CALCIUM DISORDERS
Bones are main reservoir of calcium, containing ~99% of total body calcium. Normal plasma calcium level is 9-11 mg/dl, which is ~60% is in bound form with albumin or other anions, e.g.
phosphates, and the rest in free ionic form (4.0-5.2 mg/dl).Calcium in extracellular fluids is in equilibrium with skeletal calcium and plays vital role in many physiological processes, e.g. neuromuscular transmission, coagulation and cellular functions. Calcium affects cellular functions through it binding regulatory protein - calmodulin.
RDA for calcium varies with age as 300 mg/day in infants, 500-600 mg/day in children and ~1000 mg/day in adolescents.
Sources: Dairy products are most important source of calcium along with millets, e.g. ragi and root vegetables, e.g. tapioca. Cow milk has more calcium than breast milk (1200 mg/dl vs 300 mg/dl), though later is absorbed better than former. Presence of phytates, oxalates and citrates in diet inhibits its absorption.
Physiology: Calcium homeostasis largely depends on renal reabsorption, mobilization from bones and intestinal absorption, regulated by various hormones, e.g. parathormone, vitamin D and calcitonin, as follows, (Fig. 7.2):
• Parathyroid hormone (PTH) increases S. Ca++ levels by facilitating its absorption from gut, reabsorption from kidneys and mobilization from bones. PTH levels are controlled by a feedback mechanism, dependent on serum calcium levels.
TABLE 7.8: Causes of hyperkalemia
a. Decreased renal excretion
- Acute/chronic renal failure
- Hypoaldosteronism, salt-loosing CAH
- Use of potassium-sparing diuretics
b. Increased intake
- Iatrogenic: Potassium salts, penicillin
- Blood transfusions (sp. old blood)
c. Hypercatabolic states (release from tissues)
- Medical: Burns, tumor lysis syndrome*
- Surgical: Extensive trauma, major surgery
d.
Transcellular distribution**- Metabolic acidosis
- Familial hyperkalemic periodic paralysis
e. Pseudohyperkalemia: Hemolysed sample
*during chemotherapy, ** shift of K+ out of the cells.
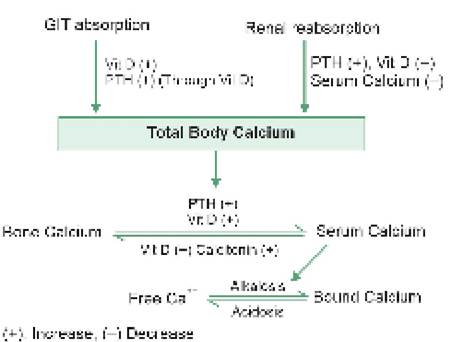
Fig. 7.2: Calcium regulation.
• Vitamin D (1,25(OH)2D3) also increases gut absorption and renal reabsorption of calcium, but unlike PTH, facilitates its deposition in the bones rather than increasing serum levels.
• Thyrocalcitonin hormone from parafollicular cells of thyroid is antagonistic to PTH, decreasing bone resorption and increasing urinary calcium excretion. Acid-base status predominantly affects ionic component
without altering total serum levels. Ionic calcium levels are increased in acidosis due to movement of Ca++ out of the cell and decreased in alkalosis due to reverse movements. This ionic component of plasma calcium is the prime determinant of its physiological activity. As commonly measured serum levels include both the bound and ionic calcium, normal S. calcium levels do not exclude physiological hypo-/hypercalcemia. Ionic component may be normal despite low serum values, due to reduced bound fraction, e.g. in hypoproteinemia.
Hypocalcemia: Though the term 'hypocalcemia' is generally used to denote S. calcium lt; 8.5 mg/dl in children or lt;8 mg/dl in term newborns, clinical manifestations depend on ionic Ca++ levels (lt; 4.0 mg/dl).
If facility to measure ionic Ca++ is not available, it is worthwhile to measure S. albumin levels simultaneously. In normo-albuminic children, low S. calcium reflects ionic hypocalcaemia. However, in hypo-albuminic states, disproportionately low S. calcium levels should be demonstrated to identify ionic hypocalcaemia (for each 1 gm/dl fall in S. albumin below 4 gm/dl, S. calcium levels fall by ~0.8 mg/dl).
Ionic Ca++ levels are also altered in acid-base imbalance, i.e.
increased in acidosis and decreased in alkalosis (0.1 unit change in pH = 10% change in ionic calcium levels).Causes: Hypocalcaemia is rarely dietary except in topfed infants, where high phosphate content of formula feeds prevents adequate calcium absorption. Common causes of hypocalcaemia are listed in Table 7.9.
Clinically, latent or manifest tetany is the typical manifestation of symptomatic hypocalcaemia (discussed below), though generalized seizures are common in infancy. Less severe cases may present with irritability and cramps/twitching.
