BLEEDING NEONATE
Newborns are prone for bleeding tendencies due to: (a) developmental thrombocytopenia, (b) developmental deficiencies of clotting factors, (c) vitamin K deficiency
due to inadequate endogenous synthesis by immature gut flora, and (d) higher vascular permeability.
Coagulation proteins do not cross placenta and synthesized in fetus from 10th week of gestation.Etiology: Bleeding problems in newborn vary from mild/moderate bleeds in an apparently healthy child, e.g. hemorrhagic disease of newborn (HDN), to lifethreatening hemorrhage, e.g. DIC in critically sick babies (Table 12.52).
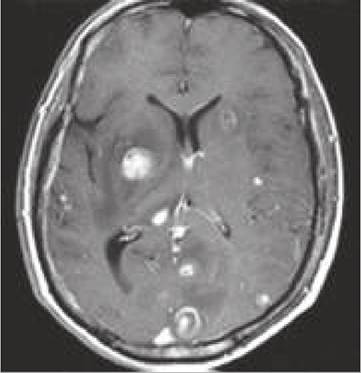
Diagnostic approach: A bleeding newborn may bleed externally from umbilical cord, skin, gastrointestinal; tract and IV sites etc; or internally, e.g. intracranial hemorrhage. Severity of clinical signs depends on the site and severity of bleed as well as primary cause.
Important diagnostic clue include:
• Detailed history, with special reference to:
± Age of onset (Table 12.53)
± Family history of bleeding disorders
± Antenatal maternal infections
± Obstetric complications, e.g. APH (swallow-blood),
± Postnatal feeding, (e.g. HDN in breastfeds)
• Clinical examination, with special reference to:
± General appearance: term and healthy (HDN) or preterm and sick (DIC).
± Site of bleed: IV sites (DIC), cord (slipped ligature, hemophilia), vagina (withdrawal bleeding, HDN).
± Associated sepsis, asphyxia, hypothermia (DIC).
± Hepatosplenomegaly (IU infections).
Signs of concealed/internal bleeding, e.g. progressive pallor, deep icterus, and shock are rare in classic HDN and usually indicate more severe etiology.
• Laboratory investigations: Need for investigations (Table 12.54) depends on severity of bleed and probable etiology.
No investigations are necessary in healthy breastfed term newborn with minor bleeding, who has not received vitamin K at birth and responds rapidly to single dose of vitamin K (suggestive of HDN).
Apt and Downey test is used to distinguish swallowed maternal blood from fetal blood in babies with blood mixed vomiting/melena. Mix 1 part of vomitus/stool with 5 parts of distilled water gt; centrifuge gt; add 1 ml of 1% NaOH gt; a change of color to yellowish-brown indicates swallowed maternal blood, due to denaturation of adult Hb. Fetal Hb is resistant to alkali denaturation.
A step-wise approach is preferred in other cases, beginning with three base-line investigations: (a) platelet count, (b) prothrombin time, and (c) partial thromboplastin time; to differentiate common causes of bleeding neonate (Table 12.55). Detailed investigations may be necessary to confirm the diagnosis or detect uncommon defects.
TABLE 12.54: Lab. investigations in bleeding neonate
TABLE 12.52: Causes of bleeding neonate
• Coagulation disorders
- Hemorrhagic disease of newborn (HDN)
- Inherited: hemophilia, von-Willebrand disease
- Hepatic injury: hypoxia, infections
- Maternal drugs: anticoagulants, salicylate, phenytoin
• Platelet disorders (purpura)
- Increased destruction:
#9830; Immunological: Neonatal ITP
#9830; Mechanical: Hemagioma, NEC
- Decreased bone marrow production:
#9830; BM depression—infections, hypoxia, drugs
#9830; BM infiltration—leukemia, Gaucher disease
- Hereditary disorders:
#9830; Wiskott-Aldrich syndrome
#9830; Function defects—Glanzmann thrombasthenia
• Vascular immaturity/injury
- Intra-ventricular hemorrhage
- Trauma: Birth trauma, slipped cord ligature
• Disseminated intravascular coagulation (DIC)
• Swallowed maternal blood
Step I. Baseline investigations
• Apt test (swallowed blood)
• Platelet count (thrombocytopenia)
• Peripheral smear (sepsis, leukemia)
• Basic clotting profile (BT, CT, PT, PTT)
Step II. Relevant investigations
• Platelet function tests
• Clotting factor assays
• FDP or D-dimer assay (DIC)
• Maternal platelet count (for neonatal ITP)
• Coomb test (platelet isoimmunization)
• Liver function tests
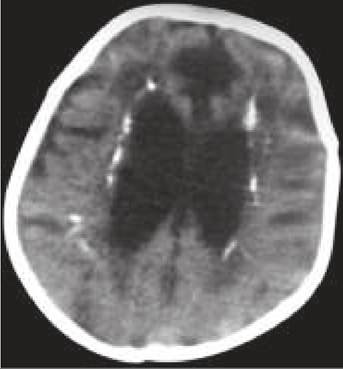
TABLE 12.55: Diagnostic approach to bleeding neonate
Plc: Platelet count.
