Common Lower-Limb Deficiencies
Longitudinal Deficiency of the Fibula
The most common, and possibly the most controversial, deficiency is the longitudinal deficiency of the fibula. Many classifications and levels of involvement exist.
With partial deficiencies of the fibula, outcomes will vary.There is no evidence that this anomaly, in isolation, is genetically transmitted (12). It has been suggested that the fibula is undergoing “regressive evolution” and that may be the reason for the prevalence of deficiency of the fibula and susceptibility to congenital absence (122).
The clinical presentation of longitudinal deficiency of the fibula, which is a completely absent fibula, generally has a foreshortened tibial section, and frequently has ipsilateral femoral shortening. This tibial section appears shorter than it is as a result of kyphoscoli- otic bowing. This anterior bowing of the tibia shortens the segment longitudinally and creates an anterior prominence of the tibia. This anterior prominence is indicated by a subcutaneous dimple, which can range from superficial to invaginated. Figure 13.15 shows a child with a fibular deficiency. Proximally, the limb is often in genu valgum or drifts into genu valgum as the child grows. The distal involvement is usually an equinus position and a valgus posture during weight bearing due to lack of lateral support. Lateral tarsal and ray absences are often associated with this lateral long bone absence. As the child grows, the popliteal area becomes convex, with the medial hamstrings descending much lower than the lateral hamstrings. On

Figure 13.15 Child with fibular deficiency. Note subcutaneous dimple, leg length discrepancy, and four-rayed foot.
physical examination, the degree of internal hip rotation is often less than that of external hip rotation.
Many surgical options are available for treatment of longitudinal deficiencies of the lower limb. Historically, the most common treatment of a complete fibular absence has been with a Syme amputation, which is successful in providing an end-bearing surface for ambulation, with or without a prosthesis (123,124). Amputation takes place when the child is beginning to pull to stand and cruise with the assist of furniture or toys. Migration of the heel pad posterolat- erally has been noted in the follow-up of many Syme amputations, as shown in Figure 13.16. This migration may be due to the use of the posterior calf musculature during active ambulation in the prosthesis. The Boyd amputation serves to centralize the heel pad more effectively and is the surgery of choice in many clinics. In addition to the ankle disarticulation procedures, it may be necessary for the child to undergo unilateral epiphysiodesis or angulation osteotomies if the genu valgum becomes a prosthetic challenge to fit. Outcomes from Syme amputations have shown that these children are able to perform very well in their communities, have a good self-image, and are rarely limited in activities (125).
External fixator applications and advancements have provided options which challenge the team and orthopedists to reconsider amputation. Saving the foot would be the first choice if the procedure were proven to be as successful as the Syme amputation (125). Considerations for these procedures include level of involvement or “grade,” risks and psychological effects of multiple surgeries, potential (and probable) infections around pin sites, and physical effects of “down time” the child will experience during and

Figure 13.16 Limb with longitudinal deficiency of the fibula following Syme amputation. Note posterior lateral migration of heel pad.
after wearing the external fixator (7). In the event that the foot ablation is not imminent, orthotic fitting combined with shoe modifications will be necessary for the child to ambulate successfully.
Femoral Abnormalities
The term that has been used to define the most common deficiency of the femur has been proximal femoral focal deficiency (PFFD). With varying levels described first by Aitken in the late 1960s, PFFD has been the acronym of choice for many femoral anomalies. Congenital short femur differs from PFFD by having the proximal aspect of the femur and intact ipsilateral acetabulum.
Although the skeletal structures are quite variable, the clinical presentation for these limbs is similar. The femoral section is shorter, with a larger mass of soft tissue, which includes musculature, between the pelvis and the involved knee. A typical appearance is shown in Figure 13.17. These muscles are highly ineffective as a result of being slack and not stretched to their full potential. The hip posture and stability is quite variable. All of the limbs present with some degree

