BASIC CONSIDERATIONS
The hallmark of immune defense is recognition of a foreign or non-self antigen, as well as tolerance of own tissue antigen or self-antigen. Some basic concepts in immunology are as follows:
Antigen: The term antigen refers to a molecule recognizable by immunological cells, which have specific binding sites (receptors) for these molecules.
Only a small portion of antigen (epitope), e.g. cell-wall component or DNA-nucleotide sequence, etc. is recognized by antigen-specific receptors, though complex antigens have many such epitopes. All antigens are not equally immunogenic. Proteins antigens are more immunogenic than carbohydrates, e.g. lipopolysaccharides (haptens). However, immunogenicity of haptens may be enhanced by conjugating them with protein vehicles, e.g. tetanus toxoid, as done in conjugate vaccines.All cells have antigens, including viruses, bacteria, etc. and even the host's own cells. However, tolerance to self-antigens develops during early fetal life by selective elimination of those T-cells (apoptosis), which do not recognize self-antigens, i.e. major histocompatibility complex (MHC) antigens.
Major histocompatibility complex (MHC) is the surface antigen (glycoprotein), present on most human cells, including leukocytes (human leukocyte antigen or HLA). These antigens may be broadly divided into two types: MHC class I molecules (HLA-A, B, C) present on most the nucleated body cells and platelets; and MHC class II molecules (HLA-DP, DQ, DR), present on macrophages, dendritic cells and B cells.
HLA type of a person is determined by a cluster of genetic loci on short arm of 6th chromosome and denoted as HLA-B27, HLA-D8, etc. Major significance of HLA antigens lies in: (a) tissue typing before transplants to select suitable donor, and (b) their association with many autoimmune disorders.
Types of immunity: Immune-defense mechanisms may be broadly divided into:
• Innate immunity, which is antigen non-specific and attempts to eliminate any invading pathogens before the development of antigen-specific adaptive immunity.
It is provided by: (a) physical, chemical and mechanical barriers, (b) inflammatory response to bring cellular elements at the site of invasion, e.g. phagocytes and natural killer cells, to engulf and kill invading organisms, and (c) release of chemical mediators, e.g. cytokines and chemokines.Innate immune system also triggers development of adaptive immunity by processing the pathogen by antigen-presenting cells, i.e. macrophages and dendritic cells, and transport them to T-lymphocytes, largely present in lymph nodes.
• Adaptive (Acquired) immunity is antigen-specific, develops over few days/weeks after the first exposure and persists throughout the life due to development of memory B-cells, though not necessarily in protective range. Mediated by T cells (cell-mediated immunity) and/or B cell generated immunoglobulins (humoral immunity) adaptive immunity is responsible for clearance of primary infection and prevention of disease during subsequent exposures. Adaptive immunity may be induced by natural exposure (infection) or artificial exposure (vaccine).
Components of Immune System
As stated earlier, immunological mechanisms are mediated by various cellular and humoral components of immune system, as follows:
• Antigen non-specific components, e.g. phagocytes, dendritic cells, natural killer cells, complements, etc.
• Antigen-specific components, e.g. T-cells and B-cells (immunoglobulins).
There is considerable interdependence between these immunological mediators, which act in coordinated manner to induce adequate immune response.
I. Phagocytic system is the first line of immunological defense to: (a) engulf and digest foreign antigens, and (b) process them for presentation to antigen-specific cells.
It is mediated by two different cell types: (i) circulatory phagocytes, i.e. neutrophils and (ii) tissue phagocytes, i.e. macrophages, which are derived from monocytes and populate tissues like lung, liver, kidney, spleen, brain and lymph nodes.
Neutrophilic phagocytes mainly act against pyogenic bacteria, while macrophages are predominantly involved in killing of intracellular organisms, e.g. mycobacteria, toxoplasma, etc. and inducing T-cell mediated immune response.Phagocytosis of a foreign element involves a cascade of activity, including: (a) recognition of the invader as a non-self-antigen, (b) chemotaxis, i.e. recruitment of more phagocytic cells, mobilized from other sites as well as bone marrow, (c) phagocytosis, i.e. attachment and entrapment of antigen within phagocytes by a process of vacuolization, and (d) microbiocidal activity within the phagocytes to eliminate entrapped pathogens by various oxidative, hydrolytic or defensins mediated systems.
Phagocytosis is facilitated by: (a) specific antibodies on phagocytes, which act as ligands to bind them with pathogen, and (b) opsonins in serum-products of complement system, which neutralize anti-phagocytic factors on bacterial cells.