Management: Hypocalcaemic seizures or tetany is treated as follows:
• Immediate IV calcium gluconate 10% (2 ml/kg) infusion slowly over 8-10 minutes with cardiac monitoring for bradycardia or arrhythmia. IV site should be observed carefully during the injection as subcutaneous effusion may cause local necrosis.
TABLE 7.9: Causes of hypocalcemia
a. Vitamin D deficiency:
- Nutritional
- Malabsorption
- Chronic liver or renal disease
b. Decreased parathormone (PTH) activity:
- Hypoparathyroidism
- Pseudohypoparathyroidism
c. Hyperphosphatemia:
- Formula feeding
- Familial or chronic renal disease
d. Magnesium deficiency
e. Alkalosis or over-correction of acidosis
• Immediate therapy should be followed by IV calcium boluses as above repeated every 6-8 hours till next 2448 hours. In mild cases, oral calcium supplementation (40-80 mg/kg/day) is enough, preferably with vitamin D.
• In cases refractory to calcium boluses, concurrent hypomagnesemia is likely and must be treated with IV magnesium sulphate 50% infusion as 25-50 mg/kg diluted 5-10 times in normal saline, which may be repeated every 6 hours, if required.
• Reduction of phosphate content in formula feeds may be necessary to reduce the risk of recurrence.
Tetany is a clinical entity, indicative of neuronal hyperexcitability due to abnormal concentration of various ions in the fluid bathing nerve cells.
Causes: Tetany is caused by:
• Hypocalcaemia (S. ionic Ca++ lt; 3.0 mg/dl)
• Hypomagnesemia (S. Mg++ lt; 1.0 mg/dl)
• Alkalosis: Respiratory or metabolic.
Clinical manifestations: Carpopedal spasm is the hallmark of tetany, though latent tetany is more common. Important signs of latent/manifest tetany are as follows:
• Latent tetany:
- Chvostek sign—facial twitching after tapping over the facial nerve at angle of mandible;
- Trousseau sign—carpopedal spasm after squeezing of upper arm or during blood pressure measurement;
- Peroneal sign—carpopedal spasm, after tapping over the peroneal nerve behind lateral malleolus;
- Erb's sign—lower excitatory threshold on electrical stimulation of peripheral nerves;
- Prolonged QTc interval (gt; 0.45 sec)
• Manifest tetany:
- Carpopedal spasms, i.e. flexion of wrists, extension of fingers, adduction of thumb with/without extension and adduction of feet (Fig. 7.3);
- Laryngeal spasms with stridor, croup or sudden death due to choking;
- Paresthesia, i.e. tingling and numbness of fingers and toes;
- Generalized seizures in infancy.

Fig. 7.3: Tetany—carpopedal spasm.
Treatment depends on the urgent correction of primary metabolic defect, e.g. hypocalcemia, hypomagnesemia or alkalosis. Careful re-breathing into an overhead bag to increase pCO2 may control alkalotic tetany.
Hypercalcemia is relatively less common, defined as S. calcium gt;11 mg/dl.
Causes: Hypercalcemia is usually a chronic metabolic abnormality, secondary to increased parathyroid hormone or vitamin D activity or low phosphates to bind free calcium (Table 7.10).
Clinically hypercalcemia presents with:
• Impaired urinary concentration, leading to polyuria and polydipsia;
• Hypercalciuria with nephrocalcinosis, tubulointerstitial nephropathy and nephrolithiasis;
• Lethargy, confusion, headache and coma in severe cases
• Arrhythmia, due to sudden hypercalcemia following IV calcium administration.
Treatment is indicated only when S. calcium levels cross 12 mg/dl and includes:
• Normal saline infusion along with diuretics, to increase calcium excretion in acute cases.
• Bisphosphonates, e.g. pamidronate or etidronate to block bone resorption and treat chronic hypercalcemia, e.g. in malignancies, immobilizations and hyperparathyroidism. IV calcitonin (4-8 U/kg q6hr) may also be used in some cases.
TABLE 7.10: Causes of hypercalcemia
• Primary Hyperparthyroidism
• Hypervitaminosis D (Iatrogenic)
• Bone demineralization: Immobilization, malignancy
• Iatrogenic calcium overdose
• Low phosphate intake: LBW, milk-alkali syndrome
• Increased phosphate excretion: Thiazide diuretics
• Others: William syndrome*, thyrotoxicosis
*Elfin facies, hypercalcemia and supravalvular aortic stenosis.
• Peritoneal dialysis in selected cases, specially in those with renal failure.
• Surgical intervention may be needed in cases with hyperparathyroidism with persistent hypercalcemia (gt; 12.5 mg/dl) and recurrent renal stones.
7.4