Brachial Plexus and Cervical Nerve Root Lesions
Traumatic obstetrical brachial plexopathy usually results from traction on the brachial plexus (predominantly upper trunk) and its associated spinal roots. This can lead to stretching or rupture of the trunks of the plexus and/or partial axonotmesis or avulsion of the spinal roots.
The most common cause is a shoulder dystocia of the anteriorly presenting shoulder causing excessive lateral neck traction. Injury to the upper trunk of the brachial plexus and/or C5-6 cervical roots is the more common injury known as Duchenne-Erb's palsy. Damage to the lower trunk and/or C8-T1 cervical roots is referred to as Klumpke's palsy. Severe brachial plexus injuries may involve the entire plexus and C5-T1 nerve roots diffusely. A Horner's syndrome due to injury of the C8 and T1 roots and the superior cervical sympathetic ganglion may be an associated clinical finding. An isolated Klumpke's palsy is rare in the setting of traumatic birth palsy and usually results from a fall onto a hyperabducted shoulder, penetrating trauma, or tumor.Electrodiagnostic studies help determine the location (root and/or plexus), extent, and severity of
the brachial plexus injury. Examination should be deferred until at least three to four weeks after the injury to allow for abnormal spontaneous rest activity (fibrillations and positive sharp waves) to develop in the setting of denervation and axon loss (Fig. 7.8). Complete injuries are characterized electromyograph- ically by absent MUAPs and absent CMAP amplitudes in peripheral nerves supplied by the transected axons. In the setting of total motor paralysis, motor nerve conduction studies with measurement of the amplitude of the CMAPs in distal and proximal muscles provides useful prognostic information. For example, the preservation of the CMAP amplitude 10 days or more after the injury with complete clinical paralysis suggests that the damage is, in part, a neuropraxic injury with better prognosis.
In this setting, F-waves are absent. If motor function is absent and no MUAPs are observed, examination of the amplitude of the sensory nerve action potentials in the dermatomal distribution of the branches of the affected brachial plexus trunks can help distinguish injuries to the plexus from severe cervical root injuries or avulsions. The sensory dorsal root ganglion lies in the intervertebral foramen distal to the damaged segment with a root injury, leaving the sensory axon projection from the dorsal root ganglion to the limb intact. Thus, the sensory nerve action potential is obtainable in the setting of a root avulsion with absent clinical sensation.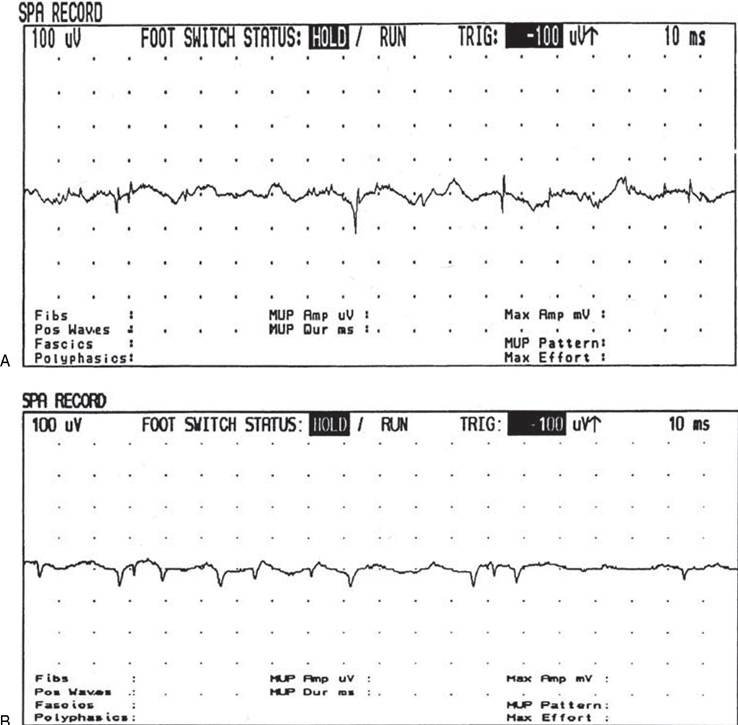
Figure 7.8 Fibrillation potential (A) and positive sharp waves (B) indicative of acute denervation and axon loss.
In the setting of Erb's palsy, assessment of a superficial radial sensory or median sensory response to the index finger is useful in making a distinction between a C6 root avulsion and a more distal lesion involving the trunk of the brachial plexus. The median SNAP to the middle finger provides information about the integrity of C7 axon projections distal to the dorsal root ganglion. The presence or absence of an ulnar sensory nerve action potential can help distinguish a lower trunk injury from a C8 nerve root injury.