Figure 13.17 Child with femoral abnormality. Note clinical presentation of the hip flexion, abduction, and external rotation.
of hip flexion, abduction, and external rotation. For the congenitally short femur and lesser involved PFFD, the labrum is present, resisting proximal subluxation. More involved presentations have progressive sulux- ation to dislocation of the femur. Often, there is an associated fibular absence.
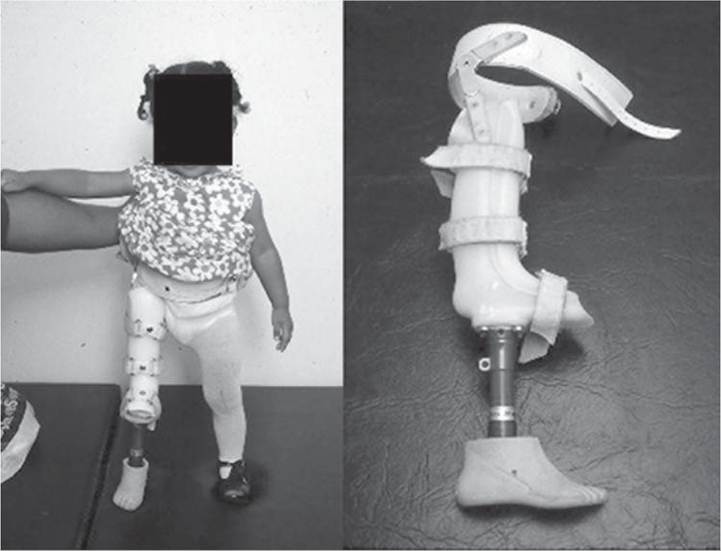
Surgical options for the congenitally short femur are numerous. The first option is “no surgery.” In some cases, some clinics and families feel that no surgical intervention is the best option for treatment of this disorder. In these cases, various lengthening devices such as shoe lifts and extension prostheses are necessary. These are sometimes referred to as “pros- thoses,” because they often combine a proximal orthosis with distal prosthetic components. An example of the “prosthosis” is seen in Figure 13.18. Children with bilateral femoral involvement often have no surgeries and no prostheses.
For those who have an intact short femur with both proximal and distal growth plates, this option may be a consideration; the addition of an external fixator to lengthen the foreshortened femur may also be considered. If the amount of lengthening necessary is unattainable, the limb lengthening may be performed in conjunction with appropriately timed epiphysiodesis of the contralateral leg to equalize leg lengths at full maturity.Ankle disarticulation along with knee arthrodesis is another option. It is performed when the proximal femur is affected and when the length discrepancy is such that an external fixator could not achieve the desired lengthening. The ankle disarticulation amputation is either a Syme or Boyd. Figure 13.19 is an example of a Syme amputation. Fusion of the knee may be delayed, as arrest of the proximal tibial and
B
Figure 13.18 (A) Child with femoral abnormality wearing “prosthosis.” Prosthosis is a combination Bi-valve KAFO with pelvic band and hip joint (B), extended with a prosthetic pylon and foot.

Figure 13.19 Child with femoral abnormality following Syme amputation. Note bulbous distal end of limb and proximal thigh musculature.
distal femoral growth plates will occur at that time, leaving a shorter overall limb length to control a prosthesis. This delay may be unnecessary if the overall limb length and the attempt to provide adequate space for congruency of a prosthetic knee with the noninvolved knee may be achieved during one surgery.
Another surgical option is that of a rotationplasty procedure. An intact fibula is preferred for this surgical procedure. The procedure involves rotation of the foot 180 degrees through removal of the distal femoral and proximal tibial epiphyses, and rotation of the distal segment prior to internal fixation (126).
The rotated foot can now act as a knee, utilizing ankle dorsiflexion as knee flexion and ankle plantar flexion as knee extension, as in Figure 13.20. This procedure has demonstrated effective outcomes; however, the aesthetic appearance of the limb following surgery has limited its popularity (127,128). It is crucial that the therapist and family aggressively work on maintaining the full range of motion of the ankle, especially in the sagittal plane. If this does not occur, all that has been accomplished is turning a foot “backwards” on the leg. Derotation of the foot has occurred on occasion, requiring additional surgery to again position the forefoot posteriorly.The Van Ness procedure has been utilized in other disorders such as burns and osteosarcomas (129,130).
In order to address the proximal subluxation of the femur and provide for a single articulation within the prosthesis, an iliofemoral fusion may be performed.

Figure 13.20 Rotationplasty limb (A) and close-up of prosthetic socket (B). Note knee center discrepancy and use of external knee hinges.
This may be in conjunction with a rotationplasty procedure or in isolation (131).
Longitudinal Deficiency of the Tibia
Longitudinal deficiency of the tibia occurs in 1 in 1 million births. Genetic transmission has been associated with these anomalies, particularly when a bifurcated distal femur exists; 30% of partial tibial deficiency occurs as an autosomal-dominant inherited pattern. The treatment is straightforward since the tibia is the major weight bearing bone. Differences in treatment occur between complete versus partial tibial absence. Figure 13.21 shows examples of tibial deficiency by radiograph.
The clinical presentation of a longitudinal tibial deficiency may include a varus foot and lower leg, a short leg, and an unstable knee and ankle (or both). The foot may have medial tarsals, metatarsals, and rays missing as well.
On radiograph, a distal femoral bifurcation may add to the challenge of prosthetic fitting as well as being an indicator for genetic influence (132).When there is a complete absence of the tibia, the treatment of choice is disarticulation at the knee. The fibula cannot sustain weight bearing of the individual at full maturity, and the instability of the knee and ankle is too great for corrective measures. For the child with a partial tibial deficiency, the segment length is important. If the tibial segment is short, the surgeon creates a synostosis with the intact fibula in conjunction with amputation of the foot. If the heel pad is retained, this procedure will create a walking surface for the child, providing stability without a prosthesis. However, this limb length is shorter than
B

Figure 13.21 Radiographs of child with tibial deficiency.
the aforementioned Syme amputation and may prove difficult for the child to walk without his or her prosthesis. Although treated as a “transtibial amputation,” many of these residua grow in quite a different manner. Often, the distal tibia and fibula fuse, while the fibula continues to grow at a faster rate than the tibia. The resulting deformity is a laterally bowing lower leg (the distal end is pushed medially), a fibular head that becomes more prominent and continues to grow proximal-laterally, or both. These additional deformities may not be able to be accommodated by the prosthetists in the socket fitting.