CONGENITAL DIAPHRAGMATIC HERNIA
Congenital diaphragmatic hernia (CDH) denotes ‘herniation of abdominal contents into the thoracic cavity through an abnormal opening in diaphragm, e.g. posterolateral foramen of Bochdalek or antero-lateral foramen of Morgagni'.
Embryogenesis: Thoracic and abdominal cavities separate from each other by closure of posterolateral pleuro-peritoneal canals at 8th week of gestation.
Failure of such closure leads to development of Foramen of Bochdalek, through which abdominal contents, usually a part of intestine, may herniate into thoracic cavity and compress the developing lung, leading to pulmonary hypoplasia and respiratory insufficiency of variable severity. Strangulation of herniated sac may also cause intestinal obstruction and sepsis.Congenital anomalies, e.g. heart defects, esophageal/ duodenal atresia, neural tube defects, renal anomalies, and chromosomal trisomies are present in ~20-30% cases.
Incidence: Diaphragmatic hernia is present in ~1: 2000 births. Most of them are on left side (70-85%). Bilateral hernia is seen in 5%, while isolated hernia through foramen of Morgagni is rare (lt;2%).
Clinical presentation depends on size of the hernial sac, severity of pulmonary hypoplasia and presence of associated anomalies.
A typical case presents in early neonatal period with-(a) progressive respiratory distress, (b) scaphoid abdomen, and (c) decreased breath sounds and presence of bowel sounds on affected side with shift of mediastinum on opposite side. Chest may be unusually prominent or bulging on affected side.
History of maternal polyhydramnios is common due to impaired absorption of amniotic fluid.
Children with smaller defects or herniation through foramen of Morgagni may present in later life with recurrent vomiting, respiratory infections and failure to thrive.
Diagnosis: Diaphragmatic hernia may be diagnosed prenatally on ultrasonography by 16-20 weeks.
Postnatal diagnosis may be confirmed on chest X-ray showing-(a) presence of air-filled bowel loops on left side, (b) absence of the cupola of diaphragm on affected side, and (c) shift of mediastinum on opposite side (Fig. 14.8). Lateral view may reveal intestines passing through the posterior portion of diaphragm.Other useful investigations include Barium contrast studies to delineate the herniated bowel segments and chest CT to identify the severity of lung hypoplasia.
D/D: Radiological appearance is characteristic but may be rarely confused with-(a) pneumothorax, (b) staphylococcal pneumonia with pneumatoceles, (c) lung cysts and (d) eventration of diaphragm.
Management of diaphragmatic hernia is essentially surgical, involving reduction of herniated segment and repair of diaphragmatic defect, as early as possible after pre-operative stabilization.
Pre-operative stabilization requires - (a) nasogastric decompression, (b) fluid and electrolyte correction, and

Fig. 14.8: Congenital diaphragmatic hernia.
(c) ventilatory assistance after endotracheal intubation. Bag and mask ventilation is contraindicated during resuscitation as air-distended herniated intestines may cause further respiratory embarrassment.
Lung hypoplasia in these cases may lead to severe pulmonary hypertension with right to left shunt, which needs to be treated with vasodilators (dopamine, nitric oxide inhalation), surfactant and extracorporeal membrane oxygenation, if possible.
In antenatally diagnosed cases, in utero reduction of hernial sac or tracheal ligation to prevent egress of lung fluids and pulmonary hypoplasia, has been attempted. Prognosis: Overall mortality is ~30-40%, being higher in cases with—(a) respiratory distress within 24 hours of birth, (b) severe lung hypoplasia, and (c) co-existing congenital anomalies. In operated cases, late effects like-(a) restrictive lung disease (b) GERD, (c) recurrence (~20-40%), and (d) thoracic cage deformities, (e.g.
scoliosis) are common.Other important diaphragmatic abnormalities are as follows:
Eventration, refers to congenital hypoplasia of dia phragmatic muscles, leading to elevation of entire hemidiaphragm or more commonly, the anterior crux into thoracic cavity. It is more common on left side.
Clinically, large eventration presents like diaphragmatic hernia with neonatal respiratory distress, while smaller defects may remain asymptomatic or manifest with recurrent chest infections in older children. Recurrent vomiting and abdominal pain after meals are common. Diagnosis is established on chest X-ray, showing 'rainbow' like elevation of diaphragm with smooth contour and cloudy mottling appearance of intestine below it (Fig. 14.9). Fluroscopy may be useful to differentiate it from diaphragmatic hernia, showing paucity of diaphragmatic movements on affected side.
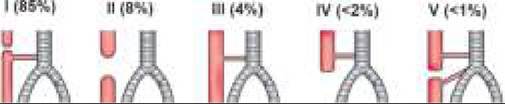
Fig. 14.9: Eventration of diaphragm.
Treatment involves fundoplication through abdominal or thoracic approach, though mild asymptomatic cases need no intervention.
Hiatus hernia denotes sliding or herniation of gastroesophageal junction or a portion of stomach through normal or patulous esophageal opening in diaphragm, usually associated with severe GERD. Treatment is directed towards GERD and not for hernia. Patients with symptomatic giant hiatal hernias need surgical intervention.
14.8