/fistula formation (in tubercular effusion).
Pericardiocentesis, i.e. drainage of pericardial fluid collections is a relatively risky procedure that should be performed under continuous monitoring of vital signs, ECG and pulse oximetry.
Indications: (a) diagnosis of the type of pericardial effusions, (b) therapeutic drainage of large effusions in cases with cardiac tamponade.
Site: Preferred site is just below and to the left of xiphoid process (Fig. 32.25).
Procedure: Restrain and position the child in supine positiongt; confirm the presence of pericardial fluid by ultrasonography gt; clean the selected site with an antiseptic gt; drape the surrounding area gt; infiltrate 1-2% xylocaine for local anesthesia, gt; ask the patient to hold the breath gt; insert a 16-18 gz. needle attached to a syringe at 45° to skin surface directed towards the left scapula
gt; advance the needle till fluid is obtained or ECG changes appear (signs of contact with ventricular wall) gt; aspirate with gentle negative suction, gt; withdraw the needle and seal the site with tinc. bezoin.
Complications include: (a) arrhythmia, (b) traumatic hemopericardium, (c) myocardial injury. All patients should be kept under continuous supervision for 6-8 hours after the procedure.
Abdominocentesis is a common procedure to obtain ascitic fluid from peritoneal space.
Indications: (a) diagnosis of the type of ascites, (b) therapeutic drainage of large collections, leading to abdominal discomfort or respiratory embarrassment.
Site: Preferred site is the mid-way between umbilicus and anterior superior iliac spine on right side (Fig. 32.26). Procedure: Restrain and position the child, in supine position, gt; confirm the ascites by USG or by percussion, gt; clean the selected site with an antiseptic gt; drape the surrounding area gt; infiltrate 1-2% xylocaine for local anesthesia, gt; insert a 16-18 gz. Needle attached to a syringe, obliquely to prevent leakage of ascitic fluid, till fluid is obtained, gt; aspirate without suction, gt; withdraw the needle and seal the site with Tinc. bezoin.
Note that:
• For therapeutic drainage of large ascites, a three-way stopcock must be fixed between the syringe and needle to avoid repeated disengagement of syringe and risk of pneumoperitoneum.
• Total aspirated volume in one sitting should not exceed 5% of body weight.
Complications include: (a) trauma to deeper structures, e.g. intestines, (b) peritonitis.
Supra-pubic puncture is the safe and reliable method to obtain uncontaminated urine sample in infants.
Site: Midline, just above the pubic symphysis.
Procedure: Restrain and position the child in supine position, gt; confirm that the bladder is full by percussion
Fig. 32.25: Pericardiocentesis.
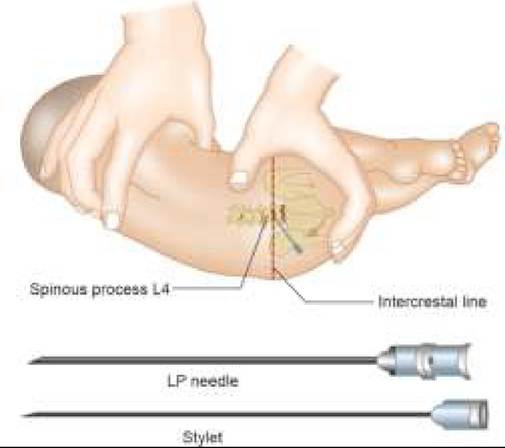
Fig. 32.26: Abdominocentesis.
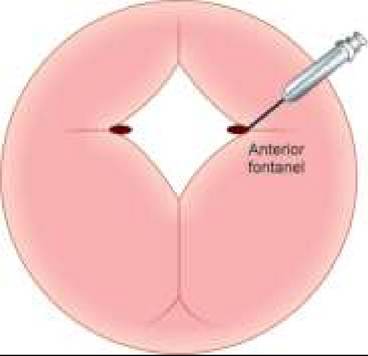
Fig. 32.27: Suprapubic puncture.
gt; clean the selected site with antiseptic gt; drape the surrounding area gt; infiltrate 1-2% xylocaine for local anesthesia gt; insert a 21 gz needle/syringe, perpendicular to selected site for a depth of 2-3 cm, gt; aspirate the urine with gentle suction gt; withdraw the needle and seal the site with tincture benzoin (Fig. 32.27).
32.2