II. Dendritic cells are antigen-presenting cells widely distributed in skin, lungs and other tissues, which primarily act against extracellular antigen, e.g. microbial cell-wall components, dead host-cells, etc. These cells recognize a foreign antigen, collect a sample by endocytosis to process it into smaller peptide fragments and then migrate to regional lymph nodes to present them to T and B cells. Thus, these cells may be considered as antigen-priming cells for induction of acquired immunity.
III. Natural killer (NK) cells are lymphocytes without T-cell receptors, which primarily act against intracellular antigens, e.g. virus-infected cells and malignant cells, i.e. aberrant host cells and killing them. Recognition of intracellular antigen by these cells depends on:
(a) antibody-coating on virus-infected cells, and (b) suppression of MHC molecules on aberrant/malignant host cells to render them as foreign antigens. Intracellular killing by NK cells is a complex process involving injection of target cells with cytotoxic granzymes.
IV. Complement system consists of many non-specific, heat-labile interacting protein components, which contribute to ~10% of total plasma globulin fraction.
These components are numbered (C1, C2..., etc.) in order of the discovery and not in sequence of their activation. Complements and their by-products act as a principle mediator of inflammatory response, after nonspecific or specific antigenic challenge. Various components of complement system are activated in sequentially by two different pathways:
a. Classic pathway, which is primarily stimulated by immunological mechanisms, i.e. fixation of C1 to Fc portion of antibody (antigen-specific) or C-reactive proteins (antigen-non-specific).
b. Alternative or properdin pathway, which is mainly stimulated by non-immunological stimuli, e.g. endotoxins, leukocyte degradation products, etc. Or after activation of a component of the classic pathway C
3b.
Both pathways converge at the level of C3 activation, followed by a common sequence to generate highly active complement components, e.g. opsonins (C3b), chemotactic factors (C5a), mast-cell activators, i.e. anaphylatoxins (C3a, C5a), cell lysis activity (membrane attack complex). C3 is most abundant and crucial component of complement system.
Complement system plays a vital role in both innate and adaptive immunity with: (a) neutralization of viruses, (b) opsonization of bacteria, (c) deactivation of endotoxins, (d) lysis of virus-infected or malignant cells, and (e) regulation of immune response by induction of granulocytosis or suppression of excessive antibody response.
Controlling mechanisms to prevent excess consumption of complement activity involve simultaneous activation of various complement inhibitors during complement cascade, e.g. C1 inhibitor and others.
V. Cytokines or chemokines are glycoproteins, synthesized and released by immunologically activated lymphocytes (lymphokines), macrophages, monocytes and vascular endothelium.
Cytokines predominantly act as immune messengers to regulate immune response, i.e. to localize, limit or facilitate it, depending on the type of cytokines produced. Important cytokines are: Interleukins (IL118), interferons (IFN-#946;, #947;), tumor necrosis factors (TNF-#945;), colony stimulating factors (GM-CSF, G-CSF, M-CSF) and erythropoietin, etc.
Cytokines also participate in regulation of hematopoiesis and inflammation. Most of the cytokines act as both—facilitator or inhibitor of immune response, depending on the target cells.
VI. Acute phase proteins may be: (a) pro-inflammatory, e.g. C-reactive protein, which assists in recognition of pathogen/damaged cell, complement activation and cytokine production, or (b) anti-inflammatory, e.g. proteinase inhibitors or coagulation proteins, which help in wound healing.
VII. T lymphocytes may be considered as the orchestra director of acquired immunity, which not only mediate cellular immunity but also activate B-cell for immunoglobulin production.
Cell-mediated immunity (CMI) is mainly involved in: (a) immunity against intracellular organisms (viruses, mycobacteria), fungi and protozoa, (b) immune surveillance of cancer cells, and (c) graft-rejection or graft versus host disease.
T lymphocytes develop from stem cells in bone marrow, but migrate and mature in thymus. Thymic maturation involves three important changes: (a) cluster differentiation, i.e. switch-on of various surface markers- termed CD markers; (b) positive selection, i.e. development of T cells which recognize self-MHC antigens, and (c) negative selection, i.e. elimination of T cells which do not recognize self-antigens and may be self-destructive. Subsequently, these cells enter circulation and repopulate lymphoid organs, e.g. lymph nodes, spleen and Peyer's patches. Depending on their functions and CD markers, T cells may be divided into 2 major groups:
• T helper-inducer cells (CD4 cells), which induce antibody production by B cells and regulate immune response by cytokines production.
These cells are further divided into: Th1 cells, which are important for macrophage activation and cell-mediated immunity; and Th2 cells, which help in activation and differentiation of B cells and down-regulation of immune response. Th1 cells predominantly help in elimination of intracellular pathogens, e.g. viruses, while Th2 cells are more important for elimination of extracellular pathogens, e.g. helminths. Excess Thl or Th2 activity is a major contributing factor for autoimmunity and allergy, respectively.• Cytotoxic-suppressor cells (CD8 cells), which are responsible for killing of virus-infected cells or tumor cells, as well as suppression of immune response.
