Diagnostics
Checklist for Diagnosing Neurogenic Bladder
■ Are the bladder and kidney studies up to date?
■ If voiding on own, is it overflow incontinence?
■ Is bladder size and bladder compliance appropriate for age?
■ Is post-void residual (PVR) appropriate?
■ Is the sphincter mechanism competent?
■ Is the current management preserving the kidneys?
Diagnostic Tests
■ US—Ultrasound of kidneys and bladder to determine any structural abnormalities.
■ VCUG—Voiding cystourethrogram to detect vesicoureteral reflux (VUR), evaluate the bladder contour, and evaluate the urethra. The first VCUG study is a contrast VCUG for boys and girls. Subsequent VCUG studies, for boys and especially girls, should be nuclear cystograms, as the radiation is markedly reduced.
■ UDY—Urodynamics to determine detrusor leak point pressure, uninhibited bladder contractions, detrusor sphincter dyssynergia, bladder capacity, post-void residual, and bladder compliance and sensation. The basic urodynamic formulas are:
Pressure detrusor = pressure vesical (bladder)— Pressure abdominal (rectum)
Bladder compliance = change in bladder volume / change in pressure
It is recommended that these tests (US, UDY, and VCUG) be performed in the neonatal period, as newborns with spina bifida need baseline studies. As growth of the infant is rapid in the first 12 months, abnormal studies may require two subsequent studies in the first year of life. It is generally recommended that bladder and renal ultrasounds be repeated at three-month intervals in the first year and then twice yearly the second year and then yearly. The UDY and VCUG is repeated at 3 months of age, at 1 year, then at 2-3 years of age, and then repeated every other year (83). Small-for-age and/ or high-pressure bladders may need studies more frequently.
Abnormalities on ultrasound will likely lag those found on UDY. Studies should be repeated with significant clinical changes in bowel or bladder incontinence, infections, or gait.Other Studies. The excretory urethrogram (EXU) and intravenous pyelography (IVP) tests detect urinary tract stones, anatomic abnormalities, and obstruction. Diethylene triamine acetic acid (DTPA) and mercaptoacetyltriglycine (MAG3) evaluate urinary tract (UT) drainage/obstruction. The DTPA and MAG3 attach to a radioactive tracer and are processed by the kidneys. While MAG3 is expensive, it can also be used to assess renal cortex functioning. Cystoscopy for bladder cancer surveillance is typically performed for the first time 10 years after bladder augmentation surgery or after the initialization of long-term indwelling catheter use. It is then performed yearly thereafter. Consolation with an urologist in the case of either bladder augmentation surgery or long-term indwelling catheter use is advised for current recommendation (84). Technetium 99m dimercaptosuccinic acid (DMSA) is the best test for determining the functioning areas of the renal cortex and those areas with scarring. This test should be done when there is abnormality on a renal ultrasound, a history of multiple urinary tract infections (UTIs), or pyelonephritis.
Urinalysis. The nitrate test indirectly detects urine bacteria with enzymes that reduce nitrate to nitrite in urine (eg, Klebsiella, Enterobacteriaceae, E. coli, and Proteus).
The Leukocyte Esterase Test. While leukocytes in the urine can disintegrate and disappear rapidly, leukocyte esterase persists.
Figures 9.5 and 9.6 show a normal urodynamic study and a urodynamic study reflecting spastic bladder detrusor and sphincter dyssynergia.
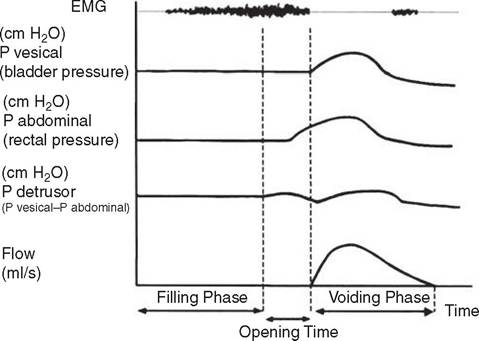
Figure 9.5 Normal urodynamic study.
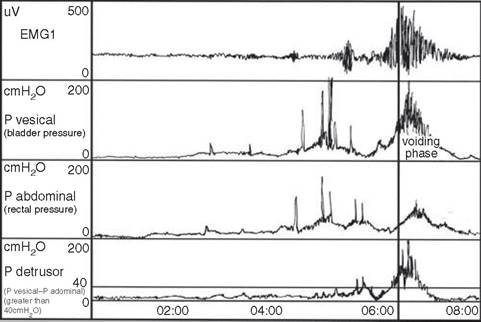
Figure 9.6 Urodynamic study reflecting spastic bladder detrusor and sphincter dyssynergia.
Risk Factors for Upper Tract/Kidney Deterioration
■ Leak point pressures >40 cm H20
■ Vesicoureteral reflux
■ Detrusor sphincter dyssynergia
■ Poor bladder compliance
■ Bladder hyperreflexia
■ Increased post-void residual (greater than 10% of the total bladder capacity)