*e.g. in preterms, acidosis, asphyxia **excessive platelet destruction, e.g. in sepsis, NEC, hemangiomaHemorrhagic disease of newborn (HDN) is the commonest cause of bleeding in newborns, due to transient Vitamin K deficiency—required for synthesis of coagulation factors—II, VII, IX and X. The term Vitamin K deficiency bleeding (VKDB) is preferred by some workers, as HDN is not limited to newborns and neonates may bleed due to other causes rather than vitamin K deficiency.
According to the age of presentation and etiology, HDN may be divided into 3 types:
a. Classical HDN, manifests on 2-7th day and almost exclusively seen in full-term breastfed newborns with estimated incidence of ~0.5-1.0%.
Etiologically, it is linked to—(i) marginal vitamin K content in breast milk, (ii) delayed/inadequate feeding, and (iii) inadequate endogenous vitamin K synthesis due to relatively sterile gut.
Clinically, these newborns are apparently healthy, except mild bleeding from superficial sites, e.g. umbilical stump, nose, vagina, venepunctures, circumcision wounds, etc. Mild transient gastrointestinal bleeding is not uncommon but serious intracranial bleeds are very rare.
b. Early HDN presents with severe bleeding manifestations within 24 hours of birth, due to vitamin K deficiency following maternal therapy with drugs that interfere with vitamin K metabolism, e.g. anticoagulants, anticonvulsants, antitubercular drugs and salicylates.
c. Late HDN presents beyond 1st week of life (usually 3-8th week) due to inadequate endogenous synthesis in gut, usually in sick babies with cholestatic liver disease, malabsorption syndromes and prolonged antibiotic therapy, when normal gut flora is destroyed. Unlike classic disease, serious internal bleeding and intracranial hemorrhage is common.
Diagnosis of classical HDN is largely clinical (bleeding in apparently healthy newborn), supported by abnormal coagulation profile and therapeutic response to vitamin K within 30-120 minutes.
In early/late HDN, diagnosis may be confirmed by elevated PIVKA-II levels (proteins induced in vitamin K absence).Vitamin K levels are difficult to measure and unreliable.
Management: A single dose IV or SC vitamin K1 (1-5 mg) is the treatment of choice for VKDB/HDN, even before laboratory confirmation. IM injections should be avoided due to risk of large hematoma formation. Severe or persistent bleeding may require repeated doses along with factor replacement therapy with fresh frozen plasma (10 ml/kg) or prothrombin complex concentrates.
Late VKDB is a chronic problem and may need regular vitamin K supplements (1 mg/months IM or 50- 100 mg/ day PO) as well as treatment of primary cause.
Prevention: Prophylactic administration of a single dose of IM vitamin K 1mg (0.5 mg in babies weighing lt; 1000 gm) at birth is an established practice to prevent almost all cases of classic/Late HDN. While oral vitamin K prophylaxis is equally effective to prevent classic HDN in fullterms, protection is inadequate against late HDN. Infants on antibiotics for gt; 2 weeks should receive 0.5 mg vit K per week.
Pregnant mothers on oral anticonvulsants should receive daily vitamin K supplements (PO 10-20 mg) for 15-30 days before delivery to prevent early HDN.
12.17.2