VIII. B-Iymphocytes are mediators of acquired humoral immunity, by production of antigen-specific or nonspecific immunoglobulins.
Like T-cells, B-cells also develop from stem-cells in bone marrow. However unlike them, human B-cells mature in bone marrow itself (bursa of fabricius in birds), before circulating and populating lymphoid follicles in spleen, liver, tonsils and Peyer's patches. B-cells comprise 5-15% of total circulating lymphocytes. On antigenic stimulus, these cells differentiate into plasma cells, to produce various immunoglobulins.
B-cells are of two types: B1 (CD5) cells, which produce non-specific IgM immunoglobulins against variety of antigens; and B2 cells which produce specific IgM, IgE and IgA antibodies in response to specific antigenic challenge.
IX. Immunoglobulins (Ig) or antibodies are serum proteins, produced by B-cells, which: (a) inactivate, agglutinate or opsonise antigens for phagocytosis, and
(b) activate complement system for cytolysis. These immunoglobulins are present on the surface of B-cells (surface immunoglobulins) or secreted in extracellular medium (secretory immunoglobulins). Depending on their properties and role in immune system, immunoglobulins may be divided into 5 types:
• IgM constitutes ~10% of serum immunoglobulins and mainly remains within the circulatory compartment. IgM antibodies are the first class of immunoglobulins secreted after antigenic challenge, though levels decline soon after the infection is controlled within 2-3 months. Thus, raised IgM levels indicate acute infection. IgM does not cross the placenta and high IgM levels in newborn indicate true fetal infection.
• IgG, most abundant serum immunoglobulin (~70%), is produced later than IgM after primary antigenic exposure and persist longer for many months or years but in declining titers. Thus, IgG levels may be high due to past infection and not necessarily indicate acute infection. However, on a subsequent challenge with same antigen, IgG response is anamnestic, profound and persistent. While predominantly present in serum, IgG diffuse
well in tissues as well as cross the placenta to transfer the maternal immunity to baby. Hence, raised IgG titers in fetus or newborn may be due to maternal transmission and not necessarily indicate fetal infection.
Four major subclasses of IgG are IgG1, IgG2, IgG3 and IgG4C. Of these, IgG2 is unique, as it also responds to polysaccharide antigens.
• IgA contributes to ~15-20% of serum immunoglobulins (serum IgA), as well as also present in various body secretions (secretory IgA), e.g. nasobronchial or gut secretions, saliva, lacrimal fluid and colostrums (protective antibody in human milk).
Secretory IgA is predominantly responsible for local immunity, i.e. clearance of antigen from mucosal sites. IgA does not activate complement system or provoke inflammatory response.
• IgE is present in miniscule amounts in serum but acts as principal mediator of immediate hypersensitivity (allergy) as well as also has some role in immunity against helminths.
Two types of IgE antibodies are - non-specific IgE, present in serum/tissues of normal individuals which appear to defend against parasitic invasion; and specific or reaginic antibodies, synthesized on exposure to a specific allergen.
• IgD accounts for lt;1% of serum immunoglobulins with indefinite role, probably as an antigen receptor site on circulating B-cells.
Physiology of Adaptive Immune Response
Immune responses are initiated by the exposure to an antigen that carries a danger signal, e.g. bacterial products, endotoxin, viral DNA or tissue necrosis. Important steps in development of immune responses (Fig. 8.1) are as follows:
• Innate immunity directly attempts to eliminate invading pathogen by itself using: (a) physical, chemical and mechanical barriers, (b) inflammatory response to bring cellular elements, e.g. phagocytes and natural killer cells at the site of invasion to engulf and kill invading organisms as well as macrophages and dendritic cells (antigen-processing cells) to process the antigen/s of pathogens, and (c) release of chemical mediators, e.g. cytokines and chemokines.
• Antigen-processing: Innate immunity also triggers development of adaptive immunity using these antigen presenting cells, to process the pathogens and express their antigen/s on the surface for recognition by immune cells. Processed antigens are transported to T lymphocytes, largely present in lymph nodes.
• T-cell dependent response is triggered by processed antigens and induce: (a) direct killing of virus- infected or tumor cells by cytotoxic or NK cells, (b) further activation of macrophages and cytotoxic cells by Th1 cells, (c) differentiation of antigen-specific B-cells by T-helper or Th2 cells, and (d) secretion of various cytokines, which act as immune messenger or regulator.