In perinatal traumatic brachial plexopathy, positive sharp waves and fibrillations, indicative of true denervation, can be found by 14 to 21 days after injury (57). Absence of fibrillations or positive sharp waves after this time frame suggests a neuropraxic lesion with intact axons. In this setting, the prognosis for recovery is favorable. Early in the course of recovery prior to reinnervation, interference pattern usually is reduced or discrete and recruitment frequencies increased into the neuropathic range (often >20 Hz). A follow-up needle EMG evaluation three to six months after the injury is useful to determine subclinical evidence of reinnervation.
Such reinnervation is typically characterized initially by “nascent” polyphasic MUAPs (Fig. 7.9). With reinnervation, the numbers of positive sharp waves and fibrillations decreases over time, amplitude of MUAPs increases as collateral spouting occurs, and with evaluation of interference pattern, there is an observed increasing number of voluntary MUAPs.The author prefers to initially obtain sensory nerve conduction studies (occasionally with sedation) consisting of a median sensory nerve conduction study recorded from the index finger (C6 dermatome), a median sensory nerve conduction study recorded from the middle finger (C7 dermatome), and an ulnar sensory nerve conduction study recorded from the fifth digit (C8 dermatome). Median and ulnar motor nerve conduction studies are useful to evaluate the integrity of axons traveling through the lower trunk. Axillary and musculocutaneous motor nerve conduction studies (with assessment of CMAP amplitudes) are useful if an upper trunk injury is suspected. These CMAP amplitudes may be compared to the intact side, depending on patient tolerance of the study (58). A CMAP amplitude reduction of more than 90%, compared to the unaffected side, predicted severe weakness of the corresponding root level. During the EMG study of the deltoid, the examiner should assess the clinical sensation of the C5 dermatome. The use of dermatomal and mixed-nerve SSEPs in brachial plexus injuries are discussed in a following section.
In addition to a complete needle EMG screen of upper extremity muscles clinically affected, electromyographic examination of the infraspinatus or supraspinatus can help localize an upper trunk injury proximal to or distal to the takeoff to the suprascapular nerve. While the examination of the rhomboid can be difficult in the infant, a finding of fibrillations or positive sharp waves supports the presence of a C5 root injury. While in the adult electromyographic evaluation of the cervical paraspinal muscles may help evaluate the extent and severity of cervical root injuries, generally the cervical paraspinals are extremely difficult to study in the infant due to poor relaxation.
In the young child, adequate relaxation of the cervical paraspinals may be obtained with general anesthesia,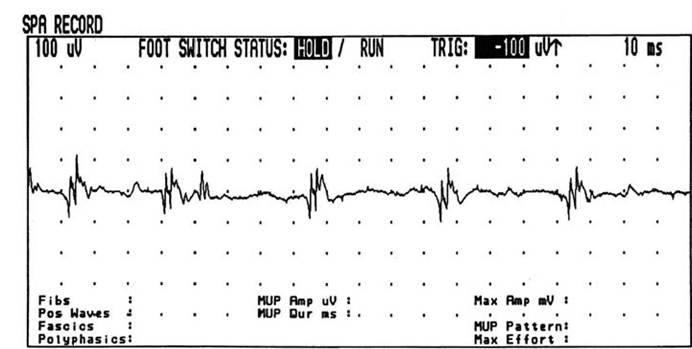
Figure 7.9 Polyphasic motor unit action potential (MUAP) with a neuropathic firing frequency at 25 Hz. These polyphasic MUAPs obtained 4 months after brachial plexus injury are indicative of reinnervation.
but this is usually not necessary and does not influence management. In addition, study of the serratus anterior and rhomboids (typically performed to assess involvement of C5 and C5-C7 roots, respectively) may be technically difficult in the infant due to intact sensation, the presence of the trapezius overlying the rhomboids, depth of the rhomboids and serratus anterior, and the risk that sudden movement may cause penetration of the needle into the pleural space. Usually, a combination of needle EMG evaluation, sensory and motor conduction studies, and F-wave studies allows the electromyographer to determine the location and severity of the injury.
The natural history of conservatively managed brachial plexus birth palsy has been reported (59). Seventy-two percent of those referred for rehabilitation evaluation showed stable functional status at follow-up. There has been a resurgence of interest in surgical exploration of obstetrical brachial plexus palsy with external and internal neurolysis, neurotization, and, in selected cases, nerve grafting (60-66). EMG evaluation at approximately 4-9 months postinjury may support the possible utility of a surgical exploration for neurolysis, neurotization, and/or nerve grafting if there is limited electrophysiologic evidence of reinnervation. Some authors suggest a repeat study within three months of the injury (67). Preoperative electrodiagnostic studies, intraoperative nerve conduction studies, and somatosensory-evoked potentials are helpful in the surgical decision making. Preoperative and/or intraoperative somatosensory-evoked potentials may provide evidence of upper cervical root avulsion versus partial trunk and nerve root integrity, as discussed in a following section.