Activate T-helper cells also stimulate B-cell differentiation to develop as plasma cells and produce specific immunoglobulins and memory B cells. Memory cells directly recognize the offending agent on re-exposure for accelerated immunoglobulin production.
• T-cell independent response is usually seen against organisms covered by a polysaccharide capsule, (e.g. H. influenza B, pneumococci, meningococci). This capsule resists ingestion of organism by phagocytes, preventing expression of antigen and T-cell activation. In such cases, naive B cells themselves recognize the pathogen and get activated to produce antibodies. Antibodies produced against T-cell independent responses are largely of IgM class, and no memory cells develop for anamnestic response on re-exposure.
Immunological Disorders
The term immunological disorders includes three distinct abnormalities, discussed elsewhere:
a. Immunodeficiency states, i.e. inability to recognize or clear foreign antigens leading to recurrent or opportunistic infections (Ch 8.2).
b. Hypersensitivity reactions, i.e. inappropriate or disproportionate immune response, which may be predominantly IGE mediated, IgM/IgG mediated or cell-mediated (Ch 8.4).
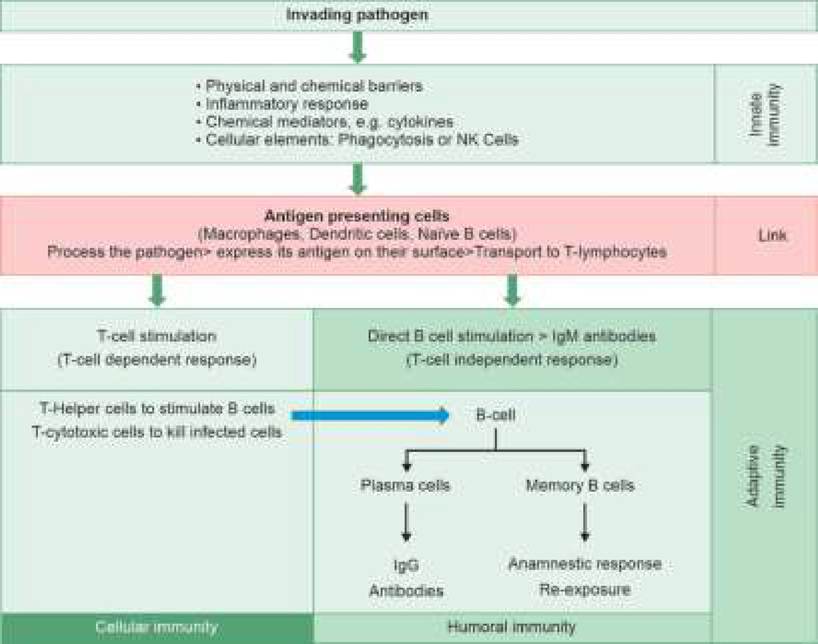
Fig. 8.1: Immunological defense mechanisms.
| TABLE 8.1: Common immunodeficiency disorders/states in children | |
| Primary or inherited | Secondary or acquired |
| A. Phagocytic defects | A. Developmental |
| - Cyclic neutropenia | - Prematurity |
| - Chronic granulomatous disease of childhood | - Newborns (? complement deficiency) |
| - Chediak-Higashi syndrome | B. Nutritional |
| - Lazy leukocyte syndrome | - Protein-energy malnutrition |
| - Hyper-IgE syndrome | - Zinc deficiency |
| - Enzyme defects (G6PD, myeloperoxidase) | C. Infections |
| B. Primary T cell defects | - HIV/AIDS |
| - DiGeorge syndrome | - Others: Measles, pertussis |
| - Chronic mucocutaneous candidiasis | D. Impaired splenic function |
| - Hyper-IgM syndrome | - Asplenia |
| C. Primary B cell defects | - Splenectomy |
| - Transient hypogammaglobulinemia | - Dysfunction: Sickle cell disease |
| - X-linked (Bruton) agammaglobulinemia | E. Iatrogenic |
| - Common variable immunodeficiency | - Drugs: Steroids, cytotoxic agents |
| - Selective IgA/IgG subclass deficiency | - Irradiation |
| D. Combined B and T cell defects | - Organ transplantation |
| - Severe combined immunodeficiency (SCID) | F. Miscellaneous: |
| - Wiskott-Aldrich syndrome | - Protein-loss: Nephrotic syndrome, burns |
| E. Complement defects (rarely primary) | - Metabolic: Diabetes mellitus, uremia |
| - Hereditary angioedema | |
TABLE 8.2: Warning Signs for Primary immunodeficiency disorders (PID) in children
c. Autoimmune disorders, i.e. inability to recognize selfantigen that triggers the immune reactions against own tissues, e.g. rheumatoid disorders (Ch 24).
8.2